Real-World Safety of Niraparib for Maintenance Treatment of Ovarian Cancer in Canada

 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Population and Setting
2.2. Study Design
2.3. Data Sources
2.4. Key Study Measures
2.4.1. Exposure
2.4.2. Outcomes
2.5. Statistical Analyses
Supplementary Analysis
3. Results
3.1. Cohort Characteristics
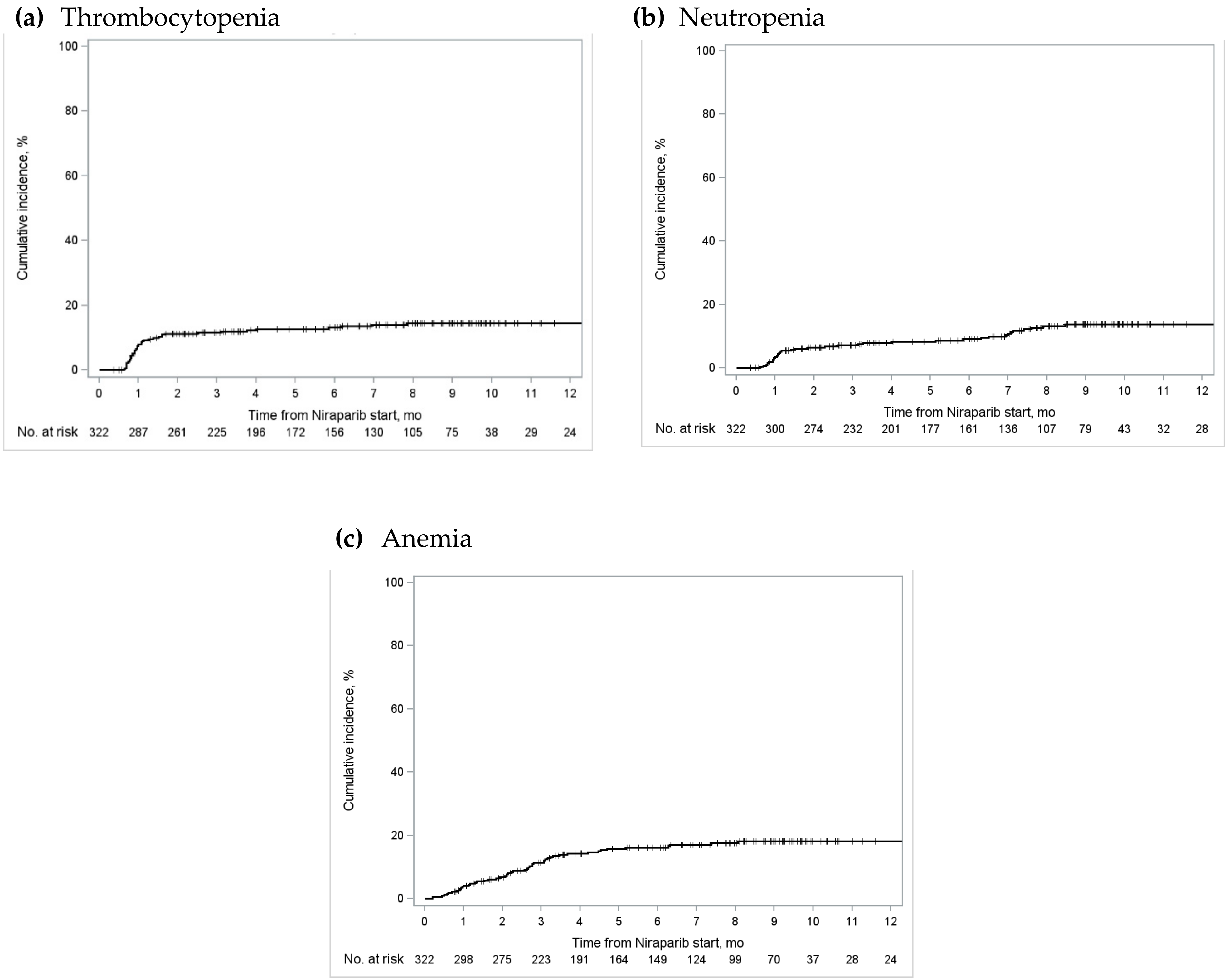
3.2. Primary and Secondary Outcomes

{kind=link}
{kind=link}
| All Provinces N = 426 (%) | Ontario N = 322 (%) 1 | Alberta N = 45 (%) | British Columbia N = 93 (%) 1 | Quebec N = 31 (%) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Any Grade | Grade 3/4 | Any Grade | Grade 3/4 | Any Grade | Grade 3/4 | Any Grade | Grade 3/4 | Any Grade | Grade 3/4 | |
| Thrombocytopenia | 209 (42.5) | 65 (13.2) | 136 (42.2) | 43 (13.4) | 16 (35.6) | <10 | 43 (46.2) | 13 (14.0) | 14 (45.2) | <6 |
| Neutropenia | 192 (39.0) | 60 (12.2) | 107 (33.2) | 37 (11.5) | 23 (51.1) | <10 | 45 (48.4) | 13 (14.0) | 17 (54.8) | <6 |
| Anemia | 384 (78.0) | 66 (13.4) | 258 (80.1) | 52 (16.2) | 34 (75.6) | <10 | 7 (76.3) | 8 (8.6) | 21 (67.7) | <6 |
3.3. Supplementary Analyses
4. Discussion
4.1. Summary
4.2. Comparison with Existing Literature
4.3. Implications for Future Research
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Canadian Cancer Society Cancer Statistics at a Glance. 2014. Available online: https://cancer.ca/en/research/cancer-statistics/cancer-statistics-at-a-glance?gad_source=1&gclid=EAIaIQobChMI0_n-i-f4ggMVtNDCBB10LQ6uEAAYASAAEgKr0_D_BwE (accessed on 1 December 2023).
- Tinker, A.V.; Altman, A.D.; Bernardini, M.Q.; Ghatage, P.; Gien, L.T.; Provencher, D.; Salvador, S.; Doucette, S.; Oza, A.M. A Pan-Canadian Consensus Statement on First-Line PARP Inhibitor Maintenance for Advanced, High-Grade Serous and Endometrioid Tubal, Ovarian, and Primary Peritoneal Cancers. Curr. Oncol. 2022, 29, 4354–4369. [Google Scholar] [CrossRef]
- Canadian Cancer Society Survival Statistics for Ovarian Cancer. Available online: https://cancer.ca/en/cancer-information/cancer-types/ovarian/prognosis-and-survival/survival-statistics (accessed on 23 July 2023).
- Canadian Cancer Society. Ovarian Cancer. 2023. Available online: https://cancer.ca/en/cancer-information/cancer-types/ovarian (accessed on 23 July 2023).
