Paraneoplastic Syndromes in Neuroendocrine Prostate Cancer: A Systematic Review

Abstract
1. Introduction
2. Materials and Methods
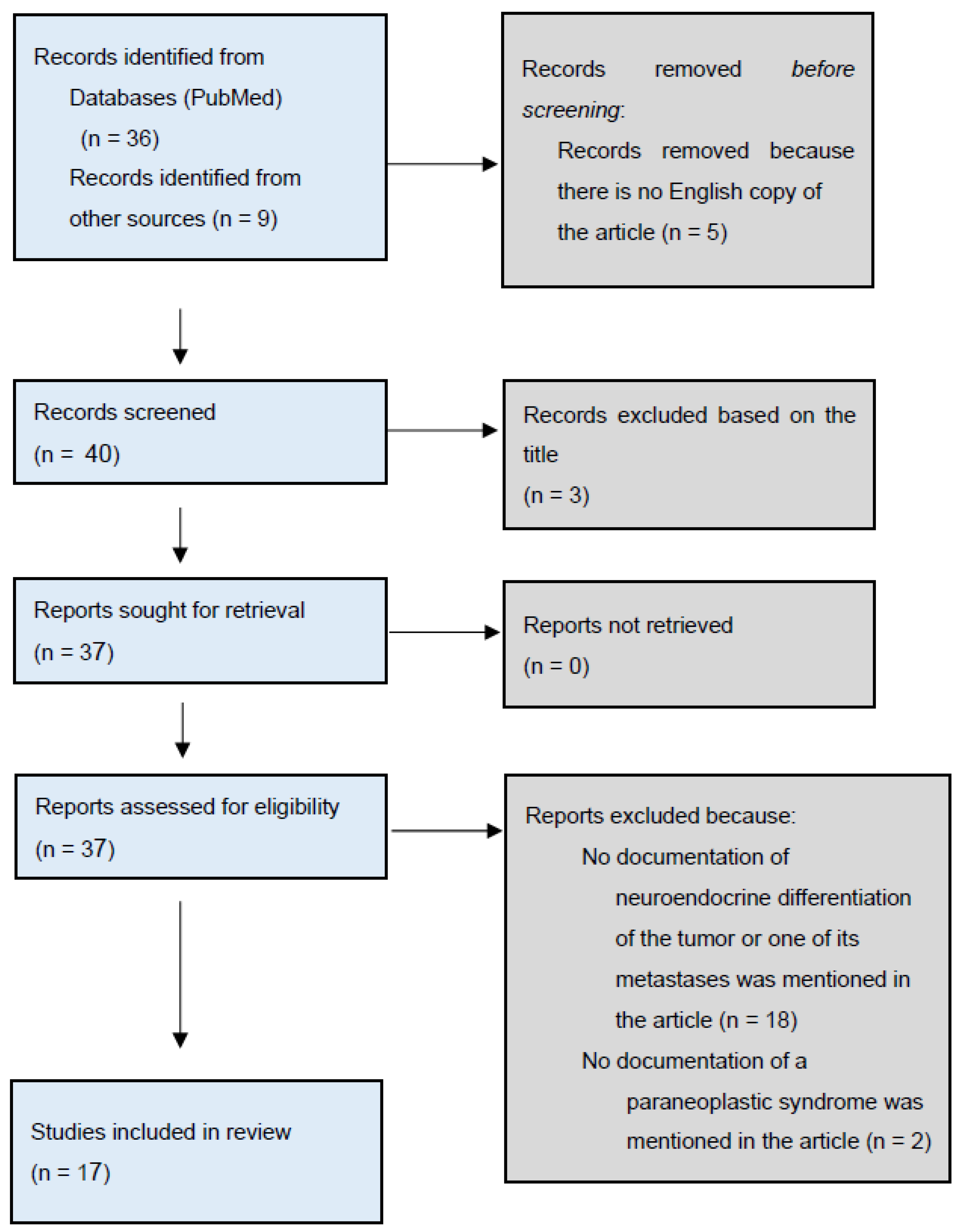
2.1. Literature Search
2.2. Inclusion Criteria
2.3. Study Selection and Data Extraction
2.4. Quality Assessment
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Yamada, Y.; Beltran, H. Clinical and Biological Features of Neuroendocrine Prostate Cancer. Curr. Oncol. Rep. 2021, 23, 15. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, Y.; Ci, X.; Choi, S.Y.C.; Crea, F.; Lin, D.; Wang, Y. Molecular events in neuroendocrine prostate cancer development. Nat. Rev. Urol. 2021, 18, 581–596. [Google Scholar] [CrossRef] [PubMed]
- Spetsieris, N.; Boukovala, M.; Patsakis, G.; Alafis, I.; Efstathiou, E. Neuroendocrine and Aggressive-Variant Prostate Cancer. Cancers 2020, 12, 3792. [Google Scholar] [CrossRef]
- Gupta, K.; Gupta, S. Neuroendocrine differentiation in prostate cancer: Key epigenetic players. Transl. Cancer Res. 2017, 6 (Suppl. S1), S104–S108. [Google Scholar] [CrossRef]
- Aparicio, A.; Logothetis, C.J.; Maity, S.N. Understanding the lethal variant of prostate cancer: Power of examining extremes. Cancer Discov. 2011, 1, 466–468. [Google Scholar] [CrossRef] [PubMed]
- Kaltsas, G.; Androulakis, I.I.; de Herder, W.W.; Grossman, A.B. Paraneoplastic syndromes secondary to neuroendocrine tumours. Endocr. Relat. Cancer 2010, 17, R173–R193. [Google Scholar] [CrossRef] [PubMed]
- Sacco, E.; Pinto, F.; Sasso, F.; Racioppi, M.; Gulino, G.; Volpe, A.; Bassi, P. Paraneoplastic Syndromes in Patients with Urological Malignancies. Urol. Int. 2009, 83, 1–11. [Google Scholar] [CrossRef]
- Cerra-Franco, J.A.; Fernandez-Cruz, C.; Estremera-Marcial, R.; Pagan-Torres, H.; Martinez-Souss, J.; Toro, D.H. Anti-Hu-mediated paraneoplastic chronic intestinal pseudo-obstruction arising from small cell prostate cancer. ACG Case Rep. J. 2019, 6, e00105. [Google Scholar] [CrossRef]
- Papagoras, C.; Arelaki, S.; Botis, I.; Chrysafis, I.; Giannopoulos, S.; Skendros, P. Co-occurrence of dermatomyositis and polycythemia unveiling rare de Novo neuroendocrine prostate tumor. Front. Oncol. 2018, 8, 534. [Google Scholar] [CrossRef]
- Murphy, N.; Shen, J.; Shih, A.; Liew, A.; Khalili, H.; Yaskiv, O.; Katona, K.; Lee, A.; Zhu, X.-H. Paraneoplastic syndrome secondary to treatment emergent neuroendocrine tumor in metastatic castration-resistant prostate cancer: A unique case. Clin. Genitourin. Cancer 2019, 17, e56–e60. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Henry, K. Paraneoplastic syndromes: Definitions, classification, pathophysiology and principles of treatment. Semin. Diagn. Pathol. 2019, 36, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Aromataris, E.; Munn, Z. Introduction to Scoping Reviews. In JBI Manuals for Evidence Synthesis; JBI: Adelaide, Australia, 2020; pp. 2018–2021. Available online: https://synthesismanual.jbi.global (accessed on 24 February 2024).
