Programmed Cell Death-Ligand 1 Expression and Clinical Outcomes Among Patients with Resected, Early-Stage Non-Small Cell Lung Cancer: A Real-World Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Eligibility Criteria
2.2. Data Source and Study Timeframe
2.3. Study Outcomes
2.4. Data Analysis
2.5. Ethics
3. Results
3.1. PD-L1 Prevalence Cohort
3.2. PD-L1+ Cohort
3.2.1. Patient Demographics and Clinical Characteristics
3.2.2. Disease Recurrence
3.2.3. Treatment Patterns
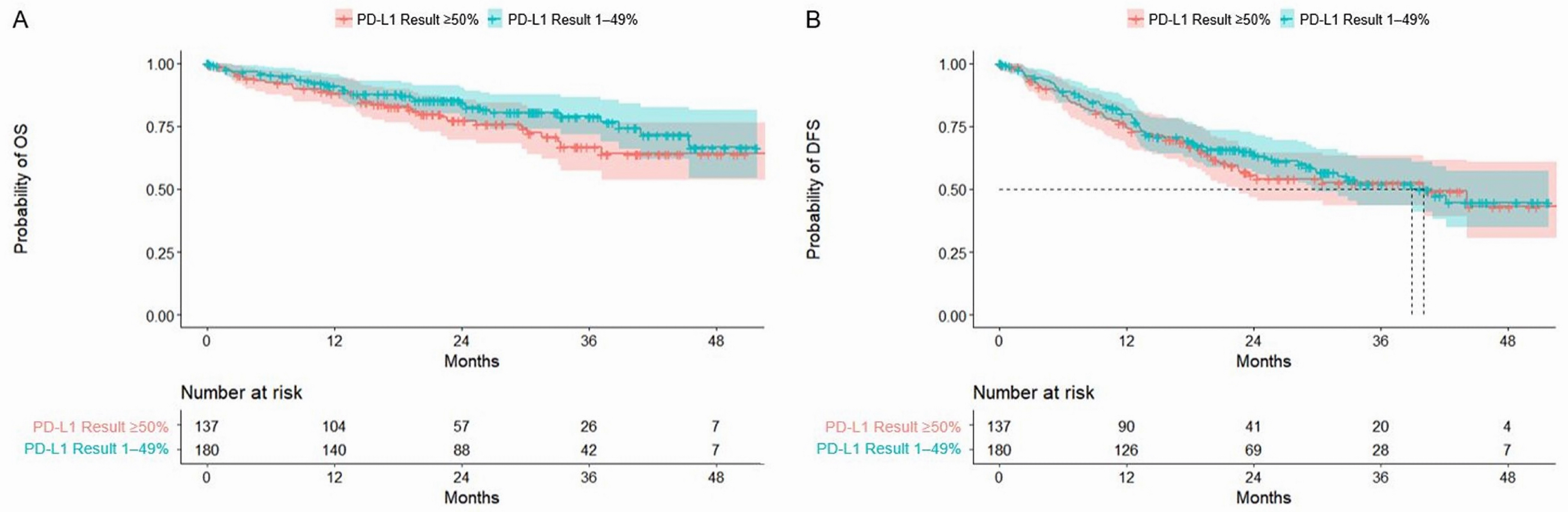
3.2.4. Overall and Disease-Free Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef] [PubMed]
- Canadian Cancer Society. Lung and Bronchus Cancer Statistics. Last Updated May 2024. Available online: https://cancer.ca/en/cancer-information/cancer-types/lung/statistics (accessed on 9 August 2024).
- Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics: A 2020 Special Report on Lung Cancer. Canadian Cancer Society. 2020. Available online: https://cdn.cancer.ca/-/media/files/cancer-information/resources/publications/2020-canadian-cancer-statistics-special-report/2020-canadian-cancer-statistics-special-report-en.pdf (accessed on 9 August 2024).
