Colorectal Cancer Patients’ Reported Frequency, Content, and Satisfaction with Advance Care Planning Discussions

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Context
2.2. Participants
2.3. Survey Instruments
2.4. Data Collection
2.5. Data Analysis
3. Results
3.1. Demographics and Data Collection
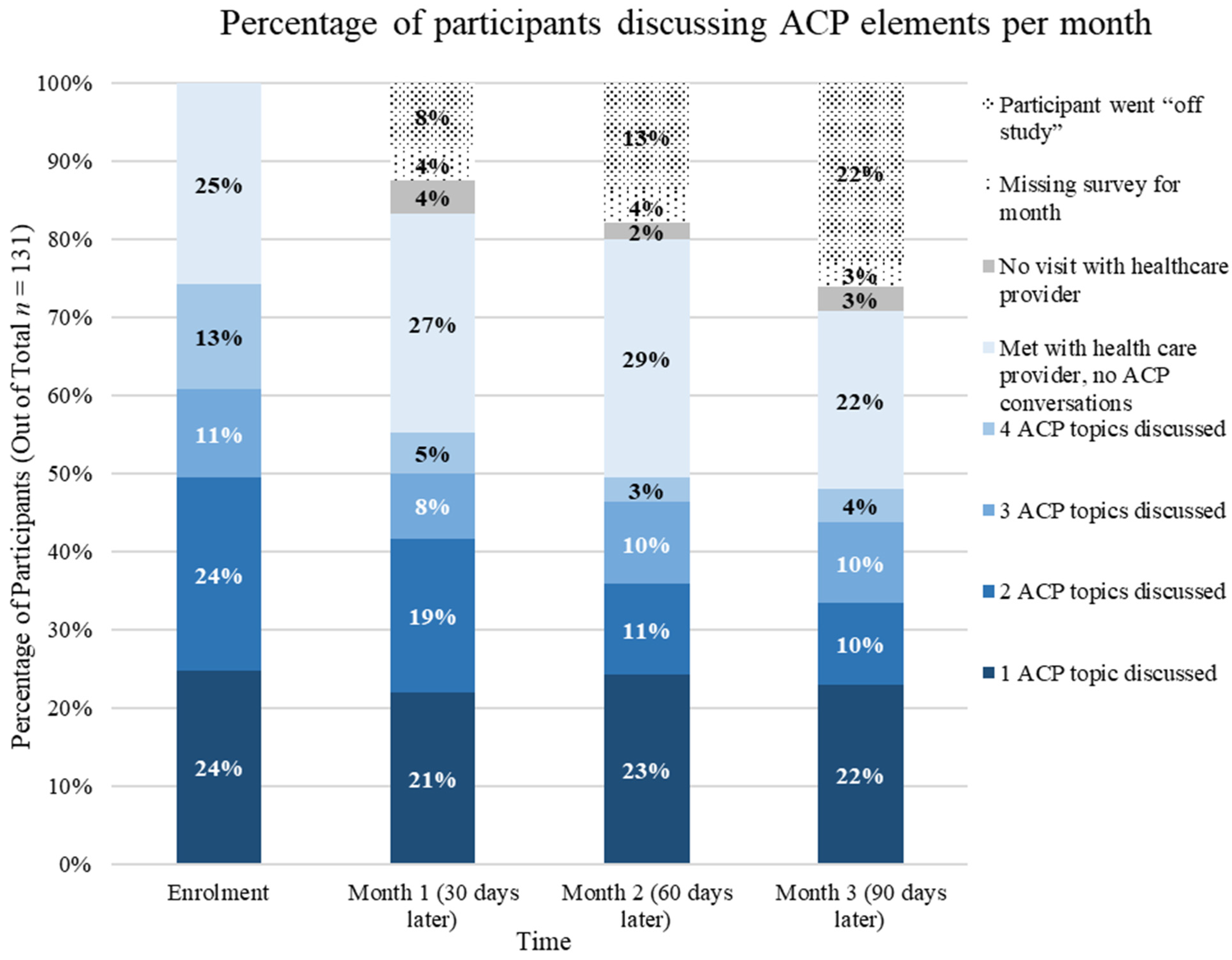
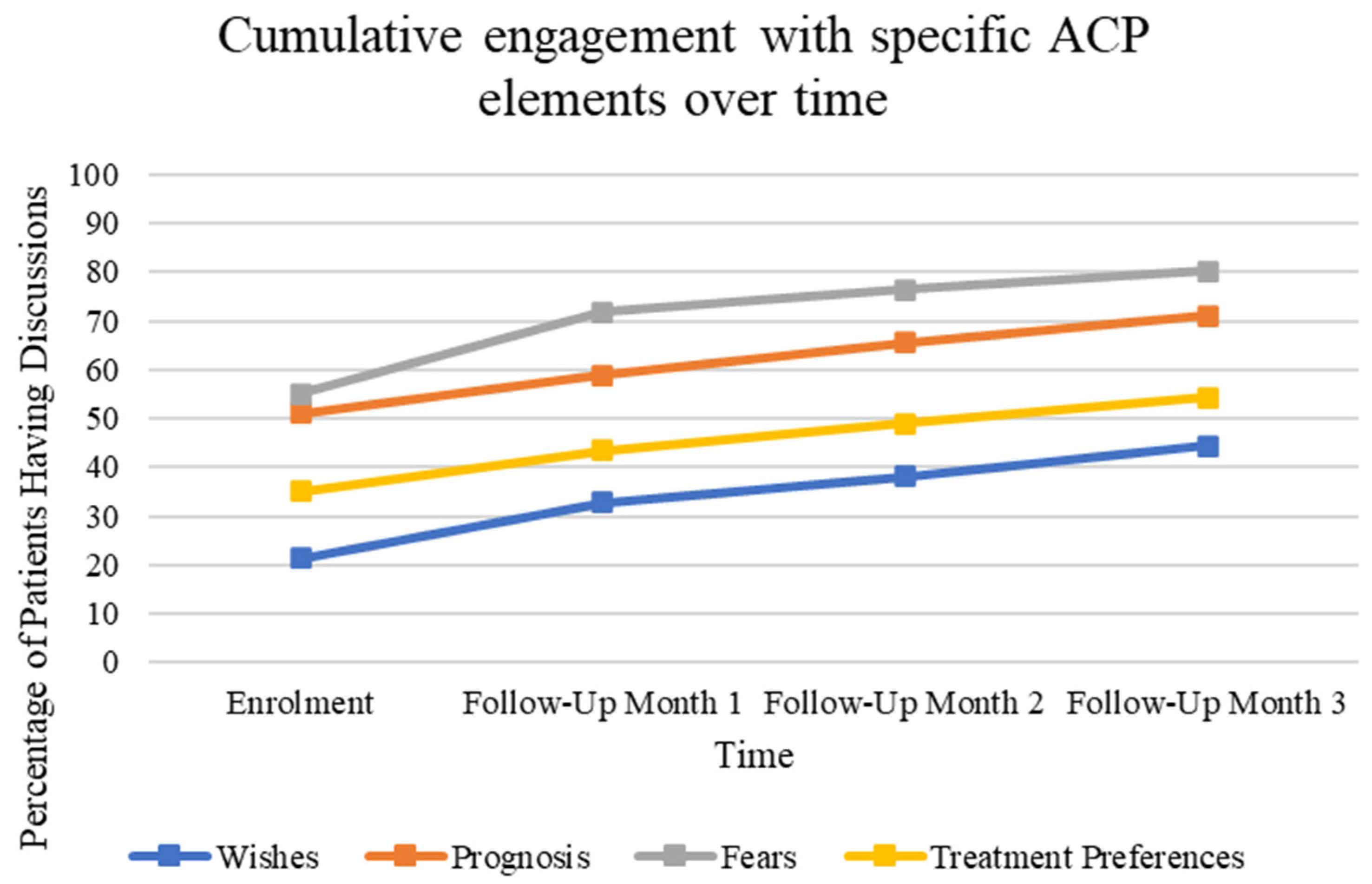
3.2. Frequency of ACP Discussion and GCD Order Reporting over Time
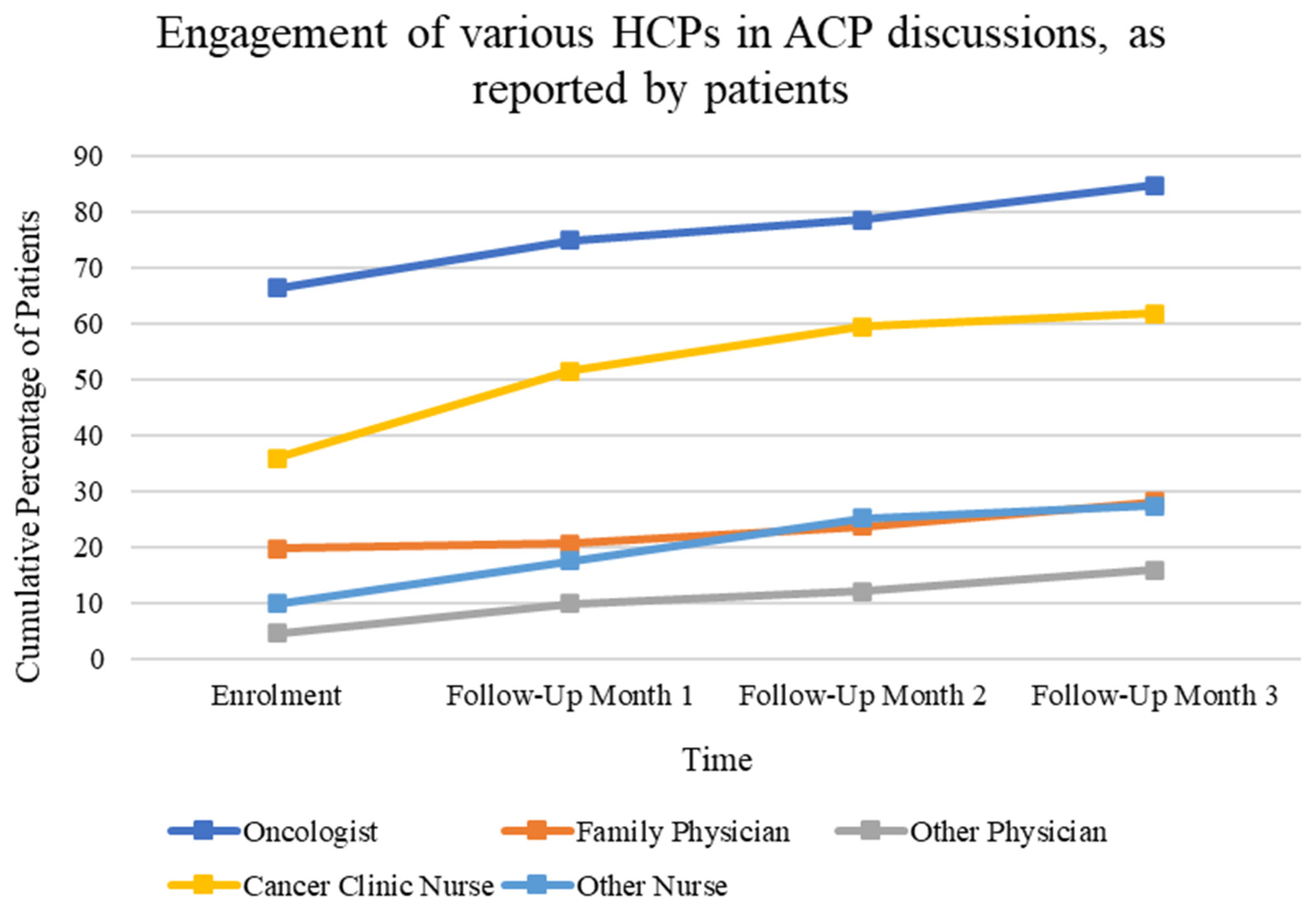
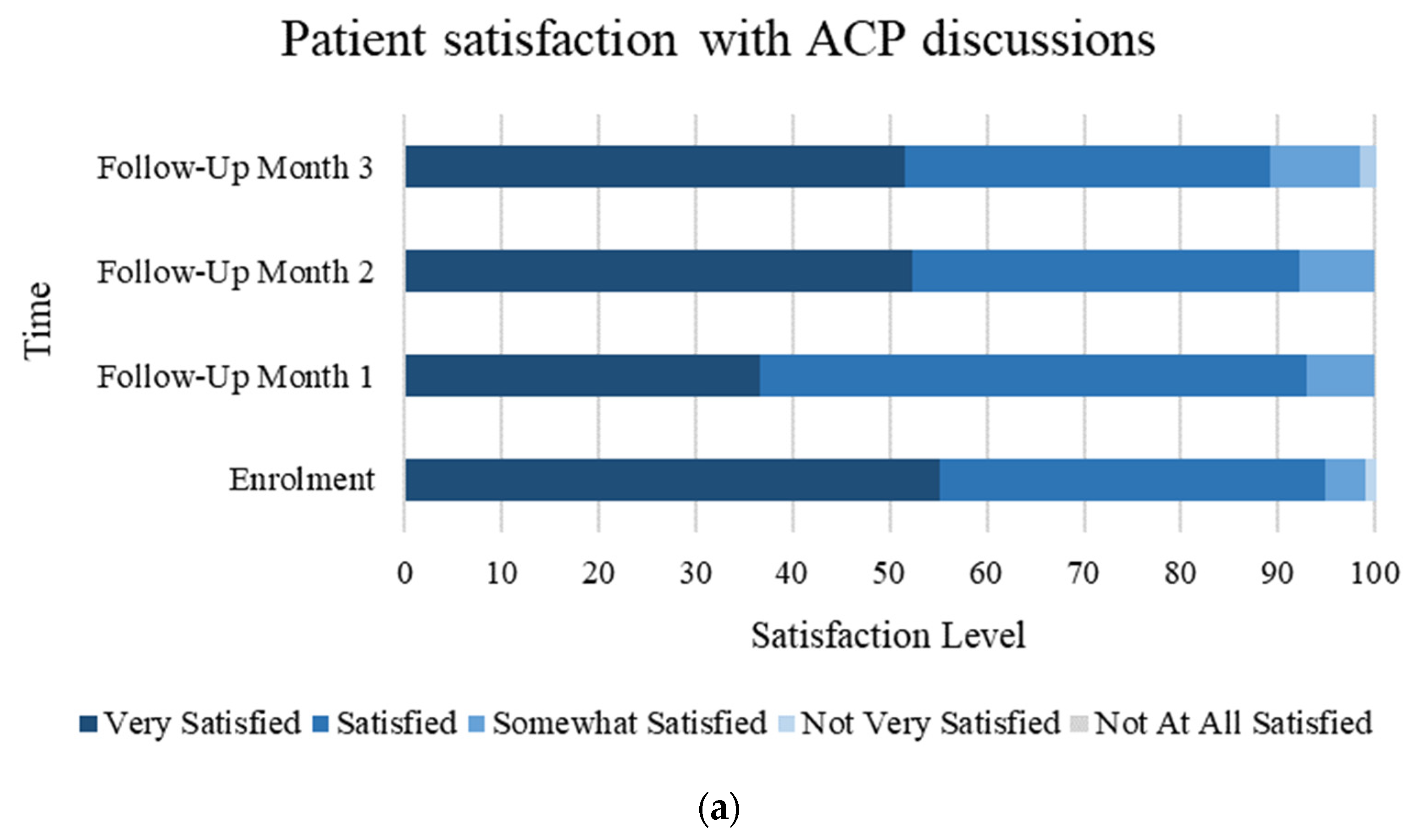
3.3. Satisfaction and HCP Participation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sudore, R.L.; Lum, H.D.; You, J.J.; Hanson, L.C.; Meier, D.E.; Pantilat, S.Z.; Matlock, D.D.; Rietjens, J.; Korfage, I.J.; Ritchie, C.S.; et