Treatment Outcomes in Spinal Tumors According to Patients’ Perspectives: A Focus on Indeterminate Spinal Instability

 , , and
, , and
Abstract
1. Introduction
2. Material and Methods
2.1. Data Collection
2.2. Pain Evaluation
2.3. Inclusion and Exclusion Criteria
2.3.1. Inclusion Criteria
2.3.2. Exclusion Criteria
2.4. Primary Outcome
- Better;
- Equal;
- Worse;
- Never experienced pain/remained pain-free.
2.5. Statistics
3. Results
3.1. Treatment Strategies for the Indeterminate Group
3.2. Outcomes in the Indeterminate Group
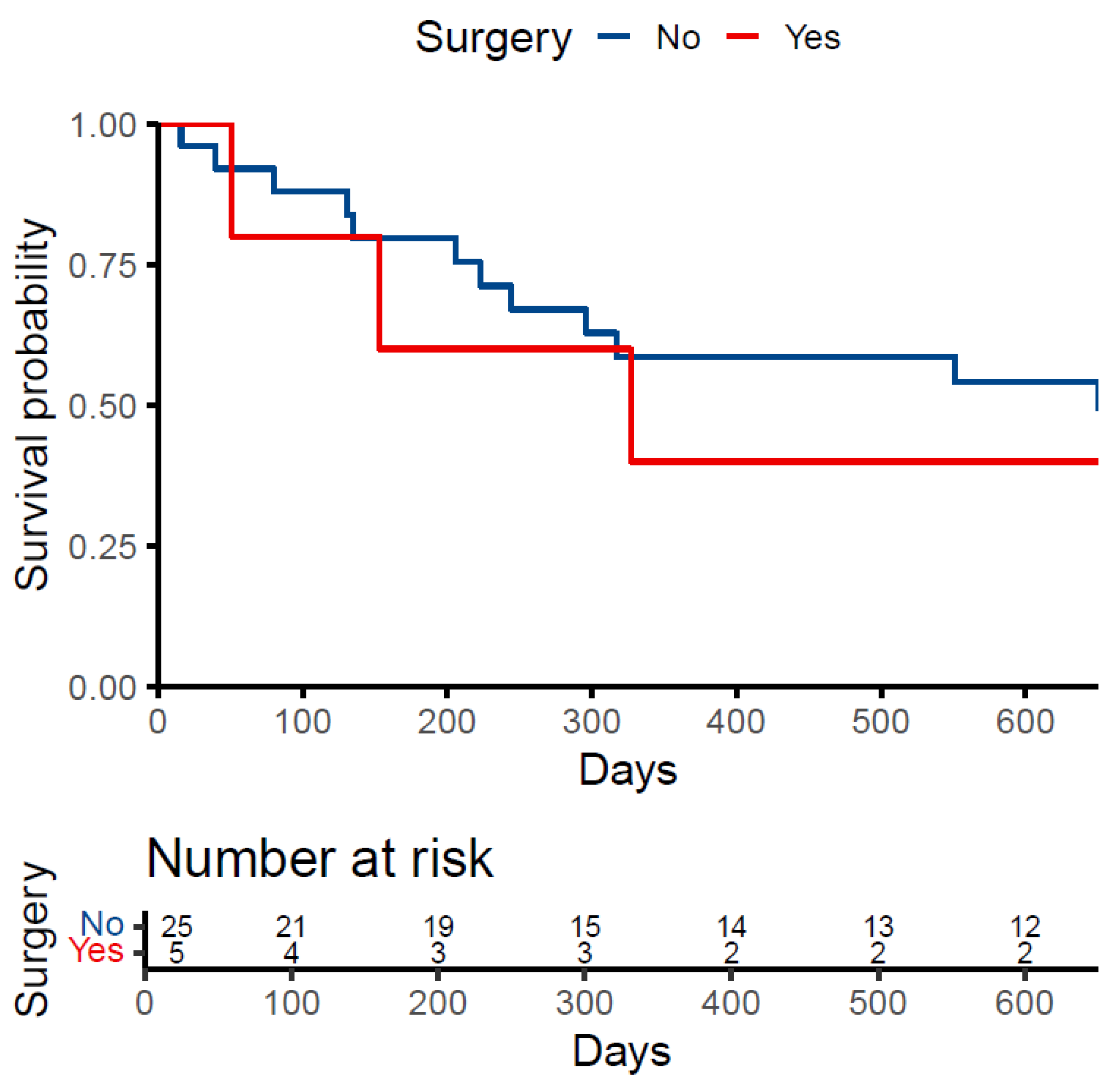
3.3. Patient Survival
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.A.; Fornasier, V.L.; MacNAB, I.A.N. Spinal Metastases The Obvious, the Occult, and the Impostors. Spine 1990, 15, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Van Den Brande, R.; Mj Cornips, E.; Peeters, M.; Ost, P.; Billiet, C.; Van De Kelft, E. Epidemiology of spinal metastases, metastatic epidural spinal cord compression and pathologic vertebral compression fractures in patients with solid tumors: A systematic review. J. Bone Oncol. 2022, 35, 100446. [Google Scholar] [CrossRef] [PubMed]
- Pishnamaz, M.; Quack, V.; Herren, C.; Hildebrand, F.; Kobbe, P. Versorgungsstrategien bei pathologischen Frakturen der Wirbelsäule. Unfallchirurg 2021, 124, 720–730. [Google Scholar] [CrossRef] [PubMed]
- Ly, R.; Terrier, L.M.; Cognacq, G.; Benboubker, L.; Destriex, C.; Velut, S.; Zemmoura, I.; Francois, P.; Aggad, M.; Amelot, A. Spinal lesions in multiple myeloma: Primary bone tumors with distinct prognostic factors. Surg. Oncol. 2023, 48, 101927. [Google Scholar] [CrossRef] [PubMed]
- Milavec, H.; Ravikumar, N.; Syn, N.L.; Yentia Soekojo, C.; Chng, W.J.; Kumar, N. Surgical Management of Multiple Myeloma With Symptomatic Involvement of the Spine. Int. J. Spine Surg. 2020, 14, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Fisher, C.G.; DiPaola, C.P.; Ryken, T.C.; Bilsky, M.H.; Shaffrey, C.I.; Berven, S.H.; Harrop, J.S.; Fehlings, M.G.; Boriani, S.; Chou, D.; et al. A Novel Classification System for Spinal Instability in Neoplastic Disease: An Evidence-Based Approach and Expert Consensus From the Spine Oncology Study Group. Spine 2010, 35, E1221–E1229. [Google Scholar] [CrossRef] [PubMed]
