

Natural Activators of Autophagy Increase Maximal Walking Distance and Reduce Oxidative Stress in Patients with Peripheral Artery Disease: A Pilot Study


 , , , , ,
, , , , ,  ,
, 
 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Mixture Composition
2.2. Study Outcomes
2.3. Randomization and Blinding
2.4. Blood Sampling and Preparations
2.5. Six Min Walking Test
2.6. Ankle–Brachial Index Measurements
2.7. FMD Measurement
2.8. Serum Nitric Oxide
2.9. Serum Endothelin 1 Measurements
2.10. Serum sNOX2-dp
2.11. Serum H2O2 Production
2.12. Serum Hydrogen Peroxide Scavenging Activity
2.13. Plasma ATG5 Detection
2.14. Plasma P62 Detection
2.15. Sample Size Calculation
2.16. Statistical Analyses
3. Results
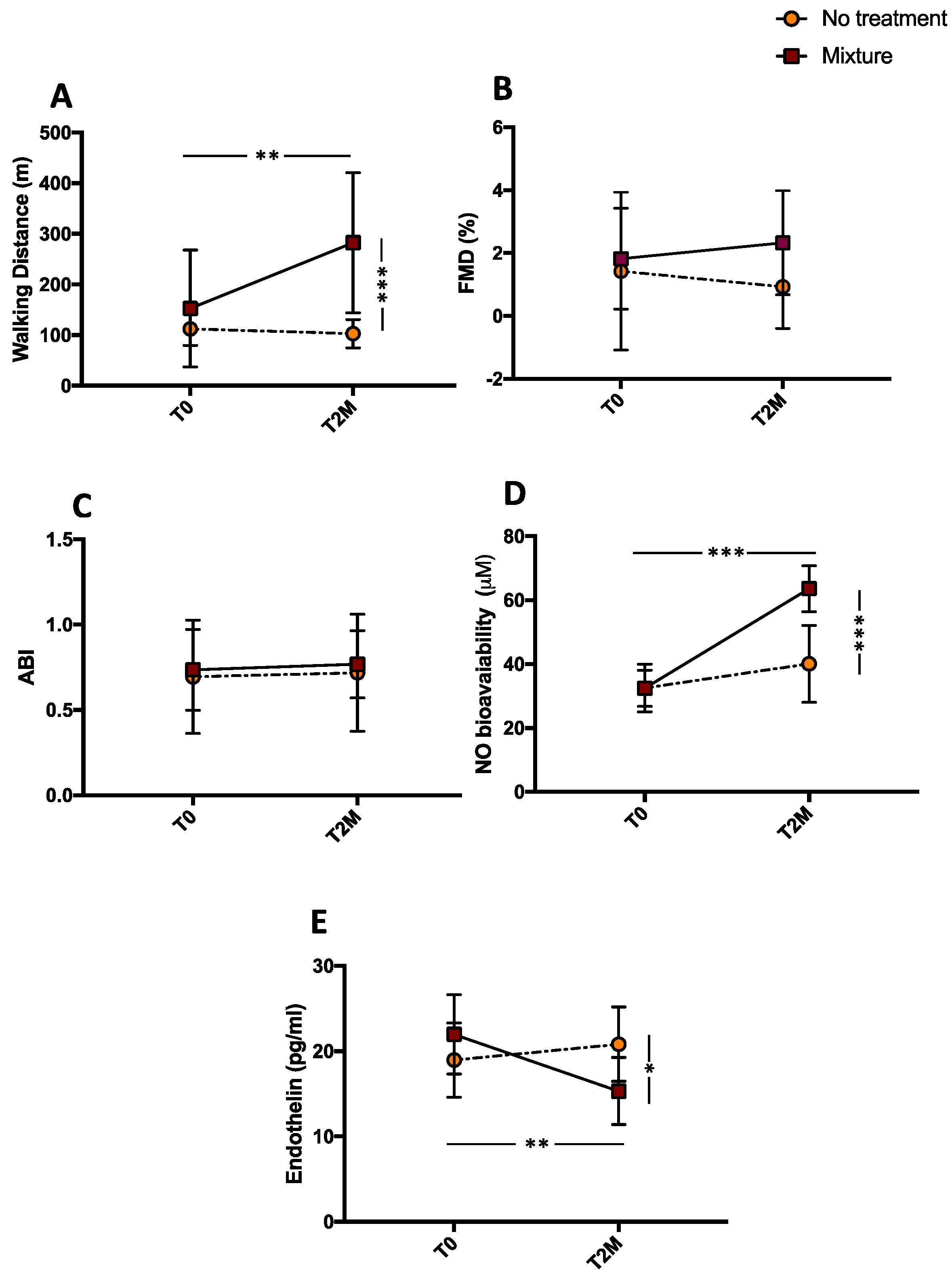
3.1. Clinical Outcome
3.2. Endothelial Dysfunction
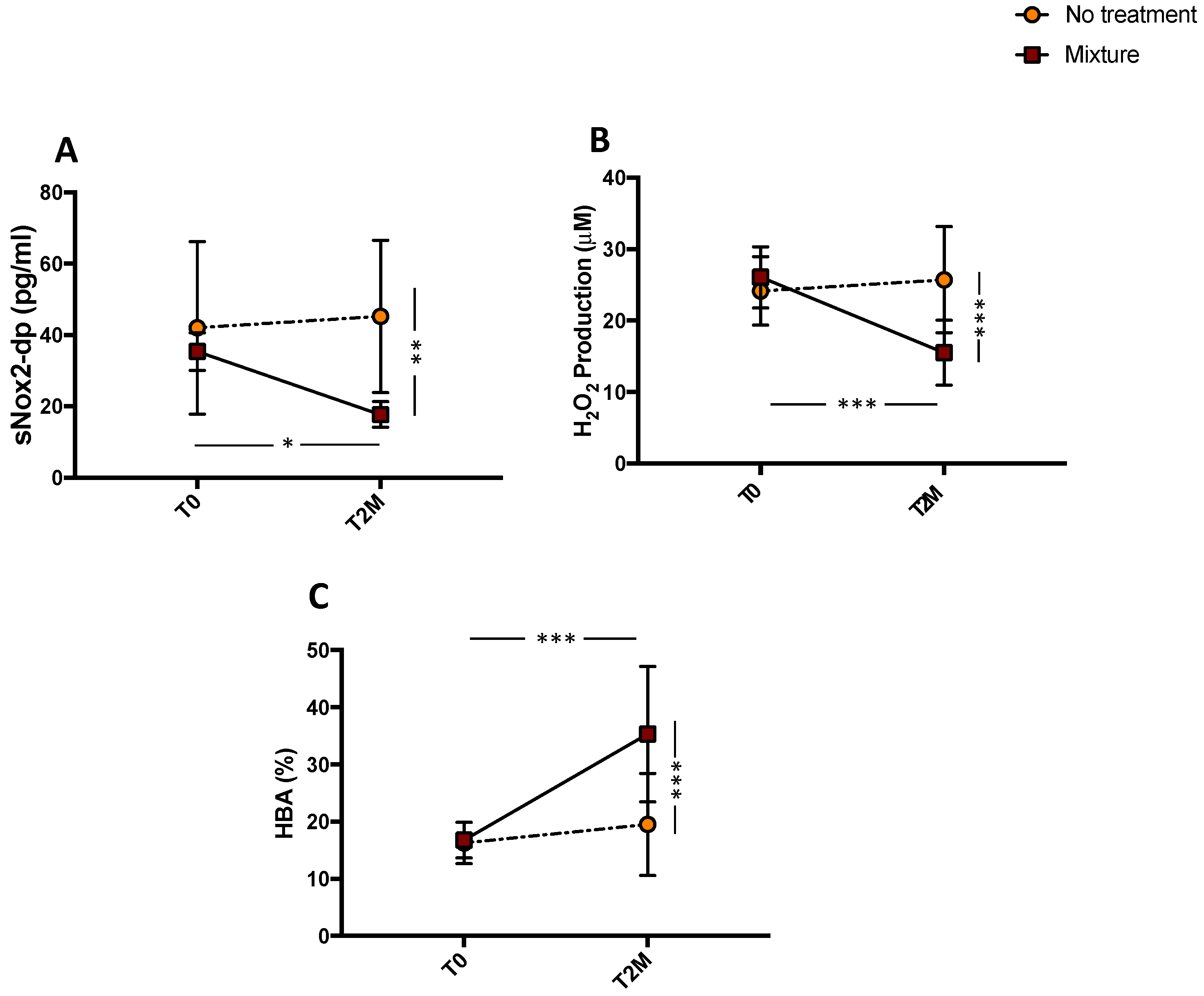
3.3. Oxidative Stress Evaluation
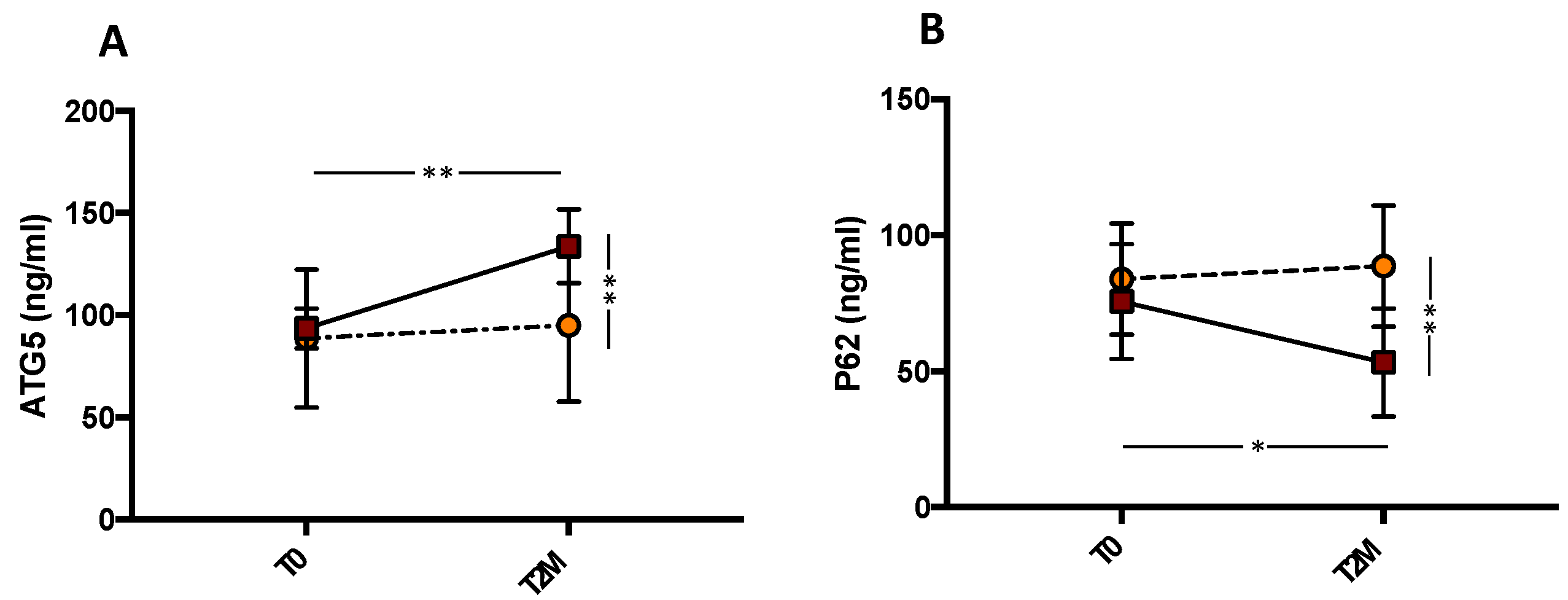
3.4. Autophagy Evaluation
3.5. Linear Correlation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Aronow, W.S. Peripheral arterial disease of the lower extremities. Arch. Med. Sci. 2012, 8, 375–388. [Google Scholar] [CrossRef] [PubMed]
- Norgren, L.; Hiatt, W.R.; Dormandy, J.A.; Nehler, M.R.; Harris, K.A.; Fowkes, F.G.R. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). J. Vasc. Surg. 2007, 45, S5–S67. [Google Scholar] [CrossRef] [PubMed]
- Selvin, E.; Erlinger, T.P. Prevalence of and risk factors for peripheral arterial disease in the United States: Results from the National Health and Nutrition Examination Survey, 1999–2000. Circulation 2004, 110, 738–743. [Google Scholar] [CrossRef] [PubMed]
- Levine, B.; Klionsky, D.J. Development by self-digestion: Molecular mechanisms and biological functions of autophagy. Dev. Cell 2004, 6, 463–477. [Google Scholar] [CrossRef]
- Li, L.; Tan, J.; Miao, Y.; Lei, P.; Zhang, Q. ROS and Autophagy: Interactions and Molecular Regulatory Mechanisms. Cell. Mol. Neurobiol. 2015, 35, 615–621. [Google Scholar] [CrossRef]
- Mizushima, N. Autophagy: Process and function. Genes Dev. 2007, 21, 2861–2873. [Google Scholar] [CrossRef] [PubMed]
