
Heart Dysfunction in Essential Hypertension Depends on Systemic Proinflammatory Influences: A Retrospective Clinical Pathophysiological Study

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
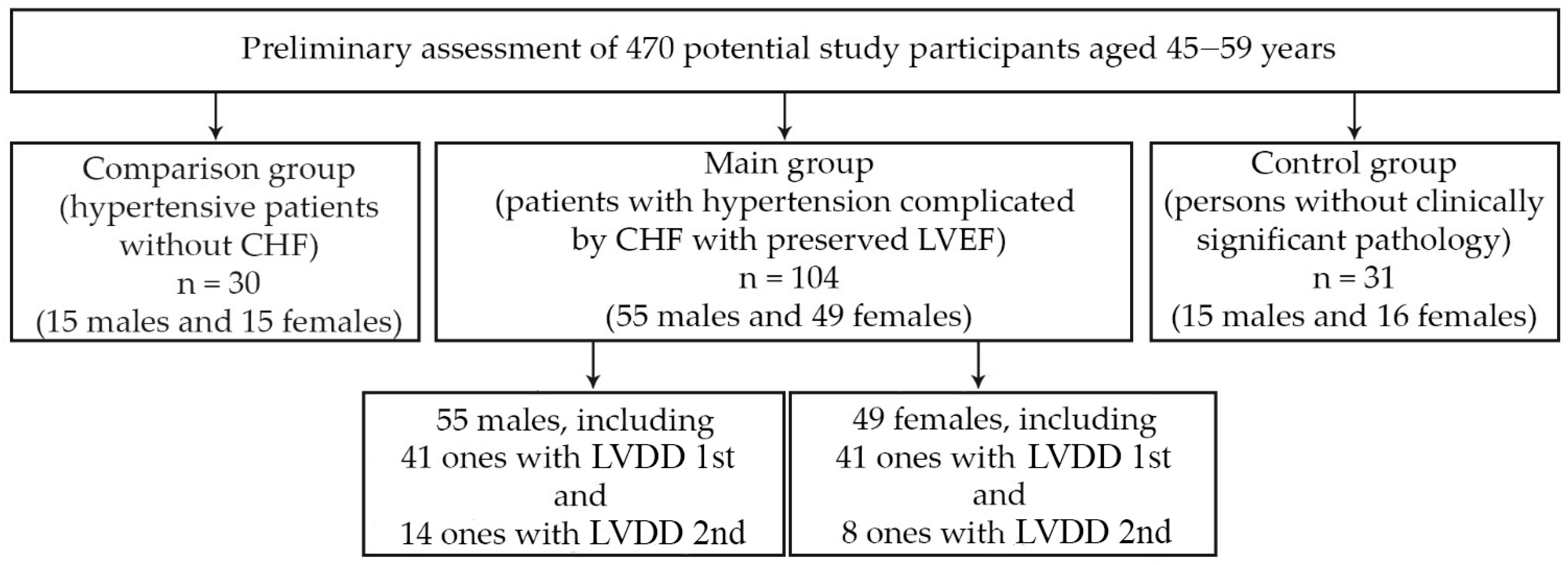