- Elston, M.S.; Crawford, V.B.; Swarbrick, M.; Dray, M.S.; Head, M.; Conaglen, J.V. Severe Cushing’s syndrome due to small cell prostate carcinoma: A case and review of literature. Endocr. Connect. 2017, 6, R80–R86. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Klomjit, N.; Rowan, D.J.; Kattah, A.G.; Bancos, I.; Taler, S.J. New-onset resistant hypertension in a newly diagnosed prostate cancer patient. Am. J. Hypertens. 2019, 32, 1214–1217. [Google Scholar] [CrossRef]
- Zeng, W.; Khoo, J. Challenging case of ectopic ACTH secretion from prostate adenocarcinoma. Case Rep. Endocrinol. 2022, 2022, 3739957. [Google Scholar] [CrossRef] [PubMed]
- Hassan, B.; Yazbeck, Y.; Akiki, V.; Salti, I.; Tfayli, A. ACTH-secreting metastatic prostate cancer with neuroendocrine differentiation. BMJ Case Rep. 2022, 15, e247997. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.; Triay, J. Ectopic adrenocorticotrophic hormone syndrome secondary to treatment-related neuroendocrine differentiation of metastatic castrate-resistant prostate cancer. Endocrinol. Diabetes Metab. Case Rep. 2023, 2023, 22-0347. [Google Scholar] [CrossRef]
- Feffer, J.B.; Branis, N.M.; Albu, J.B. Dual paraneoplastic endocrine syndromes heralding onset of extrapulmonary small cell carcinoma: A case report and narrative review. Front. Endocrinol. 2018, 9, 170. [Google Scholar] [CrossRef]
- Soundarrajan, M.; Zelada, H.; Fischer, J.V.; Kopp, P. Ectopic Adrenocorticotropic Hormone Syndrome Due to Metastatic Prostate Cancer with Neuroendocrine Differentiation. AACE Clin. Case Rep. 2019, 5, e192–e196. [Google Scholar] [CrossRef]
- Schepers, L.M.; Kisters, J.M.H.; Wetzels, C.; Creemers, G.J. Hypokalaemia and peripheral oedema in a Cushingoid patient with metastatic prostate cancer. Neth. J. Med. 2020, 78, 401–403. [Google Scholar]
- Fernandes, R.; Santos, J.D.; Reis, F.; Monteiro, S. Cushing syndrome as a manifestation of neuroendocrine prostate cancer: A rare presentation within a rare tumor. Cureus 2021, 13, e18160. [Google Scholar] [CrossRef]
- Montes, M.R.; Calvo, P.A.; Sánchez, J.A.G. Small cell metastatic prostate cancer with ectopic adrenocorticotropic hormone hypersecretion: A case report. Ann. Palliat. Med. 2021, 10, 12911–12914. [Google Scholar] [CrossRef]
- Peverelli, G.; Grassi, P. Pure small cell recurrent prostate cancer developing syndrome of inappropriate antidiuretic hormone secretion. Tumori J. 2017, 103 (Suppl. S1), S56–S59. [Google Scholar] [CrossRef]
- Fiordoliva, I.; Marcantognini, G.; Rinaldi, S.; Cimadamore, A.; Montironi, R.; Berardi, R. Syndrome of inappropriate antidiuresis in prostate adenocarcinoma with neuroendocrine differentiation: A case report and literature review. Cancer Metastasis Treat. 2019, 5, 59. [Google Scholar] [CrossRef]