- Levine, B.; Kroemer, G. Autophagy in the Pathogenesis of Disease. Cell 2008, 132, 27–42. [Google Scholar] [CrossRef] [PubMed]
- Sciarretta, S.; Forte, M.; Castoldi, F.; Frati, G.; Versaci, F.; Sadoshima, J.; Kroemer, G.; Maiuri, M.C. Caloric restriction mimetics for the treatment of cardiovascular diseases. Cardiovasc. Res. 2021, 117, 1434–1449. [Google Scholar] [CrossRef] [PubMed]
- Frati, G.; Vecchione, C.; Sciarretta, S. Novel beneficial cardiovascular effects of natural activators of autophagy. Circ. Res. 2018, 123, 947–949. [Google Scholar] [CrossRef] [PubMed]
- Elbein, A.D.; Pan, Y.T.; Pastuszak, I.; Carroll, D. New insights on trehalose: A multifunctional molecule. Glycobiology 2003, 13, 17R–27R. [Google Scholar] [CrossRef] [PubMed]
- Minutoli, L.; Altavilla, D.; Bitto, A.; Polito, F.; Bellocco, E.; Laganà, G.; Giuliani, D.; Fiumara, T.; Magazù, S.; Ruggeri, P.; et al. The disaccharide trehalose inhibits proinflammatory phenotype activation in macrophages and prevents mortality in experimental septic shock. Shock 2007, 27, 91–96. [Google Scholar] [CrossRef]
- Minutoli, L.; Altavilla, D.; Bitto, A.; Polito, F.; Bellocco, E.; Laganà, G.; Fiumara, T.; Magazù, S.; Migliardo, F.; Venuti, F.S.; et al. Trehalose: A biophysics approach to modulate the inflammatory response during endotoxic shock. Eur. J. Pharmacol. 2008, 589, 272–280. [Google Scholar] [CrossRef]
- Forte, M.; Marchitti, S.; Cotugno, M.; Di Nonno, F.; Stanzione, R.; Bianchi, F.; Schirone, L.; Schiavon, S.; Vecchio, D.; Sarto, G.; et al. Trehalose, a natural disaccharide, reduces stroke occurrence in the stroke-prone spontaneously hypertensive rat. Pharmacol. Res. 2021, 173, 105875. [Google Scholar] [CrossRef]
- Evans, T.D.; Jeong, S.J.; Zhang, X.; Sergin, I.; Razani, B. TFEB and trehalose drive the macrophage autophagy-lysosome system to protect against atherosclerosis. Autophagy 2018, 14, 724–726. [Google Scholar] [CrossRef]
- Schaeffer, V.; Goedert, M. Stimulation of autophagy is neuroprotective in a mouse model of human tauopathy. Autophagy 2012, 8, 1686–1687. [Google Scholar] [CrossRef]
