A Real-World Retrospective Analysis of the Management of Advanced Urothelial Carcinoma in Canada

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Analysis
2.2. Patient Criteria
- Patients must have been diagnosed with unresectable locally advanced or metastatic urothelial carcinoma (aUC), either de novo aUC or as a progression from an earlier stage of UC.
- The diagnosis must have been no earlier than January 2021, to coincide with the availability of new therapeutic options.
- Patients must have received or completed, at the time of data entry, at least one systemic therapy, which should have included first-line platinum-based chemotherapy.
- Patients should not have shown disease progression during first-line platinum-based chemotherapy or within 12 months of neoadjuvant or adjuvant treatment.
2.3. Focus Groups
3. Results
3.1. Participants
3.1.1. Oncologist Demographics
3.1.2. Creatinine Clearance Threshold for Cisplatin Eligibility
3.2. Patient Baseline Demographics and Clinical Charactersistics
3.2.1. Demographics
3.2.2. De Novo aUC vs. Metastatic Progression from Early-Stage Disease
3.2.3. Diagnostic Workup
3.2.4. Cystectomy
3.2.5. Molecular Testing
3.3. Patient Management
3.3.1. Subgroups
3.3.2. Treatment Goals
3.3.3. First-Line Chemotherapy
3.3.4. Surveillance
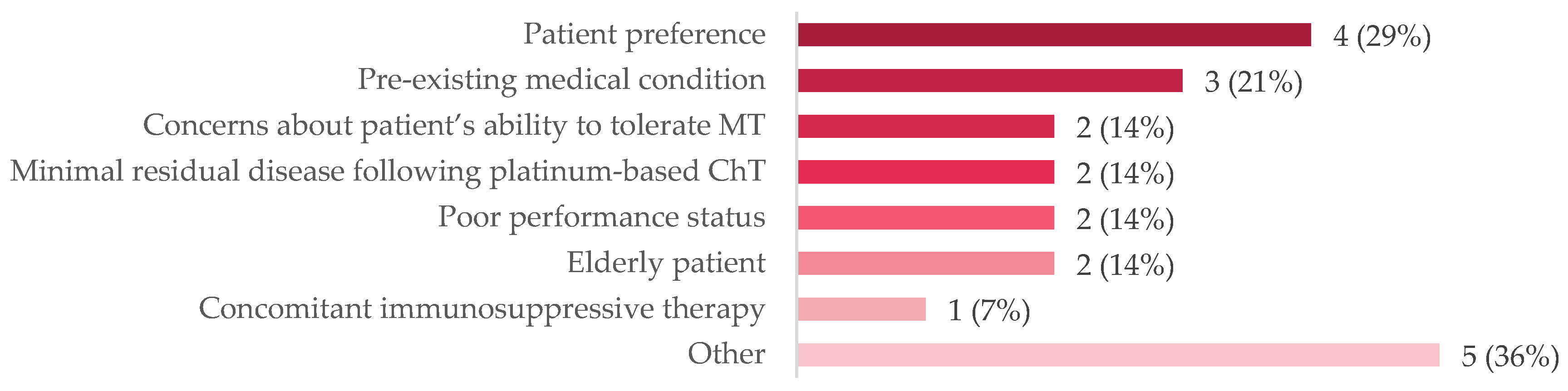
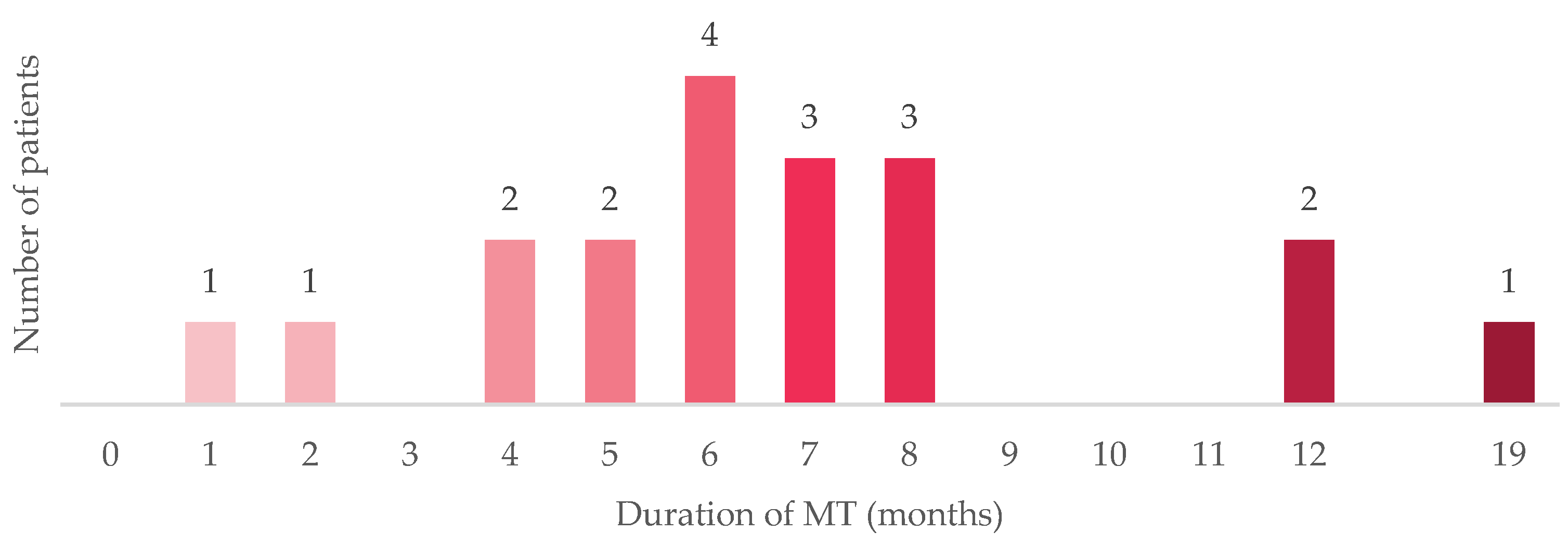
3.3.5. Maintenance Therapy
3.3.6. Second-Line Therapy or Beyond
3.4. Provider Reflections
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Common Cancer Sites—Cancer Stat Facts. Available online: https://seer.cancer.gov/statfacts/html/common.html (accessed on 27 July 2023).
- Brenner, D.R.; Poirier, A.; Woods, R.R.; Ellison, L.F.; Billette, J.-M.; Demers, A.A.; Zhang, S.X.; Yao, C.; Finley, C.; Fitzgerald, N.; et al. Projected Estimates of Cancer in Canada in 2022. Can. Med. Assoc. J. 2022, 194, E601–E607. [Google Scholar] [CrossRef]
- Shariat, S.F.; Sfakianos, J.P.; Droller, M.J.; Karakiewicz, P.I.; Meryn, S.; Bochner, B.H. The Effect of Age and Gender on Bladder Cancer: A Critical Review of the Literature. BJU Int. 2010, 105, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Lenis, A.T.; Lec, P.M.; Chamie, K.; Mshs, M. Bladder Cancer: A Review. JAMA 2020, 324, 1980. [Google Scholar] [CrossRef] [PubMed]
- van Osch, F.H.; Jochems, S.H.; van Schooten, F.-J.; Bryan, R.T.; Zeegers, M.P. Quantified Relations between Exposure to Tobacco Smoking and Bladder Cancer Risk: A Meta-Analysis of 89 Observational Studies. Int. J. Epidemiol. 2016, 45, 857–870. [Google Scholar] [CrossRef] [PubMed]