- Ontario Health. Homologous Recombination Deficiency Testing to Inform Patient Decisions about Niraparib Maintenance Therapy for High-Grade Serous or Endometrioid Epithelial Ovarian Cancer: Recommendation; Ontario Health: Toronto, ON, Canada, 2023; pp. 1–7. [Google Scholar]
- Mirza, M.R.; Monk, B.J.; Herrstedt, J.; Oza, A.M.; Mahner, S.; Redondo, A.; Fabbro, M.; Ledermann, J.A.; Lorusso, D.; Vergote, I.; et al. Niraparib Maintenance Therapy in Platinum-Sensitive, Recurrent Ovarian Cancer. N. Engl. J. Med. 2016, 375, 2154–2164. [Google Scholar] [CrossRef]
- González-Martín, A.; Pothuri, B.; Vergote, I.; DePont Christensen, R.; Graybill, W.; Mirza, M.R.; McCormick, C.; Lorusso, D.; Hoskins, P.; Freyer, G.; et al. Niraparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2391–2402. [Google Scholar] [CrossRef]
- Wu, X.H.; Zhu, J.Q.; Yin, R.T.; Yang, J.X.; Liu, J.H.; Wang, J.; Wu, L.Y.; Liu, Z.L.; Gao, Y.N.; Wang, D.B.; et al. Niraparib Maintenance Therapy in Patients with Platinum-Sensitive Recurrent Ovarian Cancer Using an Individualized Starting Dose (NORA): A Randomized, Double-Blind, Placebo-Controlled Phase III Trial☆. Ann. Oncol. 2021, 32, 512–521. [Google Scholar] [CrossRef]
- Vilming, B.; Fallås Dahl, J.; Bentzen, A.G.; Ingebrigtsen, V.A.; Berge Nilsen, E.; Vistad, I.; Dørum, A.; Solheim, O.; Bjørge, L.; Zucknick, M.; et al. Real-World Data on Niraparib Maintenance Treatment in Patients with Non-gBRCA Mutated Platinum-Sensitive Recurrent Ovarian Cancer. Int. J. Gynecol. Cancer 2023, 33, 1898–1905. [Google Scholar] [CrossRef]
- Zhao, M.; Qiu, S.; Wu, X.; Miao, P.; Jiang, Z.; Zhu, T.; Xu, X.; Zhu, Y.; Zhang, B.; Yuan, D.; et al. Efficacy and Safety of Niraparib as First-Line Maintenance Treatment for Patients with Advanced Ovarian Cancer: Real-World Data from a Multicenter Study in China. Targ. Oncol. 2023, 18, 869–883. [Google Scholar] [CrossRef]
- GlaxoSmithKline. ZEJULA—A New Maintenance Treatment Option for Canadians Living with Ovarian Cancer—Now Available in Canada. Available online: https://ca.gsk.com/en-ca/media/press-releases/zejula-a-new-maintenance-treatment-option-for-canadians-living-with-ovarian-cancer-now-available-in-canada/ (accessed on 23 July 2023).