- Laufer, I.; Rubin, D.G.; Lis, E.; Cox, B.W.; Stubblefield, M.D.; Yamada, Y.; Bilsky, M.H. The NOMS Framework: Approach to the Treatment of Spinal Metastatic Tumors. Oncologist 2013, 18, 744–751. [Google Scholar] [CrossRef] [PubMed]
- Milavec, H.; Kellner, C.; Ravikumar, N.; Cristoph, E.A.; Lerch, T.; Hoppe, S.; Deml, M.C.; Bigdon, S.F.; Kumar, N.; Benneker, L.M. First Clinical Experience with a Carbon Fibre Reinforced PEEK Composite Plating System for Anterior Cervical Discectomy and Fusion. J. Funct. Biomater. 2019, 10, 29. [Google Scholar] [CrossRef] [PubMed]
- Pennington, Z.; Ahmed, A.K.; Westbroek, E.M.; Cottrill, E.; Lubelski, D.; Goodwin, M.L.; Sciubba, D.M. SINS Score and Stability: Evaluating the Need for Stabilization Within the Uncertain Category. World Neurosurg. 2019, 128, e1034–e1047. [Google Scholar] [CrossRef] [PubMed]
- Lenschow, M.; Lenz, M.; Von Spreckelsen, N.; Ossmann, J.; Meyer, J.; Keßling, J.; Nadjiri, L.; Telentschak, S.; Zarghooni, K.; Knöll, P.; et al. Impact of Spinal Instrumentation on Neurological Outcome in Patients with Intermediate Spinal Instability Neoplastic Score (SINS). Cancers 2022, 14, 2193. [Google Scholar] [CrossRef] [PubMed]
- Barzilai, O.; Fisher, C.G.; Bilsky, M.H. State of the Art Treatment of Spinal Metastatic Disease. Neurosurgery 2018, 82, 757–769. [Google Scholar] [CrossRef]
- Serratrice, N.; Faddoul, J.; Tarabay, B.; Attieh, C.; Chalah, M.A.; Ayache, S.S.; Abi Lahoud, G.N. Ten Years After SINS: Role of Surgery and Radiotherapy in the Management of Patients With Vertebral Metastases. Front. Oncol. 2022, 12, 802595. [Google Scholar] [CrossRef]
- Vargas, E.; Lockney, D.T.; Mummaneni, P.V.; Haddad, A.F.; Rivera, J.; Tan, X.; Jamieson, A.; Mahmoudieh, Y.; Berven, S.; Braunstein, S.E.; et al. An analysis of tumor-related potential spinal column instability (Spine Instability Neoplastic Scores 7–12) eventually requiring surgery with a 1-year follow-up. Neurosurg. Focus 2021, 50, E6. [Google Scholar] [CrossRef] [PubMed]
- Mahakul, D.J.; Visen, A.; Agarwal, J. The Truly Intermediate Subgroup Within the SINS “Potentially Unstable” Category: The Matryoshka Doll Phenomenon. World Neurosurg. 2024, 189, e745–e752. [Google Scholar] [CrossRef]
