A Clinical–Radiomics Nomogram for the Preoperative Prediction of Aggressive Micropapillary and a Solid Pattern in Lung Adenocarcinoma

Abstract
1. Introduction
Background
2. Materials and Methods
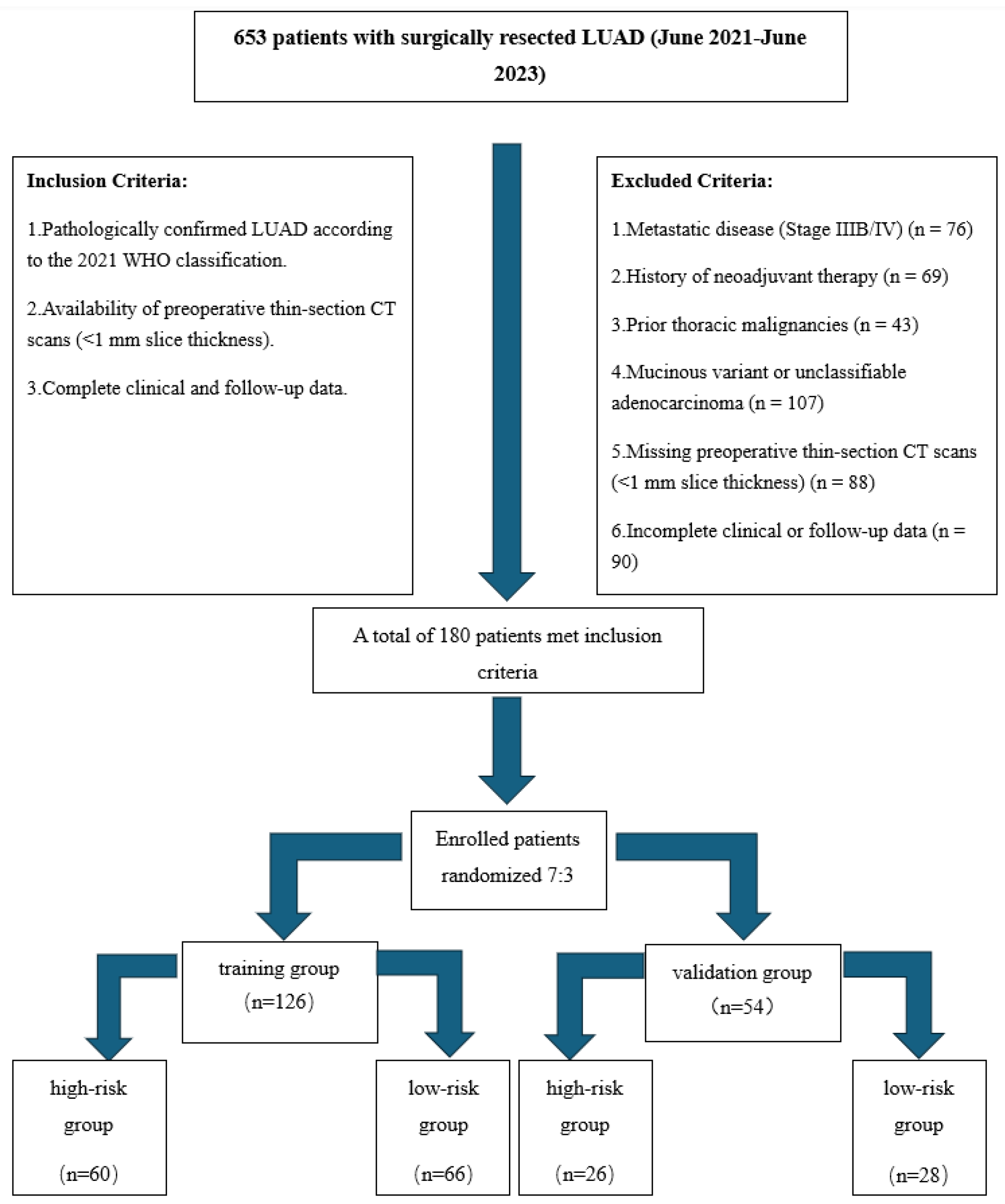
2.1. Study Design and Population
2.2. CT Acquisition and Radiomics Standardization
- Tube voltage: 120 kVp with automatic tube current modulation (SD 12–15).
- Rotation time: 0.35 s per rotation.
- Reconstruction kernel: FC81 (sharp), 1 mm isotropic voxels.
- Radiation dose: median CTDIvol of 3.2 mGy (range: 2.8–3.6 mGy); DLP: 110–150 mGy·cm.
- Contrast-enhanced CT was obtained during the venous phase (60–70 s post-injection) using Meglumine Diatrizoate (65% w/v, 306 mgI/mL). A dual-syringe injector was used to deliver 1.5–2.0 mL/kg (maximum 100 mL) of contrast at 2.5–3.0 mL/s, followed by a 30 mL saline flush. Patients fasted for ≥4 h before scanning, and renal function was verified within 72 h (eGFR > 45 mL/min/1.73 m2).