- Arai, C.; Arai, N.; Mizote, A.; Kohno, K.; Iwaki, K.; Hanaya, T.; Arai, S.; Ushio, S.; Fukuda, S. Trehalose prevents adipocyte hypertrophy and mitigates insulin resistance. Nutr. Res. 2010, 30, 840–848. [Google Scholar] [CrossRef]
- DeBosch, B.J.; Heitmeier, M.R.; Mayer, A.L.; Higgins, C.B.; Crowley, J.R.; Kraft, T.E.; Chi, M.; Newberry, E.P.; Chen, Z.; Finck, B.N.; et al. Trehalose inhibits solute carrier 2A (SLC2A) proteins to induce autophagy and prevent hepatic steatosis. Sci. Signal. 2016, 9, ra21. [Google Scholar] [CrossRef]
- Sciarretta, S.; Yee, D.; Nagarajan, N.; Bianchi, F.; Saito, T.; Valenti, V.; Tong, M.; Del Re, D.P.; Vecchione, C.; Schirone, L.; et al. Trehalose-Induced Activation of Autophagy Improves Cardiac Remodeling After Myocardial Infarction. J. Am. Coll. Cardiol. 2018, 71, 1999–2010. [Google Scholar] [CrossRef]
- Eisenberg, T.; Abdellatif, M.; Schroeder, S.; Primessnig, U.; Stekovic, S.; Pendl, T.; Harger, A.; Schipke, J.; Zimmermann, A.; Schmidt, A.; et al. Cardioprotection and lifespan extension by the natural polyamine spermidine. Nat. Med. 2016, 22, 1428–1438. [Google Scholar] [CrossRef]
- Michiels, C.F.; Kurdi, A.; Timmermans, J.P.; De Meyer, G.R.Y.; Martinet, W. Spermidine reduces lipid accumulation and necrotic core formation in atherosclerotic plaques via induction of autophagy. Atherosclerosis 2016, 251, 319–327. [Google Scholar] [CrossRef]
- Kang, H.T.; Hwang, E.S. Nicotinamide enhances mitochondria quality through autophagy activation in human cells. Aging Cell 2009, 8, 426–438. [Google Scholar] [CrossRef] [PubMed]
- Forte, M.; Bianchi, F.; Cotugno, M.; Marchitti, S.; De Falco, E.; Raffa, S.; Stanzione, R.; Di Nonno, F.; Chimenti, I.; Palmerio, S.; et al. Pharmacological restoration of autophagy reduces hypertension-related stroke occurrence. Autophagy 2020, 16, 1468–1481. [Google Scholar] [CrossRef] [PubMed]
- Carnevale, R.; Nocella, C.; Schiavon, S.; Cammisotto, V.; Cotugno, M.; Forte, M.; Valenti, V.; Marchitti, S.; Vecchio, D.; Biondi Zoccai, G.; et al. Beneficial effects of a combination of natural product activators of autophagy on endothelial cells and platelets. Br. J. Pharmacol. 2021, 178, 2146–2159. [Google Scholar] [CrossRef]