- Bhindi, B.; Kool, R.; Kulkarni, G.S.; Siemens, D.R.; Aprikian, A.G.; Breau, R.H.; Brimo, F.; Fairey, A.; French, C.; Hanna, N.; et al. Canadian Urological Association Guideline on the Management of Non-Muscle Invasive Bladder Cancer. Can. Urol. Assoc. J. 2021, 15, E424. [Google Scholar] [CrossRef] [PubMed]
- Freedman, N.D.; Silverman, D.T.; Hollenbeck, A.R.; Schatzkin, A.; Abnet, C.C. Association between Smoking and Risk of Bladder Cancer among Men and Women. JAMA 2011, 306, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Saginala, K.; Barsouk, A.; Aluru, J.S.; Rawla, P.; Padala, S.A.; Barsouk, A. Epidemiology of Bladder Cancer. Med. Sci. 2020, 8, 15. [Google Scholar] [CrossRef] [PubMed]
- Soukup, V.; Čapoun, O.; Cohen, D.; Hernández, V.; Babjuk, M.; Burger, M.; Compérat, E.; Gontero, P.; Lam, T.; MacLennan, S.; et al. Prognostic Performance and Reproducibility of the 1973 and 2004/2016 World Health Organization Grading Classification Systems in Non–Muscle-Invasive Bladder Cancer: A European Association of Urology Non-Muscle Invasive Bladder Cancer Guidelines Panel Systematic Review. Eur. Urol. 2017, 72, 801–813. [Google Scholar] [CrossRef] [PubMed]
- Warren, M.; Kolinsky, M.; Canil, C.M.; Czaykowski, P.; Sridhar, S.S.; Black, P.C.; Booth, C.M.; Kassouf, W.; Eapen, L.; Mukherjee, S.D.; et al. Canadian Urological Association Consensus Statement: Management of Unresectable Locally Advanced and Metastatic Urothelial Carcinoma. Can. Urol. Assoc. J. 2019, 13, 318. [Google Scholar] [CrossRef] [PubMed]
- Bellmunt, J.; de Wit, R.; Vaughn, D.J.; Fradet, Y.; Lee, J.-L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; et al. Pembrolizumab as Second-Line Therapy for Advanced Urothelial Carcinoma. N. Engl. J. Med. 2017, 376, 1015–1026. [Google Scholar] [CrossRef]
- Powles, T.; Bellmunt, J.; Comperat, E.; Santis, M.D.; Huddart, R.; Loriot, Y.; Necchi, A.; Valderrama, B.P.; Ravaud, A.; Shariat, S.F.; et al. Bladder Cancer: ESMO Clinical Practice Guideline for Diagnosis, Treatment and Follow-Up☆. Ann. Oncol. 2022, 33, 244–258. [Google Scholar] [CrossRef]
- NCCN Clinical Practice Guidelines in Oncology—Bladder Cancer (Version 3.2023). Available online: https://www.nccn.org/professionals/physician_gls/pdf/bladder.pdf (accessed on 8 August 2023).
- O’Donnell, P.H.; Milowsky, M.I.; Petrylak, D.P.; Hoimes, C.J.; Flaig, T.W.; Mar, N.; Moon, H.H.; Friedlander, T.W.; McKay, R.R.; Bilen, M.A.; et al. Enfortumab Vedotin with or Without Pembrolizumab in Cisplatin-Ineligible Patients with Previously Untreated Locally Advanced or Metastatic Urothelial Cancer. J. Clin. Oncol. 2023, 41, 4107–4117. [Google Scholar] [CrossRef]