2.2.1. Image Analysis
2.2.2. Pathological Evaluation
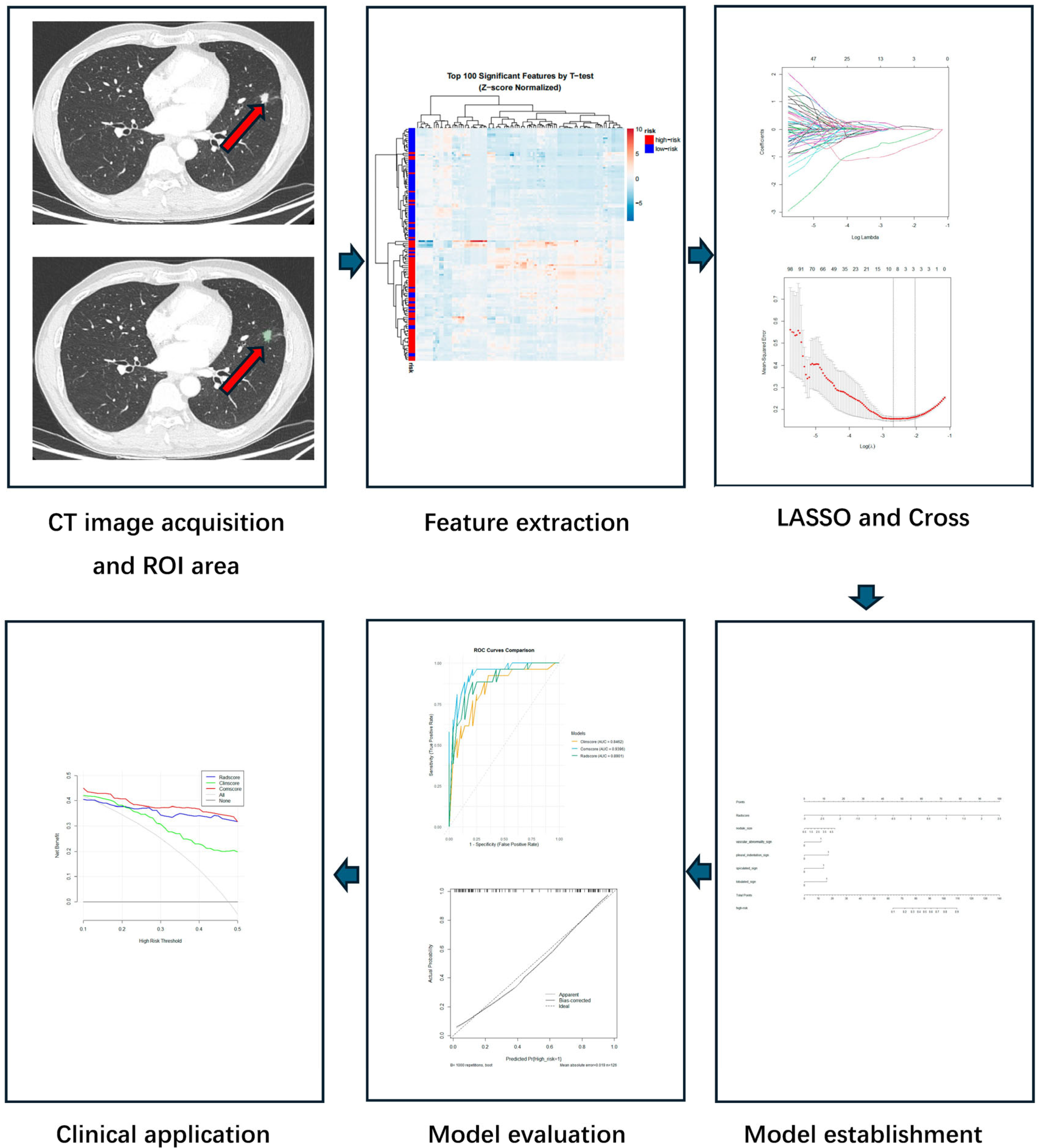
2.2.3. Radiomics Workflow
- Gray-level discretization using a fixed bin width of 25 HU within the intensity range of −1000 to 400 HU.
- Wavelet decomposition using a 3-level Haar transform (yielding 8 wavelet subbands).
- ROI segmentation was manually performed using 3D Slicer (v5.2.2) in three orthogonal planes.
- Feature extraction was conducted using PyRadiomics (v3.0) or the SlicerRadiomics extension, compliant with IBSI standards.
- The extracted features comprised first-order statistics, 2D/3D shape descriptors, and second-order texture features from the GLCM, GLRLM, GLSZM, and NGTDM matrices.
2.3. Statistical Analysis
2.3.1. Clinical Model Development
- Continuous variables: normality tested via the Shapiro–Wilk test, t-test, or Mann–Whitney U test, applied accordingly.
- Categorical variables: χ2 test or Fisher’s exact test.
- Variables significant in the univariate analysis were entered into multivariate logistic regression with forward selection.
2.3.2. Radiomics Model Development
