
Phase II Study Combining Pembrolizumab with Aromatase Inhibitor in Patients with Metastatic Hormone Receptor Positive Breast Cancer

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics
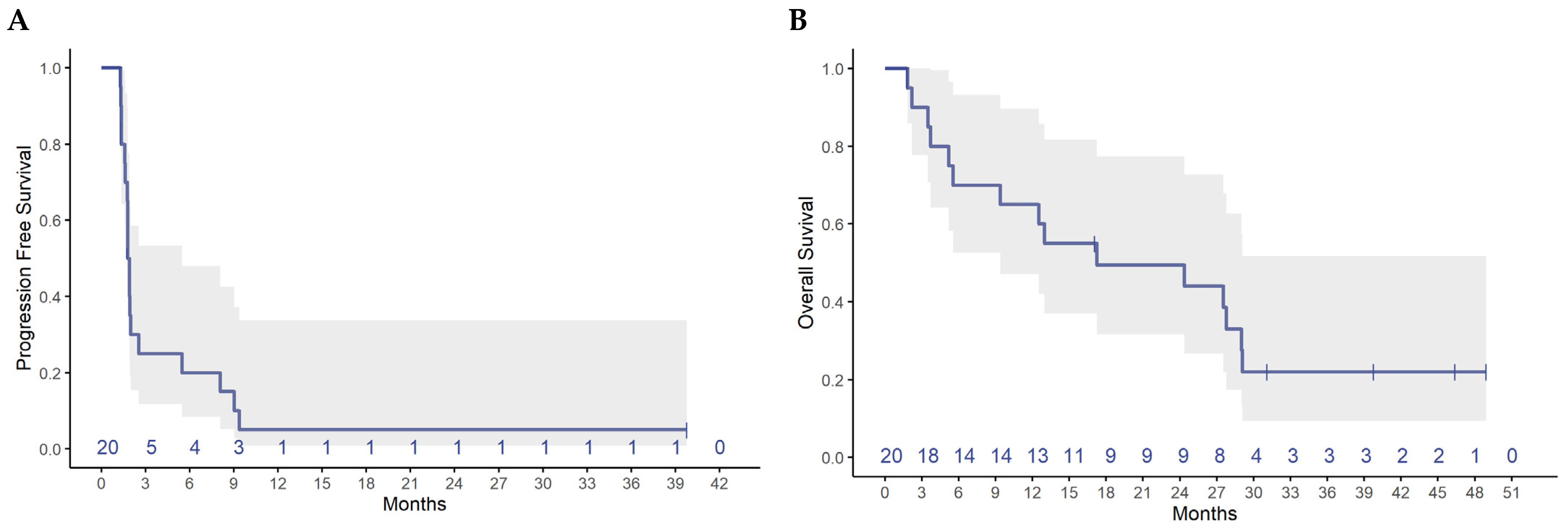
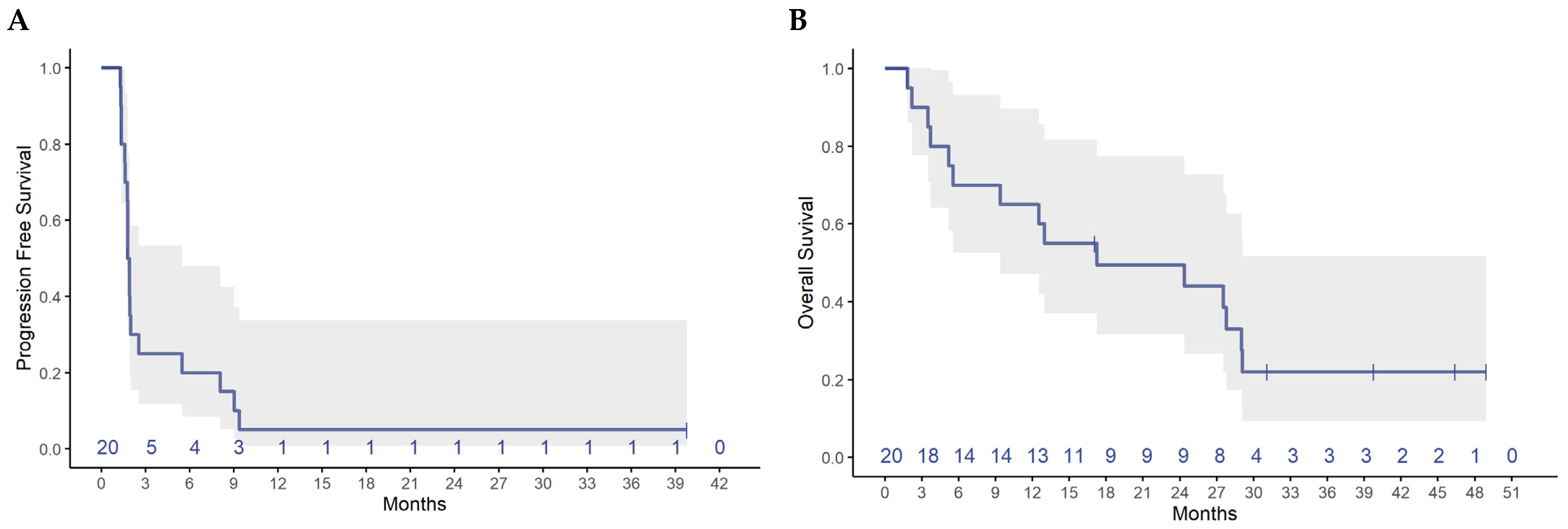
3.2. Efficacy
3.3. Safety
3.4. Immune Biomarkers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rozeboom, B.; Dey, N.; De, P. ER+ metastatic breast cancer: Past, present, and a prescription for an apoptosis-targeted future. Am. J. Cancer Res. 2019, 9, 2821–2831. [Google Scholar] [PubMed]
- Finn, R.S.; Martin, M.; Rugo, H.S.; Jones, S.; Im, S.A.; Gelmon, K.; Harbeck, N.; Lipatov, O.N.; Walshe, J.M.; Moulder, S.; et al. Palbociclib and Letrozole in Advanced Breast Cancer. N. Engl. J. Med. 2016, 375, 1925–1936. [Google Scholar] [CrossRef] [PubMed]
- Cristofanilli, M.; Turner, N.C.; Bondarenko, I.; Ro, J.; Im, S.-A.; Masuda, N.; Colleoni, M.; DeMichele, A.; Loi, S.; Verma, S.; et al. Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): Final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol. 2016, 17, 425–439. [Google Scholar] [PubMed]
- Hortobagyi, G.N.; Stemmer, S.M.; Burris, H.A.; Yap, Y.-S.; Sonke, G.S.; Paluch-Shimon, S.; Campone, M.; Blackwell, K.L.; André, F.; Winer, E.P.; et al. Ribociclib as First-Line Therapy for HR-Positive, Advanced Breast Cancer. N. Engl. J. Med. 2016, 375, 1738–1748. [Google Scholar] [CrossRef]