- von der Maase, H.; Hansen, S.W.; Roberts, J.T.; Dogliotti, L.; Oliver, T.; Moore, M.J.; Bodrogi, I.; Albers, P.; Knuth, A.; Lippert, C.M.; et al. Gemcitabine and Cisplatin Versus Methotrexate, Vinblastine, Doxorubicin, and Cisplatin in Advanced or Metastatic Bladder Cancer: Results of a Large, Randomized, Multinational, Multicenter, Phase III Study. J. Clin. Oncol. 2000, 18, 3068–3077. [Google Scholar] [CrossRef]
- von der Maase, H.; Sengelov, L.; Roberts, J.T.; Ricci, S.; Dogliotti, L.; Oliver, T.; Moore, M.J.; Zimmermann, A.; Arning, M. Long-Term Survival Results of a Randomized Trial Comparing Gemcitabine plus Cisplatin, with Methotrexate, Vinblastine, Doxorubicin, plus Cisplatin in Patients with Bladder Cancer. J. Clin. Oncol. 2005, 23, 4602–4608. [Google Scholar] [CrossRef]
- Dogliotti, L.; Cartenì, G.; Siena, S.; Bertetto, O.; Martoni, A.; Bono, A.; Amadori, D.; Onat, H.; Marini, L. Gemcitabine plus Cisplatin versus Gemcitabine plus Carboplatin as First-Line Chemotherapy in Advanced Transitional Cell Carcinoma of the Urothelium: Results of a Randomized Phase 2 Trial. Eur. Urol. 2007, 52, 134–141. [Google Scholar] [CrossRef]
- De Santis, M.; Bellmunt, J.; Mead, G.; Kerst, J.M.; Leahy, M.; Maroto, P.; Gil, T.; Marreaud, S.; Daugaard, G.; Skoneczna, I.; et al. Randomized Phase II/III Trial Assessing Gemcitabine/Carboplatin and Methotrexate/Carboplatin/Vinblastine in Patients with Advanced Urothelial Cancer Who Are Unfit for Cisplatin-Based Chemotherapy: EORTC Study 30986. J. Clin. Oncol. 2012, 30, 191–199. [Google Scholar] [CrossRef]
- Powles, T.; Park, S.H.; Voog, E.; Caserta, C.; Valderrama, B.P.; Gurney, H.; Kalofonos, H.; Radulović, S.; Demey, W.; Ullén, A.; et al. Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma. N. Engl. J. Med. 2020, 383, 1218–1230. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Park, S.H.; Caserta, C.; Valderrama, B.P.; Gurney, H.; Ullén, A.; Loriot, Y.; Sridhar, S.S.; Sternberg, C.N.; Bellmunt, J.; et al. Avelumab First-Line Maintenance for Advanced Urothelial Carcinoma: Results From the JAVELIN Bladder 100 Trial after ≥2 Years of Follow-Up. J. Clin. Oncol. 2023, 41, 3486–3492. [Google Scholar] [CrossRef] [PubMed]
- Galsky, M.D.; Hahn, N.M.; Rosenberg, J.; Sonpavde, G.; Hutson, T.; Oh, W.K.; Dreicer, R.; Vogelzang, N.; Sternberg, C.N.; Bajorin, D.F.; et al. Treatment of Patients with Metastatic Urothelial Cancer “Unfit” for Cisplatin-Based Chemotherapy. J. Clin. Oncol. 2011, 29, 2432–2438. [Google Scholar] [CrossRef]