- Prior to feature selection, all radiomics features were standardized using Z-score normalization. Subsequently, the least absolute shrinkage and selection operator (LASSO) regression with 10-fold cross-validation was performed to select the most predictive features.
- The radiomics score (RadScore) was calculated as a linear combination of the selected features weighted by their LASSO coefficients, using the original (non-normalized) feature values.
- Combined clinical and radiomics predictors were incorporated into a multivariate logistic regression model (ComScore).
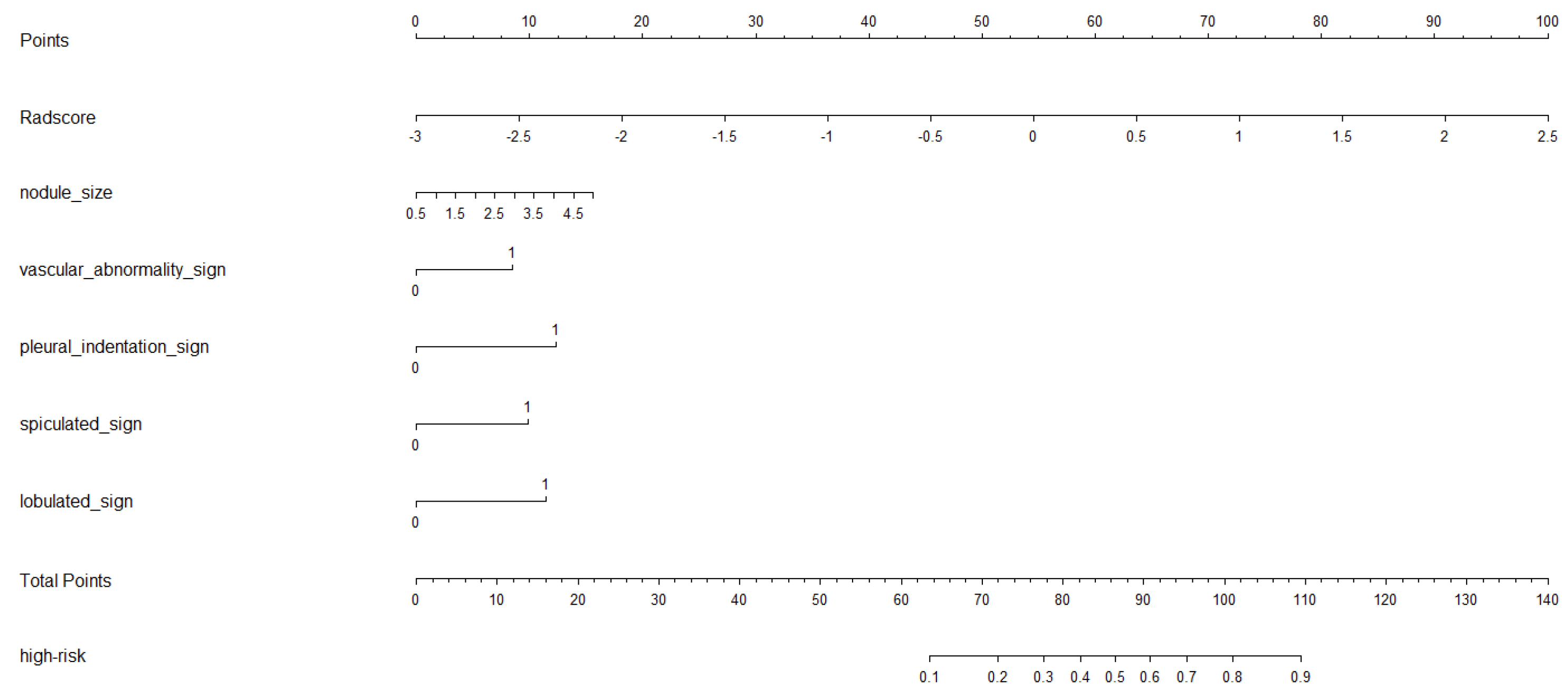
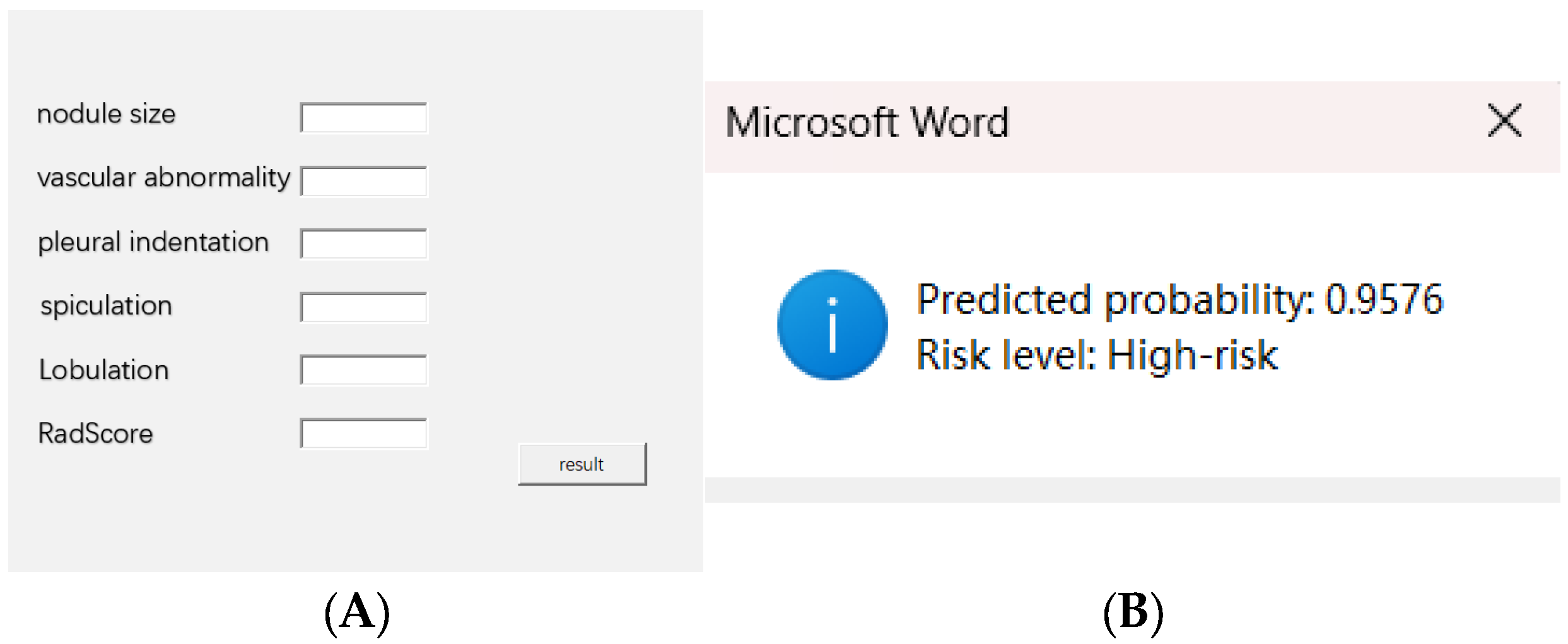
- A nomogram was constructed to visualize the model.
2.4. Model Validation and Comparison
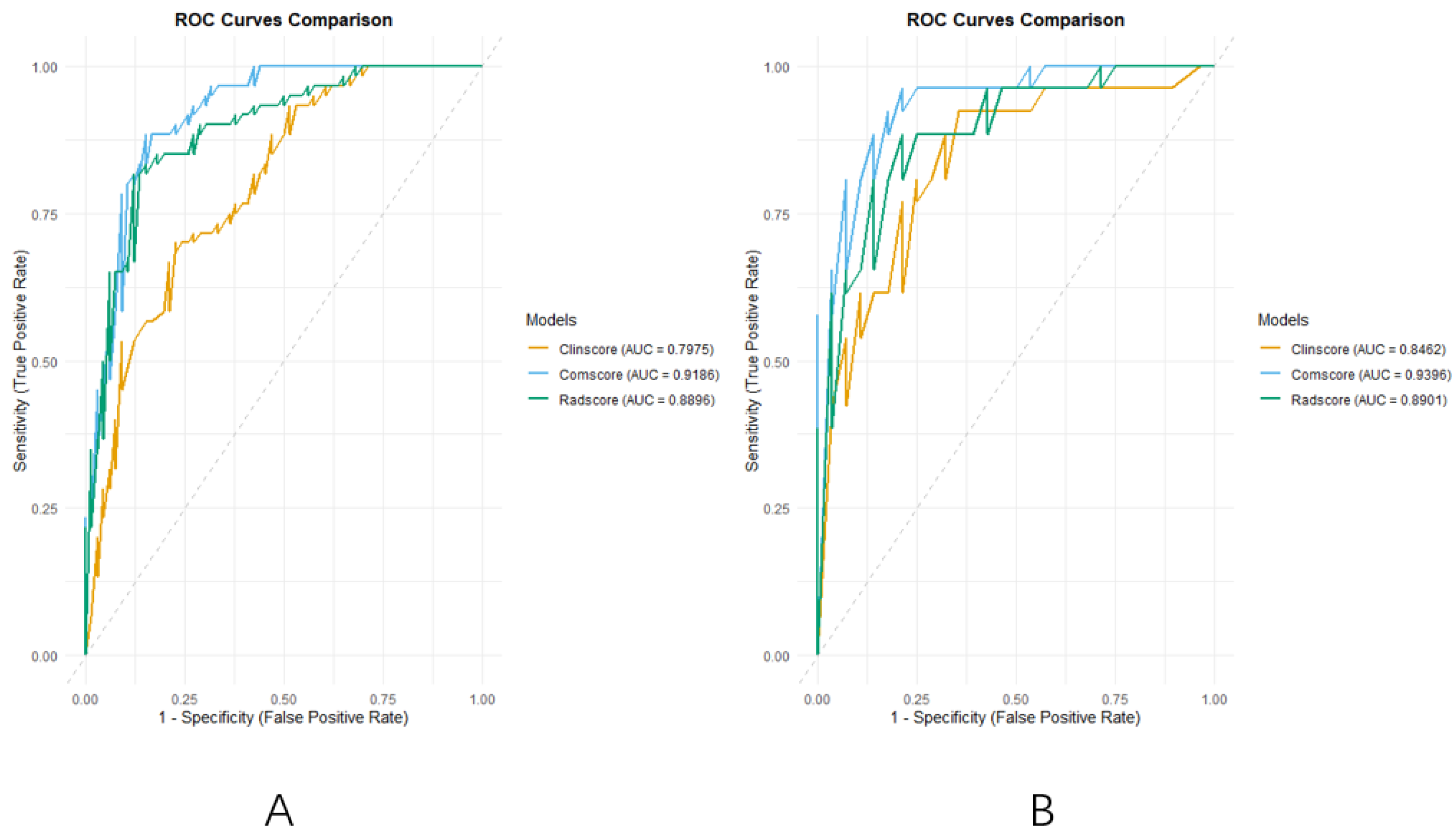
- Discrimination: Receiver operating characteristic (ROC) curve analysis was performed for each model in both the training and validation cohorts. The area under the curve (AUC) and corresponding 95% confidence intervals (CIs) were calculated to quantify the discriminative ability of each model in distinguishing between patients with and without a pneumothorax.
