Primary Central Nervous System Tumors in Adolescents: A Population-Based Study on Epidemiology and Clinical Pathways in a Challenging Age Group

 , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Statistical Analysis
3. Results
3.1. Incidence: Newly Diagnosed Primary CNS Tumors in Adolescents, 2008–2020
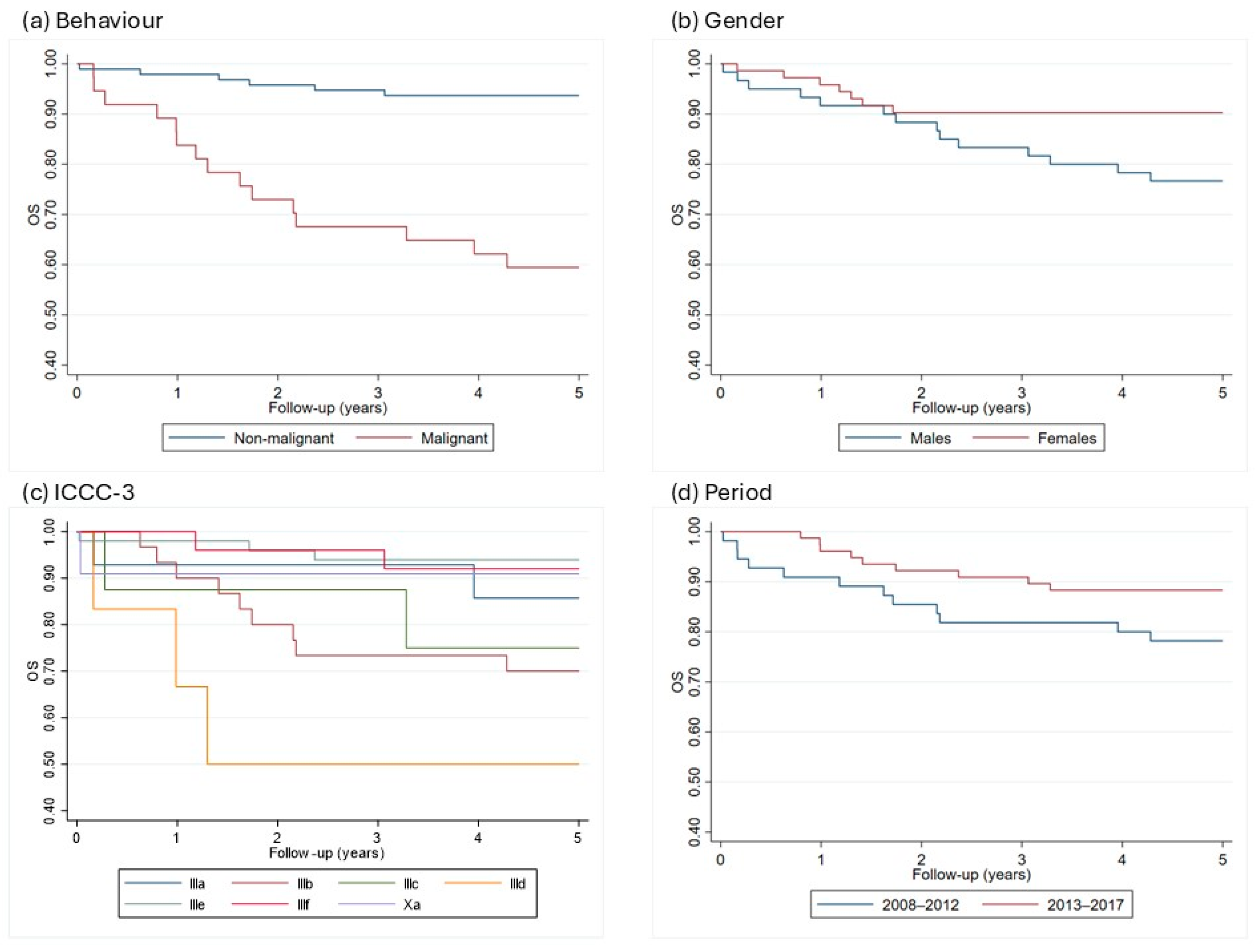
3.2. Survival: From Diagnosis to 5 Years in Adolescents, 2008–2017
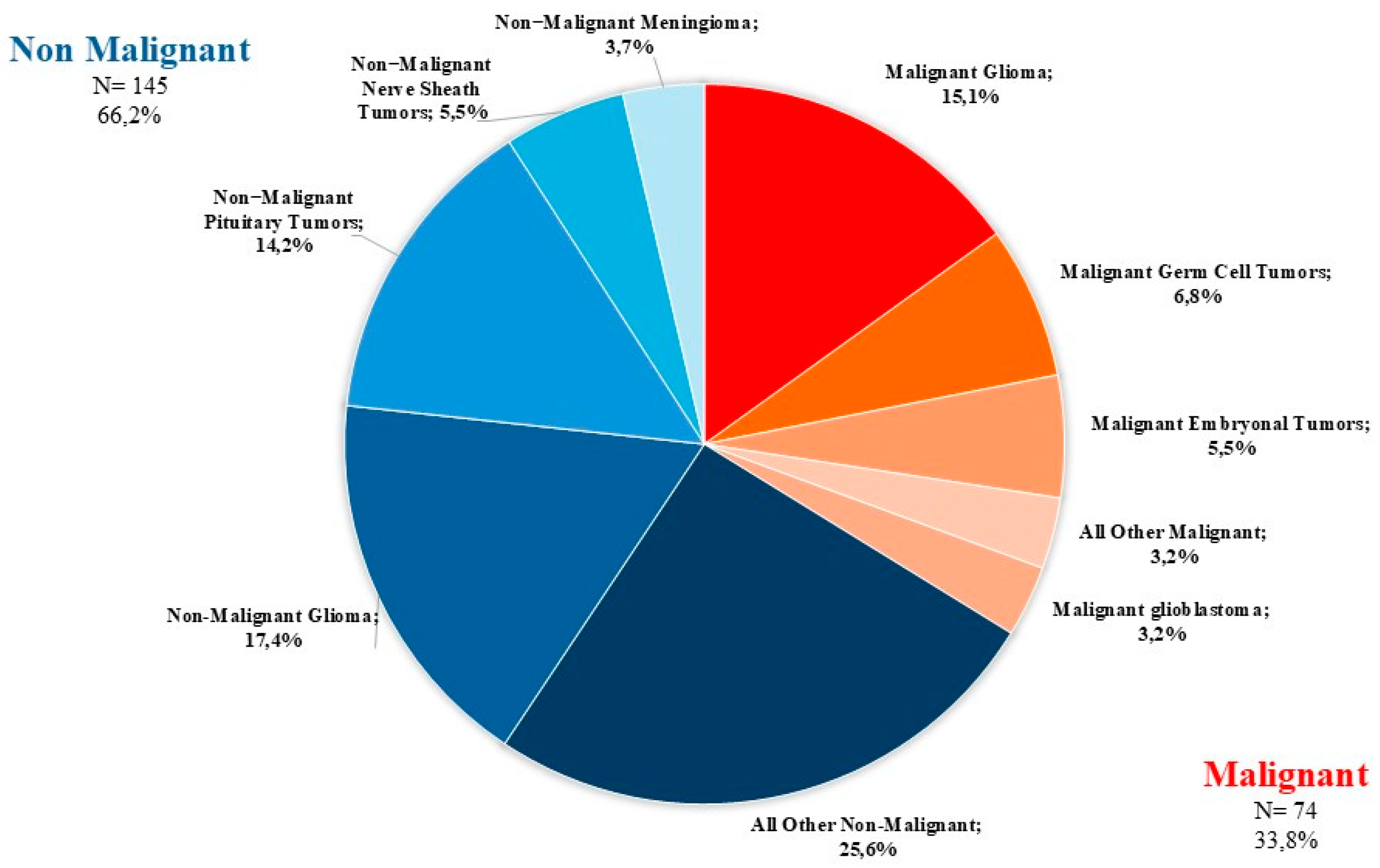
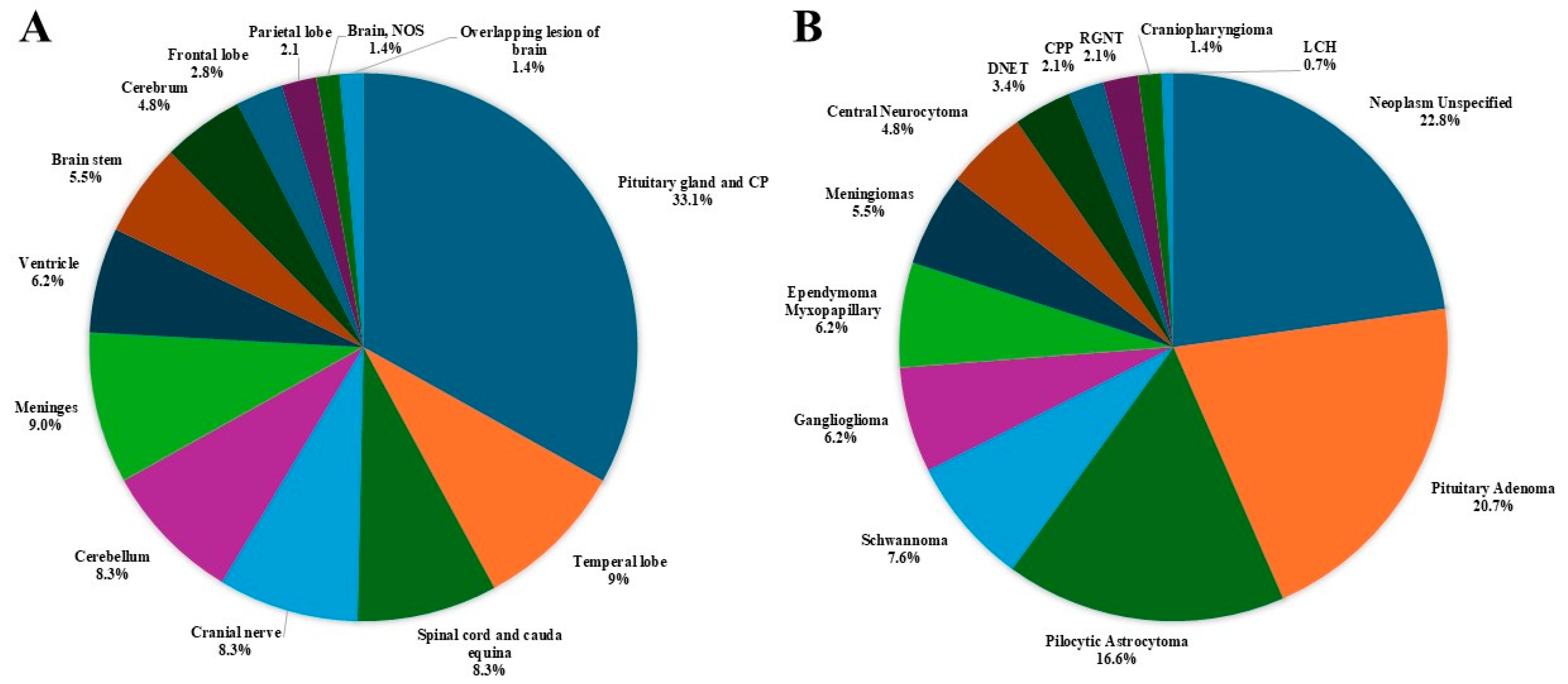
3.3. Distributions of Tumors by Behavior, Site and Histology
- The most common tumor site was the pituitary gland and craniopharyngeal duct, representing 22.4% of all tumors.
- Frontal (4.6%), temporal (7.3%), and parietal (4.6%) lobes combined represented 16.5% of all tumors.
- The cerebellum accounted for 12.3% of all tumors.
- The most frequently reported histology overall was non-malignant pituitary tumors (13.7%), followed by pilocytic astrocytoma (11%) and ependymal tumors (7.3%).
- For malignant tumors, parietal (9.5%), frontal (8.1%), temporal (4.1%) lobes accounted for 21.7% of cases (Figure 4).
- The most common malignant CNS tumors were germ cell tumors (20.3%), followed by embryonal tumors (16.2%). Among embryonal tumors, medulloblastoma and atypical teratoid rhabdoid tumor (ATRT) accounted for 91.7% and 8.3%, respectively.
- For non-malignant tumors, 33.1% were located in the pituitary gland and craniopharyngeal duct (CP).
- The most common histology among non-malignant tumors was pituitary adenoma (20.7%), followed by pilocytic astrocytoma (16.6%).