- GlaxoSmithKline. ZEJULA Is Approved in Canada for First-Line Maintenance Treatment of Women with Advanced Ovarian Cancer. Available online: https://www.newswire.ca/news-releases/zejula-is-approved-in-canada-for-first-line-maintenance-treatment-of-women-with-advanced-ovarian-cancer-849289412.html (accessed on 23 July 2023).
- BC Cancer. Systemic Therapy Update. 2021. Available online: http://www.bccancer.bc.ca/health-professionals/clinical-resources/systemic-therapy/systemic-therapy-update (accessed on 23 July 2023).
- Ontario Ministry of Health. Exceptional Access Program Reimbursement Criteria for Frequently Requested Drugs. 2023. Available online: https://files.ontario.ca/moh-frequently-requested-drugs.pdf (accessed on 23 July 2023).
- Alberta Health Services. Outpatient Cancer Drug Benefit Program. 2023. Available online: https://www.albertahealthservices.ca/services/page2328.aspx (accessed on 16 April 2024).
- Regie de L’assurance Maladie du Quebec. Liste Des Medicaments—29 Septembre 2021. 2021. Available online: https://www.ramq.gouv.qc.ca/fr/media/12091 (accessed on 23 July 2023).
- Sheldrick, R.C. Randomized Trials vs. Real-World Evidence: How Can Both Inform Decision-Making? JAMA 2023, 329, 1352. [Google Scholar] [CrossRef]
- Kim, H.-S.; Lee, S.; Kim, J.H. Real-World Evidence versus Randomized Controlled Trial: Clinical Research Based on Electronic Medical Records. J. Korean Med. Sci. 2018, 33, e213. [Google Scholar] [CrossRef]
- CoLab Mainpage. Available online: https://colab.cadth.ca/ (accessed on 16 April 2024).
- CCRE Mainpage. Available online: https://ccreplatform.com/ (accessed on 16 April 2024).
- Exactis Innovation Mainpage. Available online: https://www.exactis.ca/ (accessed on 16 April 2024).
- ClinicalTrials.gov. Personalize My Treatment (PMT) Registry (PMT). Available online: https://www.clinicaltrials.gov/study/NCT02355171?cond=NCT02355171&rank=1 (accessed on 23 July 2023).
- National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) Common Terminology Criteria for Adverse Events (CTCAE) v5.0. 2017. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 23 July 2023).
- Austin, P.C.; Steyerberg, E.W.; Putter, H. Fine-Gray Subdistribution Hazard Models to Simultaneously Estimate the Absolute Risk of Different Event Types: Cumulative Total Failure Probability May Exceed 1. Stat. Med. 2021, 40, 4200–4212. [Google Scholar] [CrossRef]
- Allison, P.D. Survival Analysis Using SAS: A Practical Guide, 2nd ed.; SAS Press: Cary, NC, USA, 2010; ISBN 978-1-59994-640-5. [Google Scholar]
- Guan, Q.; Aktar, S.; Pataky, R.; Stephen, M.M.; Marques, M.; Gambaro, K.; Forster, K.; Strub, S.; Cheung, W.Y.; Peacock, S.; et al. The Safety of Niraparib in Ovarian Cancer; Canadian Cancer Real-World Evaluation Platform: Ottawa, ON, Canada, 2024. [Google Scholar]
- Nakamura, K.; Matsuoka, H.; Yorimitsu, M.; Ogawa, M.; Kanemori, M.; Sueoka, K.; Kozai, A.; Nakamura, H.; Haruma, T.; Shiroyama, Y.; et al. Efficacy and Safety of Olaparib, Olaparib plus Bevacizumab and Niraparib Maintenance Treatment in Japanese Patients with Platinum-Sensitive Advanced Ovarian Cancer. Jpn. J. Clin. Oncol. 2023, 54, 31–37. [Google Scholar] [CrossRef]
- Li, J.; Yang, J.; Shou, H.; Zhang, L.; Huang, X.; Tang, X.; Zheng, F.; Liu, F.; Wen, H.; Yang, H.; et al. Real-world Outcomes of Niraparib Treatment in Patients with Ovarian Cancer: A Multicenter Non-interventional Study in China. Cancer Commun. 2023, 43, 716–719. [Google Scholar] [CrossRef]
- GlaxoSmithKline. Product Monograph Including Patient Medication Information: Zejula. 2023. Available online: https://ca.gsk.com/media/6229/zejula_pm_en.pdf (accessed on 16 April 2024).