- Kulkarni, G.S.; Black, P.C.; Sridhar, S.S.; Kapoor, A.; Zlotta, A.R.; Shayegan, B.; Rendon, R.; Chung, P.; Van Der Kwast, T.; Alimohamed, N.; et al. Canadian Urological Association Guideline: Muscle-Invasive Bladder Cancer. Can. Urol. Assoc. J. 2019, 13, 230. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Vida, A.; Saggese, M.; Hughes, S.; Rudman, S.; Chowdhury, S.; Smith, N.R.; Lawrence, P.; Rooney, C.; Dougherty, B.; Landers, D.; et al. Complexity of FGFR Signalling in Metastatic Urothelial Cancer. J. Hematol. Oncol. 2015, 8, 119. [Google Scholar] [CrossRef]
- Krook, M.A.; Reeser, J.W.; Ernst, G.; Barker, H.; Wilberding, M.; Li, G.; Chen, H.-Z.; Roychowdhury, S. Fibroblast Growth Factor Receptors in Cancer: Genetic Alterations, Diagnostics, Therapeutic Targets and Mechanisms of Resistance. Br. J. Cancer 2021, 124, 880–892. [Google Scholar] [CrossRef]
- Pietzak, E.J.; Bagrodia, A.; Cha, E.K.; Drill, E.N.; Iyer, G.; Isharwal, S.; Ostrovnaya, I.; Baez, P.; Li, Q.; Berger, M.F.; et al. Next-Generation Sequencing of Nonmuscle Invasive Bladder Cancer Reveals Potential Biomarkers and Rational Therapeutic Targets. Eur. Urol. 2017, 72, 952–959. [Google Scholar] [CrossRef]
- Kang, H.W.; Kim, Y.-H.; Jeong, P.; Park, C.; Kim, W.T.; Ryu, D.H.; Cha, E.-J.; Ha, Y.-S.; Kim, T.-H.; Kwon, T.G.; et al. Expression Levels of FGFR3 as a Prognostic Marker for the Progression of Primary pT1 Bladder Cancer and Its Association with Mutation Status. Oncol. Lett. 2017, 14, 3817–3824. [Google Scholar] [CrossRef] [PubMed]
- Antonuzzo, L.; Maruzzo, M.; De Giorgi, U.; Santini, D.; Tambaro, R.; Buti, S.; Carrozza, F.; Calabrò, F.; Di Lorenzo, G.; Fornarini, G.; et al. READY: Real-World Data from an Italian Compassionate Use Program of Avelumab First-Line Maintenance (1LM) Treatment for Locally Advanced or Metastatic Urothelial Carcinoma (La/mUC). J. Clin. Oncol. 2023, 41, 469. [Google Scholar] [CrossRef]
- Geynisman, D.M.; Broughton, E.; Hao, Y.; Zhang, Y.; Le, T.; Huo, S. Real-World Treatment Patterns and Clinical Outcomes among Patients with Advanced Urothelial Carcinoma in the United States. Urol. Oncol. Semin. Orig. Investig. 2022, 40, e1–e195. [Google Scholar] [CrossRef] [PubMed]
- Bellmunt, J.; Chang, J.; Pavilack-Kirker, M.; Cappelleri, J.C.; Costa, N.; Esterberg, E.; Kearney, M.; Hitchens, A.; Candrilli, S.D.; Ajmera, M. Evaluating Real-World Characteristics of Patients with Advanced Urothelial Carcinoma Eligible for Avelumab Maintenance Therapy: A Multicountry Retrospective Medical Chart Review. Clin. Genitourin. Cancer 2023, 21, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Richards, M.; Anderson, M.; Carter, P.; Ebert, B.L.; Mossialos, E. The Impact of the COVID-19 Pandemic on Cancer Care. Nat. Cancer 2020, 1, 565–567. [Google Scholar] [CrossRef]