- Pennington, Z.; Ahmed, A.K.; Cottrill, E.; Westbroek, E.M.; Goodwin, M.L.; Sciubba, D.M. Intra- and interobserver reliability of the Spinal Instability Neoplastic Score system for instability in spine metastases: A systematic review and meta-analysis. Ann. Transl. Med. 2019, 7, 218. [Google Scholar] [CrossRef] [PubMed]
- Versteeg, A.L.; Sahgal, A.; Laufer, I.; Rhines, L.D.; Sciubba, D.M.; Schuster, J.M.; Weber, M.H.; Lazary, A.; Boriani, S.; Bettegowda, C.; et al. Correlation Between the Spinal Instability Neoplastic Score (SINS) and Patient Reported Outcomes. Glob. Spine J. 2023, 13, 1358–1364. [Google Scholar] [CrossRef]

{kind=link}
| Overall (N = 29) | |
|---|---|
| Age (mean (SD)) | 66.9 (9.8) |
| Sex = male (n (%)) | 16 (55.2) |
| Primary tumor (n (%)) | |
| Lung | 7 (24.1) |
| Lymphoma | 1 (3.4) |
| Breast | 4 (13.8) |
| Multiple Myeloma | 7 (24.1) |
| Myxofibrosarcoma | 1 (3.4) |
| Ovarian | 1 (3.4) |
| Prostate | 7 (24.1) |
| CUP * | 1 (3.4) |
| Outcome (n (%)) | |
| Better | 16 (55.2) |
| Never pain | 6 (20.7) |
| Same | 7 (24.1) |
| Overall | SINS 7–9 | SINS 10–12 | p-Value | |
|---|---|---|---|---|
| n | 101 | 74 | 27 | |
| X-ray performed (n (%)) | 96 (95.0) | 72 (97.3) | 24 (88.9) | 0.228 |
| MRI performed (n (%)) | 94 (93.1) | 67 (90.5) | 27 (100.0) | 0.225 |
| CT performed (n (%)) | 99 (99.9) | 73 (100.0) | 26 (100.0) | |
| Location (n (%)) | 0.127 | |||
| cervical | 8 (7.9) | 5 (6.8) | 3 (11.1) | |
| lumbar | 31 (30.7) | 24 (32.4) | 7 (25.9) | |
| sacral | 4 (4.0) | 1 (1.4) | 3 (11.1) | |
| thoracic | 58 (57.4) | 44 (59.5) | 14 (51.9) | |
| SINS (mean (SD)) | 8.62 (1.40) | 7.95 (0.89) | 10.48 (0.64) | <0.001 |
| Radiotherapy (n (%)) | 55 (54.5) | 38 (51.4) | 17 (63.0) | 0.417 |
| Chemotherapy (n (%)) | 85 (90.4) | 64 (94.1) | 21 (80.8) | 0.115 |
| Osteometabolic therapy (n (%)) | 58 (58.0) | 45 (61.6) | 13 (48.1) | 0.324 |
| Surgery (n (%)) | 7 (8.0) | 5 (8.2) | 2 (7.7) | 1.000 |
| Overall | SINS 7–9 | SINS 10–12 | p-Value | |
|---|---|---|---|---|
| n | 101 | 74 | 27 | |
| Location (n (%)) | 0.006 | |||
| Junctional | 39 (38.6) | 22 (29.7) | 17 (63.0) | |
| Mobile spine | 23 (22.8) | 21 (28.4) | 2 (7.4) | |
| Semi-rigid | 39 (38.6) | 31 (41.9) | 8 (29.6) | |
| Mechanical pain (n (%)) | 0.001 | |||
| Yes | 26 (25.7) | 19 (25.7) | 7 (25.9) | |
| No | 46 (45.5) | 27 (36.5) | 19 (70.4) | |
| Pain free lesion | 29 (28.7) | 28 (37.8) | 1 (3.7) | |
| Bone lesion (n (%)) | 0.109 | |||