| All Provinces N = 514 (%) | Ontario N = 338 (%) | Alberta N = 45 (%) | British Columbia N = 100 (%) | Quebec N = 31 (%) | ||
|---|---|---|---|---|---|---|
| Mean Age (± SD) | 66.8 ± 10.3 | 68.8 ± 9.7 | 67.0 ± 9.0 | 66.1 ± 10.4 | 65.3 ± 11.9 | |
| Urban Residence | 396–402 (77.0–78.2) | 280 (82.8) 1 | 24 (53.3) | 92–98 (92.0–98.0) | N/A | |
| Year of Cancer Diagnosis | ≤2018 | 89 (17.3) | 81 (24.0) | <10 | <6 | <6 |
| 2019 | 45 (8.8) | 26 (7.7) | <10 | 9 (9.0) | <6 | |
| 2020 | 78 (15.2) | 60 (17.8) | <10 | <6 | 10 (32.3) | |
| 2021 | 217 (42.2) | 119 (35.2) | 28 (62.2) | 60 (60.0) | 10 (32.3) | |
| 2022 | 86 (16.7) | 52 (15.4) | <10 | 25 (25.0) | <6 | |
| Cancer Stage at Diagnosis | I–II | 37 (7.2) | 22 (6.5) | <10 | 6 (6.0) | <6 |
| III | 225 (43.8) | 123 (36.4) | 29 (64.4) | 50 (50.0) | 23 (74.2) | |
| IV | 89–101 (17.3–19.6) | 56 (16.6) | <10 | 27 (27.0) | 5–9 (16.1–29.0) | |
| Unknown | 155–163 (30.2–31.7) | 137 (40.5) | <10 | 17 (17.0) | 0 | |
| Year of Niraparib Start | 2020–2021 | 51–55 (9.9–10.7) | 32 (9.5) | 0 | <6 | 17 (54.8) |
| 2022 | 459–463 (89.3–90.1) | 306 (90.5) | 45 (100.0) | 94–98 (94.0–98.0) | 14 (45.2) | |
| Primary Tumour Location | Ovaries | 400–404 (77.8–78.6) | 312 (92.3) | 22 (48.9) | 40 (40.0) | 26–30 (83.9–96.9) |
| Fallopian Tubes | 78–86 (15.2–16.7) | 12 (3.6) | 13–21 (28.9–46.7) | 53 (53.0) | 0 | |
| Other | 32 (6.2) | 14 (4.1) | <10 | 7 (7.0) | <6 | |
| Primary Tumour Histology | Serous | 453–461 (88.1–89.7) | 292 (86.4) | 41 (91.1) | 94–98 (94.0–98.0) | 26–30 (83.8–96.8) |
| Endometriod | 9–17 (1.8–3.3) | 8 (2.4) | <10 | 0 | 0 | |
| Other | 47 (9.1) | 38 (11.2) | <10 | <6 | <6 | |
| Cancer Antigen-125 Level >35 units/mL | 38 (21.6) | N/A | 12 (26.7) | 18 (19.0) | 8 (25.8) | |
| Prior Platinum-Based Chemotherapy | 505 (98.2) | 336 (99.4) 2 | 36–44 (80.0–97.8) | 100 (100.0) | 26–30 (83.9–96.7) | |
| Mean Number of Prior Cycles of Platinum-Based Chemotherapy (±SD) | 6.5 ± 2.9 | 8.8 ± 4.9 | 4.0 ± 2.0 | 6.4 ± 1.0 | 6.6 ± 1.9 | |
| Mean Number of Days Between Last Platinum-Based Chemotherapy and Niraparib Start (±SD) 2 | 57.3 ± 25.9 | 55.3 ± 31.3 | 60.4 ± 27.0 | 55.1 ± 21.8 | 58.3 ± 22.2 | |
| Initial Daily Dose of Niraparib 3 | 100 mg | 103 (24.1) | 58 (22.9) | 17 (37.8) | 28 (28.0) | 0 |
| 200 mg | 288–292 (67.3–68.2) | 175 (69.2) | 28 (62.2) | 60 (60.0) | 25–29 (83.3–96.7) | |
| 300 mg | 33–37 (7.7–8.6) | 20 (7.9) | 0 | 12 (12.0) | <6 | |