- Woods, J.; Elmore, S.N.; Glenn, L.; Maues, J.; James, D.; Roberson, M.L. A Qualitative Study of the Impact of the COVID-19 Pandemic on Metastatic Breast Cancer Care. J. Patient Exp. 2023, 10, 23743735231167973. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, J.D.; Gray, E.; Pashayan, N.; Deandrea, S.; Karch, A.; Vale, D.B.; Elder, K.; Procopio, P.; van Ravesteyn, N.T.; Mutabi, M.; et al. The Impact of the COVID-19 Pandemic on Breast Cancer Early Detection and Screening. Prev. Med. 2021, 151, 106585. [Google Scholar] [CrossRef]
- Fortin, J.; Rivest-Beauregard, M.; Defer, C.; Leblanc, M.; Thamar Louis, L.A.; Roy, C.-A.; Lapierre, I.; Brunet, A.; Montreuil, M.; Marin, M.-F. The Impact of Canadian Medical Delays and Preventive Measures on Breast Cancer Experience: A Silent Battle Masked by the COVID-19 Pandemic. Can. J. Nurs. Res. 2023, 55, 55–67. [Google Scholar] [CrossRef]
- Gavi, F.; Santoro, P.E.; Amantea, C.; Russo, P.; Marino, F.; Borrelli, I.; Moscato, U.; Foschi, N. Impact of COVID-19 on Uro-Oncological Patients: A Comprehensive Review of the Literature. Microorganisms 2023, 11, 176. [Google Scholar] [CrossRef] [PubMed]
- Chen-See, S. Disruption of Cancer Care in Canada during COVID-19. Lancet Oncol. 2020, 21, e374. [Google Scholar] [CrossRef] [PubMed]
- Jiang, D.M.; Gupta, S.; Kitchlu, A.; Meraz-Munoz, A.; North, S.A.; Alimohamed, N.S.; Blais, N.; Sridhar, S.S. Defining Cisplatin Eligibility in Patients with Muscle-Invasive Bladder Cancer. Nat. Rev. Urol. 2021, 18, 104–114. [Google Scholar] [CrossRef]
- Canter, D.; Long, C.; Kutikov, A.; Plimack, E.; Saad, I.; Oblaczynski, M.; Zhu, F.; Viterbo, R.; Chen, D.Y.T.; Uzzo, R.G.; et al. Clinicopathological Outcomes after Radical Cystectomy for Clinical T2 Urothelial Carcinoma: Further Evidence to Support the Use of Neoadjuvant Chemotherapy. BJU Int. 2011, 107, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Haleblian, G.E.; Skinner, E.C.; Dickinson, M.G.; Lieskovsky, G.; Boyd, S.D.; Skinner, D.G. Hydronephrosis as a Prognostic Indicator in Bladder Cancer Patients. J. Urol. 1998, 160, 2011–2014. [Google Scholar] [CrossRef]
- Abufaraj, M.; Dalbagni, G.; Daneshmand, S.; Horenblas, S.; Kamat, A.M.; Kanzaki, R.; Zlotta, A.R.; Shariat, S.F. The Role of Surgery in Metastatic Bladder Cancer: A Systematic Review. Eur. Urol. 2018, 73, 543–557. [Google Scholar] [CrossRef] [PubMed]
- Longo, N.; Celentano, G.; Napolitano, L.; La Rocca, R.; Capece, M.; Califano, G.; Collà Ruvolo, C.; Mangiapia, F.; Fusco, F.; Morra, S.; et al. Metastasis-Directed Radiation Therapy with Consolidative Intent for Oligometastatic Urothelial Carcinoma: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 2373. [Google Scholar] [CrossRef]