- Cagle, P.T.; Allen, T.C.; Olsen, R.J. Lung cancer biomarkers: Present status and future developments. Arch. Pathol. Lab. Med. 2013, 137, 1191–1198. [Google Scholar] [CrossRef] [PubMed]
- Le Chevalier, T. Adjuvant chemotherapy for resectable non-small-cell lung cancer: Where is it going? Ann. Oncol. 2010, 21 (Suppl. S7), vii196–vii198. [Google Scholar] [CrossRef] [PubMed]
- Postmus, P.E.; Kerr, K.M.; Oudkerk, M.; Senan, S.; Waller, D.A.; Vansteenkiste, J.; Escriu, C.; Peters, S. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv1–iv21. [Google Scholar] [CrossRef] [PubMed]
- Kris, M.G.; Gaspar, L.E.; Chaft, J.E.; Kennedy, E.B.; Azzoli, C.G.; Ellis, P.M.; Lin, S.H.; Pass, H.I.; Seth, R.; Shepherd, F.A.; et al. Adjuvant systemic therapy and adjuvant radiation therapy for stage I to IIIA completely resected non-small-cell lung cancers: American Society of Clinical Oncology/Cancer Care Ontario Clinical Practice Guideline update. J. Clin. Oncol. 2017, 35, 2960–2974. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Non-small Cell Lung Cancer; Version 7.2024; National Comprehensive Cancer Network: Fort Washington, PA, USA, 2024. [Google Scholar]
- Provincial Health Services Authority. BC Cancer. Management of Non-Small Cell Lung Cancer. Last Updated: February 2008. Available online: http://www.bccancer.bc.ca/health-professionals/clinical-resources/cancer-management-manual/lung/lung#Non-Small-Cell-Lung-Cancer-(NSCLC) (accessed on 9 August 2024).
- Lim, J.U.; Yeo, C.D. Update on adjuvant therapy in completely resected NSCLC patients. Thorac. Cancer 2022, 13, 277–283. [Google Scholar] [CrossRef]
- Pignon, J.P.; Tribodet, H.; Scagliotti, G.V.; Douillard, J.Y.; Shepherd, F.A.; Stephens, R.J.; Dunant, A.; Torri, V.; Rosell, R.; Seymour, L.; et al. Lung adjuvant cisplatin evaluation: A pooled analysis by the LACE Collaborative Group. J. Clin. Oncol. 2008, 26, 3552–3559. [Google Scholar] [CrossRef]
- Bradbury, P.; Sivajohanathan, D.; Chan, A.; Kulkarni, S.; Ung, Y.; Ellis, P.M. Postoperative adjuvant systemic therapy in completely resected non-small-cell lung cancer: A systematic review. Clin. Lung Cancer 2017, 18, 259–273. [Google Scholar] [CrossRef]
- Taylor, M.D.; Nagji, A.S.; Bhamidipati, C.M.; Theodosakis, N.; Kozower, B.D.; Lau, C.L.; Jones, D.R. Tumor recurrence after complete resection for non-small cell lung cancer. Ann. Thorac. Surg. 2012, 93, 1813–1820; discussion 1820–1811. [Google Scholar] [CrossRef]
- Uramoto, H.; Tanaka, F. Recurrence after surgery in patients with NSCLC. Transl. Lung Cancer Res. 2014, 3, 242–249. [Google Scholar]
- Felip, E.; Rosell, R.; Maestre, J.A.; Rodríguez-Paniagua, J.M.; Morán, T.; Astudillo, J.; Alonso, G.; Borro, J.M.; González-Larriba, J.L.; Torres, A.; et al. Preoperative chemotherapy plus surgery versus surgery plus adjuvant chemotherapy versus surgery alone in early-stage non-small-cell lung cancer. J. Clin. Oncol. 2010, 28, 3138–3145. [Google Scholar] [CrossRef]
- Deslypere, G.; Gullentops, D.; Wauters, E.; Vansteenkiste, J. Immunotherapy in non-metastatic non-small cell lung cancer: Can the benefits of stage IV therapy be translated into earlier stages? Ther. Adv. Med. Oncol. 2018, 10, 1758835918772810. [Google Scholar] [CrossRef] [PubMed]
