Real-World Treatment Patterns, Healthcare Resource Utilization, and Healthcare Costs in the First-Line Treatment of Metastatic Non-Small Cell Lung Cancer in the US


Abstract
1. Introduction
2. Materials and Methods
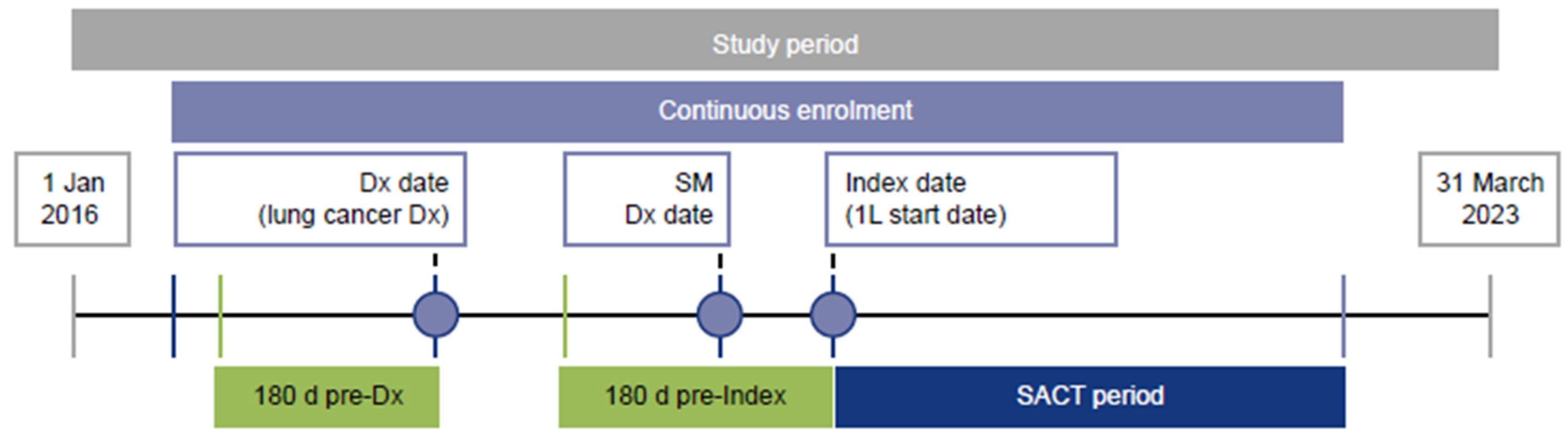
2.1. Study Design and Population
2.2. Treatment Classification