al. Defining Advance Care Planning for Adults: A Consensus Definition from a Multidisciplinary Delphi Panel. J. Pain. Symptom Manage 2017, 53, 821–832. [Google Scholar] [CrossRef] [PubMed]
- Rietjens, J.A.C.; Sudore, R.L.; Connolly, M.; van Delden, J.J.; Drickamer, M.A.; Droger, M.; van der Heide, A.; Heyland, D.K.; Houttekier, D.; Janssen, D.J.A.; et al. Definition and recommendations for advance care planning: An international consensus supported by the European Association for Palliative Care. Lancet. Oncol. 2017, 18, e543–e551. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, G.; Tan, W.S.; Virk, A.K.; Low, C.K.; Car, J.; Ho, A. State of advance care planning research: A descriptive overview of systematic reviews. Palliat. Support. Care 2019, 17, 234–244. [Google Scholar] [CrossRef] [PubMed]
- McMahan, R.D.; Tellez, I.; Sudore, R.L. Deconstructing the Complexities of Advance Care Planning Outcomes: What Do We Know and Where Do We Go? A Scoping Review. J. Am. Geriatr. Soc. 2021, 69, 234–244. [Google Scholar] [CrossRef] [PubMed]
- Karim, S.; Lupichuk, S.; Tan, A.; Sinnarajah, A.; Simon, J. Real World Implementation of the Serious Illness Care Program in Cancer Care: Results of a Quality Improvement Initiative. J. Palliat. Med. 2021, 24, 905–909. [Google Scholar] [CrossRef] [PubMed]