- Dickler, M.N.; Tolaney, S.M.; Rugo, H.S.; Cortés, J.; Diéras, V.; Patt, D.; Wildiers, H.; Hudis, C.A.; O’Shaughnessy, J.; Zamora, Z.; et al. MONARCH 1, A Phase II Study of Abemaciclib, a CDK4 and CDK6 Inhibitor, as a Single Agent, in Patients with Refractory HR(+)/HER2(−) Metastatic Breast Cancer. Clin. Cancer Res. 2017, 23, 5218–5224. [Google Scholar] [CrossRef]
- Baselga, J.; Campone, M.; Piccart, M.; Burris, H.A., 3rd; Rugo, H.S.; Sahmoud, T.; Noguchi, S.; Gnant, M.; Pritchard, K.I.; Lebrun, F.; et al. Everolimus in postmenopausal hormone-receptor-positive advanced breast cancer. N. Engl. J. Med. 2012, 366, 520–529. [Google Scholar] [CrossRef]
- André, F.; Ciruelos, E.; Rubovszky, G.; Campone, M.; Loibl, S.; Rugo, H.S.; Iwata, H.; Conte, P.; Kaufman, B.; Yamashita, T.; et al. Alpelisib for PIK3CA-Mutated, Hormone Receptor-Positive Advanced Breast Cancer. N. Engl. J. Med. 2019, 380, 1929–1940. [Google Scholar] [CrossRef]
- PD-1 Inhibitor Promising in Treatment of Triple-Negative Breast Cancer. Hum. Vaccin Immunother. 2015, 11, 1298. Available online: https://pubmed.ncbi.nlm.nih.gov/26290901/ (accessed on 29 August 2022).