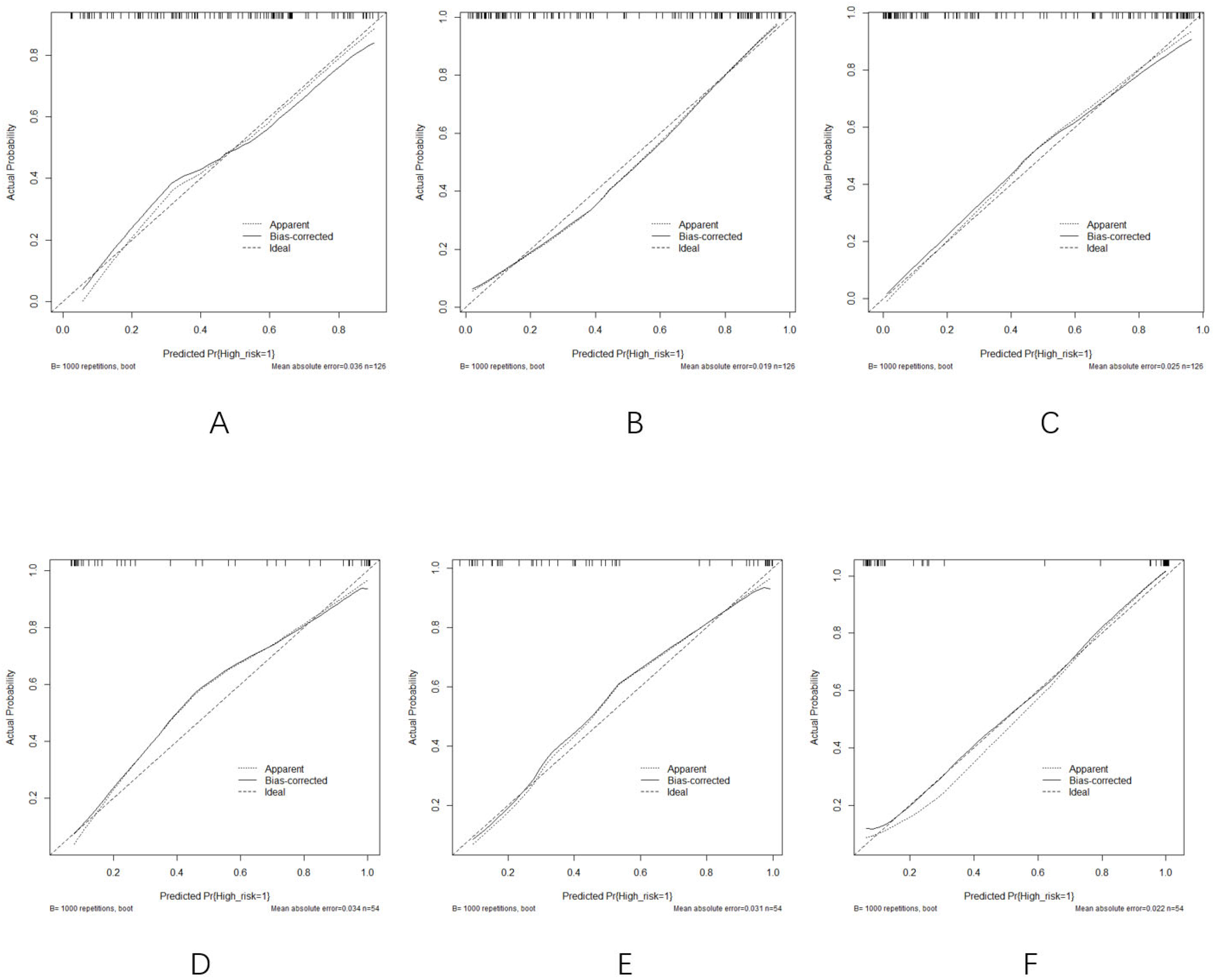
- Calibration: Calibration performance was assessed using calibration curves based on 1000 bootstrap resamples. This evaluation was conducted to determine the agreement between the predicted probabilities and the observed outcomes, ensuring the model’s reliability in clinical settings.