- Raskin, W.; Harle, I.; Hopman, W.M.; Booth, C.M. Prognosis, Treatment Benefit and Goals of Care: What Do Oncologists Discuss with Patients Who Have Incurable Cancer? Clin. Oncol. 2016, 28, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Heyland, D.K.; Barwich, D.; Pichora, D.; Dodek, P.; Lamontagne, F.; You, J.J.; Tayler, C.; Porterfield, P.; Sinuff, T.; Simon, J. Failure to Engage Hospitalized Elderly Patients and Their Families in Advance Care Planning. JAMA Intern. Med. 2013, 173, 778–787. [Google Scholar] [CrossRef] [PubMed]
- Harle, I.; Karim, S.; Raskin, W.; Hopman, W.M.; Booth, C.M. Toward improved goals-of-care documentation in advanced cancer: Report on the development of a quality improvement initiative. Curr. Oncol. 2017, 24, 383–389. [Google Scholar] [CrossRef]
- Sudore, R.L.; Heyland, D.K.; Lum, H.D.; Rietjens, J.; Korfage, I.J.; Ritchie, C.S.; Hanson, L.C.; Meier, D.E.; Pantilat, S.Z.; Lorenz, K.; et al. Outcomes That Define Successful Advance Care Planning: A Delphi Panel Consensus. J. Pain. Symptom Manage 2018, 55, 245–255. [Google Scholar] [CrossRef] [PubMed]
- The Palliative Care Early and Systematic (PaCES) Project. Available online: https://cumming.ucalgary.ca/research/paces-project (accessed on 13 September 2023).
- Alberta Health Services. Advance Care Planning and Goals of Care Designation Policy. 2016. Available online: https://extranet.ahsnet.ca/teams/policydocuments/1/clp-advance-care-planning-hcs-38-policy.pdf. (accessed on 13 September 2023).