| Lytic | 64 (63.4) | 51 (68.9) | 13 (48.1) | |
| Mixed | 36 (35.6) | 22 (29.7) | 14 (51.9) | |
| Blastic | 1 (1.0) | 1 (1.4) | 0 (0.0) | |
| Spinal alignment = Normal (n (%)) | 55 (55.6) | 47 (64.4) | 8 (30.8) | 0.006 |
| Vertebral body collapse (n (%)) | 0.006 | |||
| Collapse with >50% body involved | 20 (19.8) | 9 (12.2) | 11 (40.7) | |
| Collapse with <50% body involved | 27 (26.7) | 21 (28.4) | 6 (22.2) | |
| No collapse with >50% body involved | 39 (38.6) | 34 (45.9) | 5 (18.5) | |
| None | 15 (14.9) | 10 (13.5) | 5 (18.5) | |
| Posterolateral involvement (n (%)) | <0.001 | |||
| Bilateral | 15 (15.2) | 5 (6.8) | 10 (38.5) | |
| Unilateral | 16 (16.2) | 14 (19.2) | 2 (7.7) | |
| None | 68 (68.7) | 54 (74.0) | 14 (53.8) |
| SINS 7–9 | SINS 10–12 | |
|---|---|---|
| n | 5 | 2 |
| Age (mean (SD)) | 67.40 (2.88) | 63.00 (2.83) |
| Sex = male (n (%)) | 3 (60.0) | 1 (50.0) |
| Primary tumor (n (%)) | ||
| Lung | 2 (40.0) | 1 (50.0) |
| Lymphoma | 1 (20.0) | 0 (0.0) |
| Breast | 0 (0.0) | 0 (0.0) |
| Multiple Myeloma | 1 (20.0) | 0 (0.0) |
| Myxofibrosarcoma | 0 (0.0) | 0 (0.0) |
| Ovarian | 0 (0.0) | 0 (0.0) |
| Prostate | 1 (20.0) | 1 (50.0) |
| unknown | 0 (0.0) | 0 (0.0) |
| X-ray performed (n (%)) | 5 (100.0) | 2 (100.0) |
| MRI performed (n (%)) | 5 (100.0) | 2 (100.0) |
| CT performed (n (%)) | 5 (100.0) | 2 (100.0) |
| Location (n (%)) | ||
| cervical | 1 (20.0) | 0 (0.0) |
| lumbar | 3 (60.0) | 0 (0.0) |
| thoracic | 1 (20.0) | 2 (100.0) |
| SINS (mean (SD)) | 8.40 (0.89) | 11.00 (0.00) |
| Radiotherapy (n (%)) | 3 (60.0) | 1 (50.0) |
| Chemotherapy (n (%)) | 5 (100.0) | 2 (100.0) |
| Osteometabolic therapy (n (%)) | 4 (80.0) | 1 (50.0) |
| Surgery (n (%)) | 5 (100.0) | 2 (100.0) |
| SINS—Location (n (%)) | ||
| Junctional | 1 (20.0) | 2 (100.0) |
| Mobile spine | 3 (60.0) | 0 (0.0) |
| Semi-rigid | 1 (20.0) | 0 (0.0) |
| SINS—Mechanical pain (n (%)) | ||
| Yes | 2 (40.0) | 1 (50.0) |
| No | 1 (20.0) | 1 (50.0) |
| Pain free lesion | 2 (40.0) | 0 (0.0) |
| SINS—bone lesion = Mixed (n (%)) | 3 (60.0) | 2 (100.0) |
| SINS—spinal alignment = Normal (n (%)) | 3 (60.0) | 1 (50.0) |
| SINS—body collapse (n (%)) | ||
| Collapse with >50% body involved | 2 (40.0) | 1 (50.0) |
| Collapse with <50% body involved | 1 (20.0) | 0 (0.0) |
| No collapse with >50% body involved | 1 (20.0) | 1 (50.0) |