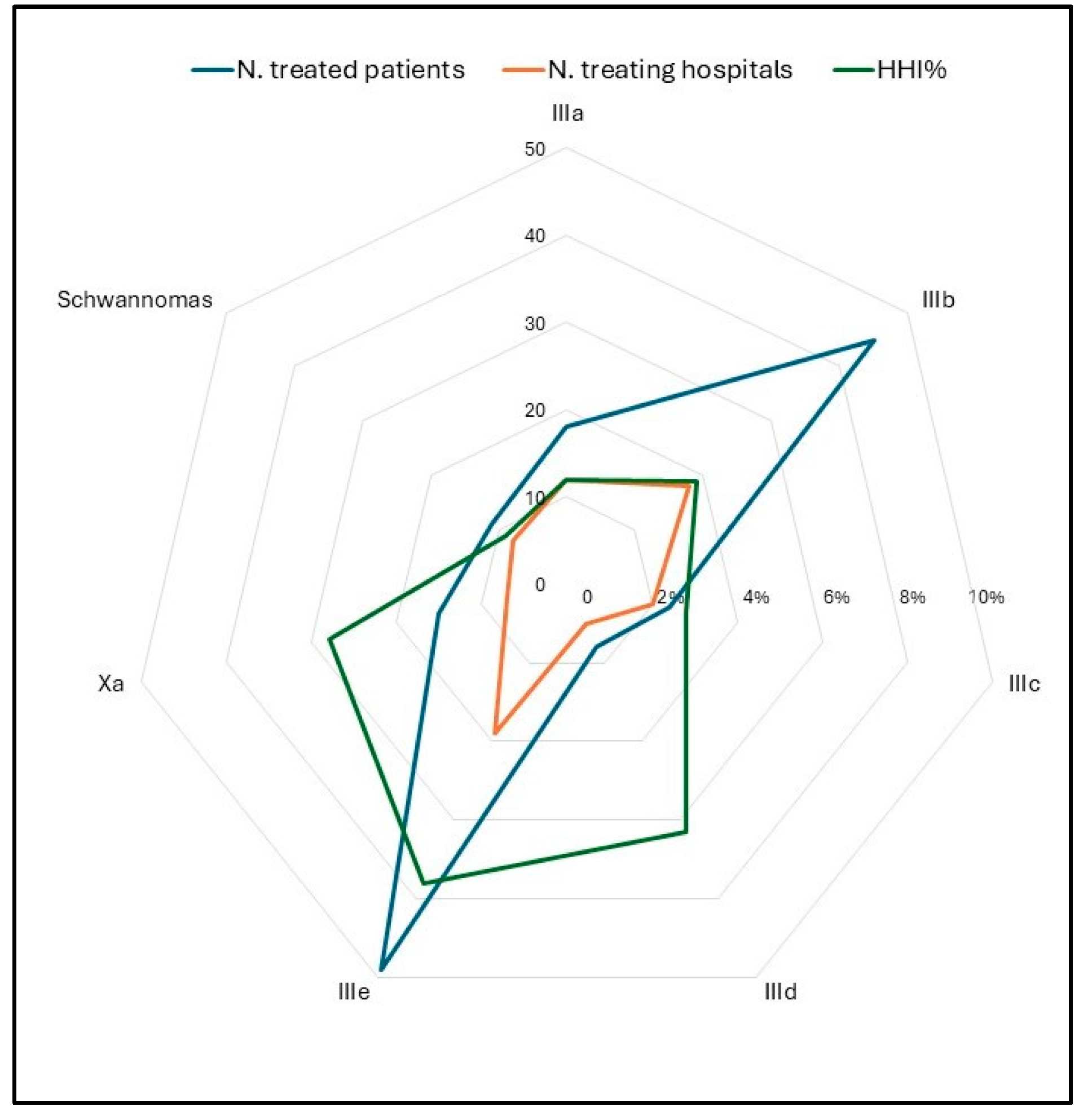
3.4. Pathway of Care
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CCRC | Childhood Cancer Registry of Campania |
| CNS | Central nervous system |
| AYAs | Adolescents and young adults |
| AIEOP | Associazione Italiana Ematologia Oncologia Pediatrica |
| ICD-O | Classification of Diseases for Oncology |
| ICCC | Classification of Childhood Cancer |
| WHO | World Health Organization |
| OS | Observed survival |
| IR | Incident rate |
| CPP | Choroid plexus papilloma |
| ESMO | European Society for Medical Oncology |
| SIOPE | European Society for Pediatric Oncology |
References
- Price, M.; Neff, C.; Nagarajan, N.; Kruchko, C.; Waite, K.A.; Cioffi, G.; Cordeiro, B.B.; Willmarth, N.; Penas-Prado, M.; Gilbert, M.R.; et al. CBTRUS Statistical Report: American Brain Tumor Association & NCI Neuro-Oncology Branch Adolescent and Young Adult Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2016–2020. Neuro Oncol. 2024, 26, iii1–iii53. [Google Scholar] [CrossRef] [PubMed]
- Trama, A.; Botta, L.; Stiller, C.; Visser, O.; Cañete-Nieto, A.; Spycher, B.; Bielska-Lasota, M.; Katalinic, A.; Vener, C.; Innos, K.; et al. Survival of European adolescents and young adults diagnosed with cancer in 2010–2014. Eur. J. Cancer 2024, 202, 113558. [Google Scholar] [CrossRef] [PubMed]
- AIRTUM Working Group. I Tumori in Italia—Rapporto 2012. I tumori dei bambini e degli adolescenti. Epidemiol. Prev. 2013, 37, 1–296. Available online: https://www.registri-tumori.it/cms/pubblicazioni/i-tumori-italia-rapporto-2012-i-tumori-dei-bambini-e-degli-adolescenti (accessed on 31 March 2025).