2.1. Object of the Study
2.2. Laboratory Methods
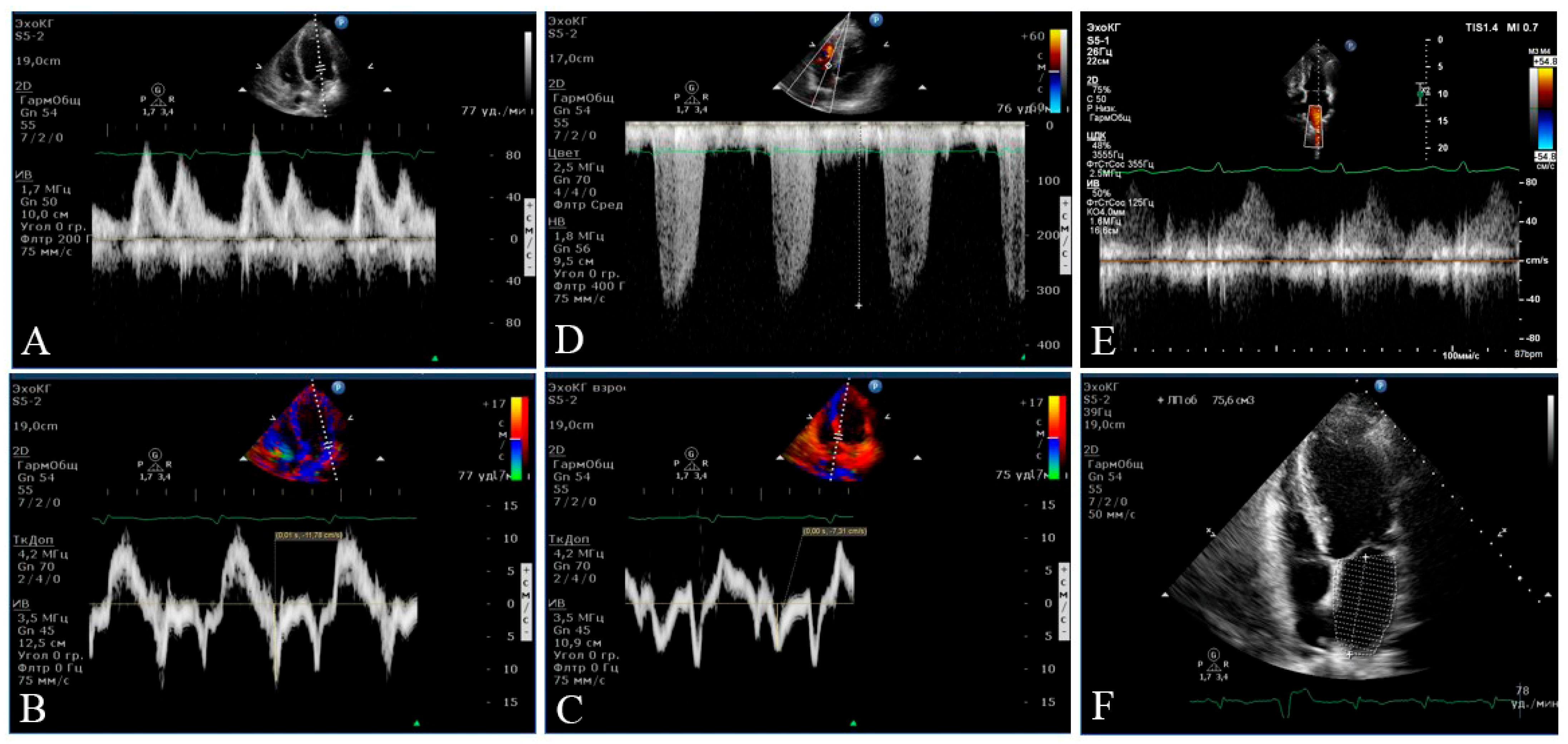
2.3. Instrumental Methods
2.4. Statistical Analysis
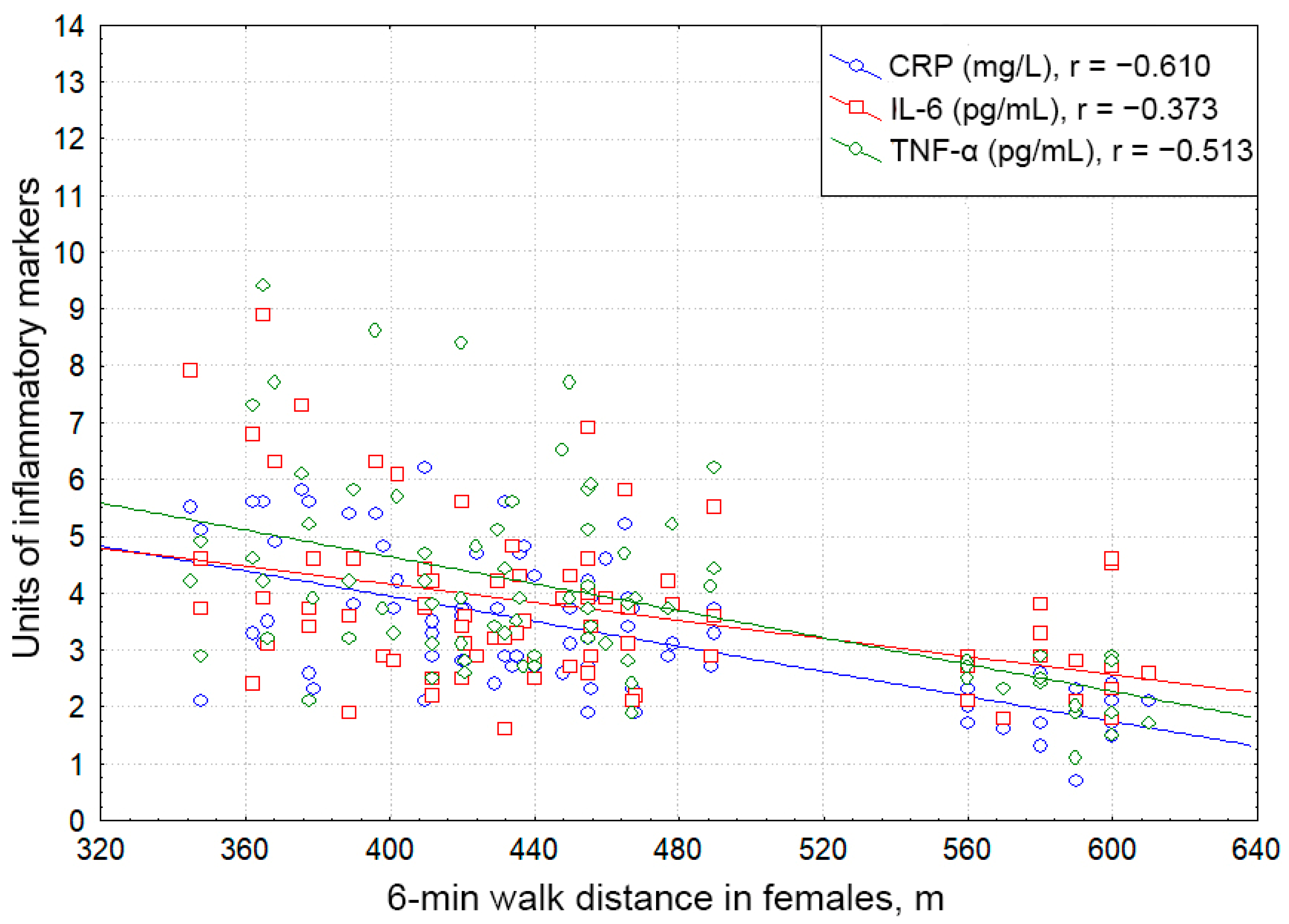
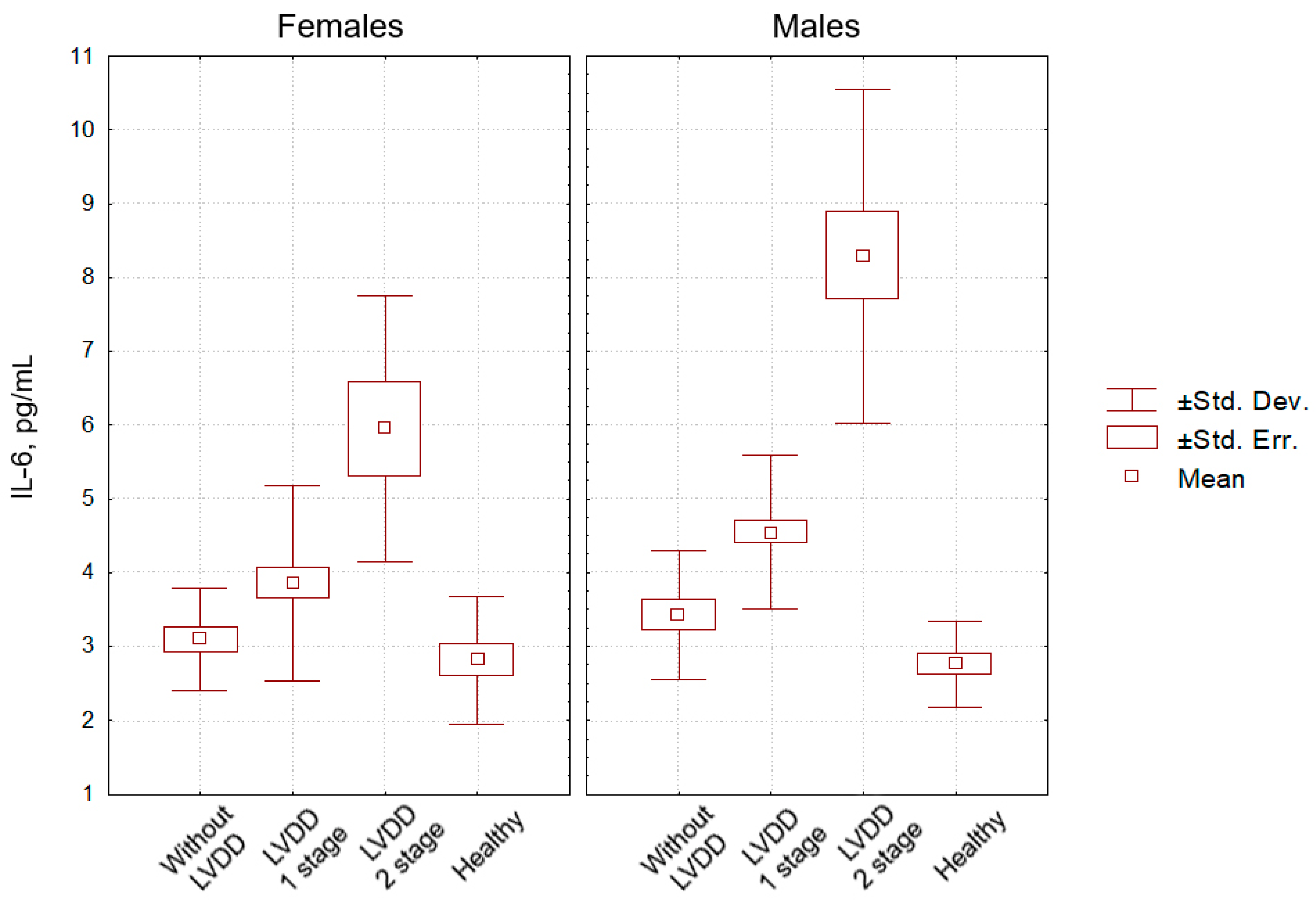
3. Results
4. Discussion
5. Conclusions
- Compared to females, males with essential hypertension complicated by HFpEF display significantly higher blood levels of pro-inflammatory autacoids: C-reactive protein, tumor necrosis factor alpha, and interleukin-6.