2.3. Baseline Characteristics
2.4. Study Outcomes
2.5. Analysis
3. Results
3.1. Study Population
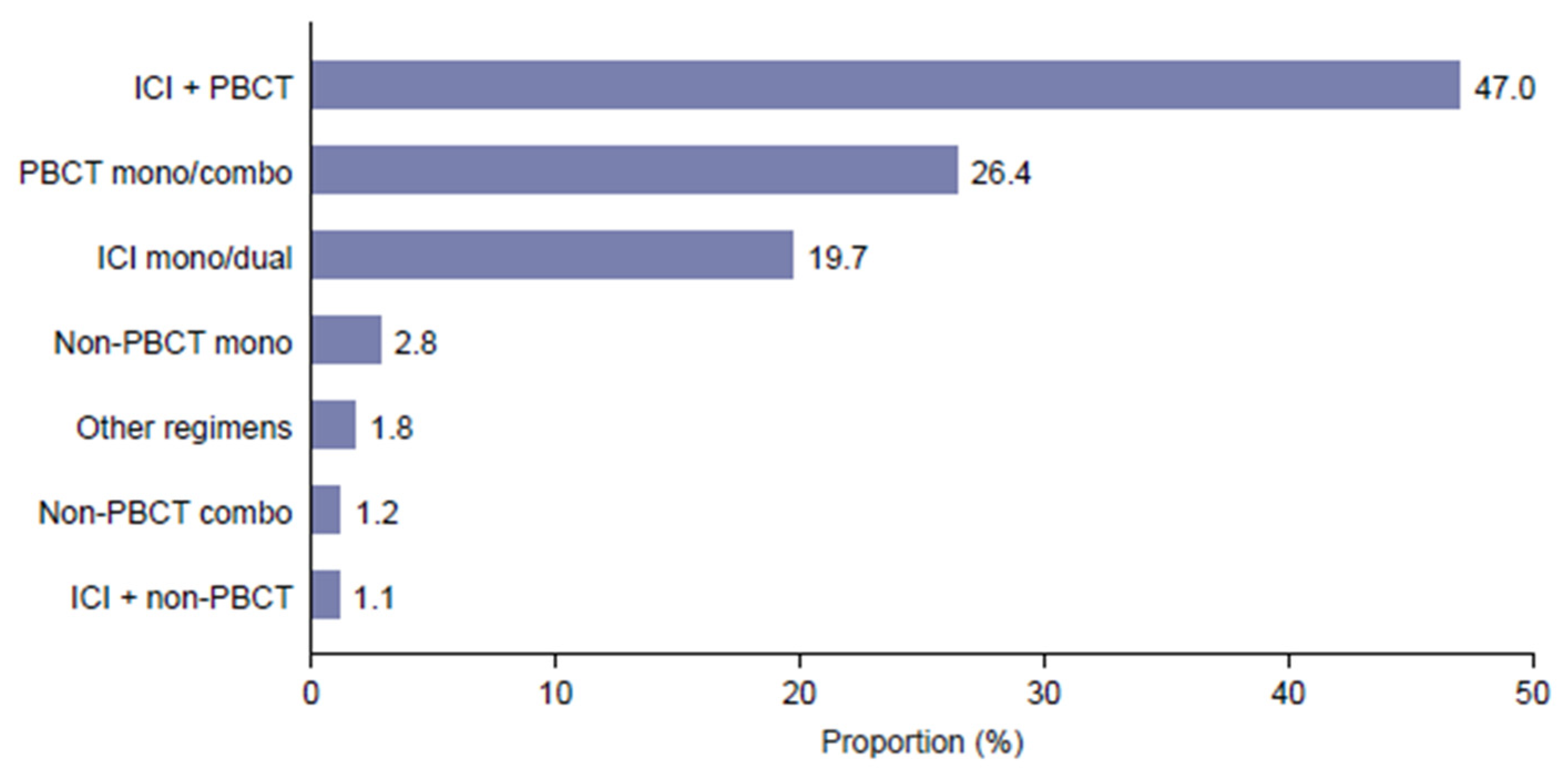
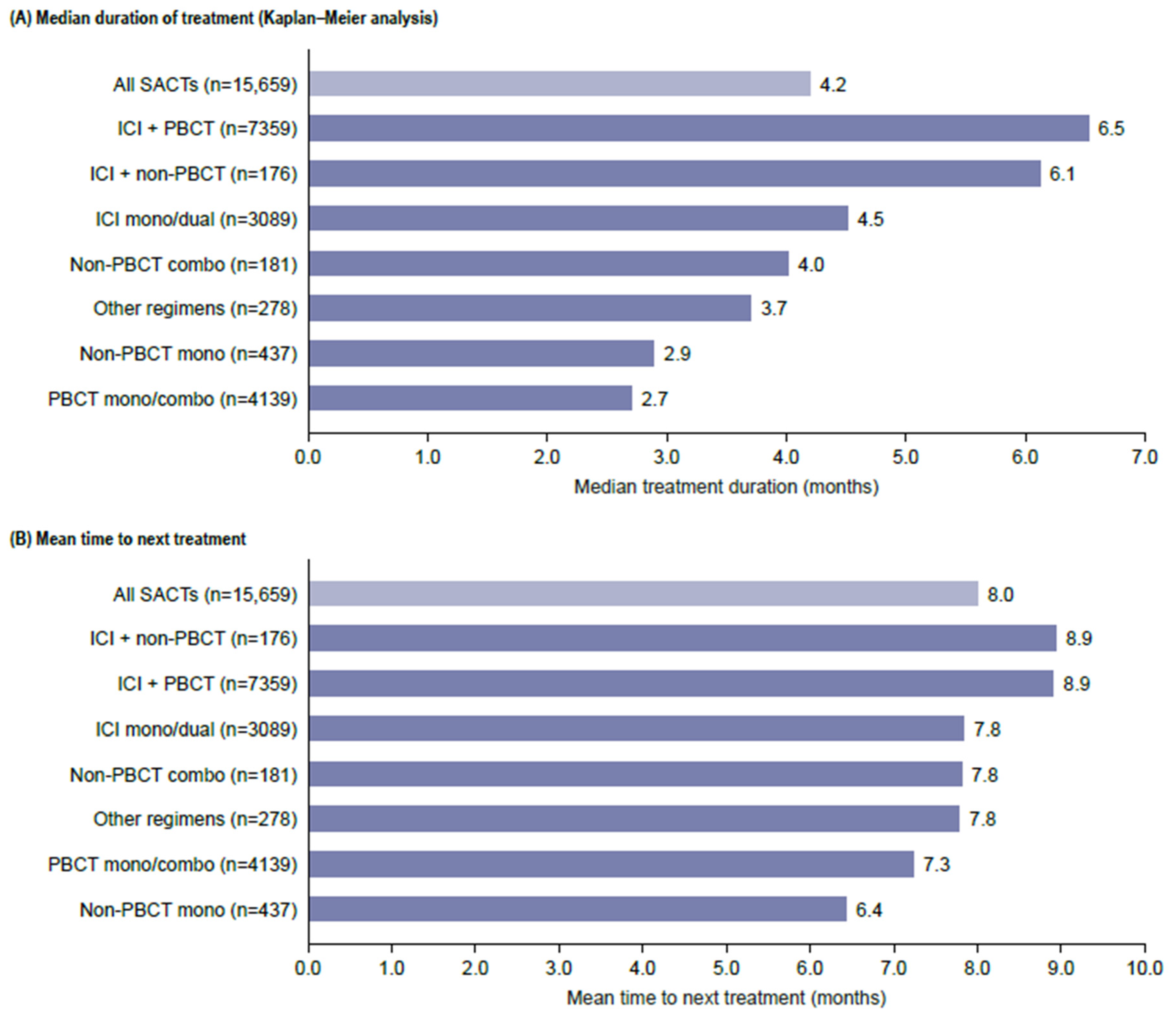
3.2. Treatment Patterns
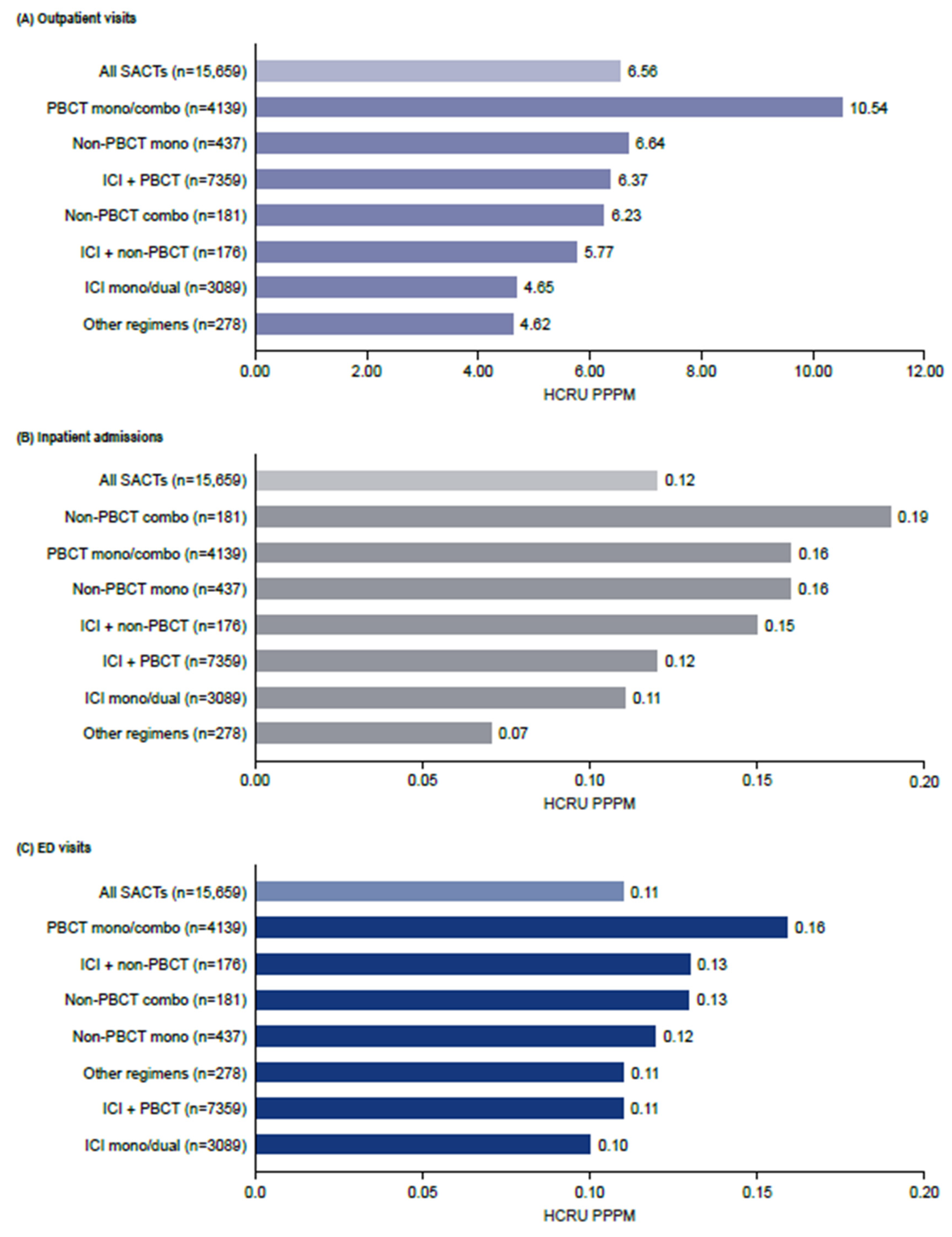
3.3. HCRU
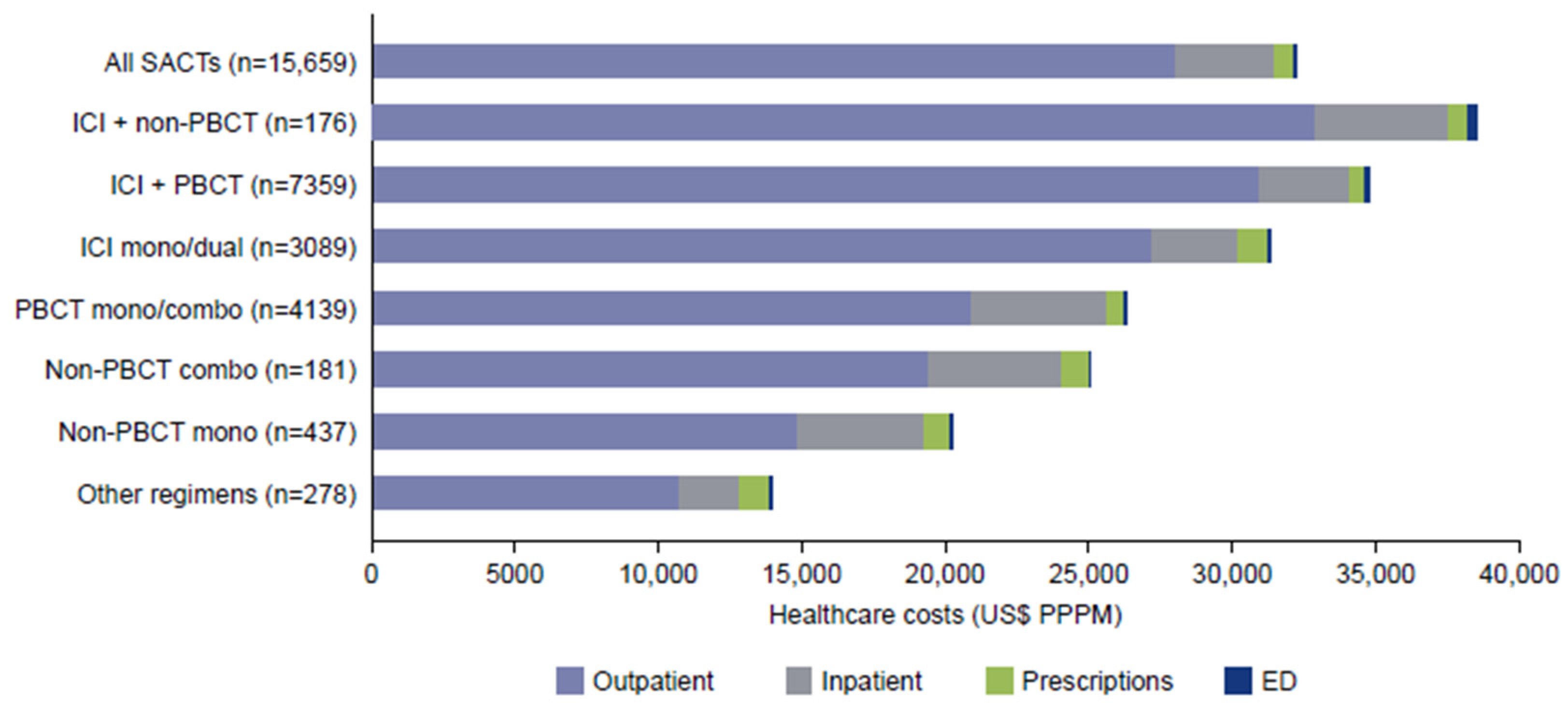
3.4. Healthcare Costs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 1L | first-line |
| 2L | second line |
| COPD | chronic obstructive pulmonary disease |
| ED | emergency department |
| HCRU | healthcare resource utilization |
| ICD-10-CM | The International Classification of Diseases, 10th Edition, Clinical Modification |
| ICI | immune checkpoint inhibitor |
| KRAS | Kirstin rat sarcoma virus |
| NCI-CCI | National Cancer Institute-adapted Charlson Comorbidity Index |
| NCCN | National Comprehensive Cancer Network |
| NSCLC | non-small cell lung cancer |
| PBCT | platinum-based chemotherapy |
| PPPM | per patient per month |
| SACT | systemic anticancer therapy |
| SD | standard deviation |
| STROBE | Strengthening the Reporting of Observational Studies in Epidemiology |
| TTNT | time to the next treatment |
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Key Statistics for Lung Cancer. Available online: https://www.cancer.org/cancer/types/lung-cancer/about/key-statistics.html (accessed on 6 June 2024).