- Ostrom, Q.T.; Gittleman, H.; Xu, J.; Kromer, C.; Wolinsky, Y.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2009–2013. Neuro Oncol. 2016, 18, v1–v75. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A.; Stark, D.; Peccatori, F.A.; Fern, L.; Laurence, V.; Gaspar, N.; Bozovic-Spasojevic, I.; Smith, O.; De Munter, J.; Derwich, K.; et al. Adolescents and young adults (AYA) with cancer: A position paper from the AYA Working Group of the European Society for Medical Oncology (ESMO) and the European Society for Paediatric Oncology (SIOPE). ESMO Open 2021, 6, 100096. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A.; Rondelli, R.; Pession, A.; Mascarin, M.; Buzzoni, C.; Mosso, M.L.; Maule, M.; Barisone, E.; Bertolotti, M.; Clerici, C.A.; et al. Adolescents with Cancer in Italy: Improving Access to National Cooperative Pediatric Oncology Group (AIEOP) Centers. Pediatr. Blood Cancer 2016, 63, 1116–1119. [Google Scholar] [CrossRef] [PubMed]
- Fritz, A.G. International Classification of Diseases for Oncology, 3rd ed.; Percy, C.J.A., Shanmugartnam, K., Sobin, L., Parkin, D.M., Eds.; 1st Revision; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Fritz, A.G. International Classification of Diseases for Oncology, 3rd ed.; Percy, C.J.A., Sobin, L., Parkin, D.M., Whelan, S., Eds.; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Louis, D.N.; Ohgaki, H.; Wiestler, O.D.; Cavenee, W.K.; Burger, P.C.; Jouvet, A.; Scheithauer, B.W.; Kleihues, P. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 2007, 114, 97–109. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed]
- Steliarova-Foucher, E.; Fidler, M.M.; Colombet, M.; Lacour, B.; Kaatsch, P.; Piñeros, M.; Soerjomataram, I.; Bray, F.; Coebergh, J.W.; Peris-Bonet, R.; et al. Changing geographical patterns and trends in cancer incidence in children and adolescents in Europe, 1991–2010 (Automated Childhood Cancer Information System): A population-based study. Lancet Oncol. 2018, 19, 1159–1169. [Google Scholar] [CrossRef] [PubMed]
- Zapotocky, M.; Ramaswamy, V.; Lassaletta, A.; Bouffet, E. Adolescents and young adults with brain tumors in the context of molecular advances in neuro-oncology. Pediatr. Blood Cancer 2018, 65, e26861. [Google Scholar] [CrossRef] [PubMed]
- Botta, L.; Gatta, G.; Capocaccia, R.; Stiller, C.; Cañete, A.; Dal Maso, L.; Innos, K.; Mihor, A.; Erdmann, F.; Spix, C.; et al. Long-term survival and cure fraction estimates for childhood cancer in Europe (EUROCARE-6): Results from a population-based study. Lancet Oncol. 2022, 23, 1525–1536. [Google Scholar] [CrossRef] [PubMed]
- Bleyer, A.; Budd, T.; Montello, M. Adolescents and young adults with cancer: The scope of the problem and criticality of clinical trials. Cancer 2006, 107, 1645–1655. [Google Scholar] [CrossRef] [PubMed]
- Bleyer, A.; Ferrari, A.; Whelan, J.; Barr, R.D. Global assessment of cancer incidence and survival in adolescents and young adults. Pediatr. Blood Cancer 2017, 64, e26497. [Google Scholar] [CrossRef] [PubMed]