- Broderick, S.R. Adjuvant and neoadjuvant immunotherapy in non-small cell lung cancer. Thorac. Surg. Clin. 2020, 30, 215–220. [Google Scholar] [CrossRef]
- Wu, Y.L.; Tsuboi, M.; He, J.; John, T.; Grohe, C.; Majem, M.; Goldman, J.W.; Laktionov, K.; Kim, S.W.; Kato, T.; et al. Osimertinib in resected EGFR-mutated non-small-cell lung cancer. N. Engl. J. Med. 2020, 383, 1711–1723. [Google Scholar] [CrossRef] [PubMed]
- Remon, J.; Soria, J.-C.; Peters, S.; On behalf of the ESMO Guidelines Committee. Early and locally advanced non-small-cell lung cancer: An update of the ESMO Clinical Practice Guidelines focusing on diagnosis, staging and systemic and local therapy. Ann. Oncol. 2021, 32, 1637–1641. [Google Scholar] [CrossRef] [PubMed]
- Pisters, K.; Kris, M.G.; Gaspar, L.E.; Ismaila, N. Adjuvant systemic therapy and adjuvant radiation therapy for stage I-IIIA completely resected non–small-cell lung cancer: ASCO guideline rapid recommendation update. J. Clin. Oncol. 2022, 40, 1127–1129. [Google Scholar] [CrossRef]
- Felip, E.; Altorki, N.; Zhou, C.; Csoszi, T.; Vynnychenko, I.; Goloborodko, O.; Luft, A.; Akopov, A.; Martinez-Marti, A.; Kenmotsu, H.; et al. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB-IIIA non-small-cell lung cancer (IMpower010): A randomised, multicentre, open-label, phase 3 trial. Lancet 2021, 398, 1344–1357. [Google Scholar] [CrossRef]
- Besse, B.; Havel, L.; Peters, S.; Marreaud, S.I.; Jha, N.; Oselin, K.; Gonzalez, E.E.; Casado, M.D.I.; Martinez-Marti, A.; Faehling, M.; et al. 120MO—Adjuvant pembrolizumab versus placebo for early-stage NSCLC after resection and optional chemotherapy: Updated results From PEARLS/KEYNOTE-091. Ann. Oncol. 2023, 20, 100589. [Google Scholar] [CrossRef]
- Forde, P.M.; Spicer, J.; Lu, S.; Provencio, M.; Mitsudomi, T.; Awad, M.M.; Felip, E.; Broderick, S.R.; Brahmer, J.R.; Swanson, S.J.; et al. Neoadjuvant nivolumab plus chemotherapy in resectable lung cancer. N. Engl. J. Med. 2022, 386, 1973–1985. [Google Scholar] [CrossRef]
- Wakelee, H.; Liberman, M.; Kato, T.; Tsuboi, M.; Lee, S.H.; Gao, S.; Chen, K.N.; Dooms, C.; Majem, M.; Eigendorff, E.; et al. Perioperative pembrolizumab for early-stage non-small-cell lung cancer. N. Engl. J. Med. 2023, 389, 491–503. [Google Scholar] [CrossRef]
- Spicer, J.D.; Gao, S.; Liberman, M.; Kato, T.; Tsuboi, M.; Lee, S.H.; Chen, K.N.; Dooms, C.; Majem, M.; Eigendorff, E.; et al. LBA56 Overall survival in the KEYNOTE-671 study of perioperative pembrolizumab for early-stage non-small-cell lung cancer (NSCLC). Ann. Oncol. 2023, 34, S1297–S1298. [Google Scholar] [CrossRef]
- Heymach, J.V.; Harpole, D.; Mitsudomi, T.; Taube, J.M.; Galffy, G.; Hochmair, M.; Winder, T.; Zukov, R.; Garbaos, G.; Gao, S.; et al. Perioperative durvalumab for resectable non–small-cell lung cancer. N. Eng. J. Med. 2023, 389, 1672–1684. [Google Scholar] [CrossRef]
- Cascone, T.; Awad Mark, M.; Spicer Jonathan, D.; He, J.; Lu, S.; Sepesi, B.; Tanaka, F.; Taube Janis, M.; Cornelissen, R.; Havel, L.; et al. Perioperative nivolumab in resectable lung cancer. N. Eng. J. Med. 2024, 390, 1756–1769. [Google Scholar] [CrossRef]