- Karray, O.; Tolner, S.; Yarak, N.; Cherfan, M.; Cosma, M.D.; Sleiman, W.; Niclot, P.; Dubost, J.L.; Coloby, P.; Bart, S. Rare paraneoplastic syndrome of prostatic cancer: Limbic encephalitis: A case report. J. Med. Case Rep. 2021, 15, 405. [Google Scholar] [CrossRef]
- Sidda, A.; Manu, G.; Abdallah, M.; Griswold, D.; Alsharedi, M.; Pacioles, T. Paraneoplastic Evans Syndrome in a Patient with Prostate Cancer with Small Cell Transformation. Cureus 2022, 14, e24505. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.S.; Takahashi, K.; Duane, R.T.; Payne, R.; Liu, C.-K. Primary Thrombocytopenic Purpura and Acquired Hemolytic Anemia: Evidence for a Common Etiology. AMA Arch. Intern. Med. 1951, 87, 48–65. [Google Scholar] [CrossRef] [PubMed]
- Hong, M.K.; Kong, J.; Namdarian, B.; Longano, A.; Grummet, J.; Hovens, C.M.; Costello, A.J.; Corcoran, N.M. Paraneoplastic syndromes in prostate cancer. Nat. Rev. Urol. 2010, 7, 681–692. [Google Scholar] [CrossRef] [PubMed]
- Newell-Price, J.; Trainer, P.; Besser, M.; Grossman, A. The diagnosis and differential diagnosis of Cushing’s syndrome and pseudo-Cushing’s states. Endocr. Rev. 1998, 19, 647–672. [Google Scholar] [CrossRef] [PubMed]
- Nadal, R.; Schweizer, M.; Kryvenko, O.N.; Epstein, J.I.; Eisenberger, M.A. Small cell carcinoma of the prostate. Nat. Rev. Urol. 2014, 11, 213–219. [Google Scholar] [CrossRef]
- Hirano, D.; Okada, Y.; Minei, S.; Takimoto, Y.; Nemoto, N. Neuroendocrine differentiation in hormone refractory prostate cancer following androgen deprivation therapy. Eur. Urol. 2004, 45, 586–592; discussion 592. [Google Scholar] [CrossRef]
- Huang, J.; Yao, J.L.; di Sant’Agnese, P.A.; Yang, Q.; Bourne, P.A.; Na, Y. Immunohistochemical characterization of neuroendocrine cells in prostate cancer. Prostate 2006, 66, 1399–1406. [Google Scholar] [CrossRef] [PubMed]
- Isidori, A.M.; Lenzi, A. Ectopic ACTH syndrome. Arq. Bras. Endocrinol. Metabol. 2007, 51, 1217–1225. [Google Scholar] [CrossRef]
- Alexandraki, K.I.; Grossman, A.B. Therapeutic Strategies for the Treatment of Severe Cushing’s Syndrome. Drugs 2016, 76, 447–458. [Google Scholar] [CrossRef]
- Nieman, L.K.; Biller, B.M.K.; Findling, J.W.; Murad, M.H.; Newell-Price, J.; Savage, M.O.; Tabarin, A. Treatment of Cushing’s Syndrome: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2015, 100, 2807–2831. [Google Scholar] [CrossRef]
- Sarlis, N.J.; Chanock, S.J.; Nieman, L.K. Cortisolemic indices predict severe infections in Cushing syndrome due to ectopic production of adrenocorticotropin. J. Clin. Endocrinol. Metab. 2000, 85, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Pelosof, L.C.; Gerber, D.E. Paraneoplastic Syndromes: An Approach to Diagnosis and Treatment. Mayo Clin. Proc. 2010, 85, 838–854. [Google Scholar] [CrossRef]