- Lim-Fat, M.J.; Bennett, J.; Ostrom, Q.; Touat, M.; Franceschi, E.; Schulte, J.; Bindra, R.S.; Fangusaro, J.; Dhall, G.; Nicholson, J.; et al. Central nervous system tumors in adolescents and young adults: A Society for Neuro-Oncology Consensus Review on diagnosis, management, and future directions. Neuro Oncol. 2025, 27, 13–32. [Google Scholar] [CrossRef] [PubMed]
- Agha, L.; Frandsen, B.; Rebitzer, J.B. Fragmented division of labor and healthcare costs: Evidence from moves across regions. J. Public Econ. 2019, 169, 144–159. [Google Scholar] [CrossRef]
- Ferrari, A.; Quarello, P.; Mascarin, M.; Milano, G.M.; Tornesello, A.; Bertolotti, M.; Spinelli, M.; Ballotta, P.; Read Borghi, M.; Maule, M.; et al. Evolving Services for Adolescents with Cancer in Italy: Access to Pediatric Oncology Centers and Dedicated Projects. J. Adolesc. Young Adult Oncol. 2020, 9, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Howell, D.L.; Ward, K.C.; Austin, H.D.; Young, J.L.; Woods, W.G. Access to pediatric cancer care by age, race, and diagnosis, and outcomes of cancer treatment in pediatric and adolescent patients in the state of Georgia. J. Clin. Oncol. 2007, 25, 4610–4615. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Presidente del Consiglio dei Ministri. Decreto del Presidente del Consiglio dei Ministri, 3/3/2017,41 Identificazione dei Sistemi di Sorveglianza e dei Registri di Mortalità, di Tumori e di Altre Patologie. Available online: https://www.gazzettaufficiale.it/eli/id/2017/05/12/17A03142/sg (accessed on 20 December 2024).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n = 55 (25.1%) | Neuroimaging (n, %) | Specific Tumor Markers (n, %) |
|---|---|---|
| Non-malignant neoplasm (80,000, 80,001) | 33 (100%) | 0 |
| Malignant neoplasm (80,003) | 3 (100%) | 0 |
| Pituitary adenoma (82,710, 82,720) | 5 (33.3%) | 10 (66.7%) |
| Malignant glioma (93,803) | 3 (100%) | 0 |
| Subependymal giant cell astrocytoma (93,841) | 1 (100%) | 0 |
| Intracranial and Intraspinal Tumors International Classification of Childhood Cancer—3rd ed | ICD-O-3a Histology Code | Sex (M/F) | N° of Newly Diagnosed Tumors | % | WHO Grade | Histologically Confirmed (%) | Incidence Rate ** | |
|---|---|---|---|---|---|---|---|---|
| IIIa Ependymoma and choroid plexus tumor | 13/6 | 19 | 10.1 | 100 | 4.2 | |||
| Myxopapillary ependymoma * | 9394/1 | 5/3 | 8 | 4.3 | I | 100 | 1.8 | |
| Choroid plexus papilloma * | 9390/0 | 2/1 | 3 | 1.6 | I | 100 | 0.7 | |
| Ependymoma, other and NOS | 9391/3, 9392/3 | 6/2 | 8 | 4.3 | II | 100 | 1.8 | |
| IIIb Astrocytomas | 27/19 | 46 | 24.5 | 100 | 10.3 | |||
| Pilocytic astrocytoma * | 9421/1 | 14/10 | 24 | 12.8 | I | 100 | 5.4 | |
| Pilomyxoid astrocytoma | 9425/3 | 1/1 | 2 | 1.1 | I | 100 | 0.4 | |
| Fibrillary astrocytoma | 9420/3 | 1/0 | 1 | 0.5 | II | 100 | 0.2 | |