| All Provinces N = 514 (%) | Ontario N = 338 (%) | Alberta N = 45 (%) | British Columbia N = 100 (%) | Quebec N = 31 (%) | ||
|---|---|---|---|---|---|---|
| Febrile Neutropenia | <10 | <6 | <10 | N/A | 0 | |
| Incident Hypertension 1 | 44–52 (19.4–22.9) | 37 (20.2) | <10 | N/A | 6 (33.3) | |
| Blood Transfusion | Any Cell Type | 53 (12.8) | 33 (9.8) | 11 (24.4) | N/A | 9 (29.0) |
| Red Blood Cell | 32 (7.7) | 22 (6.5) | <10 | N/A | <6 | |
| Platelet | 18 (4.3) | 11 (3.3) | <10 | N/A | <6 | |
| Hospitalization | Any Type | 80 (19.3) | 63 (18.6) | 17 (37.8) | N/A | 0 |
| Unscheduled | 57 (15.4) | 57 (16.9) | N/A | N/A | 0 | |
| Emergency Department Visit | 153–157 (37.0–37.9) | 134 (39.6) | 18 (40.0) | N/A | 0 | |
| Niraparib Treatment Discontinuation | 150–159 (35.0–36.9) | 86 (34.0) | <10 | 41 (41.0) | 22 (73.3) | |
| Mean Time to Niraparib Treatment Discontinuation in Days (± SD) 2 | 163.6 ± 111.5 | 164.6 ± 64.1 | 135.0 ± 78.0 | 91.0 ± 53.9 | 263.8 ±191.3 | |
| Median Follow-Up Time in Days (IQR) | N/A 3 | 255 (241–267) | 299 (170–274) | 250 (78–310) | 411 (270–585) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guan, Q.; Aktar, S.J.; Pataky, R.E.; Stephen, M.M.; Marques, M.; Gambaro, K.; Rachedi, K.; Forster, K.; Strub, S.; Stock, D.; et al. Real-World Safety of Niraparib for Maintenance Treatment of Ovarian Cancer in Canada. Curr. Oncol. 2024, 31, 3591-3602. https://doi.org/10.3390/curroncol31060264
Guan Q, Aktar SJ, Pataky RE, Stephen MM, Marques M, Gambaro K, Rachedi K, Forster K, Strub S, Stock D, et al. Real-World Safety of Niraparib for Maintenance Treatment of Ovarian Cancer in Canada. Current Oncology. 2024; 31(6):3591-3602. https://doi.org/10.3390/curroncol31060264
Chicago/Turabian StyleGuan, Qi, Suriya J. Aktar, Reka E. Pataky, Mariet Mathew Stephen, Maud Marques, Karen Gambaro, Kahina Rachedi, Katharina Forster, Samara Strub, David Stock, and et al. 2024. "Real-World Safety of Niraparib for Maintenance Treatment of Ovarian Cancer in Canada" Current Oncology 31, no. 6: 3591-3602. https://doi.org/10.3390/curroncol31060264
APA StyleGuan, Q., Aktar, S. J., Pataky, R. E., Stephen, M. M., Marques, M., Gambaro, K., Rachedi, K., Forster, K., Strub, S., Stock, D., de Léséleuc, L., Cheung, W. Y., Peacock, S., Farrer, C., Gavura, S., Tadrous, M., Grant, R. C., & Chan, K. K. W. (2024). Real-World Safety of Niraparib for Maintenance Treatment of Ovarian Cancer in Canada. Current Oncology, 31(6), 3591-3602. https://doi.org/10.3390/curroncol31060264