- Gardner, A.W.; Montgomery, P.S.; Zhao, Y.D.; Ungvari, Z.; Csiszar, A.; Sonntag, W.E. Endothelial Cell Inflammation and Antioxidant Capacity are Associated With 6-Minute Walk Performance in Patients with Symptomatic Peripheral Artery Disease. Angiology 2018, 69, 416–423. [Google Scholar] [CrossRef] [PubMed]
- Loffredo, L.; Perri, L.; Catasca, E.; Pignatelli, P.; Brancorsini, M.; Nocella, C.; De Falco, E.; Bartimoccia, S.; Frati, G.; Carnevale, R.; et al. Dark chocolate acutely improves walking autonomy in patients with peripheral artery disease. J. Am. Heart Assoc. 2014, 3, e001072. [Google Scholar] [CrossRef]
- Aboyans, V.; Criqui, M.H.; Abraham, P.; Allison, M.A.; Creager, M.A.; Diehm, C.; Fowkes, F.G.R.; Hiatt, W.R.; Jönsson, B.; Lacroix, P.; et al. Measurement and interpretation of the Ankle-Brachial Index: A scientific statement from the American Heart Association. Circulation 2012, 126, 2890–2909. [Google Scholar] [CrossRef]
- Corretti, M.C.; Anderson, T.J.; Benjamin, E.J.; Celermajer, D.; Charbonneau, F.; Creager, M.A.; Deanfield, J.; Drexler, H.; Gerhard-Herman, M.; Herrington, D.; et al. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: A report of the international brachial artery reactivity task force. J. Am. Coll. Cardiol. 2002, 39, 257–265. [Google Scholar] [CrossRef]
- Carnevale, R.; Silvestri, R.; Loffredo, L.; Novo, M.; Cammisotto, V.; Castellani, V.; Bartimoccia, S.; Nocella, C.; Violi, F. Oleuropein, a component of extra virgin olive oil, lowers postprandial glycaemia in healthy subjects. Br. J. Clin. Pharmacol. 2018, 84, 1566–1574. [Google Scholar] [CrossRef]
- Nocella, C.; Cammisotto, V.; Bartimoccia, S.; Castellani, V.; Loffredo, L.; Pastori, D.; Pignatelli, P.; Sanguigni, V.; Violi, F.; Carnevale, R. A novel role of MMP2 in regulating platelet NOX2 activation. Free Radic. Biol. Med. 2020, 152, 355–362. [Google Scholar] [CrossRef]
- Ye, X.; Zhou, X.J.; Zhang, H. Exploring the role of autophagy-related gene 5 (ATG5ATG5) yields important insights into autophagy in autoimmune/autoinflammatory diseases. Front. Immunol. 2018, 9, 2334. [Google Scholar] [CrossRef]