- Araghi, M.; Mannani, R.; Heidarnejad Maleki, A.; Hamidi, A.; Rostami, S.; Safa, S.H.; Faramarzi, F.; Khorasani, S.; Alimohammadi, M.; Tahmasebi, S.; et al. Recent advances in non-small cell lung cancer targeted therapy; an update review. Cancer Cell Int. 2023, 23, 162. [Google Scholar] [CrossRef] [PubMed]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V.; et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 2016, 11, 39–51. [Google Scholar] [CrossRef]
- Duma, N.; Santana-Davila, R.; Molina, J.R. Non-Small Cell Lung Cancer: Epidemiology, Screening, Diagnosis, and Treatment. Mayo Clin. Proc. 2019, 94, 1623–1640. [Google Scholar] [CrossRef]
- Chouaid, C.; Giannopoulou, A.; Starry, A.; Stollenwerk, B.; Bozorgmehr, F. The impact of KRAS mutational status on patient-reported outcomes in advanced non-small-cell lung cancer: A cross sectional study in France and Germany. J. Med. Econ. 2025, 28, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.-Y.M.; Zheng, M.-M.; Pan, Y.; Liu, S.-Y.; Li, Y.; Wu, Y.-L. Emerging evidence and treatment paradigm of non-small cell lung cancer. J. Hematol. Oncol. 2023, 16, 40. [Google Scholar] [CrossRef]
- Friedlaender, A.; Perol, M.; Banna, G.L.; Parikh, K.; Addeo, A. Oncogenic alterations in advanced NSCLC: A molecular super-highway. Biomark Res. 2024, 12, 24. [Google Scholar] [CrossRef]
- Sathiyapalan, A.; Ellis, P.M. Molecular Testing in Non-Small-Cell Lung Cancer: A Call to Action. JCO Oncol. Pract. 2024, 20, 7–9. [Google Scholar] [CrossRef]
- de Langen, A.J.; Johnson, M.L.; Mazieres, J.; Dingemans, A.C.; Mountzios, G.; Pless, M.; Wolf, J.; Schuler, M.; Lena, H.; Skoulidis, F.; et al. Sotorasib versus docetaxel for previously treated non-small-cell lung cancer with KRAS (G12C) mutation: A randomised, open-label, phase 3 trial. Lancet 2023, 401, 733–746. [Google Scholar] [CrossRef]
- Waterhouse, D.M.; Rothschild, S.; Dooms, C.; Mennecier, B.; Bozorgmehr, F.; Majem, M.; van den Heuvel, M.H.; Linardou, H.; Chul Cho, B.; Roberts-Thomson, R.; et al. Patient-reported outcomes in CodeBreaK 200: Sotorasib versus docetaxel for previously treated advanced NSCLC with KRAS G12C mutation. Lung Cancer 2024, 196, 107921. [Google Scholar] [CrossRef]
- Kim, S.Y.; Halmos, B. Choosing the best first-line therapy: NSCLC with no actionable oncogenic driver. Lung Cancer Manag. 2020, 9, Lmt36. [Google Scholar] [CrossRef]
- NCCN. NCCN Clinical Practice Guidelines in Oncology Non-Small Cell Lung Cancer Version 11.2024—15 October 2024; NCCN: Plymouth Meeting, PA, USA, 2024. [Google Scholar]
- Gandhi, L.; Rodriguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef] [PubMed]
- DaCosta Byfield, S.; Chastek, B.; Korrer, S.; Horstman, T.; Malin, J.; Newcomer, L. Real-world outcomes and value of first-line therapy for metastatic non-small cell lung cancer. Cancer Investig. 2020, 38, 608–617. [Google Scholar] [CrossRef] [PubMed]
- Arunachalam, A.; Li, H.; Bittoni, M.A.; Camacho, R.; Cao, X.; Zhong, Y.; Lubiniecki, G.M.; Carbone, D.P. Real-World Treatment Patterns, Overall Survival, and Occurrence and Costs of Adverse Events Associated with Second-Line Therapies for Medicare Patients with Advanced Non-Small-Cell Lung Cancer. Clin. Lung Cancer 2018, 19, e783–e799. [Google Scholar] [CrossRef]
