1. Introduction
Sex and gender were found to significantly interact with social determinants of health, including socioeconomic status, education, geography, and employment. Ultimately, such factors underpin disparities in access to healthcare and the quality of the care provided [
1,
2,
3,
4]. Sex, which refers to biological, genetic, and physiologic characteristics distinguishing males and females, can be differentiated from ‘gender,’ which refers to socially constructed identities [
5,
6]. While it is clear that within intersectional frameworks, sex and gender impact health outcomes, there is a paucity of data regarding such relationships in the palliative care literature [
6,
7].
Quality indicators allow for an understanding of appropriateness, cost-effectiveness, and quality of patient care [
8,
9,
10]. When considering health inequities, such quality indicators become particularly important to discern whether certain groups may be disadvantaged. The identification of inequalities can foster a thoughtful approach to identifying root causes, initiating change, and tracking change over time [
4]. Within palliative care, in cases where patients are diagnosed with advanced and incurable cancer, quality indicators are used to measure whether patients receive supportive care for symptom management or potentially unwanted aggressive care in the last days of life [
8,
9]. Aggressive care, such as chemotherapy, emergency department visits, or admission to a hospital or an intensive care unit within the last weeks of life, is felt to be likely incongruent with clinical status and potentially indicative of inappropriate resource allocation or inadequate access to appropriate care planning and palliative supports [
11]. Further, studies showed that such potentially inappropriate care at EOL is associated with the poorer well-being of relatives in the bereavement period [
12]. Studies of the quality of end-of-life (EOL) care have previously demonstrated disparities between sexes and genders, with the male sex often being associated with the receipt of more aggressive care [
11,
13,
14,
15]; however, none of these studies directly compared rates of quality indicators by sex.
Our objective was to examine the impact of sex on the receipt of aggressive or supportive EOL care through a secondary analysis of previously published data in patients with gastrointestinal (GI) malignancies [
16]. We found that overall, the quality of EOL care varies according to sex, with a smaller proportion of females experiencing aggressive EOL care.
3. Results
In total, 29,529 females and 40,454 males were included in the study (
Table 1). A breakdown of the study population by year is available in
Table A3. A larger proportion of women were aged 80 years or older at the time of death [
30]. Some differences were noted between sexes in income quintile, rurality, DCCI, and survival, though standardized differences were small. GI malignancy type varied according to sex, with a greater proportion of females diagnosed with colorectal, gallbladder, and pancreatic cancers, while a greater proportion of males were diagnosed with esophageal and liver cancer.
3.1. Quality Indicators
In comparing quality indicators (
Table 2), a smaller percentage of females died in an acute care hospital bed compared to males (38.0% vs. 43.2%, SD = 0.11), though similar proportions of females and males received a palliative care service within the last year of life (93.3%, vs. 92.8%, SD = 0.02).
Of patients not hospitalized in the last 30 days of life, significantly fewer proportions of females had a new hospital admission in the last 30 days of life (47.2% vs. 54.4%, SD = 0.15), though there were no significant differences found between sexes with regards to new ICU admissions or palliative care homecare services.
Of patients not hospitalized in the last 14 days of life, again, a smaller proportion of females were found to have any ED visits (29.9% vs. 37.7%, SD = 0.17). However, there were no significant differences found between sexes in chemotherapy use or the receipt of a physician house call.
Quality indicator aggregates (
Table 3) showed that, overall, a smaller proportion of females experienced aggressive care at EOL (14.3% vs. 19.0%, SD = 0.13), with a smaller proportion having at least two ED visits in the last 30 days of life (11.9% vs. 15.7%, SD = 0.11). Differences in hospitalizations and ICU admissions in the last 30 days of life were not significant. Despite the differences seen in the receipt of aggressive EOL care, there were no significant differences between sexes in receiving supportive care at EOL.