- The formation of the clinical syndrome of hypertensive HFpEF is associated with an increase in the intensity of systemic pro-inflammatory pattern both among males and females.
- Regardless of sex, hypertensive patients with the second stage of the left ventricular diastolic dysfunction have significantly higher (compared to the first stage) systemic blood concentrations of C-reactive protein, tumor necrosis factor alpha, and interleukin-6.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in blood pressure from 1975 to 2015: A pooled analysis of 1479 population-based measurement studies with 19·1 million participants. Lancet 2017, 389, 37–55. [Google Scholar] [CrossRef]
- Mebazaa, A.; Yilmaz, M.B.; Levy, P.; Ponikowski, P.; Peacock, W.F.; Laribi, S.; Ristic, A.D.; Lambrinou, E.; Masip, J.; Riley, J.P.; et al. Recommendations on pre-hospital & hospital management of acute heart failure: A consensus paper from the Heart Failure Association of the European Society of Cardiology, the European Society of Emergency Medicine and the Society of Academic Emergency Medicine. Eur. J. Heart Fail. 2015, 17, 544–558. [Google Scholar] [CrossRef] [PubMed]
- Sanderson, J.E. Heart failure with a normal ejection fraction. Heart 2007, 93, 55–58. [Google Scholar] [CrossRef]
- Lam, C.S.P.; Voors, A.A.; de Boer, R.A.; Solomon, S.D.; van Veldhuisen, D.J. Heart failure with preserved ejection fraction: From mechanisms to therapies. Eur. Heart J. 2018, 39, 2780–2792. [Google Scholar] [CrossRef] [PubMed]
- Ziaeian, B.; Fonarow, G.C. Epidemiology and aetiology of heart failure. Nat. Rev. Cardiol. 2016, 13, 368–378. [Google Scholar] [CrossRef] [PubMed]
- Ammar, K.A.; Jacobsen, S.J.; Mahoney, D.W.; Kors, J.A.; Redfield, M.M.; Burnett, J.C., Jr.; Rodeheffer, R.J. Prevalence and prognostic significance of heart failure stages: Application of the American College of Cardiology/American Heart Association heart failure staging criteria in the community. Circulation 2007, 115, 1563–1570. [Google Scholar] [CrossRef]
- Lüscher, T.F. Heart failure with preserved ejection fraction: Unravelling an enigma. Eur. Heart J. 2018, 39, 2763–2766. [Google Scholar] [CrossRef]
- Hollan, I.; Meroni, P.L.; Ahearn, J.M.; Cohen Tervaert, J.W.; Curran, S.; Goodyear, C.S.; Hestad, K.A.; Kahaleh, B.; Riggio, M.; Shields, K.; et al. Cardiovascular disease in autoimmune rheumatic diseases. Autoimmun. Rev. 2013, 12, 1004–1015. [Google Scholar] [CrossRef]
- Petermann Smits, D.R.; Wilde, B.; Kianersi, A.M.; de Jongh, H.; van Paassen, P.; Cohen Tervaert, J.W. Metabolic syndrome in ANCA-associated vasculitis. Rheumatology 2013, 52, 197–203. [Google Scholar] [CrossRef]
- Mahtta, D.; Gupta, A.; Ramsey, D.J.; Rifai, M.A.; Mehta, A.; Krittanawong, C.; Lee, M.T.; Nasir, K.; Samad, Z.; Blumenthal, R.S.; et al. Autoimmune Rheumatic Diseases and Premature Atherosclerotic Cardiovascular Disease: An Analysis from the VITAL Registry. Am. J. Med. 2020, 133, 1424–1432.e1. [Google Scholar] [CrossRef]
- Haverich, A.; Boyle, E.C. Atherosclerosis Pathogenesis and Microvascular Dysfunction; Springer International Publishing: New York, NY, USA, 2019. [Google Scholar] [CrossRef]
- Heise, E.L.; Churilov, L.P.; Novitskaya, T.A.; Yablonsky, P.K.; Haverich, A. The pathogenesis of pulmonary hypertension—Vessel wall ischemia as the driving force in disease initiation and progression. Vestn. St. Petersburg Univ. Med. 2021, 16, 20–36. [Google Scholar] [CrossRef]