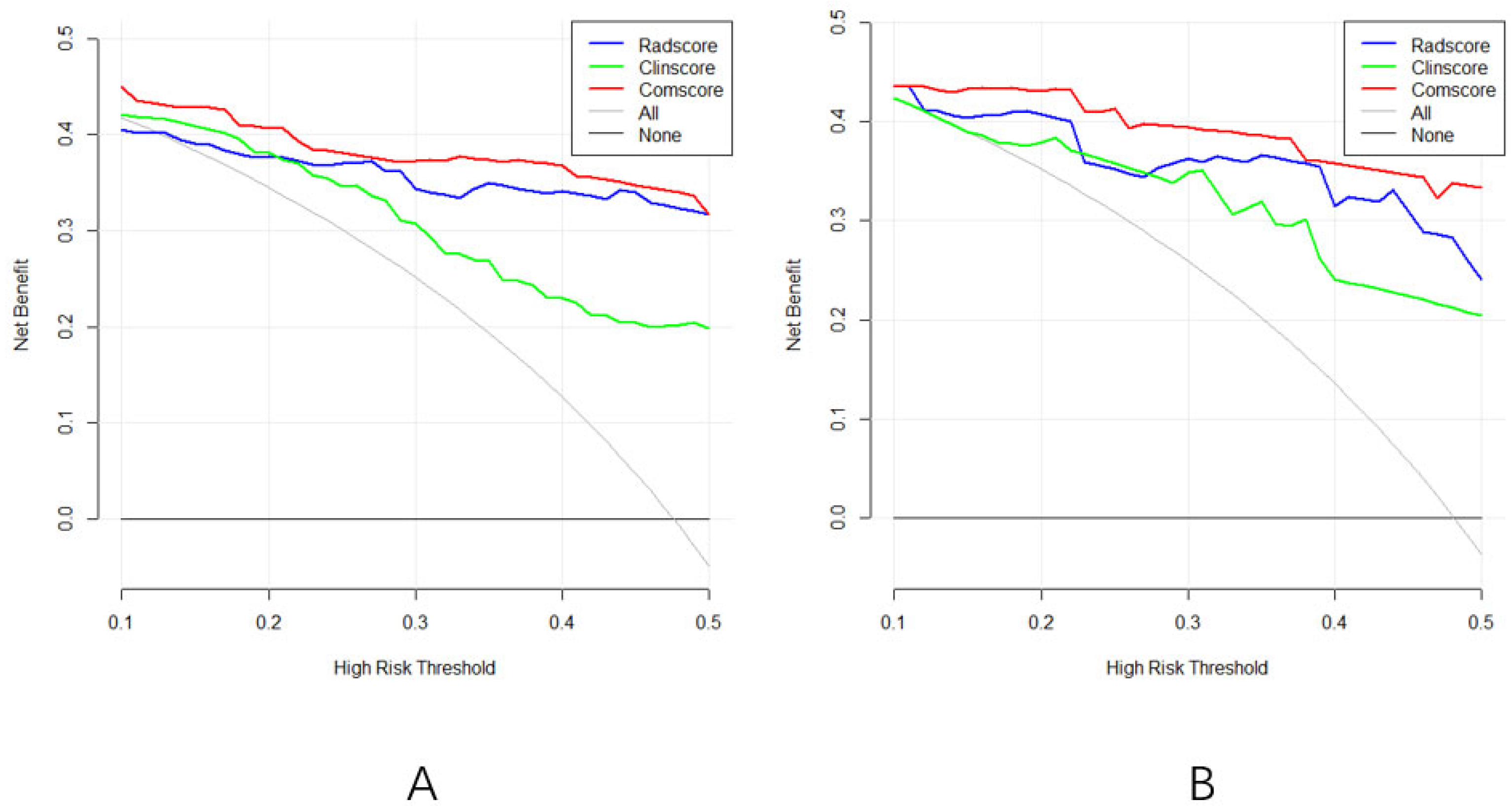
- Clinical Utility: DCA was employed to evaluate the net clinical benefit of each model across a range of threshold probabilities. This method reflects the potential utility of the models in real-world decision-making by quantifying the trade-off between true positives and false positives at varying decision thresholds.
- Comparative Performance: To assess whether differences in discrimination among models were statistically significant, DeLong’s test was applied to compare the AUC values between pairs of models in both cohorts.
- Threshold Selection and Diagnostic Performance: The optimal classification threshold for each model was determined by maximizing the Youden index, which identifies the point that optimizes the trade-off between sensitivity and specificity. At the Youden-derived threshold, additional diagnostic metrics—including sensitivity, specificity, the positive predictive value (PPV), the negative predictive value (NPV), accuracy, and the F1 score—were computed to provide a comprehensive evaluation of each model’s diagnostic performance and clinical applicability. All statistical analyses were performed using R software (version 4.2.2), with significance defined as a two-sided p-value < 0.05.
3. Results
3.1. Clinical Model Development
3.2. Radiomics Model Development
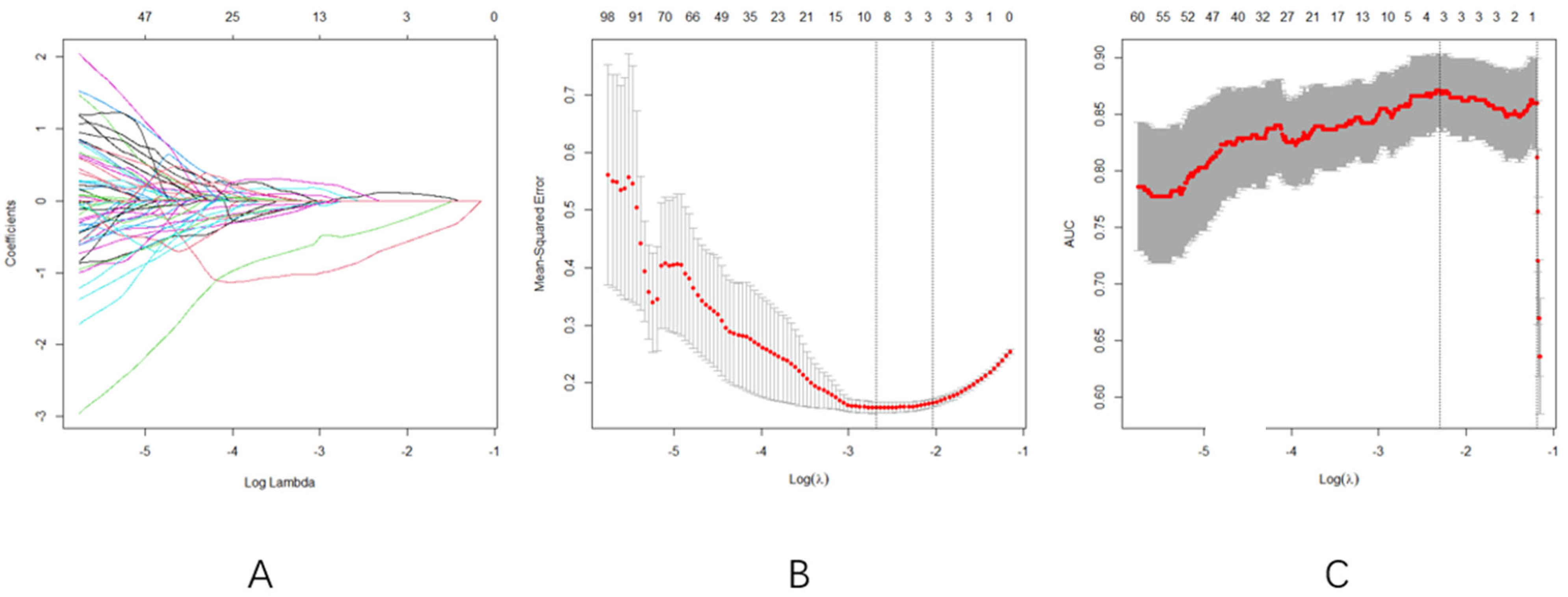
- Optimal Regularization: At log(λ) = −2.1 (Figure 3A), the model achieved equilibrium between feature sparsity (3 features retained) and predictive performance.