- Nadler, E.; Espirito, J.L.; Pavilack, M.; Boyd, M.; Vergara-Silva, A.; Fernandes, A. Treatment Patterns and Clinical Outcomes Among Metastatic Non-Small-Cell Lung Cancer Patients Treated in the Community Practice Setting. Clin. Lung Cancer 2018, 19, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.D.; Allo, M.A.; Gu, L.; Vashistha, V.; Press, A.; Kelley, M. Health outcomes and healthcare resource utilization among Veterans with stage IV non-small cell lung cancer treated with second-line chemotherapy versus immunotherapy. PLoS ONE 2023, 18, e0282020. [Google Scholar] [CrossRef]
- Zhang, X.; Beachler, D.C.; Masters, E.; Liu, F.; Yang, M.; Dinh, J.; Jamal-Allial, A.; Kolitsopoulos, F.; Lamy, F.X. Health care resource utilization and costs associated with advanced or metastatic nonsmall cell lung cancer in the United States. J. Manag. Care Spec. Pharm. 2022, 28, 255–265. [Google Scholar] [CrossRef]
- Simmons, D.; Welch, E.; Pyrih, N.; Jiang, Z.; Xiao, Y.; Jassim, R. EE270 The Economic Burden of Metastatic Non-Small Cell Lung Cancer in US Patients without an EGFR or ALK Mutation. Value Health 2023, 26, S108. [Google Scholar] [CrossRef]
- Vanderpoel, J.; Emond, B.; Ghelerter, I.; Milbers, K.; Lafeuille, M.H.; Lefebvre, P.; Ellis, L.A. Healthcare Resource Utilization and Costs in Patients with EGFR-Mutated Advanced Non-Small Cell Lung Cancer Receiving First-Line Treatment in the United States: An Insurance Claims-Based Descriptive Analysis. PharmacoEcon. Open 2023, 7, 617–626. [Google Scholar] [CrossRef]
- Chopra, D.; Waterhouse, D.; Sultan, I.; Lonshteyn, A.; Weycker, D.; Delea, T. Real-world treatment patterns, health care costs and health care utilization in US patients with non–small cell lung cancer receiving sotorasib. J. Manag. Care Spec. Pharm. 2023, 29, S16. [Google Scholar]
- Meng, W.; Ou, W.; Chandwani, S.; Chen, X.; Black, W.; Cai, Z. Temporal phenotyping by mining healthcare data to derive lines of therapy for cancer. J. Biomed. Inform. 2019, 100, 103335. [Google Scholar] [CrossRef]
- Klabunde, C.N.; Legler, J.M.; Warren, J.L.; Baldwin, L.M.; Schrag, D. A refined comorbidity measurement algorithm for claims-based studies of breast, prostate, colorectal, and lung cancer patients. Ann. Epidemiol. 2007, 17, 584–590. [Google Scholar] [CrossRef]
- US Bureau of Labor Statistics. CPI for All Urban Consumers (CPI-U), Medical Care in U.S. City Average, All Urban Consumers, Not Seasonally Adjusted; Series ID: CUUR0000SAM; US Bureau of Labor Statistics: Washington, DC, USA, 2023.
- Kish, J.; Liassou, D.; Hartman, J.; Lubinga, S.J.; Chopra, D.; Feinberg, B. Better together? costs of first-line chemoimmunotherapy for advanced non-small cell lung cancer. Am. J. Manag. Care 2023, 29, e129–e135. [Google Scholar] [CrossRef] [PubMed]
- Spira, A.; Knoll, S.; Smith, T.; Scotchmer, A.; Bauer, M. Costs of first-line systemic therapy (1LT) for locally advanced or metastatic non-small cell lung cancer (a/mNSCLC)—A secondary analysis of claims data from the United States (US) (abstract). Value Health 2023, 26, S67. [Google Scholar] [CrossRef]
- Pham, T.T.; Gordon, A.S.; Chen, X.; Debono, D.; Fisch, M.J. Immunotherapy in combination with chemotherapy vs. immunotherapy alone for advanced non-small cell lung cancer and programmed death ligand 1 score < 50. Cancer Treat. Res. Commun. 2023, 37, 100769. [Google Scholar] [CrossRef]
- Gines Rubio, J.; Delgado, O.; Callejo, A.; Dominguez, M.; Torres, C. Healthcare Resource Utilization and Associated Costs among Patients with Advanced Non-Small-Cell Lung Cancer Receiving Chemotherapy or Immunotherapy in Spain: A Single-Center, Real-World, Exploratory Study. Cancers 2024, 16, 2068. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.K.; Wu, Y.L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G., Jr.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Reck, M.; Rodriguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csoszi, T.; Fulop, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef]