| None | 1 (20.0) | 0 (0.0) |
| SINS—posterolateral involvement = None (n (%)) | 4 (100.0) | 1 (50.0) |
| Description surgery (%) | ||
| Dorsal Instrumentation T10–L2 | 0 (0.0) | 1 (50.0) |
| Dorsal Instrumentation T10–L2 | 1 (20.0) | 0 (0.0) |
| Corpectomy with dorsal instrumentation | 1 (20.0) | 0 (0.0) |
| Kyphoplasty L3 | 1 (20.0) | 0 (0.0) |
| Kyphoplasty T12–L2 | 1 (20.0) | 0 (0.0) |
| Operation terminated due to complications | 0 (0.0) | 1 (50.0) |
| Kyphoplasty L4 | 1 (20.0) | 0 (0.0) |
| Overall | SINS 7–9 | SINS 10–12 | |
|---|---|---|---|
| n | 101 | 74 | 27 |
| Treatment success (%) | |||
| better | 59 (58.4) | 42 (56.8) | 17 (63.0) |
| same | 19 (18.8) | 18 (24.3) | 5 (18.5) |
| worse | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| never pain | 23 (22.8) | 14 (18.9) | 5 (18.5) |
| Conservative | Surgery | |
|---|---|---|
| n | 94 | 7 |
| Treatment success (%) | ||
| better | 53 (56.4) | 6 (85.7) |
| same | 19 (20.2) | 0 (0.0) |
| worse | 0 (0.0) | 0 (0.0) |
| never pain | 22 (23.4) | 1 (14.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schimmelpenning, V.H.; Brugger, R.; Rommers, N.; Kunst, J.; Jäger, M.; Albers, C.E.; Milavec, H. Treatment Outcomes in Spinal Tumors According to Patients’ Perspectives: A Focus on Indeterminate Spinal Instability. Curr. Oncol. 2025, 32, 38. https://doi.org/10.3390/curroncol32010038
Schimmelpenning VH, Brugger R, Rommers N, Kunst J, Jäger M, Albers CE, Milavec H. Treatment Outcomes in Spinal Tumors According to Patients’ Perspectives: A Focus on Indeterminate Spinal Instability. Current Oncology. 2025; 32(1):38. https://doi.org/10.3390/curroncol32010038
Chicago/Turabian StyleSchimmelpenning, Victoria H., Robin Brugger, Nikki Rommers, Johann Kunst, Martin Jäger, Christoph E. Albers, and Helena Milavec. 2025. "Treatment Outcomes in Spinal Tumors According to Patients’ Perspectives: A Focus on Indeterminate Spinal Instability" Current Oncology 32, no. 1: 38. https://doi.org/10.3390/curroncol32010038
APA StyleSchimmelpenning, V. H., Brugger, R., Rommers, N., Kunst, J., Jäger, M., Albers, C. E., & Milavec, H. (2025). Treatment Outcomes in Spinal Tumors According to Patients’ Perspectives: A Focus on Indeterminate Spinal Instability. Current Oncology, 32(1), 38. https://doi.org/10.3390/curroncol32010038