- Maráz, A.; Nagy, B.; Macher, T.; Jeskó, J.; Tischler, E.; Csongvai, C.; Kearney, M. Nationwide Study of Real-World Treatment Patterns and Clinical Outcomes in Patients with Metastatic Urothelial Carcinoma in Hungary. Adv. Ther. 2023, 40, 5475–5488. [Google Scholar] [CrossRef]
- Swami, U.; Grivas, P.; Pal, S.K.; Agarwal, N. Utilization of Systemic Therapy for Treatment of Advanced Urothelial Carcinoma: Lessons from Real World Experience. Cancer Treat. Res. Commun. 2021, 27, 100325. [Google Scholar] [CrossRef]
- Powles, T.B.; Valderrama, B.P.; Gupta, S.; Bedke, J.; Kikuchi, E.; Hoffman-Censits, J.; Iyer, G.; Vulsteke, C.; Park, S.H.; Shin, S.J.; et al. LBA6 EV-302/KEYNOTE-A39: Open-Label, Randomized Phase III Study of Enfortumab Vedotin in Combination with Pembrolizumab (EV+P) vs Chemotherapy (Chemo) in Previously Untreated Locally Advanced Metastatic Urothelial Carcinoma (La/mUC). Ann. Oncol. 2023, 34, S1340. [Google Scholar] [CrossRef]
- van der Heijden, M.S.; Sonpavde, G.; Powles, T.; Necchi, A.; Burotto, M.; Schenker, M.; Sade, J.P.; Bamias, A.; Beuzeboc, P.; Bedke, J.; et al. Nivolumab plus Gemcitabine–Cisplatin in Advanced Urothelial Carcinoma. N. Engl. J. Med. 2023, 389, 1778–1789. [Google Scholar] [CrossRef] [PubMed]
- Pal, S.K.; Albiges, L.; Tomczak, P.; Suárez, C.; Voss, M.H.; de Velasco, G.; Chahoud, J.; Mochalova, A.; Procopio, G.; Mahammedi, H.; et al. Atezolizumab plus Cabozantinib versus Cabozantinib Monotherapy for Patients with Renal Cell Carcinoma after Progression with Previous Immune Checkpoint Inhibitor Treatment (CONTACT-03): A Multicentre, Randomised, Open-Label, Phase 3 Trial. Lancet 2023, 402, 185–195. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristics (n = 18) | n | % |
|---|---|---|
| Oncology specialty | ||
| Medical oncologist | 16 | 94 |
| Hematologist oncologist | 1 | 6 |
| Province of practice | ||
| Ontario | 5 | 29 |
| Quebec | 4 | 24 |
| British Columbia | 4 | 24 |
| Alberta | 1 | 6 |
| New Brunswick | 1 | 6 |
| Nova Scotia | 1 | 6 |
| Saskatchewan | 1 | 6 |
| Primary setting of practice | ||
| Academic-/university-affiliated hospital | 14 | 82 |
| Community-based hospital/clinic/practice | 3 | 18 |
| Years practicing oncology | ||
| 0–10 | 9 | 53 |
| 11–20 | 5 | 29 |
| 21–30 | 2 | 12 |
| More than 30 | 1 | 6 |
| Number of new aUC consultations in the last month | ||
| 0 | 0 | 0 |
| 1–2 | 2 | 12 |
| 3–5 | 8 | 47 |
| 5–10 | 7 | 41 |
| More than 10 | 0 | 0 |
| Creatinine clearance threshold for cisplatin eligibility | ||
| 60 mL/min | 3 | 18 |
| 55 mL/min | 1 | 6 |
| 50 mL/min | 12 | 70 |
| 45 mL/min | 1 | 6 |
| Characteristic (n = 146) | n | % |
|---|---|---|
| Male | 106 | 73 |
| Female | 40 | 27 |