- Manger, B.; Schett, G. Rheumatic paraneoplastic syndromes—A clinical link between malignancy and autoimmunity. Clin. Immunol. 2018, 186, 67–70. [Google Scholar] [CrossRef]
- Tandon, R.; Goel, P.; Kataria, S.; Saha, P.K.; Punia, R.P.S.; Dimri, K. Paraneoplastic erythrocytosis in a malignant ovarian steroid cell tumour. Indian J. Hematol. Blood Transfus. 2014, 30, 54–55. [Google Scholar] [CrossRef] [PubMed]
- Kitayama, H.; Kondo, T.; Sugiyama, J.; Hirayama, M.; Oyamada, Y.; Tsuji, Y. Paraneoplastic Erythrocytosis of Colon Cancer, with Serum Erythropoietin within the Normal Reference Range. Am. J. Case Rep. 2016, 17, 417–420. [Google Scholar] [CrossRef][Green Version]
- Dalmau, J.; Rosenfeld, M.R. Paraneoplastic syndromes of the CNS. Lancet Neurol. 2008, 7, 327–340. [Google Scholar] [CrossRef]
- Lennon, V.A.; Sas, D.F.; Busk, M.F.; Scheithauer, B.; Malagelada, J.-R.; Camilleri, M.; Miller, L.J. Enteric neuronal autoantibodies in pseudoobstruction with small-cell lung carcinoma. Gastroenterology 1991, 100, 137–142. [Google Scholar] [CrossRef]
- Li, Q.; Michel, K.; Annahazi, A.; Demir, I.E.; Ceyhan, G.O.; Zeller, F.; Komorowski, L.; Stöcker, W.; Beyak, M.J.; Grundy, D.; et al. Anti-Hu antibodies activate enteric and sensory neurons. Sci. Rep. 2016, 6, 38216. [Google Scholar] [CrossRef]
- Di Nardo, G.; Karunaratne, T.B.; Frediani, S.; De Giorgio, R. Chronic intestinal pseudo-obstruction: Progress in management? Neurogastroenterol. Motil. 2017, 29, e13231. [Google Scholar] [CrossRef]
- Vedeler, C.A.; Antoine, J.C.; Giometto, B.; Graus, F.; Grisold, W.; Hart, I.K.; Honnorat, J.; Smitt, P.A.E.S.; Verschuuren, J.J.G.M.; Voltz, R.; et al. Management of paraneoplastic neurological syndromes: Report of an EFNS Task Force. Eur. J. Neurol. 2006, 13, 682–690. [Google Scholar] [CrossRef]
- Petereit, C.; Zaba, O.; Teber, I.; Lüders, H.; Grohé, C. A rapid and efficient way to manage hyponatremia in patients with SIADH and small cell lung cancer: Treatment with tolvaptan. BMC Pulm. Med. 2013, 13, 55. [Google Scholar] [CrossRef] [PubMed]
- Grohé, C.; Berardi, R.; Burst, V. Hyponatraemia—SIADH in lung cancer diagnostic and treatment algorithms. Crit. Rev. Oncol. Hematol. 2015, 96, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Höftberger, R.; Titulaer, M.J.; Sabater, L.; Dome, B.; Rózsás, A.; Hegedus, B.; Hoda, M.A.; Laszlo, V.; Ankersmit, H.J.; Harms, L.; et al. Encephalitis and GABAB receptor antibodies: Novel findings in a new case series of 20 patients. Neurology 2013, 81, 1500–1506. [Google Scholar] [CrossRef] [PubMed]