- Cross-validation Consistency: Both MSE and AUC plateaued in the log(λ) range of −3 to −2 (Figure 3B,C), confirming the selection stability
- LASSO regression with 10-fold cross-validation selected three radiomics features: original-firstorder-median, original-firstorder-skewness, and original-firstorder-clustershade.
3.3. Comprehensive Model Development
3.4. Model Comparison and Validation
4. Discussion
4.1. Key Findings and Interpretation
4.2. Clinical Implications of the Regression Model
4.3. Clinical and Therapeutic Relevance
4.4. Comparison with Existing Models
4.5. Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thai, A.A.; Solomon, B.J.; Sequist, L.V.; Gainor, J.F.; Heist, R.S.; Shaw, A.T.; Riely, G.J.; Ramalingam, S.S.; Gray, J.E.; Hellmann, M.D.; et al. Lung cancer. Lancet 2021, 398, 535–554. [Google Scholar] [CrossRef] [PubMed]
- Pei, Q.; Luo, Y.; Chen, Y.; Li, J.; Yang, X.; Zhang, L.; Wang, H.; Zhou, J.; Liu, Y.; Zheng, M.; et al. Artificial intelligence in clinical applications for lung cancer. Clin. Chem. Lab. Med. 2022, 60, 1974–1983. [Google Scholar] [CrossRef] [PubMed]
- Wadowska, K.; Bil-Lula, I.; Trembecki, Ł.; Śliwińska-Mossoń, M.; Milnerowicz, H. Genetic Markers in Lung Cancer Diagnosis. Int. J. Mol. Sci. 2020, 21, 4569. [Google Scholar] [CrossRef] [PubMed]
- Ashrafi, A.; Akter, Z.; Modareszadeh, P.; Harford, T.J.; Daneshian, M.; Asghari, W.; Amini, A.; Jahanban-Esfahlan, R.; Zare, P. Therapeutic Resistance in Lung Cancer. Cancers 2022, 14, 4562. [Google Scholar] [CrossRef]
- Li, Y.; Yan, B.; He, S. Advances in lung cancer treatment. Biomed. Pharmacother. 2023, 169, 115891. [Google Scholar] [CrossRef]
- Butnor, K.J. Histologic subtyping of lung adenocarcinoma. Transl. Lung Cancer Res. 2020, 9, 839–846. [Google Scholar] [CrossRef]
- Wilson, R.; Devaraj, A. Radiomics of pulmonary nodules. Transl. Lung Cancer Res. 2017, 6, 86–91. [Google Scholar] [CrossRef]
- Wang, W.; Hu, Z.; Zhao, J.; Zhang, X.; Chen, C.; Li, Q.; Wang, Y.; Liu, J.; Zhang, L.; Li, X.; et al. Micropapillary component predicts poor prognosis. J. Cardiothorac. Surg. 2020, 15, 154. [Google Scholar] [CrossRef]
- Avanzo, M.; Stancanello, J.; Pirrone, G.; Sartor, G.; Drigo, A.; Bregant, C.; Mileto, M.; Guerrisi, A.; Russo, G.; Frezza, G.; et al. Radiomics and deep learning in lung cancer. Strahlenther. Onkol. 2020, 196, 879–887. [Google Scholar] [CrossRef]
- Wang, Y.; Hu, J.; Sun, Y.; Zhang, X.; Chen, H.; Li, W.; Zhou, Q.; Liu, Y.; Zhang, Z.; Wu, Y.; et al. Micropapillary/solid component in stage IA adenocarcinoma. Medicine 2023, 102, e36503. [Google Scholar] [CrossRef]
- Choi, S.H.; Jeong, J.Y.; Lee, S.Y.; Kim, H.R.; Kim, Y.H.; Cho, B.C.; Lee, C.G.; Kim, D.J.; Kim, J.H.; Park, C.K.; et al. Minimal solid/micropapillary component. Thorac. Cancer 2021, 12, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Bensussan, A.V.; Lin, J.; Guo, C.; Zhang, Y.; Wang, L.; Chen, X.; Li, H.; Liu, Y.; Zhou, J.; Yang, K.; et al. DESI-MSI in lung cancer diagnosis. Clin. Chem. 2020, 66, 1424–1433. [Google Scholar] [CrossRef] [PubMed]
- Tosi, D.; Nosotti, M.; Bonitta, G.; Righi, I.; Mendogni, P.; Rosso, L.; Palleschi, A.; Ruggeri, P.; Santambrogio, L.; Carrinola, R.; et al. Segmentectomy vs. lobectomy. Interact. Cardiovasc. Thorac. Surg. 2021, 32, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Zuo, S.; Wei, M.; Wang, S.; Dong, D.; Tian, J.; Li, X.; Liu, L.; Zheng, X.; Chen, Y.; Fang, M.; et al. Immune-Cell Characteristic Score in LUAD. Front. Immunol. 2020, 11, 1218. [Google Scholar] [CrossRef]
- Wu, Z.; Wang, F.; Cao, W.; Xu, J.; Zhang, L.; Chen, R.; Li, X.; Liu, Y.; Zhou, J.; Yang, X.; et al. Lung cancer risk prediction models. Thorac. Cancer 2022, 13, 664–677. [Google Scholar] [CrossRef]
- Kim, Y.J.; Lee, H.J.; Kim, K.G.; Lee, S.H.; Kim, Y.H.; Han, D.H.; Kim, H.J.; Choi, Y.H.; Park, C.M. CT parameters and radiomic features. Comput. Math. Methods Med. 2019, 2019, 8790694. [Google Scholar] [CrossRef]
- Kumar, V.; Gu, Y.; Basu, S.; Berglund, A.; Eschrich, S.A.; Schabath, M.B.; Forster, K.; Aerts, H.J.; Dekker, A.; Fenstermacher, D.; et al. Radiomics: Process and challenges. Magn. Reson. Imaging 2012, 30, 1234–1248. [Google Scholar] [CrossRef]
- Hatt, M.; Krizsan, A.K.; Rahmim, A.; Bradshaw, T.J.; Costa, P.F.; Forgacs, A.; Seifert, R.; Zwanenburg, A.; El Naqa, I.; Kinahan, P.E.; et al. Radiomics guideline. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 352–375. [Google Scholar] [CrossRef]
- Mayerhoefer, M.E.; Materka, A.; Langs, G.; Häggström, I.; Szczypiński, P.; Gibbs, P.; Cook, G. Introduction to Radiomics. J. Nucl. Med. 2020, 61, 488–495. [Google Scholar] [CrossRef]
- Choi, E.R.; Lee, H.Y.; Jeong, J.Y.; Choi, Y.L.; Kim, J.H.; Kim, H.K.; Shim, Y.M.; Lee, K.S. Quantitative image variables in LUAD. Oncotarget 2016, 7, 67302–67313. [Google Scholar] [CrossRef]