3.2. Trends over Time
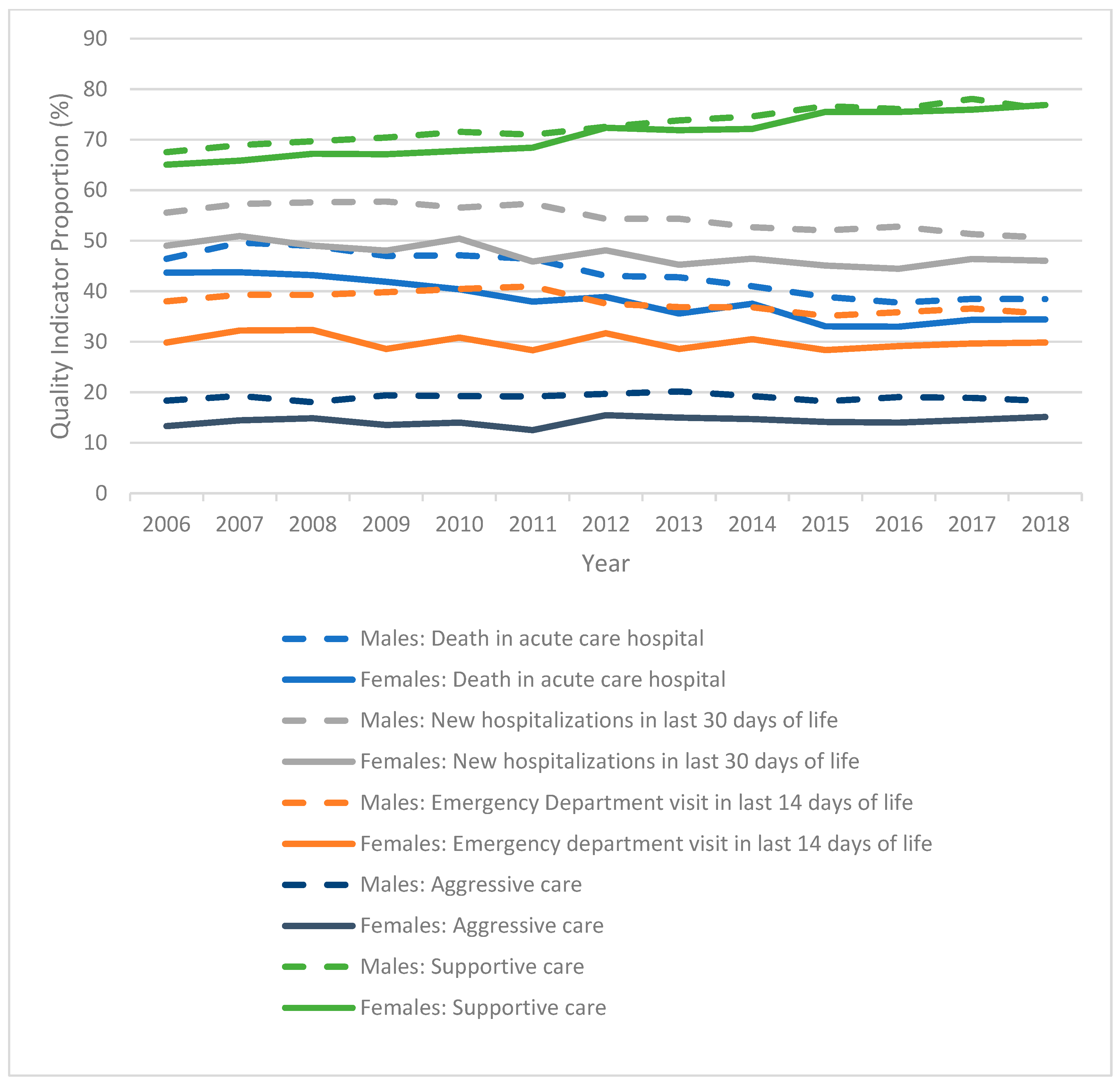
Trends for individual and aggregate indicators of aggressive and supportive EOL care are shown in
Figure 1. For both sexes, rates of death in an acute care hospital bed (
p < 0.001) and new hospitalizations (
p < 0.001) in the last 30 days of life significantly decreased over time. For males, the rate of ED visits in the last 14 days of life decreased over time (
p < 0.001), but there was no significant change seen for females (
p = 0.072). There was no significant change in rates of aggressive EOL care for either sex (
p = 0.186 for females,
p = 0.833 for males), but rates of supportive EOL care increased for both sexes over the study period (
p < 0.001).
3.3. Factors Associated with Aggressive and Supportive Care
Results of the multivariable logistic regression models of aggregate quality indicators, both aggressive and supportive care, are shown by sex in
Table 4 and
Table 5, respectively. The odds of receiving either aggressive care or supportive care varied between sexes according to age at death, survival, cancer type, and income quintile.
Females aged 18–39 had significantly increased odds of aggressive EOL care, while there was no age bracket for males with such an association. For both sexes, being over the age of 60 was associated with reduced odds of aggressive EOL care. The comorbidity index was found not to be associated with aggressive care for either sex; however, females with a comorbidity score of 1 or more had significantly reduced odds of supportive EOL care.