- Schmid, P.; Adams, S.; Rugo, H.S.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Diéras, V.; Hegg, R.; Im, S.-A.; Shaw Wright, G.; et al. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. N. Engl. J. Med. 2018, 379, 2108–2121. [Google Scholar] [CrossRef]
- Cortes, J.; Cescon, D.W.; Rugo, H.S.; Nowecki, Z.; Im, S.A.; Yusof, M.M.; Gallardo, C.; Lipatov, O.; Barrios, C.H.; Holgado, E.; et al. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): A randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet 2020, 396, 1817–1828. [Google Scholar] [CrossRef]
- Guo, H.; Ding, Q.; Gong, Y.; Gilcrease, M.Z.; Zhao, M.; Zhao, J.; Sui, D.; Wu, Y.; Chen, H.; Liu, H.; et al. Comparison of three scoring methods using the FDA-approved 22C3 immunohistochemistry assay to evaluate PD-L1 expression in breast cancer and their association with clinicopathologic factors. Breast Cancer Res. BCR 2020, 22, 69. [Google Scholar] [CrossRef] [PubMed]
- Shuai, C.; Yang, X.; Pan, H.; Han, W. Estrogen Receptor Downregulates Expression of PD-1/PD-L1 and Infiltration of CD8(+) T Cells by Inhibiting IL-17 Signaling Transduction in Breast Cancer. Front. Oncol. 2020, 10, 582863. [Google Scholar] [CrossRef]
- Frankel, P.H.; Chung, V.; Tuscano, J.; Siddiqi, T.; Sampath, S.; Longmate, J.; Groshen, S.; Newman, E.M. Model of a Queuing Approach for Patient Accrual in Phase 1 Oncology Studies. JAMA Netw. Open 2020, 3, e204787. [Google Scholar] [CrossRef] [PubMed]
- Thürlimann, B.; Robertson, J.; Nabholtz, J.; Buzdar, A.; Bonneterre, J. Efficacy of tamoxifen following anastrozole (‘Arimidex’) compared with anastrozole following tamoxifen as first-line treatment for advanced breast cancer in postmenopausal women. Eur. J. Cancer 2003, 39, 2310–2317. [Google Scholar] [CrossRef]
- Schiavon, G.; Smith, I.E. Endocrine Therapy for Advanced/Metastatic Breast Cancer. Hematol. Clin. North Am. 2013, 27, 715–736. [Google Scholar] [CrossRef] [PubMed]
- Salgado, R.; Denkert, C.; Demaria, S.; Sirtaine, N.; Klauschen, F.; Pruneri, G.; Wienert, S.; Van den Eynden, G.; Baehner, F.L.; Penault-Llorca, F.; et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: Recommendations by an International TILs Working Group 2014. Ann. Oncol. 2015, 26, 259–271. [Google Scholar] [CrossRef]
- Muro, K.; Chung, H.C.; Shankaran, V.; Geva, R.; Catenacci, D.; Gupta, S.; Eder, J.P.; Golan, T.; Le, D.T.; Burtness, B.; et al. Pembrolizumab for patients with PD-L1-positive advanced gastric cancer (KEYNOTE-012): A multicentre, open-label, phase 1b trial. Lancet Oncol. 2016, 17, 717–726. [Google Scholar] [CrossRef]