- Sala, E.; Mema, E.; Himoto, Y.; Veeraraghavan, H.; Mikheev, A.; Yoshida, H.; Vargas, H.A.; Galluzzo, A.; Goldman, D.A.; Jambawalikar, S.; et al. Radiogenomics and habitat imaging. Clin. Radiol. 2017, 72, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Bousabarah, K.; Temming, S.; Hoevels, M.; Koch, D.; Borggrefe, J.; Nowak, S.; Desideri, S.; Cirillo, M.; Giraud, P.; Nierer, L.; et al. Radiomic analysis for radiation injury. Strahlenther. Onkol. 2019, 195, 830–842. [Google Scholar] [CrossRef] [PubMed]
- Liang, Z.R.; Lv, F.J.; Fu, B.J.; Li, X.T.; Wang, W.; Dong, D.; Tian, J.; Fang, M.J.; Liu, L.; Zheng, X.C.; et al. Reticulation Sign on Thin-Section CT: Utility for Predicting Invasiveness of Pure Ground-Glass Nodules. Am. J. Roentgenol. 2023, 221, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Song, L.; Xing, T.; Zhu, Z.; Yang, F.; Li, J.; Wang, J.; Liu, J.; Zhang, J.; Zhang, Y.; Xie, Y.; et al. Hybrid Clinical-Radiomics Model for Precisely Predicting the Invasiveness of Lung Adenocarcinoma Manifesting as Pure Ground-Glass Nodule. Acad. Radiol. 2021, 28, e267–e277. [Google Scholar] [CrossRef]
- Yagi, T.; Yamazaki, M.; Ohashi, R.; Ogura, T.; Masuda, M.; Matsumoto, Y.; Hattori, A.; Matsuoka, T.; Nagashima, T.; Tomizawa, K.; et al. HRCT texture analysis for pure or part-solid ground-glass nodules: Distinguishability of adenocarcinoma in situ or minimally invasive adenocarcinoma from invasive adenocarcinoma. Jpn. J. Radiol. 2018, 36, 113–121. [Google Scholar] [CrossRef]
- Wang, J.; Ma, H.; Ni, C.J.; Zhang, L.; Wang, Y.; Liu, Y.; Chen, X.; Li, W.; Zhou, Q.; Sun, Y. Clinical characteristics and prognosis of ground-glass opacity nodules in young patients. J. Thorac. Dis. 2019, 11, 557–563. [Google Scholar] [CrossRef]
- Wang, Z.; Zhang, N.; Liu, J.; Liu, J. Predicting Micropapillary or Solid Pattern of Lung Adenocarcinoma with CT-Based Radiomics, Conventional Radiographic, and Clinical Features. Respir. Res. 2023, 24, 282. [Google Scholar] [CrossRef]
- Zhang, Y.P.; Heuvelmans, M.A.; Zhang, H.; Oudkerk, M.; Vliegenthart, R.; Xie, X.Q. Changes in quantitative CT image features of ground-glass nodules in differentiating invasive pulmonary adenocarcinoma from benign and in situ lesions: Histopathological comparisons. Clin. Radiol. 2018, 73, e504-e9–e504-e16. [Google Scholar] [CrossRef]
- Miao, Y.; Zhang, J.; Zou, J.; Zhu, Z.; Li, W.; Zhou, Q.; Chen, H.; Liu, Y.; Wang, Y.; Sun, Y. Correlation in histological pattern with high resolution computed tomography signatures of early-stage lung adenocarcinoma. Transl. Lung Cancer Res. 2017, 6, 14–22. [Google Scholar] [CrossRef]
- Gao, F.; Sun, Y.; Zhang, G.; Li, Z.; Wang, H.; Chen, X.; Liu, Y.; Zheng, M.; Yang, X.; Li, J. CT characterization of different pathological types of subcentimeter pulmonary ground-glass nodular lesions. Br. J. Radiol. 2017, 92, 20180204. [Google Scholar] [CrossRef]
- Domagala-Kulawik, J.; Trojnar, A.; Safianowska, A.; Nowicka, U.; Walkiewicz, D.; Maskey-Warzechowska, M.; Chazan, R. Lung cancer in women in 21th century. J. Thorac. Dis. 2020, 12, 4398–4410. [Google Scholar] [CrossRef] [PubMed]
- Lau, S.C.M.; Pan, Y.; Velcheti, V.; Wong, K.K.; Sacher, A.G.; Costa, D.B.; Neal, J.W.; Sholl, L.M.; Heist, R.S.; Wirth, L.J.; et al. Squamous cell lung cancer: Current landscape and future therapeutic options. Cancer Cell 2022, 40, 1279–1293. [Google Scholar] [CrossRef] [PubMed]
- Holzinger, A.; Haibe-Kains, B.; Jurisica, I. Why imaging data alone is not enough: AI-based integration of imaging, omics, and clinical data. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2722–2730. [Google Scholar] [CrossRef] [PubMed]
- Sata, Y.; Nakajima, T.; Fukuyo, M.; Morimoto, J.; Hara, T.; Matsuura, R.; Ihara, S.; Miyashita, Y.; Horie, M.; Matsusaka, K.; et al. High expression of CXCL14 is a biomarker of lung adenocarcinoma with micropapillary pattern. Cancer Sci. 2020, 111, 2588–2597. [Google Scholar] [CrossRef]
- Matsushima, K.; Sonoda, D.; Mitsui, A.; Kitazono, I.; Ikeda, R.; Yoshizawa, A.; Tsuchiya, T.; Nagayasu, T. Factors associated with lymph node metastasis upstage after resection for patients with micropapillary lung adenocarcinoma. Thorac. Cancer 2022, 13, 48–53. [Google Scholar] [CrossRef]
- Wang, C.; Shao, J.; Lv, J.; Deng, L.; Xu, H.; Wang, Z.; Zhang, Y.; Liu, Y.; Zheng, M.; Yang, X.; et al. Deep learning for predicting subtype classification and survival of lung adenocarcinoma on computed tomography. Transl. Oncol. 2021, 14, 101141. [Google Scholar] [CrossRef]
- Xing, X.; Li, L.; Sun, M.; Zhang, Y.; Wang, Z.; Liu, Y.; Chen, X.; Li, W.; Zhou, Q.; Sun, Y. A combination of radiomic features, clinic characteristics, and serum tumor biomarkers to predict the possibility of the micropapillary/solid component of lung adenocarcinoma. Ther. Adv. Respir. Dis. 2024, 18, 17534666241249168. [Google Scholar] [CrossRef]