There was considerable variability by cancer type in association with odds of aggressive or supportive EOL care. For females, all cancer types were associated with increased odds of aggressive EOL care when compared to anal and colorectal cancers, while for men, such an association was only found for esophageal, liver, and gastric cancers. For both males and females, gallbladder/biliary cancers, pancreatic cancers, and gastric cancers were associated with increased odds of supportive EOL care.
The income quintile was not significantly associated with the odds of receiving aggressive care for females, but there was an association between lower income quintiles (quintiles 1–3) and aggressive care for males. Both males and females in the lowest two income quintiles had reduced odds of experiencing supportive EOL care. Residency in a rural area was found to be associated with increased odds of supportive EOL care and aggressive EOL care for both sexes. A later year of death within the study period was found to be associated with increased odds of receiving supportive care at the end of life, though there was no such association between receipt of aggressive care and year of death.
4. Discussion
This secondary analysis elaborates on our previous work and highlights sex-based differences in aggressive and supportive EOL care in patients with GI malignancies. Generally, rates of aggressive care remained stable over time, while rates of supportive care increased for both sexes. However, significantly more males experienced aggressive EOL care when compared to females. Further, our previous work found that younger age, residency in the three lowest-income quintile neighbourhoods, and rurality were associated with increased odds of experiencing aggressive care at EOL. However, sex was not included as a predictor in this model [
16]. In this secondary analysis, we found that the female population may be driving the associations between increased odds of aggressive care at EOL and younger age. Conversely, the male population may strongly contribute to the association between aggressive care EOL and lower income quintiles.
More generally, females experienced less aggressive care at EOL, when compared to males. This greater resource intensity of EOL care for males is generally consistent with other studies that showed males are more likely to experience aggressive care at EOL [
11,
13,
15,
29]. The lack of significant difference between sexes in the use of supportive EOL care is somewhat surprising, given a number of studies showing that females are more likely to prefer palliative care in the context of serious illness [
13,
31,
32]. Other studies found that females are more likely to understand that their disease is incurable [
33] and be aware of palliative care [
34]. Such preferences and insight into prognosis would typically be necessary to arrange home care or a physician house call, which were used as indices of supportive EOL care in our study.
We found an association between younger age and increased odds of aggressive EOL care in females, yet not males. Other social factors not captured in our data may be driving this association. Previous research found reduced odds of aggressive care at EOL in older age cohorts regardless of sex [
11,
14,
15,
35]. One study of patients with hematologic and solid tumour malignancies found that female sex and age ≤45 years were associated with receipt of chemotherapy in the last 14 days of life, another indicator of aggressive EOL care [
36]. Similarly, a study of lung cancer decedents found a stronger association between aggressive care at EOL and females under age 50, as compared to males [
37]. While the multivariable logistic regression model accounted for cancer type, comorbidities, rurality, and income, we did not capture other relevant social variables, such as family status, children, and traditional gender roles, that may influence treatment received. Previous studies showed that family status and gender roles do influence preferences for treatment in patients with cancer [
38,
39,
40].
We also found an association between aggressive care at EOL and lower income quintile for males, yet not females, though the differences were only marginally different, making the true significance difficult to interpret. A study of US patients found that while income was not associated with treatment preferences, lower education level was noted to be associated with a desire for more aggressive care [
41]. It is possible that a lower income quintile is a surrogate marker of education level for males. The same relationship, however, may not appear for females, who, despite education level, may have lower incomes due to the longstanding gender wage gap in addition to traditional gender norms driving increased caregiver responsibilities and less income-generating work outside the home [
42,
43]. Other studies showed an association between increased risk of aggressive EOL care and lower income [
16,
44,
45,
46], though, to our knowledge, this is the first study to directly compare how income may affect the aggressiveness of care for each sex.
As with our initial analysis, this study is limited by the retrospective and observational nature of our study design. The use of data from a single province may limit generalizability. The use of administrative data also creates some limitations in collecting other relevant data on gender identity, intersex individuals, and how sex and gender intersect with other social determinants. Factors impacting end-of-life decision-making, such as patient preferences, family preferences, and doctor–patient communication, are also missing, nor did this study investigate congruence between advance care planning and the end-of-life care received. Lastly, our definitions of aggressive and supportive care do not capture the entire realm of elements within aggressive and supportive care, so we are only able to provide a partial picture.
Future studies would benefit from the collection of a full spectrum of social determinants of health, gender identity, and sex. An analysis of the relationship between supportive and aggressive care interventions would allow us to better examine how supportive care interventions may decrease potentially inappropriate, aggressive EOL care, particularly within populations facing health inequities.

 ,
, 
{kind=link}