- Turner, R.M.; Chen, Y.W.; Fernandes, A.W. Validation of a Case-Finding Algorithm for Identifying Patients with Non-small Cell Lung Cancer (NSCLC) in Administrative Claims Databases. Front. Pharmacol. 2017, 8, 883. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criterion | Number of Patients |
|---|---|
| Diagnosis of lung cancer (Dx date) | 280,355 |
| Diagnosis of secondary malignancy on or after Dx date | 145,915 |
| SACT for NSCLC on or after diagnosis of secondary malignancy | 60,843 |
| ≥1 LOT initiated on or after 1 January 2020 (index date) | 32,820 |
| Continuously enrolled for ≥180 days before diagnosis to ≥30 days after index date | 22,014 |
| No medications are typically administered for SCLC before the index date | 20,368 |
| No claims for targeted treatment during the study period | 19,055 |
| No diagnosis of secondary malignancy or use of SACT within 180 days prior to Dx date | 17,571 |
| Age ≥ 18 years on the index date | 17,571 |
| 1L SACT for NSCLC | 15,659 |
| Characteristics | Value | |
|---|---|---|
| Age, years, mean (SD) | 71.7 (8.6) | |
| Sex, male, % | 51.8 | |
| US census region, % | Northeast | 14.1 |
| Midwest | 26.1 | |
| South | 43.4 | |
| West | 16.2 | |
| Medicare Advantage, % | 85.5 | |
| Index year, % | 2020 | 30.3 |
| 2021 | 30.2 | |
| 2022 | 33.7 | |
| 2023 Q1 | 7.7 | |
| Comorbidities, % | Hypertension | 72.7 |
| COPD | 44.3 | |
| Coronary heart disease | 29.2 | |
| Anemia | 28.8 | |
| Diabetes | 28.5 | |
| Chronic kidney disease | 14.8 | |
| Brain/spinal cord | 14.1 | |
| Chronic liver disease | 12.5 | |
| Dementia | 1.7 | |
| Cerebrovascular disease | 1.1 | |
| Other | 64.2 | |
| NCI-CCI, mean (SD) | 2.3 (1.9) | |
| Secondary metastases, % | Bone | 21.6 |
| Brain/spinal cord | 14.1 | |
| Liver | 11.3 | |
| Other | 64.2 | |
| History of smoking, % a | 79.8 | |
| Time from lung cancer diagnosis, months, median (IQR) | 1.5 (0.9–2.8) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chopra, D.; Waterhouse, D.M.; Sultan, I.; Stollenwerk, B. Real-World Treatment Patterns, Healthcare Resource Utilization, and Healthcare Costs in the First-Line Treatment of Metastatic Non-Small Cell Lung Cancer in the US. Curr. Oncol. 2025, 32, 151. https://doi.org/10.3390/curroncol32030151
Chopra D, Waterhouse DM, Sultan I, Stollenwerk B. Real-World Treatment Patterns, Healthcare Resource Utilization, and Healthcare Costs in the First-Line Treatment of Metastatic Non-Small Cell Lung Cancer in the US. Current Oncology. 2025; 32(3):151. https://doi.org/10.3390/curroncol32030151
Chicago/Turabian StyleChopra, Divyan, David M. Waterhouse, Ihtisham Sultan, and Björn Stollenwerk. 2025. "Real-World Treatment Patterns, Healthcare Resource Utilization, and Healthcare Costs in the First-Line Treatment of Metastatic Non-Small Cell Lung Cancer in the US" Current Oncology 32, no. 3: 151. https://doi.org/10.3390/curroncol32030151
APA StyleChopra, D., Waterhouse, D. M., Sultan, I., & Stollenwerk, B. (2025). Real-World Treatment Patterns, Healthcare Resource Utilization, and Healthcare Costs in the First-Line Treatment of Metastatic Non-Small Cell Lung Cancer in the US. Current Oncology, 32(3), 151. https://doi.org/10.3390/curroncol32030151