- Grisold, W.; Giometto, B.; Vitaliani, R.; Oberndorfer, S. Current approaches to the treatment of paraneoplastic encephalitis. Ther. Adv. Neurol. Disord. 2011, 4, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, J.K.; Zakharia, E.R.; Boysen, A.K.; Andersen, H.; Schlesinger, F.E.; Lund, L. Prostate cancer may trigger paraneoplastic limbic encephalitis: A case report and a review of the literature. Int. J. Urol. 2013, 20, 734–737. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Puthenparambil, J.; Lechner, K.; Kornek, G. Autoimmune hemolytic anemia as a paraneoplastic phenomenon in solid tumors: A critical analysis of 52 cases reported in the literature. Wien. Klin. Wochenschr. 2010, 122, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Michel, M.; Chanet, V.; Dechartres, A.; Morin, A.-S.; Piette, J.-C.; Cirasino, L.; Emilia, G.; Zaja, F.; Ruggeri, M.; Andrès, E.; et al. The spectrum of Evans syndrome in adults: New insight into the disease based on the analysis of 68 cases. Blood 2009, 114, 3167–3172. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Figueroa-Silva, O.; Espasandín-Arias, M.; García-Martínez, F.J.; Fernández-Redondo, V.; Toribio, J. Is it just a psoriasiform dermatitis? Dermatol. Online J. 2017, 23, 18. [Google Scholar] [CrossRef]
- Kazama, A.; Saito, T.; Ishikawa, S.; Takeda, K.; Kobayashi, K.; Tanikawa, T.; Tomita, Y. Small cell prostate cancer producing syndrome of inappropriate secretion of antidiuretic hormone; A case report. Nihon Hinyokika Gakkai Zasshi 2018, 109, 233–236. [Google Scholar] [CrossRef] [PubMed]
- Bost, C.; Chanson, E.; Picard, G.; Meyronet, D.; Mayeur, M.-E.; Ducray, F.; Rogemond, V.; Psimaras, D.; Antoine, J.-C.; Delattre, J.-Y.; et al. Malignant tumors in autoimmune encephalitis with anti-NMDA receptor antibodies. J. Neurol. 2018, 265, 2190–2200. [Google Scholar] [CrossRef]
- Hansen, A.R.; Massard, C.; Ott, P.A.; Haas, N.B.; Lopez, J.S.; Ejadi, S.; Wallmark, J.M.; Keam, B.; Delord, J.-P.; Aggarwal, R.; et al. Pembrolizumab for advanced prostate adenocarcinoma: Findings of the KEYNOTE-028 study. Ann. Oncol. 2018, 29, 1807–1813. [Google Scholar] [CrossRef]
- Hu, J.; He, T.; Jin, L.; Li, Y.; Zhao, Y.; Li, W.; Wei, B.; Mao, X.M.; Lai, Y.Q.; Ni, L.C. Pure small-cell carcinoma of the prostate presenting with increasing prostate-specific antigen levels: A case report and review of the literature. Mol. Clin. Oncol. 2018, 9, 197–200. [Google Scholar] [CrossRef]
- Sekii, Y.; Yoshinaga, M.; Nakagawa, M.; Kishikawa, H.; Oka, K.; Nishimura, K. Development of ectopic adrenocorticotropic hormone syndrome in a patient with prostate cancer during combined androgen blockade therapy. Hinyokika Kiyo 2018, 64, 175–179. [Google Scholar] [CrossRef]
- Miretti, V.S.; Ávila, R.A.; Sierra, J.T.; García, J.J.; Laborié, M.V. Prostate carcinoma and syndrome of inappropriate antidiuretic hormone secretion. Medicina (B Aires) 2018, 78, 290–293. Available online: https://www.ncbi.nlm.nih.gov/pubmed/30125258 (accessed on 24 February 2024).