- Aggarwal, C.; Abreu, D.R.; Felip, E.; Carcereny, E.; Gottfried, M.; Wehler, T.; Ahn, M.J.; Dolled-Filhart, M.; Zhang, J.; Shentu, Y.; et al. Prevalence of PD-L1 expression in patients with non-small cell lung cancer screened for enrollment in KEYNOTE-001, -010, and -024. Ann. Oncol. 2016, 27, vi363. [Google Scholar] [CrossRef]
- Cruz-Rico, G.; Aviles-Salas, A.; Popa-Navarro, X.; Lara-Mejia, L.; Catalan, R.; Sanchez-Reyes, R.; Lopez-Sanchez, D.; Cabrera-Miranda, L.; Aquiles Maldonado-Martinez, H.; Samtani-Bassarmal, S.; et al. Association of lung adenocarcinoma subtypes according to the IASLC/ATS/ERS classification and programmed cell death ligand 1 (PD-L1) expression in tumor cells. Pathol. Oncol. Res. 2021, 27, 597499. [Google Scholar] [CrossRef]
- Dietel, M.; Savelov, N.; Salanova, R.; Micke, P.; Bigras, G.; Hida, T.; Antunez, J.; Guldhammer Skov, B.; Hutarew, G.; Sua, L.F.; et al. Real-world prevalence of programmed death ligand 1 expression in locally advanced or metastatic non-small-cell lung cancer: The global, multicenter EXPRESS study. Lung Cancer 2019, 134, 174–179. [Google Scholar] [CrossRef]
- Holmes, M.; Mahar, A.; Lum, T.; Boyer, M.; Kao, S.; Cooper, W. P1.09-26 Prevalence of PD-L1 expression rates in different NSCLC specimens. J. Thorac. Oncol. 2019, 14, S506. [Google Scholar] [CrossRef]
- Cuffe, S.; Booth, C.M.; Peng, Y.; Darling, G.E.; Li, G.; Kong, W.; Mackillop, W.J.; Shepherd, F.A. Adjuvant chemotherapy for non-small-cell lung cancer in the elderly: A population-based study in Ontario, Canada. J. Clin. Oncol. 2012, 30, 1813–1821. [Google Scholar] [CrossRef]
- Booth, C.M.; Shepherd, F.A.; Peng, Y.; Darling, G.; Li, G.; Kong, W.; Mackillop, W.J. Adjuvant chemotherapy for non-small cell lung cancer: Practice patterns and outcomes in the general population of Ontario, Canada. J. Thorac. Oncol. 2012, 7, 559–566. [Google Scholar] [CrossRef]
- Evans, W.K.; Stiff, J.; Woltman, K.J.; Ung, Y.C.; Su-Myat, S.; Manivong, P.; Tsang, K.; Nazen-Rad, N.; Gatto, A.; Tyrrell, A.; et al. How equitable is access to treatment for lung cancer patients? A population-based review of treatment practices in Ontario. Lung Cancer Manag. 2017, 6, 77–86. [Google Scholar] [CrossRef]
- Lu, S.; Zhang, W.; Wu, L.; Wang, W.; Zhang, P.; Fang, W.; Xing, W.; Chen, Q.; Yang, L.; Mei, J.; et al. Perioperative toripalimab plus chemotherapy for patients with resectable non-small cell lung cancer: The Neotorch randomized clinical Trial. JAMA 2024, 331, 201–211. [Google Scholar] [CrossRef]
- Nakagawa, M.; Uramoto, H.; Oka, S.; Chikaishi, Y.; Iwanami, T.; Shimokawa, H.; So, T.; Hanagiri, T.; Tanaka, F. Clinical significance of IGF1R expression in non-small-cell lung cancer. Clin. Lung Cancer 2012, 13, 136–142. [Google Scholar] [CrossRef]
- Yamashita, T.; Uramoto, H.; Onitsuka, T.; Ono, K.; Baba, T.; So, T.; So, T.; Takenoyama, M.; Hanagiri, T.; Oyama, T.; et al. Association between lymphangiogenesis-/micrometastasis- and adhesion-related molecules in resected stage I NSCLC. Lung Cancer 2010, 70, 320–328. [Google Scholar] [CrossRef]
- Hoffman-La Roche. Product Monograph: TECENTRIQ (Atezolizumab for Injection). Revised: 15 March 2024. Available online: https://assets.roche.com/f/173850/x/4558b62072/tecentriq_pm_cie.pdf (accessed on 17 May 2024).