- Dolled-Filhart, M.; Locke, D.; Murphy, T.; Lynch, F.; Yearley, J.H.; Frisman, D.; Pierce, R.; Weiner, R.; Wu, D.; Emancipator, K. Development of a Prototype Immunohistochemistry Assay to Measure Programmed Death Ligand-1 Expression in Tumor Tissue. Arch. Pathol. Lab. Med. 2016, 140, 1259–1266. [Google Scholar] [CrossRef]
- Clouthier, D.L.; Lien, S.C.; Yang, S.Y.C.; Nguyen, L.T.; Manem, V.S.K.; Gray, D.; Ryczko, M.; Razak, A.R.A.; Lewin, J.; Lheureux, S.; et al. An interim report on the investigator-initiated phase 2 study of pembrolizumab immunological response evaluation (INSPIRE). J. Immunother. Cancer 2019, 7, 72. [Google Scholar] [CrossRef]
- Rugo, H.S.; Lerebours, F.; Ciruelos, E.; Drullinsky, P.; Ruiz-Borrego, M.; Neven, P.; Park, Y.H.; Prat, A.; Bachelot, T.; Juric, D.; et al. Alpelisib plus fulvestrant in PIK3CA-mutated, hormone receptor-positive advanced breast cancer after a CDK4/6 inhibitor (BYLieve): One cohort of a phase 2, multicentre, open-label, non-comparative study. Lancet Oncol. 2021, 22, 489–498. [Google Scholar] [CrossRef]
- Rugo, H.S.; Delord, J.-P.; Im, S.-A.; Ott, P.A.; Piha-Paul, S.A.; Bedard, P.L.; Sachdev, J.; Le Tourneau, C.; van Brummelen, E.M.; Varga, A.; et al. Safety and Antitumor Activity of Pembrolizumab in Patients with Estrogen Receptor–Positive/Human Epidermal Growth Factor Receptor 2–Negative Advanced Breast Cancer. Clin. Cancer Res. 2018, 24, 2804–2811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vonderheide, R.H.; LoRusso, P.M.; Khalil, M.; Gartner, E.M.; Khaira, D.; Soulieres, D.; Dorazio, P.; Trosko, J.A.; Rüter, J.; Mariani, G.L.; et al. Tremelimumab in combination with exemestane in patients with advanced breast cancer and treatment-associated modulation of inducible costimulator expression on patient T cells. Clin. Cancer Res. 2010, 16, 3485–3494. [Google Scholar] [CrossRef] [PubMed]
- Sabatier, R.; Finetti, P.; Mamessier, E.; Adelaide, J.; Chaffanet, M.; Ali, H.R.; Viens, P.; Caldas, C.; Birnbaum, D.; Bertucci, F. Prognostic and predictive value of PDL1 expression in breast cancer. Oncotarget 2014, 6, 5449–5464. [Google Scholar] [CrossRef] [PubMed]
- Barroso-Sousa, R.; Jain, E.; Cohen, O.; Kim, D.; Buendia-Buendia, J.; Winer, E.; Lin, N.; Tolaney, S.; Wagle, N. Prevalence and mutational determinants of high tumor mutation burden in breast cancer. Ann. Oncol. 2020, 31, 387–394. [Google Scholar] [CrossRef]
- Márquez-Garbán, D.C.; Deng, G.; Comin-Anduix, B.; Garcia, A.J.; Xing, Y.; Chen, H.-W.; Cheung-Lau, G.; Hamilton, N.; Jung, M.E.; Pietras, R.J. Antiestrogens in combination with immune checkpoint inhibitors in breast cancer immunotherapy. J. Steroid Biochem. Mol. Biol. 2019, 193, 105415. [Google Scholar] [CrossRef] [PubMed]