- Clifford, A.H.; Cohen Tervaert, J.W. Cardiovascular events and the role of accelerated atherosclerosis in systemic vasculitis. Atherosclerosis 2021, 325, 8–15. [Google Scholar] [CrossRef]
- Osada, H.; Minatoya, K. Updates in aortic wall pathology. Surg. Today 2021. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, J.S.C.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Otterstad, J.E. Measuring left ventricular volume and ejection fraction with the biplane Simpson’s method. Heart 2002, 88, 559–560. [Google Scholar] [CrossRef]
- Devereux, R.B.; Alonso, D.R.; Lutas, E.M.; Gottlieb, G.J.; Campo, E.; Sachs, I.; Reichek, N. Echocardiographic assessment of left ventricular hypertrophy: Comparison to necropsy findings. Am. J. Cardiol. 1986, 57, 450–458. [Google Scholar] [CrossRef]
- Aurigemma, G.; Chirinos, J.; Galderisi, M.; Gottdiener, J.; Haluska, B.; Ofili, E.; Marwick, T.H.; Gillebert, T.C.; Derumeaux, G.; Segers, P.; et al. Recommendations on the use of echocardiography in adult hypertension: A report from the European Association of Cardiovascular Imaging (EACVI) and the American Society of Echocardiography (ASE). Eur. Heart J. 2015, 16, 577–605. [Google Scholar] [CrossRef]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for Chamber Quantification: A Report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, Developed in Conjunction with the European Association of Echocardiography, a Branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Appleton, C.P.; Gillebert, T.C.; Marino, P.N.; Oh, J.K.; Smiseth, O.A.; Waggoner, A.D.; Flachskampf, F.A.; Pellikka, P.A.; Evangelista, A. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef]
- Pedrinelli, R.; Dell’Omo, G.; di Bello, V.; Pellegrini, G.; Pucci, L.; del Prato, S.; Penno, G. Low-Grade Inflammation and Microalbuminuria in Hypertension. Arter. Thromb. Vasc. Biol. 2004, 24, 2414–2419. [Google Scholar] [CrossRef]
- Tsioufis, C.; Stougiannos, P.; Kakkavas, A.; Toutouza, M.; Mariolis, A.; Vlasseros, I.; Stefanadis, C.; Kallikazaros, I. Relation of Left Ventricular Concentric Remodeling to Levels of C-Reactive Protein and Serum Amyloid A in Patients with Essential Hypertension. Am. J. Cardiol. 2005, 96, 252–256. [Google Scholar] [CrossRef]
- Chumak, B.A.; Dydyshko, V.T.; Yakovlev, V.V.; Barsukov, A.V.; Serdyukov, D.Y.; Yakovlev, V.A. The role of the concomitant diseases and their infectious and inflammatory factors in the formation of arterial hypertension in young and middle-aged men. Bull. Pirogov Natl. Med. Surg. Cent. 2022, 17, 69–74. [Google Scholar] [CrossRef]
- Chew, B.H.; Mastura, I.; Shariff-Ghazali, S.; Lee, P.Y.; Cheong, A.T.; Ahmad, Z.; Taher, S.W.; Haniff, J.; Mustapha, F.I.; Bujang, M.A. Determinants of uncontrolled hypertension in adult type 2 diabetes mellitus: An analysis of the Malaysian diabetes registry 2009. Cardiovasc. Diabetol. 2012, 11, 54. [Google Scholar] [CrossRef]
- Esser, N.; Legrand-Poels, S.; Piette, J.; Scheen, A.J.; Paquot, N. Inflammation as a link between obesity, metabolic syndrome and type 2 diabetes. Diabetes Res. Clin. Pr. 2014, 105, 141–150. [Google Scholar] [CrossRef]
- Kologrivova, I.V.; Suslova, T.E.; Koshel’skaya, O.A.; Vinnitskaya, I.; Trubacheva, O.A. System of Matrix Metalloproteinases and Cytokine Secretion in Type 2 Diabetes Mellitus and Impaired Carbohydrate Tolerance Associated with Arterial Hypertension. Bull. Exp. Biol. Med. 2014, 156, 635–638. [Google Scholar] [CrossRef]