| Age, years; median (range) | 71 (38–90) | |
| Year of diagnosis of aUC | ||
| 2021 | 59 | 40 |
| 2022 | 75 | 51 |
| 2023 | 12 | 8 |
| Comorbidities | 93 | 64 |
| Hypertension | 68 | 47 |
| Dyslipidemia | 46 | 32 |
| Chronic kidney disease | 30 | 21 |
| Diabetes | 29 | 20 |
| Atherosclerotic cardiovascular disease | 20 | 14 |
| Obesity/overweight | 8 | 5 |
| Gastrointestinal disease | 6 | 4 |
| Heart failure | 4 | 3 |
| Hearing loss | 4 | 3 |
| Other 1 | 50 | 34 |
| No comorbidities | 53 | 36 |
| History of smoking | ||
| Yes, current | 31 | 21 |
| Yes, former | 77 | 53 |
| No | 38 | 26 |
| Medical history | ||
| De novo aUC | 77 | 53 |
| Progression from an earlier stage of UC | 69 | 47 |
| Symptoms leading de novo aUC diagnosis (n = 77) | ||
| Painless gross hematuria | 19 | 25 |
| Irritative bladder symptoms 2 | 9 | 12 |
| Other 3 | 11 | 14 |
| Cystectomy if progression from earlier stage (n = 69) | ||
| Yes | 32 | 46 |
| No | 37 | 53 |
| Metastatic sites | ||
| Lymph node beyond the common iliacs | 99 | 68 |
| Lung | 55 | 38 |
| Bone | 32 | 22 |
| Liver | 20 | 14 |
| Other 4 | 14 | 10 |
| None (locally advanced unresectable disease) | 3 | 2 |
| FGFR3 mutation | ||
| Not tested 5 or unknown 6 | 87 | 60 |
| Positive | 6 | 4 |
| Negative | 53 | 36 |
| Component, n (%) | All | 1 L ChT (n = 37) | Surveillance (n = 14) | 1 L MT 1 (n = 67) | 2 L + Tx (n = 28) |
|---|---|---|---|---|---|
| 1 L ChT (n = 146) | |||||
| Gem-cis (GC) | 74 (51) | 15 (40) | 3 (21) | 38 (57) | 18 (64) |
| Gem-carb | 68 (47) | 21 (57) | 10 (72) | 28 (42) | 10 (36) |
| MVAC | 0 | 0 | 0 | 0 | 0 |
| ddMVAC | 2 (1) | 0 | 1 (7) | 1 (1) | 0 |
| Other 2 | 1 (1) | 1 (3) | 0 | 0 | 0 |
| Response to 1 L ChT (n = 109) | |||||
| Disease progression | 9 (8) | - | 5 (37) | 1 (1) | 3 (11) |
| Stable disease | 24 (22) | - | 3 (21) | 12 (18) | 9 (32) |
| Partial response | 65 (60) | - | 3 (21) | 46 (69) | 16 (57) |
| Complete response | 11 (10) | - | 3 (21) | 8 (12) | 0 |
| Received MT, n | 85 | - | - | 67 | 18 |
| MT-emergent AEs that were difficult or time-consuming to manage | 8 (9) | - | - | 5 (7) 3 | 3 (17) 4 |
| Timeframe between ChT and MT (n = 122) | |||||
| <4 weeks | 15 (12) | 6 (16) 5 | - | 7 (10) | 2 (11) |
| 4–6 weeks | 64 (53) | 23 (62) 5 | - | 32 (48) | 9 (50) |
| 6–8 weeks | 28 (23) | 5 (14) 5 | - | 18 (27) | 5 (28) |
| 8–10 weeks | 15 (12) | 3 (8) 5 | - | 10 (15) | 2 (11) |
| Duration of MT, median (range) (n = 18) 6 | - | - | - | 6 (<1–19) | |
| Reason for discontinuing MT (n = 18) 6 | |||||
| Disease progression | 17 (94) | - | - | - | 17 (94) |
| Patient preference | 1 (6) | - | - | - | 1 (6) |
| 2 L therapy (n = 28) | - | - | - | ||