- Alberta Health Services. Integrating an Early Palliative Approach into Advanced Colorectal Cancer. 2020. Available online: https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-metastatic-colorectal-early-palliative-cancer-care.pdf. (accessed on 13 September 2023).
- Watanabe, S.M.; Nekolaichuk, C.; Beaumont, C.; Johnson, L.; Myers, J.; Strasser, F. A Multicenter Study Comparing Two Numerical Versions of the Edmonton Symptom Assessment System in Palliative Care Patients. J. Pain. Symptom Manage 2011, 41, 456–468. [Google Scholar] [CrossRef]
- You, J.J.; Dodek, P.; Lamontagne, F.; Downar, J.; Sinuff, T.; Jiang, X.; Day, A.G.; Heyland, D.K. What Really Matters in End-of-Life Discussions? Perspectives of Patients in Hospital with Serious Illness and Their Families. CMAJ 2014, 186, E679–E687. [Google Scholar] [CrossRef]
- Bradley, E.H.; Hallemeier, A.G.; Fried, T.R.; Johnson-Hurzeler, R.; Cherlin, E.J.; Kasl, S.V.; Horwitz, S.M. Documentation of Discussions about Prognosis with Terminally Ill Patients. Am. J. Med. 2001, 111, 218–223. [Google Scholar] [CrossRef]
- Frey, M.K.; Philips, S.R.; Jeffries, J.; Herzberg, A.J.; Harding-Peets, G.L.; Gordon, J.K.; Bajada, L.; Ellis, A.E.; Blank, S.V. A Qualitative Study of Ovarian Cancer Survivors’ Perceptions of Endpoints and Goals of Care. Gynecol. Oncol. 2014, 135, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.T.; Liu, T.W.; Liu, L.N.; Chiu, C.F.; Hsieh, R.K.; Tsai, C.M. Physician-Patient End-of-Life Care Discussions: Correlates and Associations with End-of-Life Care Preferences of Cancer Patients—A Cross-Sectional Survey Study. Palliat. Med. 2014, 28, 1222–1230. [Google Scholar] [CrossRef] [PubMed]
- Wright, A.A.; Zhang, B.; Alaka Ray, M.; Mack, J.W.; Elizabeth Trice, M.; Balboni, T.; Susan Mitchell, M.L.; Jackson, V.A.; Susan Block, M.D.; Maciejewski, P.K.; et al. Associations Between End-of-Life Discussions, Patient Mental Health, Medical Care Near Death, and Caregiver Bereavement Adjustment. JAMA 2008, 300, 1665–1673. [Google Scholar] [CrossRef]
- Kubi, B.; Istl, A.C.; Lee, K.T.; Conca-Cheng, A.; Johnston, F.M. Advance Care Planning in Cancer: Patient Preferences for Personnel and Timing. JCO Oncol. Pract. 2020, 16, e875–e883. [Google Scholar] [CrossRef] [PubMed]
- Paladino, J.; Bernacki, R.; Neville, B.A.; Kavanagh, J.; Miranda, S.P.; Palmor, M.; Lakin, J.; Desai, M.; Lamas, D.; Sanders, J.J.; et al. Evaluating an Intervention to Improve Communication between Oncology Clinicians and Patients with Life-Limiting Cancer: A Cluster Randomized Clinical Trial of the Serious Illness Care Program. JAMA Oncol. 2019, 5, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.R.; Weir, H.K.; Demers, A.A.; Ellison, L.F.; Louzado, C.; Shaw, A.; Turner, D.; Woods, R.R.; Smith, L.M. Projected Estimates of Cancer in Canada in 2020. CMAJ 2020, 192, E199–E205. [Google Scholar] [CrossRef] [PubMed]
- Cancer Care Alberta—Internal Audit. 2019.