| Anaplastic astrocytoma | 9401/3 | 1/0 | 1 | 0.5 | III | 100 | 0.2 | |
| Subependymal astrocytoma * | 9384/1 | 0/1 | 1 | 0.5 | 0 | 0.2 | ||
| Pleomorphic xanthoastrocytoma | 9424/3 | 0/1 | 1 | 0.5 | 100 | 0.2 | ||
| Glioblastoma and variants | 9440/39,441/3 | 6/2 | 8 | 4.3 | IV | 100 | 1.8 | |
| Astrocytomas, NOS | 9400/3 | 4/4 | 8 | 4.3 | 100 | 1.8 | ||
| IIIc Intracranial and intraspinal embryonal tumor | 8/5 | 12 | 6.4 | 100 | 2.7 | |||
| Medulloblastoma, variants | 9470/3, 9474/3 | 6/2 | 8 | 4.3 | IV | 100 | 1.8 | |
| Desmoplastic/nodular medulloblastoma | 1/2 | 3 | 1.6 | IV | 100 | 0.7 | ||
| Atypical teratoid/rhabdoid tumor | 9508/3 | 1/0 | 1 | 0.5 | IV | 100 | 0.2 | |
| IIId Other gliomas | 2/9 | 11 | 5.9 | 73 | 2.5 | |||
| Oligodendroglioma | 9450/3 | 0/1 | 1 | 0.5 | II | 100 | 0.2 | |
| Astroblastoma | 9430/3 | 0/1 | 1 | 0.5 | 100 | 0.2 | ||
| Glioma NOS (excl.optic nerve) | 9380/3, 9385/3 | 2/7 | 9 | 4.8 | 56 | 2.0 | ||
| IIIe Other specified CNS tumors | 23/41 | 64 | 34.0 | 77 | 14.3 | |||
| Dysembryoplastic neuroepithelial tumor * | 9413/0 | 2/3 | 5 | 2.7 | I | 100 | 1.1 | |
| Gangliocytomas, ganglioglioma * | 9505/1 | 4/5 | 9 | 4.8 | I | 100 | 2.0 | |
| Meningioma, non-malignant * | 9531/0, 9532/0, 9533/0, 9537/0, 9538/1, 9539/1 | 7/1 | 8 | 4.3 | I | 100 | 1.8 | |
| Craniopharyngioma * | 9351/1 | 2/0 | 2 | 1.1 | I | 100 | 0.4 | |
| Central neurocytoma * | 9506/1 | 1/6 | 7 | 3.7 | II | 100 | 1.6 | |
| Papillary glioneuronal tumor * | 9509/1 | 0/3 | 3 | 1.6 | I | 100 | 0.7 | |
| Pituitary tumors * | 8270/0, 8271/0 | 7/23 | 30 | 16.0 | - | 50 | 6.7 | |
| IIIf Other specified CNS tumors | 14/22 | 36 | 19.1 | 0 | 8.0 | |||
| Malignant | 8000/3 | 1/2 | 3 | 1.6 | - | 0 | 0.7 | |
| Non-malignant * | 8000/0, 1 | 13/20 | 33 | 17.6 | - | 0 | 7.4 | |
| Total malignant CNS tumors | 29/26 | 55 | 29.3 | 89 | 12.3 | |||
| Total malignant & non-malignant CNS tumors | 87/101 | 188 | 71 | 42.0 | ||||
| Other intracranial and intraspinal tumors | ||||||||
| II Lymphomas and others reticuloendothelial cell tumors | 3/0 | 3 | 9.7 | 100 | 0.7 | |||
| Malignant lymphoma, large B-cell, diffuse, NOS | 9680/3 | |||||||
| Malignant lymphoma, large B-cell, diffuse, immunoblastic, NOS | 9683/3 | |||||||
| Langerhans cell histiocytosis * | 9751/1 | |||||||
| IXb Fibrosarcomas, peripheral nerve sheath tumors | 1/0 | 1 | 3.2 | 100 | 0.2 | |||
| Nerve sheath tumors | 9540/3 | 1/0 | 1 | 3.2 | 100 | 0.2 | ||
| Xa Intracranial and intraspinal germ cell tumors | 15/0 | 15 | 48.4 | 100 | 3.3 | |||
| Dysgerminoma | 9060/3 | 1/0 | 1 | 3.2 | 100 | 0.2 | ||
| Germinoma | 9064/3 | 12/0 | 12 | 38.7 | 100 | 2.7 | ||
| Mixed germ cell tumors | 9085/3 | 2/0 | 2 | 6.5 | 100 | 0.4 | ||
| XId Melanomas | 1/0 | 1 | 3.2 | 100 | 0.2 | |||
| Meningeal melanomatosis | 8720/3 | 1/0 | 3.2 | 100 | 0.2 | |||
| No ICCC coded | 5/7 | 11 | 35.5 | 100 | 2.5 | |||