- Rosen, E.D.; Spiegelman, B.M. Adipocytes as regulators of energy balance and glucose homeostasis. Nature 2006, 444, 847–853. [Google Scholar] [CrossRef]
- Wajchenberg, B.L. Depot-specific hormonal characteristics of subcutaneous and visceral adipose tissue and their relation to the metabolic syndrome. Horm. Metab. Res. 2002, 34, 616–621. [Google Scholar] [CrossRef]
- Ryabkova, V.A.; Churilov, L.P.; Shoenfeld, Y. Influenza infection, SARS, MERS and COVID-19: Cytokine storm—The common denominator and the lessons to be learned. Clin. Immunol. 2021, 223, 108652. [Google Scholar] [CrossRef]
- Stroev, Y.I.; Kaminova, O.M.; Serdyuk, I.Y.; Nitsa, N.A.; Chesnokov, O.D.; Churilov, L.P. Immunoendocrine interactions in acute and chronic diseases as a manifestation of typical conflict between systemic and local regulation. Tavricheskij Med. Biol. Vestn. 2012, 15, 230–232. (In Russian) [Google Scholar]
- DuBrock, H.M.; Abou-Ezzeddine, O.F.; Redfield, M.M. High-sensitivity C-reactive protein in heart failure with preserved ejection fraction. PLoS ONE 2018, 13, e0201836. [Google Scholar] [CrossRef] [PubMed]
- Sveklina, T.S.; Talantseva, M.S.; Barsukov, A.V. The metabolic syndrome and inflammation: Actual issues of pathogenesis. Klin. Lab. Diagnost. 2013, 3, 7–10. [Google Scholar]
- Barron, L.; Dooms, H.; Hoyer, K.K.; Kuswanto, W.; Hofmann, J.; O’Gorman, W.E.; Abbas, A.K. Cutting edge: Mechanisms of IL-2-dependent maintenance of functional regulatory T cells. J. Immunol. 2010, 185, 6426–6430. [Google Scholar] [CrossRef]
- Camelliti, P.; Borg, T.K.; Kohl, P. Structural and functional characteristic of cardiac fibroblasts. Cardiovasc. Res. 2005, 65, 40–51. [Google Scholar] [CrossRef]
- Barsukov, A.V.; Shcherbakova, K.A.; Maltsev, D.S.; Burnasheva, M.A.; Kulikov, A.N. The relationship between the indicators of the retina condition and other target organ changes in uncomplicated essential hypertension. Arter. Hypertens. 2020, 6, 410–420. [Google Scholar] [CrossRef]
- Gatica, S.; Cabello-Verrugio, C.; Simon, F. Transforming growth factor-beta family: Advances in vascular function and signaling. Curr. Protein Pept. Sci. 2018, 19, 1164–1171. [Google Scholar] [CrossRef]
- Besse, S.; Nadaud, S.; Balse, E.; Pavoine, C. Early Protective Role of Inflammation in Cardiac Remodeling and Heart Failure: Focus on TNFα and Resident Macrophages. Cells 2022, 11, 1249. [Google Scholar] [CrossRef]
- Patel, J.; Sandhu, A.; Parizo, J.; Moayedi, Y.; Fonarow, G.; Heidenreich, P. Validity of performance and outcome measures for heart failure. Circ. Heart Fail. 2018, 11, e005035. [Google Scholar] [CrossRef]
- Hwang, S.; Harris, T.J.; Wilson, N.W.; Maisel, A.S. Immune function in patients with chronic stable congestive heart failure. Am. Heart J. 1993, 125, 1651–1658. [Google Scholar] [CrossRef]
- Singh, M.V.; Chapleau, M.W.; Harwani, S.C.; Abboud, F.M. The immune system and hypertension. Immunol. Res. 2014, 59, 243–253. [Google Scholar] [CrossRef]
- Amin, M.N.; Siddiqui, S.A.; Ibrahim, M.; Hakim, M.L.; Ahammed, M.S.; Kabir, A.; Sultana, F. Inflammatory cytokines in the pathogenesis of cardiovascular disease and cancer. SAGE Open Med. 2020, 8, 2050312120965752. [Google Scholar] [CrossRef]