- Bonaventura, P.; Shekarian, T.; Alcazer, V.; Valladeau-Guilemond, J.; Valsesia-Wittmann, S.; Amigorena, S.; Caux, C.; Depil, S. Cold Tumors: A Therapeutic Challenge for Immunotherapy. Front. Immunol. 2019, 10, 168. [Google Scholar] [CrossRef] [PubMed]
- Goel, S.; DeCristo, M.J.; Watt, A.C.; BrinJones, H.; Sceneay, J.; Li, B.B.; Khan, N.; Ubellacker, J.M.; Xie, S.; Metzger-Filho, O.; et al. CDK4/6 inhibition triggers anti-tumour immunity. Nature 2017, 548, 471–475. [Google Scholar] [CrossRef]
- Deng, J.; Wang, E.S.; Jenkins, R.W.; Li, S.; Dries, R.; Yates, K.; Chhabra, S.; Huang, W.; Liu, H.; Aref, A.R.; et al. CDK4/6 Inhibition Augments Antitumor Immunity by Enhancing T-cell Activation. Cancer Discov. 2018, 8, 216–233. [Google Scholar] [CrossRef]
- Yuan, Y.; Lee, J.S.; Yost, S.E.; Frankel, P.H.; Ruel, C.; Egelston, C.A.; Guo, W.; Padam, S.; Tang, A.; Martinez, N.; et al. Phase I/II trial of palbociclib, pembrolizumab and letrozole in patients with hormone receptor-positive metastatic breast cancer. Eur. J. Cancer 2021, 154, 11–20. [Google Scholar] [CrossRef]
- Egelston, C.; Guo, W.; Yost, S.; Lee, J.S.; Rose, D.; Avalos, C.; Ye, J.; Frankel, P.; Schmolze, D.; Waisman, J.; et al. Pre-existing effector T-cell levels and augmented myeloid cell composition denote response to CDK4/6 inhibitor palbociclib and pembrolizumab in hormone receptor-positive metastatic breast cancer. J. Immunother. Cancer 2021, 9, e002084. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristic | N (%) |
|---|---|
| Age (median, range) | 62 (34–79) |
| Gender | |
| Female | 20 (100%) |
| Race | |
| White | 15 (75%) |
| Asian | 3 (15%) |
| Pacific Islander | 1 (5%) |
| Unknown | 1 (5%) |
| Performance status | |
| 0 | 8 (40%) |
| 1 | 12 (60%) |
| Initial tumor stage | |
| Stage I | 2 (10%) |
| Stage II | 5 (25%) |
| Stage III | 10 (50%) |
| Stage IV | 3 (15%) |
| Initial histology grade | |
| Grade II | 15 (75%) |
| Grade III | 1 (5%) |
| Not done | 1 (5%) |
| Unknown | 3 (15%) |
| Prior surgery | 17 (85%) |
| Prior radiation | 12 (60%) |
| Lines of chemotherapy for MBC | |
| 0 | 1 (5%) |
| 1 | 3 (15%) |
| 2 | 7 (35%) |
| 3+ | 9 (45%) |
| Sites of metastasis | |
| Bone | 18 (90%) |
| Liver | 12 (60%) |
| Lung | 4 (20%) |
| Brain | 1 (5%) |
| Other * | 11 (55%) |
| Prior CDK 4/6i | 14 (70%) |
| Prior Fulvestrant | 15 (75%) |
| Prior AI | 14 (70%) |
| Prior Everolimus | 7 (35%) |
| Best Response | N (%) |
|---|---|
| PR | 2 (10%) |
| SD | 3 (15%) |
| PD | 15 (75%) |
| CBR (6 months) | 4 (20%) (95% CI 5.7, 43.7) |
| ORR (CR + PR) | 2 (10%) (95% CI 0.3, 44.5) |
| Adverse Event | Grade 2 | Grade 3 |
|---|---|---|
| All adverse events (worst grade per patient) | 12 | 2 |