- Bhangoo, M.S.; Cheng, B.; Botta, G.P.; Thorson, P.; Kosty, M.P. Reversible intrahepatic cholestasis in metastatic prostate cancer: An uncommon paraneoplastic syndrome. Mol. Clin. Oncol. 2018, 8, 609–612. [Google Scholar] [CrossRef]
- Agrawal, K.; Agrawal, N.; Miles, L. Disseminated intravascular coagulation as an initial manifestation of metastatic prostate cancer emergently treated with docetaxel-based chemotherapy. Case Rep. Oncol. Med. 2019, 2019, 6092156. [Google Scholar] [CrossRef]
- Tu, X.; Chang, T.; Nie, L.; Qiu, S.; Xu, H.; Huang, Y.; Bao, Y.; Liu, Z.; Yang, L.; Wei, Q. Large Cell Neuroendocrine Carcinoma of the Prostate: A Systematic Review and Pooled Analysis. Urol. Int. 2019, 103, 383–390. [Google Scholar] [CrossRef]
- Kondo, T.; Igari, R.; Sato, H.; Iseki, C.; Ishizawa, K.; Suzuki, K. Recurrent ataxia and respiratory failure with probable paraneoplastic syndrome responsive to plasma exchange therapy. Rinsho Shinkeigaku 2019, 59, 339–344. [Google Scholar] [CrossRef]
- Layman, A.A.K.; Joshi, S.; Shah, S. Metastatic prostate cancer presenting as tumour-induced osteomalacia. BMJ Case Rep. 2019, 12, e229434. [Google Scholar] [CrossRef] [PubMed]
- Romašovs, A.; Puķītis, A.; Mokricka, V.; Frolova, E. Stauffer’s syndrome in patient with metastatic prostate cancer. Case Rep. Urol. 2019, 2019, 9745301. [Google Scholar] [CrossRef]
- Brock, P.; Alvarez, J.B.; Mortazavi, A.; Roychowdhury, S.; Phay, J.; Khawaja, R.A.; Shah, M.H.; Konda, B. Co-occurrence of multiple endocrine neoplasia type 4 and spinal neurofibromatosis: A case report. Fam. Cancer 2020, 19, 189–192. [Google Scholar] [CrossRef]
- Winther-Larsen, A.; Sandfeld-Paulsen, B.; Hvas, A.-M. Hyperfibrinolysis in Patients with Solid Malignant Neoplasms: A Systematic Review. Semin. Thromb. Hemost. 2020, 47, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Ghafouri, S.R.; Escriba-Omar, A.; Wahdatyar, I.; Whited, N.; Hakim, M.N.; Gaur, S.; Dihowm, F. Exfoliative dermatitis as a para-neoplastic syndrome of prostate adenocarcinoma: A rare case report with literature review. Cancer Diagn. Progn. 2021, 1, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, C.; Amaral, M.; Rodrigues, É.; Silva, R.; Vilão, Ó. Paraneoplastic giant cell arteritis and prostate cancer: A case report of a not common association. Clin. Case Rep. 2021, 9, 1405–1407. [Google Scholar] [CrossRef]
- Lim, J.W.S.; Zhang, W.; Park, D.H.; Premchand, A.X.R. Disseminated intravascular coagulation following femoral nailing in a metastatic prostate carcinoma patient—A case report. Trauma Case Rep. 2021, 36, 100534. [Google Scholar] [CrossRef]
- Sehgal, R.; Virata, A.R.; Bansal, P.; Hart, M. Metastatic Carcinoma of Prostate as a Mimicker of SAPHO Syndrome. Clin. Med. Res. 2021, 19, 141–147. [Google Scholar] [CrossRef]
- Baleiras, M.M.; Maduro, L.; Vasques, C.; Ferreira, F.; Pinto, M.M.; Martins, A. Paraneoplastic dermatomyositis and prostate cancer: Myopathy regression under cancer-directed therapy. Dermatol. Rep. 2021, 13, 9262. [Google Scholar] [CrossRef]
- Greenberg, D.J. Disseminated intravascular coagulation as the initial presentation of metastatic prostate adenocarcinoma. Cureus 2021, 13, e14845. [Google Scholar] [CrossRef]
- Mitchell, A.P.; Meza, A.M.; Panageas, K.S.; Lipitz-Snyderman, A.; Bach, P.B.; Morris, M.J. Real-world use of bone-modifying agents in metastatic castration-sensitive prostate cancer. J. Natl. Cancer Inst. 2022, 114, 419–426. [Google Scholar] [CrossRef]
- He, T.; Zhang, Y.; Li, X.; Liu, C.; Zhu, G.; Yin, X.; Zhang, Z.; Zhao, K.; Wang, Z.; Zhao, P.; et al. Collective analysis of the expression and prognosis for LEM-domain proteins in prostate cancer. World J. Surg. Oncol. 2022, 20, 174. [Google Scholar] [CrossRef] [PubMed]
- Apiraksattayakul, N.; Songwisit, S.; Owattanapanich, W.; Tisavipat, N.; Siritho, S.; Prayoonwiwat, N.; Rattanathamsakul, N.; Jitprapaikulsan, J. AQP4-IgG-positive neuromyelitis optica spectrum disorder and temporally detected neoplasms: Case report and systematic review. Mult. Scler. Relat. Disord. 2022, 68, 104212. [Google Scholar] [CrossRef] [PubMed]
- Constante, M.; Barradas, A.R.; Esteves, A.L.; Pereira, S.; Silva, L. Dermatomyositis: A cancer red flag. Cureus 2022, 14, e32502. [Google Scholar] [CrossRef] [PubMed]