- Kosar, F.; Aksoy, Y.; Ozguntekin, G.; Ozerol, I.; Varol, E. Relationship between cytokines and tumour markers in patients with chronic heart failure. Eur. J. Heart Fail. 2006, 8, 270–274. [Google Scholar] [CrossRef]
- Lamb, F.S.; Choi, H.; Miller, M.R.; Stark, R.J. TNFα and Reactive Oxygen Signaling in Vascular Smooth Muscle Cells in Hypertension and Atherosclerosis. Am. J. Hypertens. 2020, 33, 902–913. [Google Scholar] [CrossRef]
- Niethammer, M.; Sieber, M.; von Haehling, S.; Anker, S.D.; Munzel, T.; Horstick, G.; Genth-Zotz, S. Inflammatory pathways in patients with heart failure and preserved ejection fraction. Int. J. Cardiol. 2008, 129, 111–117. [Google Scholar] [CrossRef]
- Wu, C.-K.; Lee, J.-K.; Chiang, F.-T.; Yang, C.-H.; Huang, S.-W.; Hwang, J.-J.; Lin, J.-L.; Tseng, C.-D.; Chen, J.-J.; Tsai, C.-T. Plasma levels of tumor necrosis factor-α and interleukin-6 are associated with diastolic heart failure through downregulation of sarcoplasmic reticulum Ca2+ ATPase. Crit. Care Med. 2011, 39, 984–992. [Google Scholar] [CrossRef]
- Van Tassell, B.W.; Arena, R.; Biondi-Zoccai, G.; Canada, J.M.; Oddi, C.; Abouzaki, N.A.; Jahangiri, A.; Falcao, R.; Kontos, M.C.; Shah, K.B.; et al. Effects of interleukin-1 blockade with anakinra on aerobic exercise capacity in patients with heart failure and preserved ejection fraction (from the D-HART pilot study). Am. J. Cardiol. 2014, 113, 321–327. [Google Scholar] [CrossRef]
- Knaut, C.; Bonfanti Mesquita, C.; Dourado, V.Z.; de Godoy, I.; Tanni, S.E. Evaluation of Inflammatory Markers in Patients Undergoing a Short-Term Aerobic Exercise Program while Hospitalized due to Acute Exacerbation of COPD. Int. J. Inflam. 2020, 2020, 6492720. [Google Scholar] [CrossRef]
- De With, R.R.; Arita, V.A.; Nguyen, B.; Linz, D.; Cate, H.; Spronk, H.; Schotten, U.; van Zonneveld, A.; Erküner, O.; Bayón, M.; et al. Different circulating biomarkers in women and men with paroxysmal atrial fibrillation: Results from the AF-RISK and RACE V studies. Europace 2022, 24, 193–201. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Males (n = 55) | Females (n = 49) | p Value |
|---|---|---|---|
| Age, years | 53.7 ± 6.4 | 51.5 ± 6.2 | 0.19 |
| BMI, kg/m² | 33.6 ± 5.2 | 30.3 ± 3.6 | 0.12 |
| HbA1c, % | 6.08 ± 0.09 | 5.92 ± 0.08 | 0.39 |
| NT-proBNP, pg/mL | 287 ± 96.9 | 282 ± 105 | 0.84 |
| The 6 min walk test, m | 407 ± 74 | 420 ± 80 | 0.14 |
| Office SBP, mmHg | 156 ± 8.8 | 148 ± 6.4 | 0.18 |
| Office DBP, mmHg | 90.2 ± 4.4 | 85.5 ± 5.7 | 0.32 |
| Heart rate, bpm | 74.3 ± 12.5 | 76.1 ± 8.7 | 0.21 |
| Ejection fraction, % | 62.8 ± 0.68 | 61.6 ± 0.73 | 0.27 |
| LVIDD, mm | 50.1 ± 6.61 | 49.6 ± 7.12 | 0.64 |
| LVISD, mm | 33.2 ± 5.7 | 33.6 ± 6.24 | 0.69 |
| RWT | 0.49 ± 0.07 | 0.49 ± 0.06 | 0.24 |
| LVMI, g/m2 | 128 ± 1.52 | 121 ± 1.17 | 0.03 |
| LAVI, mL/m2 | 36.7 ± 0.36 | 36.1 ± 0.34 | 0.24 |
| E/e′ | 9.85 ± 0.40 | 8.63 ± 0.38 | 0.03 |
| e′ averaged, cm/s | 7.41 ± 0.23 | 8.31 ± 0.24 | 0.009 |
| CRP, mg/L (reference ranges: 0–4.9) | 4.91 ± 0.15 | 3.77 ± 0.17 | 0.001 |
| TNF-α, pg/mL (reference ranges: 0–5.9) | 5.81 ± 0.24 | 4.74 ± 0.29 | 0.002 |
| IL-6, pg/mL (reference ranges: 0–9.9) | 5.52 ± 0.29 | 4.21 ± 0.22 | 0.001 |
| Parameters | Males (n = 15) | Females (n = 15) | p Value |
|---|---|---|---|
| Age, years | 50.4 ± 5.3 | 49.8 ± 6.7 | 0.88 |
| BMI, kg/m2 | 28.6 ± 3.4 | 29.2 ± 3.1 | 0.78 |
| HbA1c, % | 5.42 ± 0.96 | 5.09 ± 0.88 | 0.15 |