- Li, Z.; Wu, W.; Pan, X.; Chen, H.; Liu, Y.; Zhang, Z.; Wang, Y.; Sun, Y.; Zhou, Q.; Li, W. Serum tumor markers level and their predictive values for solid and micropapillary components in lung adenocarcinoma. Cancer Med. 2022, 11, 2855–2864. [Google Scholar] [CrossRef]
- Yip, S.S.F.; Aerts, H.J.W.L. Applications and limitations of radiomics. Phys. Med. Biol. 2016, 61, R150–R166. [Google Scholar] [CrossRef]
- Ganeshan, B.; Miles, K.A.; Young, R.C.D.; Chatwin, C.R. Quantifying tumour heterogeneity with CT. Cancer Imaging 2013, 13, 140–149. [Google Scholar] [CrossRef]
- Lubner, M.G.; Smith, A.D.; Sandrasegaran, K.; Sahani, D.V.; Pickhardt, P.J. CT Texture Analysis: Definitions, Applications, and Limitations. Radiographics 2017, 37, 1483–1503. [Google Scholar] [CrossRef]
- Kirienko, M.; Cozzi, L.; Antunovic, L.; Lozza, L.; Fogliata, A.; Voulaz, E.; Rossi, A.; Chiti, A.; Sollini, M. Prediction of disease-free survival by PET/CT radiomic signature in NSCLC. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 207–217. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training Group (n = 126) | Validation Group (n = 54) | |||||
|---|---|---|---|---|---|---|
| High-Risk Group | Low-Risk Group | p | High-Risk Group | Low-Risk Group | p | |
| (n = 60) | (n = 66) | (n = 26) | (n = 28) | |||
| Age | 63.91 ± 8.69 | 63.65 ± 10.84 | 0.881 | 64.00 ± 9.24 | 54.57 ± 13.91 | 0.005 |
| Height | 161.98 (156, 170) | 161.77 (158, 166.25) | 0.984 | 165.54 (159.50, 170.50) | 164.04 (158.50, 165.00) | 0.379 |
| Weight | 63.48 (54.00, 71.50) | 60.55 (53.00, 67.62) | 0.171 | 68.31 (59.50, 76.25) | 63.36 (55.00, 74.50) | 0.103 |
| BMI | 24.10 (21.34, 27.51) | 23.10 (20.26, 25.13) | 0.152 | 24.87 (22.48, 27.58) | 23.44 (21.01, 26.70) | 0.151 |
| Nodule size | 2.29 (1.50, 2.50) | 1.87 (1.30, 2.43) | 0.01 | 2.09 (1.25, 3.25) | 1.0 (0.63, 1.10) | <0.001 |
| Gender | male 26 (43.3%) | Male 20 (30.3%) | 0.129 | Male 13 (50%) | Male 18 (64.3%) | 0.289 |
| Female 34 (56.7%) | Female 46 (69.7%) | Female 13 (50%) | Female 10 (35.7%) | |||
| Smoking history | No 45 (75%) | No 53 (80.3%) | 0.475 | No 21 (80.8%) | No 23 (82.1%) | 1 |
| Yes 15 (25%) | Yes 13 (19.7%) | Yes 5 (19.2%) | Yes 5 (17.9%) | |||
| Lobulated sign | No 14 (23.3%) | No 30 (45.5%) | 0.009 | No 5 (19.2%) | No 13 (46.4%) | 0.034 |
| Yes 46 (76.7%) | Yes 36 (54.5%) | Yes 21 (80.8%) | Yes 15 (53.6%) | |||
| Spiculated sign | No 13 (21.7%) | No 30 (45.5%) | 0.005 | No 7 (26.9%) | No 17 (60.7%) | 0.013 |
| Yes47 (78.3%) | Yes 36 (54.5%) | Yes 19 (73.1%) | Yes 11 (39.3%) | |||
| Vacuole sign | No 45 (75%) | No 60 (90.9%) | 0.017 | No 17 (65.4%) | No 26 (89.3%) | 0.012 |
| Yes 15 (25%) | Yes 6 (9.1%) | Yes 9 (34.6%) | Yes 2 (10.7%) | |||
| Pleural indentation sign | No 15(25%) | No 37 (56.1%) | <0.01 | No 13 (50.0%) | No 22 (78.6%) | 0.028 |
| Yes 45 (75%) | Yes 29 (43.9%) | Yes 13 (50.0%) | Yes 6 (21.4%) | |||
| Bronchial abnormality sign | No 34 (56.7%) | No 32 (48.5%) | 0.358 | No 22 (84.6%) | No 24 (85.7%) | 0.91 |
| Yes 26 (43.3%) | Yes 34 (51.5%) | Yes 4 (15.4%) | Yes 4 (14.3%) | |||
| Vascular abnormality sign | No 20 (33.3%) | No 35 (53.0%) | 0.026 | No 6 (23.1%) | No 18 (64.3%) | 0.002 |
| Yes 40 (66.7%) | Yes 31 (47.0%) | Yes 20 (76.9%) | Yes 10 (35.7%) | |||
| Nodule type | 0.569 | 0.191 | ||||
| GGO | 5 (8.3%) | 9 (13.6%) | 3 (11.5%) | 7 (25.0%) | ||
| CTR < 50% | 10 (16.7%) | 8 (12.1%) | 3 (11.5%) | 4 (14.3%) | ||
| CTR > 50% | 10 (16.7%) | 15 (22.7%) | 5 (19.3%) | 9 (32.1%) | ||
| Solid | 35 (58.3%) | 34 (51.5%) | 15 (57.7%) | 8 (28.6%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xie, X.; Chen, L.; Li, K.; Shi, L.; Zhang, L.; Zheng, L. A Clinical–Radiomics Nomogram for the Preoperative Prediction of Aggressive Micropapillary and a Solid Pattern in Lung Adenocarcinoma. Curr. Oncol. 2025, 32, 323. https://doi.org/10.3390/curroncol32060323
Xie X, Chen L, Li K, Shi L, Zhang L, Zheng L. A Clinical–Radiomics Nomogram for the Preoperative Prediction of Aggressive Micropapillary and a Solid Pattern in Lung Adenocarcinoma. Current Oncology. 2025; 32(6):323. https://doi.org/10.3390/curroncol32060323
Chicago/Turabian StyleXie, Xiangyu, Lei Chen, Kun Li, Liang Shi, Lei Zhang, and Liang Zheng. 2025. "A Clinical–Radiomics Nomogram for the Preoperative Prediction of Aggressive Micropapillary and a Solid Pattern in Lung Adenocarcinoma" Current Oncology 32, no. 6: 323. https://doi.org/10.3390/curroncol32060323
APA StyleXie, X., Chen, L., Li, K., Shi, L., Zhang, L., & Zheng, L. (2025). A Clinical–Radiomics Nomogram for the Preoperative Prediction of Aggressive Micropapillary and a Solid Pattern in Lung Adenocarcinoma. Current Oncology, 32(6), 323. https://doi.org/10.3390/curroncol32060323