| Rash | 4 (20%) | 1 (5%) * |
| Elevated AST/ALT | 1 (5%) | 1 (5%) |
| Lymphopenia | 1 (5%) * | |
| Fatigue | 7 (35%) | |
| Hot flashes | 2 (10%) | |
| Insomnia | 1 (5%) | |
| Headache | 1 (5%) | |
| Pruritus | 1 (5%) | |
| Arthralgia | 1 (5%) | |
| Dry mouth | 1 (5%) | |
| Localized edema | 1 (5%) | |
| Cough | 1 (5%) | |
| Hypertension | 1 (5%) | |
| Hypothyroidism | 1 (5%) |
| Patient ID | Best Response | Tissue | % sTILs | PD-L1 |
|---|---|---|---|---|
| COH-01 | PD | NA | NA | NA |
| COH-02 | PD | NA | NA | NA |
| COH-03 | SD | NA | NA | NA |
| COH-04 | PD | Skin | 5% | Neg |
| COH-05 | PD | Liver | 10 | 1% |
| COH-06 | SD | Breast | 5% | Neg |
| COH-07 | PD | Frontal tumor | NA | Neg |
| COH-08 | PR | Breast | NA | Neg |
| COH-09 | PD | Liver | NA | NA |
| COH-10 | PR | Supraclavicular mass | 5% | Neg |
| COH-11 | PD | Liver | 5% | Neg |
| COH-12 | PD | Bone | NA | Neg |
| COH-13 | SD | Chest wall | 10% | 50% |
| COH-14 | PD | Axillary LN | 70% | NA |
| COH-15 | PD | Ovary | NA | 2% |
| COH-16 | PD | Skin | 2% | Neg |
| COH-17 | PD | LN | NA | NA |
| COH-18 | PD | Liver | NA | Neg |
| COH-19 | PD | Chest wall | 10% | Neg |
| COH-20 | PD | Liver | NA | Neg |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ge, X.; Yost, S.E.; Lee, J.S.; Frankel, P.H.; Ruel, C.; Cui, Y.; Murga, M.; Tang, A.; Martinez, N.; Chung, S.; et al. Phase II Study Combining Pembrolizumab with Aromatase Inhibitor in Patients with Metastatic Hormone Receptor Positive Breast Cancer. Cancers 2022, 14, 4279. https://doi.org/10.3390/cancers14174279
Ge X, Yost SE, Lee JS, Frankel PH, Ruel C, Cui Y, Murga M, Tang A, Martinez N, Chung S, et al. Phase II Study Combining Pembrolizumab with Aromatase Inhibitor in Patients with Metastatic Hormone Receptor Positive Breast Cancer. Cancers. 2022; 14(17):4279. https://doi.org/10.3390/cancers14174279
Chicago/Turabian StyleGe, Xuan, Susan E. Yost, Jin Sun Lee, Paul H. Frankel, Christopher Ruel, Yujie Cui, Mireya Murga, Aileen Tang, Norma Martinez, Samuel Chung, and et al. 2022. "Phase II Study Combining Pembrolizumab with Aromatase Inhibitor in Patients with Metastatic Hormone Receptor Positive Breast Cancer" Cancers 14, no. 17: 4279. https://doi.org/10.3390/cancers14174279
APA StyleGe, X., Yost, S. E., Lee, J. S., Frankel, P. H., Ruel, C., Cui, Y., Murga, M., Tang, A., Martinez, N., Chung, S., Yeon, C., Stewart, D., Li, D., Rajurkar, S., Somlo, G., Mortimer, J., Waisman, J., & Yuan, Y. (2022). Phase II Study Combining Pembrolizumab with Aromatase Inhibitor in Patients with Metastatic Hormone Receptor Positive Breast Cancer. Cancers, 14(17), 4279. https://doi.org/10.3390/cancers14174279