| NT-proBNP, pg/mL | 79.2 ± 5.47 | 69.6 ± 6.20 | 0.65 |
| The 6 min walk test, m | 886 ± 76.4 | 812 ± 92.3 | 0.75 |
| Office SBP, mmHg | 142.5 ± 10.3 | 145.3 ± 9.8 | 0.48 |
| Office DBP, mmHg | 90.7 ± 12.5 | 92.4 ± 10.4 | 0.40 |
| Heart rate, bpm | 72.4 ± 6.3 | 76.3 ± 8.7 | 0.55 |
| Ejection fraction, % | 64.1 ± 4.18 | 65.6 ± 3.34 | 0.66 |
| LVIDD, mm | 49.4 ± 4.67 | 51.7 ± 5.49 | 0.56 |
| LVISD, mm | 32.7 ± 3.93 | 34.6 ± 5.14 | 0.71 |
| RWT | 0.48 ± 0.04 | 0.50 ± 0.07 | 0.16 |
| LVMI, g/m2 | 122 ± 3.85 | 105 ± 7.14 | 0.01 |
| LAVI, mL/m2 | 29.2 ± 1.47 | 27.6 ± 2.20 | 0.05 |
| E/e′ | 6.66 ± 0.61 | 6.46 ± 0.58 | 0.17 |
| e′ averaged, cm/s | 11.8 ± 1.37 | 12.1 ± 1.09 | 0.19 |
| CRP, mg/L (reference ranges: 0–4.9) | 3.58 ± 0.98 | 3.42 ± 1.02 | 0.09 |
| TNF-α, pg/mL (reference ranges: 0–5.9) | 3.68 ± 1.06 | 3.33 ± 0.77 | 0.12 |
| IL-6, pg/mL (reference ranges: 0–9.9) | 3.42 ± 0.86 | 3.09 ± 0.68 | 0.10 |
| Parameters | Males (n = 15) | Females (n = 16) | p Value |
|---|---|---|---|
| Age, years | 51.3 ± 4.2 | 50.1 ± 4.5 | 0.47 |
| BMI, kg/m2 | 24.6 ± 1.7 | 25.2 ± 1.8 | 0.16 |
| HbA1c, % | 5.1 ± 1.1 | 5.2 ± 0.8 | 0.35 |
| NT-proBNP, pg/mL | 35.7 ± 6.1 | 40.6 ± 8.2 | 0.78 |
| The 6 min walk test, m | 911 ± 102 | 895 ± 98.3 | 0.87 |
| Office SBP, mmHg | 120.5 ± 7.6 | 117.1 ± 12.5 | 0.55 |
| Office DBP, mmHg | 75.7 ± 5.1 | 70.5 ± 7.2 | 0.64 |
| Heart rate, bpm | 66.1 ± 7.9 | 70.5 ± 6.7 | 0.27 |
| Ejection fraction, % | 63.3 ± 3.98 | 64.5 ± 3.52 | 0.44 |
| LVIDD, mm | 49.3 ± 5.32 | 50.7 ± 3.41 | 0.29 |
| LVISD, mm | 33.3 ± 4.77 | 34.8 ± 3.50 | 0.38 |
| RWT | 0.47±0.04 | 0.49 ± 0.05 | 0.22 |
| LVMI, g/m2 | 98.9 ± 6.26 | 91.1 ± 3.31 | 0.06 |
| LAVI, mL/m2 | 26.7 ± 2.47 | 26.2 ± 1.94 | 0.22 |
| E/e′ | 6.4 ± 0.63 | 5.9 ± 0.49 | 0.32 |
| e′ averaged, cm/s | 11.7 ± 1.03 | 11.9 ± 1.12 | 0.66 |
| CRP, mg/L (reference ranges: 0–4.9) | 1.95 ± 1.72 | 1.85 ± 1.42 | 0.10 |
| TNF-α, pg/mL (reference ranges: 0–5.9) | 2.43 ± 1.53 | 2.29 ± 1.55 | 0.21 |
| IL-6, pg/mL (reference ranges: 0–9.9) | 2.76 ± 1.07 | 2.81 ± 1.01 | 0.79 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barsukov, A.V.; Korovin, A.E.; Churilov, L.P.; Borisova, E.V.; Tovpeko, D.V. Heart Dysfunction in Essential Hypertension Depends on Systemic Proinflammatory Influences: A Retrospective Clinical Pathophysiological Study. Pathophysiology 2022, 29, 453-468. https://doi.org/10.3390/pathophysiology29030036
Barsukov AV, Korovin AE, Churilov LP, Borisova EV, Tovpeko DV. Heart Dysfunction in Essential Hypertension Depends on Systemic Proinflammatory Influences: A Retrospective Clinical Pathophysiological Study. Pathophysiology. 2022; 29(3):453-468. https://doi.org/10.3390/pathophysiology29030036
Chicago/Turabian StyleBarsukov, Anton V., Alexander E. Korovin, Leonid P. Churilov, Ekaterina V. Borisova, and Dmitry V. Tovpeko. 2022. "Heart Dysfunction in Essential Hypertension Depends on Systemic Proinflammatory Influences: A Retrospective Clinical Pathophysiological Study" Pathophysiology 29, no. 3: 453-468. https://doi.org/10.3390/pathophysiology29030036
APA StyleBarsukov, A. V., Korovin, A. E., Churilov, L. P., Borisova, E. V., & Tovpeko, D. V. (2022). Heart Dysfunction in Essential Hypertension Depends on Systemic Proinflammatory Influences: A Retrospective Clinical Pathophysiological Study. Pathophysiology, 29(3), 453-468. https://doi.org/10.3390/pathophysiology29030036