- Alçada, M.; Gaspar, V.; Cunha, G.; Manata, J.P.; Roque, F. Synchronous Double Primary Cancer Complicated with Severe Hypercalcemia. Cureus 2023, 15, e44272. [Google Scholar] [CrossRef] [PubMed]
- Jatoi, A.; Haider-Badenhorst, Y. A Rare Case of Primary Hyperparathyroidism and Hypercalcemia of Malignancy Seen in a Patient with Prostate Adenocarcinoma. Cureus 2023, 15, e43497. [Google Scholar] [CrossRef] [PubMed]
- Santandreu-Morales, I.; Redondo-Cerezo, E.; Martín-Enguix, D. Non-obstructive jaundice as paraneoplastic syndrome of prostate carcinoma: Systematic review of published cases. Med. Clin. 2023, 160, 206–212. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Question 1 | Question 2 | Question 3 | Question 4 | Question 5 | Question 6 | Question 7 | Question 8 | Score |
|---|---|---|---|---|---|---|---|---|---|
| Elston et al. (2017) [14] | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | 7.5/8 |
| Klomjit et al. (2019) [15] | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | 7.5/8 |
| Zeng et al. (2022) [16] | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | 7.5/8 |
| Hassan et al. (2022) [17] | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | 7.5/8 |
| Tan et al. (2023) [18] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8/8 |
| Feffer et al. (2018) [19] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8/8 |
| Soundarrajan et al. (2019) [20] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8/8 |
| Murphy et al. (2019) [10] | Yes | Yes | No | Yes | Yes | Yes | Unclear | Yes | 6.5/8 |
| Schepers et al. (2020) [21] | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | 7.5/8 |
| Fernandes et al. (2021) [22] | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | 7.5/8 |
| Riaza Montes et al. (2021) [23] | Yes | Yes | Yes | Yes | Yes | No | Unclear | Yes | 6.5/8 |
| Papagoras et al. (2018) [9] | Yes | Yes | Yes | Yes | No | Unclear | Unclear | Yes | 6/8 |
| Cerra-Franco et al. (2019) [8] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | 7.5/8 |
| Peverelli et al. (2017) [24] | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | 7.5/8 |
| Fiordoliva et al. (2019) [25] | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | 7.5/8 |
| Karray et al. (2021) [26] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 8/8 |
| Sidda et al. (2022) [27] | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | 7.5/8 |
| Author | Patient Age | Presentation | Paraneoplastic Syndrome | Treatment of the Paraneoplastic Syndrome | Prior Androgen Deprivation Therapy | PSA Levels at the Time of Presentation of Paraneoplastic Syndrome | Histology (Site of Sample) | Mortality |
|---|---|---|---|---|---|---|---|---|
| Elston et al. (2017) [14] | 71 | Hypokalemia, edema and new onset hypertension | Cushing’s Syndrome | Ketoconazole, Metyrapone, Spironolactone, Potassium supplementation | No | Normal | De novo high-grade (Gleason 5 + 5) acinar adenocarcinoma and a small-cell NE PC. (prostate) | After 9 months |
| Klomjit et al. (2019) [15] | 69 | Progressive bilateral lower leg edema, easy bruising, fatigue, generalized weakness and new onset severe resistant hypertension | Cushing’s Syndrome | Urgent bilateral adrenalectomy to control severe hypercortisolism, Spironolactone and antihypertensives | No | Normal | De novo Small cell NE PC with a small percentage of prostatic adenocarcinoma (prostate) | After 1 month from the progression of cancer |
| Zeng et al. (2022) [16] | 61 | Recurrent hypokalemia, lower limb weakness, and edema | Cushing’s Syndrome | Ketoconazole, Potassium supplementation, Spironolactone, antihypertensives, Metformin and Sitagliptin and Octreotide | Yes | Elevated | Acinar adenocarcinoma of the prostate with NE differentiation (prostate) | After 3 months. |
| Hassan et al. (2022) [17] | early 60′s | Abdominal distention, facial and bilateral upper limb and lower limb edema | Cushing’s Syndrome | Spironolactone and Mitotane | Yes | - | High-grade prostate adenocarcinoma with NE differentiation (Liver mets) | Due to multiple infections. |
| Tan et al. (2023) [18] | 64 | Recurrent fluid overload, severe hypokalemia with metabolic alkalosis and loss of glycemic control. | Cushing’s Syndrome | Ketoconazole, Cabergoline, fluid restriction, Spironolactone, Furosemide, Potassium replacement and Apixaban (replaced then with warfarin), Metformin and Insulin | Yes | Elevated | Prostate adenocarcinoma with NE differentiation. * (prostate) | Within 2 weeks from progression of cancer |