- European Medicines Agency. Summary of Product Characteristics: TECENTRIQ. Last Updated: 25 March 2024. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/tecentriq (accessed on 17 May 2024).
- Food and Drug Administration. Highlights of Prescribing Information for TECENTRIQ (Atezolizumab). Revised: April 2024. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/761034s053lbl.pdf (accessed on 17 May 2024).
- Food and Drug Administration. Highlights of Prescribing Information for KEYTRUDA (Pembrolizumab). Revised: March 2024. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/125514s160lbl.pdf (accessed on 17 May 2024).
- Merck. Product Monograph: KEYTRUDA (Pembrolizumab). Date of Revision: 12 April 2024. Available online: https://www.merck.ca/en/wp-content/uploads/sites/20/2021/04/KEYTRUDA-PM_E.pdf (accessed on 17 May 2024).
- European Medicines Agency. Summary of Product Characteristics: KEYTRUDA. Last Updated: 13 May 2024. Available online: https://www.ema.europa.eu/en/documents/product-information/keytruda-epar-product-information_en.pdf (accessed on 17 May 2024).
- Bristol-Myers Squib. Product Monograph: OPDIVO (Nivolumab) for Injection. Revised: 29 December 2023. Available online: https://www.bms.com/assets/bms/ca/documents/productmonograph/OPDIVO_EN_PM.pdf (accessed on 17 May 2024).
- Food and Drug Administration. Highlights of Prescribing Information for OPDIVO (Nivolumab). Revised: March 2024. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/125554s112lbl.pdf (accessed on 17 May 2024).
- European Medicines Agency. Summary of Product Characteristics: OPDIVO. Last Updated: 4 April 2024. Available online: https://www.ema.europa.eu/en/documents/product-information/opdivo-epar-product-information_en.pdf (accessed on 17 May 2024).
- Sands, J.M.; Mandrekar, S.J.; Kozono, D.; Oxnard, G.R.; Hillman, S.L.; Wigle, D.A.; Govindan, R.; Carlisle, J.; Gray, J.; Salama, J.K.; et al. Integration of immunotherapy into adjuvant therapy for resected non-small-cell lung cancer: ALCHEMIST chemo-IO (ACCIO). Immunotherapy 2021, 13, 727–734. [Google Scholar] [CrossRef]
- Calvo, V.; Domine, M.; Sullivan, I.; Gonzalez-Larriba, J.-L.; Ortega, A.L.; Bernabé, R.; Sala, M.A.; Campos, B.; Castro, J.D.; Martín-Martorell, P.; et al. A phase III clinical trial of adjuvant chemotherapy versus chemoimmunotherapy for stage IB-IIIA completely resected non-small cell lung cancer (NSCLC) patients nadim-adjuvant: New adjuvant trial of chemotherapy versus chemoimmunotherapy. J. Clin. Oncol. 2021, 39, TPS8581. [Google Scholar] [CrossRef]