- Bjørkøy, G.; Lamark, T.; Pankiv, S.; Øvervatn, A.; Brech, A.; Johansen, T. Chapter 12 Monitoring Autophagic Degradation of p62/SQSTM1. Methods Enzymol. 2009, 451, 181–197. [Google Scholar]
- Brevetti, G.; Silvestro, A.; Di Giacomo, S.; Bucur, R.; Di Donato, A.M.; Schiano, V.; Scopacasa, F. Endothdial dysfunction in peripheral arterial disease is related to increase in plasma markers of inflammation and severity of peripheral circulatory impairment but not to classic risk factors and atherosclerotic burden. J. Vasc. Surg. 2003, 38, 374–379. [Google Scholar] [CrossRef]
- Brevetti, G.; Silvestro, A.; Schiano, V.; Chiariello, M. Endothelial Dysfunction and Cardiovascular Risk Prediction in Peripheral Arterial Disease: Additive Value of Flow-Mediated Dilation to Ankle-Brachial Pressure Index. Circulation 2003, 108, 2093–2098. [Google Scholar] [CrossRef]
- Brevetti, G.; Schiano, V.; Chiariello, M. Endothelial dysfunction: A key to the pathophysiology and natural history of peripheral arterial disease? Atherosclerosis 2008, 197, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Su, J.; An, X.R.; Li, Q.; Li, X.X.; Cong, X.D.; Xu, M. Improvement of vascular dysfunction by argirein through inhibiting endothelial cell apoptosis associated with ET-1/Nox4 signal pathway in diabetic rats. Sci. Rep. 2018, 8, 12620. [Google Scholar] [CrossRef] [PubMed]
- Rapoport, R.M. Nitric oxide inhibition of endothelin-1 release in the vasculature: In vivo relevance of in vitro findings. Hypertension 2014, 64, 908–914. [Google Scholar] [CrossRef]
- De Haro Miralles, J.; Gónzalez, A.F.; Varela Casariego, C.; García, F.A. Onset of peripheral arterial disease: Role of endothelin in endothelial dysfunction☆. Interact. Cardiovasc. Thorac. Surg. 2010, 10, 760–765. [Google Scholar] [CrossRef]
- Loffredo, L.; Pignatelli, P.; Cangemi, R.; Andreozzi, P.; Panico, M.A.; Meloni, V.; Violi, F. Imbalance between nitric oxide generation and oxidative stress in patients with peripheral arterial disease: Effect of an antioxidant treatment. J. Vasc. Surg. 2006, 44, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Loffredo, L.; Carnevale, R.; Cangemi, R.; Angelico, F.; Augelletti, T.; Di Santo, S.; Calabrese, C.M.; Della Volpe, L.; Pignatelli, P.; Perri, L.; et al. NOX2 up-regulation is associated with artery dysfunction in patients with peripheral artery disease. Int. J. Cardiol. 2013, 165, 184–192. [Google Scholar] [CrossRef]