| Feffer et al. (2018) [19] | 56 | Clogged nephrostomy tubes | Cushing’s syndrome and PTHrP-mediated hypercalcemia | Pamidronate, Ketoconazole, Spironolactone, Insulin, and anti-hypertensives | Yes | - | High-grade small cell carcinoma (Liver mets) | - |
| Soundarrajan et al. (2019) [20] | 73 | Severe weakness, hyperglycemia, and hypokalemia | Cushing’s Syndrome | Ketoconazole, Metyrapone, Mifepristone, Spironolactone, Amlodipine, Insulin, and stress doses of steroids | Yes | Elevated | Small cell carcinoma (liver mets) and high-grade NE cancer (pleural fluid). | - |
| Murphy et al. (2019) [10] | 63 | Polydipsia, polyuria, and lower limb swelling | Cushing’s Syndrome | Ketoconazole | Yes | Elevated | NE PC (left inguinal lymph node) | After 1 month. |
| Schepers et al. (2020) [21] | 75 | Peripheral edema, metabolic alkalosis, hypokalemia, and hypertension | Cushing’s Syndrome | Ketoconazole, potassium chloride, and Spironolactone | Yes | Elevated | Large cell NE PC (prostate) | After several weeks. |
| Fernandes et al. (2021) [22] | 56 | Pelvic pain, rectal tenesmus, and fatigue | Cushing’s Syndrome | Metyrapone, Potassium supplementation, and anti-hypertensive medication | No | Elevated | De novo Small cell NE PC (prostate) | Within days from nosocomial UTI and multiple organ dysfunction |
| Riaza Montes et al. (2021) [23] | 65 | Acute urinary retention, arterial hypertension, and edema in lower extremities. | Cushing’s Syndrome | Ketoconazole, Etomidate, and potassium chloride | No | Normal | De novo Undifferentiated small cell PC (prostate) | After 21 days from septic shock with multiple organ failure and cardiac arrest |
| Papagoras et al. (2018) [9] | 69 | Facial erythema and symptoms of fatigue | Dermatomyositis and polycthemia | - | No | Elevated | De novo Large cell NE PC (prostate) | After 4 months. |
| Cerra-Franco et al. (2019) [8] | 75 | Worsening abdominal distention, constipation, voiding difficulty, and loss of appetite | Anti-Hu-Mediated Paraneoplastic Chronic Intestinal Pseudo-Obstruction | IV fluids, bowel rest, TPN, and gastrostomy | No | - | De novo Small cell NE PC (prostate) | After 6 weeks. |
| Peverelli et al. (2017) [24] | 71 | Fatigue, dizziness, and hyponatremia | SIADH | IV electrolytes supplementation, Tolvaptan | No | Normal | Prostate adenocarcinoma (Gleason 3 + 3) transformed into small cell PC (prostate) | - |
| Fiordoliva et al. (2019) [25] | 60 | Constipation and mild mental confusion | SIADH | Tolvaptan | Yes | Elevated | Acinar adenocarcinoma with NE differentiation (prostate). Small cell NE carcinoma. (Liver mets) | After 5 months due to liver failure |
| Karray et al. (2021) [26] | 66 | Generalized tonic–clonic seizures, followed by postictal confusion. | Limbic Encephalitis | Antiepileptics, methylprednisolone, Immunoglobulins, cyclophosphamide, and rituximab | Yes | Normal | Small cell NE PC (prostate) | - |
| Sidda et al. (2022) [27] | 63 | Fatigue, hemolytic anemia, and thrombocytopenia | Evans Syndrome | IV methylprednisone and immunoglobulin | Yes | - | Prostatic adenocarcinoma (Gleason 5 + 5) (Prostate). Metastatic PC with transformation to small cell NE carcinoma (Bone marrow) | Within a few days |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abufaraj, M.; Ramadan, R.; Alkhatib, A. Paraneoplastic Syndromes in Neuroendocrine Prostate Cancer: A Systematic Review. Curr. Oncol. 2024, 31, 1618-1632. https://doi.org/10.3390/curroncol31030123
Abufaraj M, Ramadan R, Alkhatib A. Paraneoplastic Syndromes in Neuroendocrine Prostate Cancer: A Systematic Review. Current Oncology. 2024; 31(3):1618-1632. https://doi.org/10.3390/curroncol31030123
Chicago/Turabian StyleAbufaraj, Mohammad, Raghad Ramadan, and Amro Alkhatib. 2024. "Paraneoplastic Syndromes in Neuroendocrine Prostate Cancer: A Systematic Review" Current Oncology 31, no. 3: 1618-1632. https://doi.org/10.3390/curroncol31030123
APA StyleAbufaraj, M., Ramadan, R., & Alkhatib, A. (2024). Paraneoplastic Syndromes in Neuroendocrine Prostate Cancer: A Systematic Review. Current Oncology, 31(3), 1618-1632. https://doi.org/10.3390/curroncol31030123