| Schwannomas * | 9560/0 | 4/7 | 11 | 35.5 | 100 | 2.5 | ||
| Total other intracranial and intraspinal tumors | 24/7 | 31 | 100 | 6.9 | ||||
| 5-Year Survival | Equality of Survivor Functions | ||||
|---|---|---|---|---|---|
| OS% | 95% CI | Log-Rank Test (p Value) | |||
| Sex | |||||
| Males | 76.7 | 63.8 | 85.5 | ||
| Females | 90.3 | 80.7 | 95.2 | <0.05 | |
| Behavior | |||||
| Malignant | 59.5 | 42.0 | 73.2 | ||
| Non-malignant | 93.7 | 86.5 | 97.1 | <0.001 | |
| Period | |||||
| 2008–2012 | 78.2 | 64.8 | 87.0 | ||
| 2013–2017 | 88.3 | 78.7 | 93.7 | 0.11 | |
| ICCC-3 | |||||
| IIIa Ependymoma and choroid plexus tumor | 85.7 | 53.9 | 96.2 | ||
| IIIb Astrocytomas | 70.0 | 50.3 | 83.1 | ||
| IIIc Intracranial and intraspinal embryonal tumor | 75.0 | 31.5 | 93.1 | ||
| IIId Other gliomas | 50.0 | 11.1 | 80.4 | ||
| IIIe Other specified CNS tumors | 93.9 | 82.2 | 98.0 | ||
| IIIf Other unspecified CNS tumors | 92.0 | 71.6 | 97.9 | ||
| Xa Intracranial and intraspinal germ cell tumors | 90.9 | 50.8 | 98.7 | ||
| N (%) | Histologically Confirmed | |
|---|---|---|
Adult neurosurgery
| 143 (65.3%) 79 (55.2%) 64 (44.8%) | 133 (93%) 71 (89.9%) 58 (90.6%) |
Pediatric neurosurgery
| 32 (14.6%) 17 (53.1%) 15 (46.9%) | 30 (93.7%) 14 (82.3%) 15 (100%) |
Other medical unit
| 44 (20.1%) 29 (65.9%) 15 (34.1%) | 0 (0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Martino, L.; Piga, P.; Sessa, M.; Calì, C.; Russo, C.; Picariello, S.; Onorini, N.; Spennato, P.; Quaglietta, L.; Donofrio, M.V.; et al. Primary Central Nervous System Tumors in Adolescents: A Population-Based Study on Epidemiology and Clinical Pathways in a Challenging Age Group. Curr. Oncol. 2025, 32, 222. https://doi.org/10.3390/curroncol32040222
De Martino L, Piga P, Sessa M, Calì C, Russo C, Picariello S, Onorini N, Spennato P, Quaglietta L, Donofrio MV, et al. Primary Central Nervous System Tumors in Adolescents: A Population-Based Study on Epidemiology and Clinical Pathways in a Challenging Age Group. Current Oncology. 2025; 32(4):222. https://doi.org/10.3390/curroncol32040222
Chicago/Turabian StyleDe Martino, Lucia, Patrizia Piga, Marcella Sessa, Camilla Calì, Camilla Russo, Stefania Picariello, Nicola Onorini, Pietro Spennato, Lucia Quaglietta, Maria Vittoria Donofrio, and et al. 2025. "Primary Central Nervous System Tumors in Adolescents: A Population-Based Study on Epidemiology and Clinical Pathways in a Challenging Age Group" Current Oncology 32, no. 4: 222. https://doi.org/10.3390/curroncol32040222
APA StyleDe Martino, L., Piga, P., Sessa, M., Calì, C., Russo, C., Picariello, S., Onorini, N., Spennato, P., Quaglietta, L., Donofrio, M. V., Cinalli, G., Vetrano, F., & Savoia, F. (2025). Primary Central Nervous System Tumors in Adolescents: A Population-Based Study on Epidemiology and Clinical Pathways in a Challenging Age Group. Current Oncology, 32(4), 222. https://doi.org/10.3390/curroncol32040222