- Chaft, J.E.; Dahlberg, S.E.; Khullar, O.V.; Edelman, M.J.; Simone, C.B.; Heymach, J.; Rudin, C.M.; Ramalingam, S.S. EA5142 adjuvant nivolumab in resected lung cancers (ANVIL). J. Clin. Oncol. 2018, 35, TPS8575. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristic | PD-L1 Negative | PD-L1 Positive 1 | All PD-L1–Tested Patients |
|---|---|---|---|
| Overall, n (% of 539) | 222 (41.2) | 317 (58.8) | 539 (100.0) |
| PD-L1 Expression, n (%) | |||
| 1–49% | -- | 180 (56.8) | 180 (33.4) |
| ≥50% | -- | 137 (43.2) | 137 (25.4) |
| Stage at Diagnosis, n (%) | |||
| IB | 98 (44.1) | 112 (35.3) | 210 (39.0) |
| II | 83 (37.4) | 126 (39.8) | 209 (38.8) |
| IIIA | 41 (18.5) | 79 (24.9) | 120 (22.3) |
| Sex, n (%) | |||
| Female | 116 (52.2) | 162 (51.1) | 278 (51.6) |
| Male | 106 (47.8) | 155 (48.9) | 261 (48.4) |
| Race 2, n (%) | |||
| Asian, NOS | 18 (8.1) | 13 (4.1) | 31 (5.8) |
| Caucasian | 20 (9.0) | 44 (13.9) | 64 (11.9) |
| East, Central, or South Asian | 17 (7.7) | 19 (6.0) | 36 (6.7) |
| Other | 45 (20.3) | 81 (25.5) | 126 (23.4) |
| Unknown | 122 (55.0) | 160 (50.5) | 282 (52.3) |
| Smoking Status, n (%) | |||
| Current/former smoker | 145 (65.3) | 270 (85.2) | 415 (77.0) |
| Never smoker | 66 (29.7) | 42 (13.2) | 108 (20.0) |
| Unknown | 11 (5.0) | 5 (1.6) | 16 (3.0) |
| Histopathological Diagnosis, n (%) | |||
| Adenocarcinoma | 173 (77.9) | 198 (62.4) | 371 (68.8) |
| Squamous cell carcinoma | 30 (13.5) | 87 (27.4) | 117 (21.7) |
| Adenosquamous carcinoma | 0 (0.0) | 9 (2.8) | 9 (1.7) |
| Large cell carcinoma | 12 (5.4) | 2 (0.6) | 14 (2.6) |
| Other 3 | 7 (3.2) | 21 (6.6) | 28 (5.2) |
| EGFRm Testing Status, n (%) | |||
| Unknown/Not tested | 53 (23.9) | 96 (30.3) | 149 (27.6) |
| Known/Tested 4 | 169 (76.1) | 221 (69.7) | 390 (72.4) |
| EGFRm Status 5, n (%) | |||
| Negative | 123 (72.8) | 185 (83.7) | 308 (79.0) |
| Positive | 46 (27.2) | 36 (16.3) | 82 (21.0) |
| Common Exon 19 deletion | 20 (11.8) | 14 (6.3) | 34 (8.7) |
| Common Exon 21 L858R | 17 (10.1) | 9 (4.1) | 26 (6.7) |
| Uncommon mutations | 9 (5.3) | 13 (5.9) | 22 (5.6) |
| Characteristic | Resection Alone | Resection + Adjuvant Therapy | All PD-L1+ Patients |
|---|---|---|---|
| Overall, n (% of 317) | 186 (58.7) | 131 (41.3) | 317 (100) |
| Age at Diagnosis | |||
| Years, mean (SD) | 71.8 (8.7) | 68.0 (8.5) | 70.2 (8.8) |
| ≥65 years, n (%) | 149 (80.1) | 92 (70.2) | 241 (76.0) |
| <65 years, n (%) | 37 (19.9) | 39 (29.8) | 76 (24.0) |
| Stage at Diagnosis, n (%) | |||
| IB | 102 (54.8) | 10 (7.6) | 112 (35.3) |
| II | 58 (31.0) | 68 (51.9) | 126 (39.8) |
| IIIA | 26 (13.9) | 53 (40.4) | 79 (24.9) |
| Sex | |||
| Female | 97 (52.2) | 65 (49.6) | 162 (51.1) |