- Loffredo, L.; Marcoccia, A.; Pignatelli, P.; Andreozzi, P.; Borgia, M.C.; Cangemi, R.; Chiarotti, F.; Violi, F. Oxidative-stress-mediated arterial dysfunction in patients with peripheral arterial disease. Eur. Heart J. 2007, 28, 608–612. [Google Scholar] [CrossRef]
- Signorelli, S.S.; Scuto, S.; Marino, E.; Xourafa, A.; Gaudio, A. Oxidative stress in peripheral arterial disease (PAD) mechanism and biomarkers. Antioxidants 2019, 8, 367. [Google Scholar] [CrossRef] [PubMed]
- Hosseinpour-Moghaddam, K.; Caraglia, M.; Sahebkar, A. Autophagy induction by trehalose: Molecular mechanisms and therapeutic impacts. J. Cell. Physiol. 2018, 233, 6524–6543. [Google Scholar] [CrossRef] [PubMed]
- Lou, D.; Xing, X.; Liang, Y. Dendrobine modulates autophagy to alleviate ox-LDL-induced oxidative stress and senescence in HUVECs. Drug Dev. Res. 2022, 83, 1125–1137. [Google Scholar] [CrossRef] [PubMed]
- Dharmashankar, K.; Widlansky, M.E. Vascular endothelial function and hypertension: Insights and directions. Curr. Hypertens. Rep. 2010, 12, 448–455. [Google Scholar] [CrossRef]
- McDermott, M.M.; Guralnik, J.M.; Criqui, M.H.; Liu, K.; Kibbe, M.R.; Ferrucci, L. Six-minute walk is a better outcome measure than treadmill walking tests in therapeutic trials of patients with peripheral artery disease. Circulation 2014, 130, 61–68. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Mixture Composition | Grams (g) |
|---|---|
| Trehalose | 7.5 |
| Spermidine | 0.00225 |
| Camellia Sinensis e.s. | 0.075 |
| Catechins | 0.0375 |
| Vitamin C | 0.06 |
| Niacin | 0.00375 |
| Silica | 0.225 |
| Microcrystalline cellulose | 0.075 |
| Orange aroma | 0.3 |
| Erythritol | 2.189 |
| Sucralose | 0.036 |
| Variables | PAD Treatment (n = 10) | PAD No-Treatment (n = 10) |
|---|---|---|
| Mean age, y * | 69.6 ± 8.2 | 75.6 ± 7.6 |
| Males/females | 7/3 | 6/4 |
| Hypertension, % (n) | 90% (9) | 90% (9) |