- Mack, J.W.; Cronin, A.; Taback, N.; Huskamp, H.A.; Keating, N.L.; Malin, J.L.; Earle, C.C.; Weeks, J.C. End-of-life care discussions among patients with advanced cancer: A cohort study. Ann. Intern. Med. 2012, 156, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Prater, L.C.; Wickizer, T.; Bose-Brill, S. Examining Age Inequalities in Operationalized Components of Advance Care Planning: Truncation of the ACP Process with Age. J. Pain. Symptom Manage 2019, 57, 731–737. [Google Scholar] [CrossRef]
- Oh, J.; Dennis, K.; Lefresne, S.; Livergant, J.; McKenzie, M. End-of-Life Discussions in Practice: Survey among Canadian Radiation Oncologists. Ann. Palliat. Med. 2019, 8, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Geerse, O.P.; Lamas, D.J.; Bernacki, R.E.; Sanders, J.J.; Paladino, J.; Berendsen, A.J.; Hiltermann, T.J.N.; Lindvall, C.; Fromme, E.K.; Block, S.D. Adherence and Concordance between Serious Illness Care Planning Conversations and Oncology Clinician Documentation among Patients with Advanced Cancer. J. Palliat. Med. 2021, 24, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Gonella, S.; Dimonte, V.; Arnone, Y.; Albanesi, B.; Berchialla, P.; Di Giulio, P.; van der Steen, J.T. Interventions to Promote End-of-Life Conversations: A Systematic Review and Meta-Analysis. J. Pain Symptom Manag. 2023, 66, e365–e398. [Google Scholar] [CrossRef] [PubMed]
- Levoy, K.; Salani, D.A.; Buck, H. A Systematic Review and Gap Analysis of Advance Care Planning Intervention Components and Outcomes Among Cancer Patients Using the Transtheoretical Model of Health Behavior Change. J. Pain. Symptom Manage 2019, 57, 118–139. [Google Scholar] [CrossRef] [PubMed]
- Ingersoll, L.T.; Saeed, F.; Ladwig, S.; Norton, S.A.; Anderson, W.; Alexander, S.C.; Gramling, R. Feeling Heard and Understood in the Hospital Environment: Benchmarking Communication Quality Among Patients with Advanced Cancer Before and After Palliative Care Consultation. J. Pain. Symptom Manage 2018, 56, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Thorne, S.; Hislop, T.G.; Kim-Sing, C.; Oglov, V.; Oliffe, J.L.; Stajduhar, K.I. Changing Communication Needs and Preferences across the Cancer Care Trajectory: Insights from the Patient Perspective. Support. Care Cancer 2014, 22, 1009–1015. [Google Scholar] [CrossRef]
- Back, A.L.; Trinidad, S.B.; Hopley, E.K.; Edwards, K.A. Reframing the Goals of Care Conversation: “We’re in a Different Place”. J. Palliat. Med. 2014, 17, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- Michael, N.; O’Callaghan, C.; Clayton, J.; Pollard, A.; Stepanov, N.; Spruyt, O.; Michael, M.; Ball, D. Understanding how cancer patients actualise, relinquish, and reject advance care planning: Implications for practice. Support. Care Cancer 2013, 21, 2195–2205. [Google Scholar] [CrossRef] [PubMed]
- Schulman-Green, D.; Smith, C.B.; Lin, J.J.; Feder, S.; Bickell, N.A. Oncologists’ and Patients’ Perceptions of Initial, Intermediate, and Final Goals of Care Conversations. J. Pain. Symptom Manage 2018, 55, 890–896. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.; Butow, P.; Kerridge, I.; Tattersall, M. Advance Care Planning for Cancer Patients: A Systematic Review of Perceptions and Experiences of Patients, Families, and Healthcare Providers. Psychooncology 2016, 25, 362–386. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Carreras, M.T.; Chaftari, P.; Viets-Upchurch, J. Advance Care Planning: Challenges at the Emergency Department of a Cancer Care Center. Support Care Cancer 2018, 26, 585–588. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; Steinberg, L.; Seow, H. Controversies About Advance Care Planning. JAMA 2022, 327, 684–685. [Google Scholar] [CrossRef] [PubMed]