| Male | 89 (47.8) | 66 (50.4) | 155 (48.9) |
| PD-L1 Expression, n (%) | |||
| 1–49% | 105 (56.5) | 75 (57.3) | 180 (56.8) |
| ≥50% | 81 (43.5) | 56 (42.7) | 137 (43.2) |
| Race 1, n (%) | |||
| Asian, NOS | 6 (3.2) | 7 (5.3) | 13 (4.1) |
| Caucasian | 20 (10.8) | 24 (18.3) | 44 (13.9) |
| East, Central, or South Asian | 9 (4.8) | 10 (7.6) | 19 (6.0) |
| Other | 54 (29.0) | 27 (20.6) | 81 (25.6) |
| Unknown | 97 (52.2) | 63 (48.1) | 160 (50.5) |
| Weight Category, n (%) | |||
| <60 kg | 40 (21.5) | 20 (15.3) | 60 (18.9) |
| ≥60 kg | 111 (59.7) | 92 (70.2) | 203 (64.0) |
| Unknown | 35 (18.8) | 19 (14.5) | 54 (17.0) |
| Smoking Status, n (%) | |||
| Current/former smoker | 164 (88.2) | 106 (80.9) | 270 (85.2) |
| Never smoker | 18 (9.7) | 24 (18.3) | 42 (13.3) |
| Unknown | 4 (2.2) | 1 (0.1) | 5 (1.6) |
| ECOG Status, n (%) | |||
| 0 | 69 (37.1) | 32 (24.4) | 101 (31.9) |
| 1 | 31 (16.7) | 29 (22.1) | 60 (18.9) |
| 2 | 1 (0.5) | 1 (0.8) | 2 (0.6) |
| Unknown | 85 (45.7) | 69 (52.7) | 154 (48.6) |
| Result of Surgery, n (%) | |||
| R0 | 180 (96.8) | 124 (94.7) | 304 (95.9) |
| R1 | 6 (3.2) | 5 (3.9) | 11 (3.5) |
| R2 | 0 (0.0) | 2 (1.5) | 2 (0.6) |
| Histopathological Diagnosis, n (%) | |||
| Adenocarcinoma | 110 (59.1) | 88 (67.2) | 198 (62.5) |
| Squamous cell carcinoma | 53 (28.5) | 34 (30.0) | 87 (27.4) |
| Adenosquamous carcinoma | 6 (3.2) | 3 (2.3) | 9 (2.8) |
| Large cell carcinoma | 2 (1.1) | 0 (0.0) | 2 (0.6) |
| Other | 15 (8.1) | 6 (4.6) | 21 (6.6) |
| EGFRm Testing Status, n (%) | |||
| Unknown/Not tested | 61 (32.8) | 35 (26.7) | 96 (30.3) |
| Known/Tested 2 | 125 (67.2) | 96 (73.3) | 221 (69.7) |
| EGFRm Status 3, n (%) | |||
| Negative | 110 (88.0) | 75 (78.1) | 185 (83.7) |
| Positive | 15 (12.0) | 21 (21.9) | 36 (16.3) |
| Common Exon 19 deletion | 6 (4.8) | 8 (8.3) | 14 (6.3) |
| Common Exon 21 L858R | 3 (2.4) | 6 (6.3) | 9 (4.1) |
| Uncommon mutations | 6 (4.8) | 7 (7.3) | 13 (5.9) |
| Variable | No. of Patients | No. of Deaths | Median OS mo. (95% CI) | No. of DFS Events | Median DFS mo. (95% CI) |
|---|---|---|---|---|---|
| Overall | 317 | 66 | NE (NE–NE) | 125 | 40.0 (30.0–NE) |
| Stage at Diagnosis | |||||
| IB | 112 | 11 | NE (NE–NE) | 23 | NE (NE–NE) |
| II | 126 | 31 | 45.5 (40.9–NE) | 53 | 30.0 (19.6–NE) |
| IIIA | 79 | 24 | NE (33.3–NE) | 49 | 18.7 (12.7–29.5) |
| II and IIIA combined | 205 | 55 | NE (40.9–NE) | 102 | 22.6 (19.1–32.9) |
| Result of Surgery | |||||
| R0 | 304 | 62 | NE (NE–NE) | 118 | 40.9 (30.0–NE) |
| R1 | 11 | 3 | 37.2 (37.2–NE) | 6 | 19.4 (16.9–NE) |
| R2 | 2 | 1 | 22.6 (NE–NE) | 1 | 12.0 (12.0–NE) |