| Diabetes mellitus, % (n) | 30% (3) | 40% (4) |
| Dyslipidemia, % (n) | 80% (8) | 50% (5) |
| Former smokers, % (n) | 40% (4) | 20% (2) |
| CHD | 30% (3) | 50% (5) |
| Previous stroke | 10% (1) | 0% (0) |
| BMI * | 26.1 ± 3 | 25.2 ± 3 |
| Pharmacological treatments, % (n) | ||
| ACE-inhibitors | 50% (5) | 100% (10) |
| Statin | 90% (9) | 100% (10) |
| Antiplatelets | 100% (10) | 100% (10) |
| Oral anticoagulants | 0% (0) | 0% (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinelli, O.; Peruzzi, M.; Bartimoccia, S.; D’Amico, A.; Marchitti, S.; Rubattu, S.; Chiariello, G.A.; D’Ambrosio, L.; Schiavon, S.; Miraldi, F.; et al. Natural Activators of Autophagy Increase Maximal Walking Distance and Reduce Oxidative Stress in Patients with Peripheral Artery Disease: A Pilot Study. Antioxidants 2022, 11, 1836. https://doi.org/10.3390/antiox11091836
Martinelli O, Peruzzi M, Bartimoccia S, D’Amico A, Marchitti S, Rubattu S, Chiariello GA, D’Ambrosio L, Schiavon S, Miraldi F, et al. Natural Activators of Autophagy Increase Maximal Walking Distance and Reduce Oxidative Stress in Patients with Peripheral Artery Disease: A Pilot Study. Antioxidants. 2022; 11(9):1836. https://doi.org/10.3390/antiox11091836
Chicago/Turabian StyleMartinelli, Ombretta, Mariangela Peruzzi, Simona Bartimoccia, Alessandra D’Amico, Simona Marchitti, Speranza Rubattu, Giovanni Alfonso Chiariello, Luca D’Ambrosio, Sonia Schiavon, Fabio Miraldi, and et al. 2022. "Natural Activators of Autophagy Increase Maximal Walking Distance and Reduce Oxidative Stress in Patients with Peripheral Artery Disease: A Pilot Study" Antioxidants 11, no. 9: 1836. https://doi.org/10.3390/antiox11091836
APA StyleMartinelli, O., Peruzzi, M., Bartimoccia, S., D’Amico, A., Marchitti, S., Rubattu, S., Chiariello, G. A., D’Ambrosio, L., Schiavon, S., Miraldi, F., Saade, W., D’Abramo, M., Pingitore, A., Loffredo, L., Nocella, C., Forte, M., & Pignatelli, P. (2022). Natural Activators of Autophagy Increase Maximal Walking Distance and Reduce Oxidative Stress in Patients with Peripheral Artery Disease: A Pilot Study. Antioxidants, 11(9), 1836. https://doi.org/10.3390/antiox11091836