- Karim, S.; Levine, O.; Simon, J. The Serious Illness Care Program in Oncology: Evidence, Real-World Implementation and Ongoing Barriers. Curr. Oncol. 2022, 29, 1527–1536. [Google Scholar] [CrossRef] [PubMed]
- Nouri, S.S.; Barnes, D.E.; Shi, Y.; Volow, A.M.; Shirsat, N.; Kinderman, A.L.; Harris, H.A.; Sudore, R.L. The PREPARE for Your Care program increases advance care planning engagement among diverse older adults with cancer. Cancer 2021, 127, 3631–3639. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | Total (n = 131) |
|---|---|
| Age at enrollment, median (IQR) | 64 (57–70) |
| Gender | |
| Female | 57 (44%) |
| Male | 74 (56%) |
| Race | |
| White | 115 (88%) |
| Other | 16 (12%) |
| Educational attainment | |
| <High school | 14 (11%) |
| High school | 26 (20%) |
| College (some or complete) | 40 (31%) |
| University (any level) | 51 (39%) |
| Marital status | |
| Married, or living as married | 100 (76%) |
| Widowed | 7 (5%) |
| Never married | 12 (9%) |
| Divorced, separated, not married | 12 (9%) |
| Residence prior to admission | |
| Own home | 128 (98%) |
| Retirement residence | 2 (2%) |
| Other | 1 (1%) |
| Income (Canadian dollars) | |
| <$25,000 | 14 (11%) |
| $25,000–$49,000 | 19 (15%) |
| $50,000–$74,999 | 17 (13%) |
| $75,000–$99,999 | 15 (11%) |
| $100,000 | 32 (24%) |
| Decline | 34 (26%) |
| Patient religiousness | |
| Spiritual and religious | 45 (34%) |
| Spiritual but not religious | 48 (37%) |
| Religious but not spiritual | 3 (2%) |
| Neither religious nor spiritual | 25 (18%) |
| Unsure | 9 (7%) |
| Decline | 2 (2%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hussein, S.; Lim, C.A.; Manokaran, T.; Kassam, S.; Earp, M.; Tang, P.A.; Karim, S.; Biondo, P.; Watanabe, S.M.; Sinnarajah, A.; et al. Colorectal Cancer Patients’ Reported Frequency, Content, and Satisfaction with Advance Care Planning Discussions. Curr. Oncol. 2024, 31, 1235-1245. https://doi.org/10.3390/curroncol31030092
Hussein S, Lim CA, Manokaran T, Kassam S, Earp M, Tang PA, Karim S, Biondo P, Watanabe SM, Sinnarajah A, et al. Colorectal Cancer Patients’ Reported Frequency, Content, and Satisfaction with Advance Care Planning Discussions. Current Oncology. 2024; 31(3):1235-1245. https://doi.org/10.3390/curroncol31030092
Chicago/Turabian StyleHussein, Said, Chloe Ahryung Lim, Thulasie Manokaran, Shireen Kassam, Madalene Earp, Patricia A. Tang, Safiya Karim, Patricia Biondo, Sharon M. Watanabe, Aynharan Sinnarajah, and et al. 2024. "Colorectal Cancer Patients’ Reported Frequency, Content, and Satisfaction with Advance Care Planning Discussions" Current Oncology 31, no. 3: 1235-1245. https://doi.org/10.3390/curroncol31030092
APA StyleHussein, S., Lim, C. A., Manokaran, T., Kassam, S., Earp, M., Tang, P. A., Karim, S., Biondo, P., Watanabe, S. M., Sinnarajah, A., Tan, A., & Simon, J. (2024). Colorectal Cancer Patients’ Reported Frequency, Content, and Satisfaction with Advance Care Planning Discussions. Current Oncology, 31(3), 1235-1245. https://doi.org/10.3390/curroncol31030092