| R1 + R2 | 13 | 4 | 37.2 (22.6–NE) | 7 | 19.4 (12.7–NE) |
| Treatment Type | |||||
| Resection alone | 186 | 33 | NE (NE–NE) | 58 | NE (40.0–NE) |
| Resection + adjuvant therapy (systemic and/or RT) | 131 | 33 | NE (45.5–NE) | 67 | 28.2 (20.6–42.2) |
| Adjuvant Therapy Status (systemic and/or RT) | |||||
| Complete | 86 | 20 | NE (45.5–NE) | 43 | 32.0 (22.6–NE) |
| Incomplete 1 | 38 | 10 | NE (33.1–NE) | 21 | 21.4 (10.1–NE) |
| PD-L1 Expression | |||||
| 1–49% | 180 | 33 | NE (NE–NE) | 70 | 38.9 (30.0–NE) |
| ≥50% | 137 | 33 | NE (NE–NE) | 55 | 40.0 (22.5–NE) |
| EGFRm Status | |||||
| Positive | 36 | 9 | NE (38.9–NE) | 18 | 32.9 (18.7–NE) |
| Common mutations | 23 | 5 | NE (33.3–NE) | 11 | 22.5 (14.1–NE) |
| Uncommon mutations | 13 | 3 | NE (38.9–NE) | 6 | 38.9 (16.9–NE) |
| Negative | 185 | 31 | NE (NE–NE) | 67 | 42.2 (30.5–NE) |
| Unknown | 96 | 26 | NE (NE–NE) | 40 | 40.0 (19.6–NE) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheema, P.K.; Syed, I.; Gwadry-Sridhar, F.; Rakibuz-Zaman, M.; Sachdeva, R.; Pencz, A.; Zhan, L.; Hueniken, K.; Patel, D.; Balaratnam, K.; et al. Programmed Cell Death-Ligand 1 Expression and Clinical Outcomes Among Patients with Resected, Early-Stage Non-Small Cell Lung Cancer: A Real-World Study. Curr. Oncol. 2024, 31, 6735-6748. https://doi.org/10.3390/curroncol31110497
Cheema PK, Syed I, Gwadry-Sridhar F, Rakibuz-Zaman M, Sachdeva R, Pencz A, Zhan L, Hueniken K, Patel D, Balaratnam K, et al. Programmed Cell Death-Ligand 1 Expression and Clinical Outcomes Among Patients with Resected, Early-Stage Non-Small Cell Lung Cancer: A Real-World Study. Current Oncology. 2024; 31(11):6735-6748. https://doi.org/10.3390/curroncol31110497
Chicago/Turabian StyleCheema, Parneet K., Iqra Syed, Femida Gwadry-Sridhar, Muhammad Rakibuz-Zaman, Robin Sachdeva, Alec Pencz, Luna Zhan, Katrina Hueniken, Devalben Patel, Karmugi Balaratnam, and et al. 2024. "Programmed Cell Death-Ligand 1 Expression and Clinical Outcomes Among Patients with Resected, Early-Stage Non-Small Cell Lung Cancer: A Real-World Study" Current Oncology 31, no. 11: 6735-6748. https://doi.org/10.3390/curroncol31110497
APA StyleCheema, P. K., Syed, I., Gwadry-Sridhar, F., Rakibuz-Zaman, M., Sachdeva, R., Pencz, A., Zhan, L., Hueniken, K., Patel, D., Balaratnam, K., Khan, K., Grant, B., Sheffield, B. S., Locke, M. E. O., Moldaver, D., Shanahan, M. K., Liu, G., & Kuruvilla, M. S. (2024). Programmed Cell Death-Ligand 1 Expression and Clinical Outcomes Among Patients with Resected, Early-Stage Non-Small Cell Lung Cancer: A Real-World Study. Current Oncology, 31(11), 6735-6748. https://doi.org/10.3390/curroncol31110497