| Pembrolizumab or immunotherapy alternative (avelumab, durvalumab) | 11 (39) | - | - | - | 11 (39) |
| Enfortumab-vedotin | 9 (32) | - | - | - | 9 (32) |
| Reinduction with ChT | 1 (4) | - | - | - | 1 (4) |
| Erdafitinib | 1 (4) | - | - | - | 1 (4) |
| Clinical trial | 1 (4) | - | - | - | 1 (4) |
| Other 7 | 5 (17) | - | - | - | 5 (18) |
| 3 L therapy (n = 12) | - | - | - | ||
| Enfortumab-vedotin | 4 (33) | - | - | - | 4 (33) |
| Paclitaxel | 2 (17) | - | - | - | 2 (17) |
| Erdafitinib | 1 (8) | - | - | - | 1 (8) |
| Other 8 | 5 (42) | - | - | - | 5 (42) |
| Reflection (n = 17) | n | % |
|---|---|---|
| Biggest challenges with MT | ||
| Lack of institutional resources (e.g., the ChT clinic already being at capacity) to monitor and manage patients on MT | 57 | 39 |
| Patient reluctance for further treatment (or frequency of treatment) | 52 | 36 |
| Managing treatment-emergent AEs | 46 | 32 |
| Patient or resource factors limiting the ability to start MT within 10 weeks | 8 | 6 |
| Lack of experience with MT | 5 | 3 |
| Lack of access to MT | 0 | 0 |
| Specific actions to implement in coming months | ||
| This chart review has validated my current practice | 81 | 56 |
| I will connect with peer(s) to discuss what I have learned in this chart review | 78 | 54 |
| I will review the latest guidelines | 35 | 24 |
| I will learn more about the management of AEs with MT | 30 | 21 |
| I will attend more educational programs to increase confidence in the management of these patients | 26 | 18 |
| I will gain experience with MT | 25 | 17 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moria, F.A.; Park, C.L.; Eigl, B.J.; Macfarlane, R.; Pavic, M.; Saleh, R.R. A Real-World Retrospective Analysis of the Management of Advanced Urothelial Carcinoma in Canada. Curr. Oncol. 2024, 31, 704-722. https://doi.org/10.3390/curroncol31020052
Moria FA, Park CL, Eigl BJ, Macfarlane R, Pavic M, Saleh RR. A Real-World Retrospective Analysis of the Management of Advanced Urothelial Carcinoma in Canada. Current Oncology. 2024; 31(2):704-722. https://doi.org/10.3390/curroncol31020052
Chicago/Turabian StyleMoria, Feras A., Changsu L. Park, Bernhard J. Eigl, Robyn Macfarlane, Michel Pavic, and Ramy R. Saleh. 2024. "A Real-World Retrospective Analysis of the Management of Advanced Urothelial Carcinoma in Canada" Current Oncology 31, no. 2: 704-722. https://doi.org/10.3390/curroncol31020052
APA StyleMoria, F. A., Park, C. L., Eigl, B. J., Macfarlane, R., Pavic, M., & Saleh, R. R. (2024). A Real-World Retrospective Analysis of the Management of Advanced Urothelial Carcinoma in Canada. Current Oncology, 31(2), 704-722. https://doi.org/10.3390/curroncol31020052