Two-Step Screening for Depression and Anxiety in Patients with Cancer: A Retrospective Validation Study Using Real-World Data

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mitchell, A.J.; Chan, M.; Bhatti, H.; Halton, M.; Grassi, L.; Johansen, C.; Meader, N. Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: A meta-analysis of 94 interview-based studies. Lancet Oncol. 2011, 12, 160–174. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Kennedy, E.B.; Byrne, N.; Gérin-Lajoie, C.; Katz, M.R.; Keshavarz, H.; Sellick, S.; Green, E. Systematic review and meta-analysis of collaborative care interventions for depression in patients with cancer. Psycho-Oncology 2017, 26, 573–587. [Google Scholar] [CrossRef]
- Sanjida, S.; McPhail, S.M.; Shaw, J.; Couper, J.; Kissane, D.; Price, M.A.; Janda, M. Are psychological interventions effective on anxiety in cancer patients? A systematic review and meta-analyses. Psycho-Oncology 2018, 27, 2063–2076. [Google Scholar] [CrossRef]
- Donovan, K.A.; Deshields, T.L.; Corbett, C.; Riba, M.B. Update on the implementation of NCCN guidelines for distress management by NCCN member institutions. J. Natl. Compr. Cancer Netw. 2019, 17, 1251–1256. [Google Scholar] [CrossRef] [PubMed]
- Hammer, S.L.; Clark, K.; Grant, M.; Loscalzo, M.J. Seventeen years of progress for supportive care services: A resurvey of National Cancer Institute-designated comprehensive cancer centers. Palliat. Support. Care 2015, 13, 917. [Google Scholar] [CrossRef]
- Fradgley, E.A.; Bultz, B.D.; Kelly, B.J.; Loscalzo, M.J.; Grassi, L.; Sitaram, B. Progress toward integrating Distress as the Sixth Vital Sign: A global snapshot of triumphs and tribulations in precision supportive care. J. Psychosoc. Oncol. Res. Pract. 2019, 1, e2. [Google Scholar] [CrossRef]
- Howell, D.; Olsen, K. Distress—The 6th vital sign. Curr. Oncol. 2011, 18, 208. [Google Scholar] [CrossRef]
- Commission on Cancer. Cancer Program Standards 2012: Ensuring Patient-Centered Care; American College of Surgeons: Washington, DC, USA, 2012. [Google Scholar]
- Cancer Care Standards. Accreditation Canada. 2016. Available online: https://accreditation.ca/standards/ (accessed on 3 May 2024).
- Riba, M.B.; Donovan, K.A.; Andersen, B.; Braun, I.; Breitbart, W.S.; Brewer, B.W.; Buchmann, L.O.; Clark, M.M.; Collins, M.; Corbett, C. Distress management, version 3.2019, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. 2019, 17, 1229–1249. [Google Scholar] [CrossRef]
- Bultz, B.D.; Groff, S.L.; Fitch, M.; Blais, M.C.; Howes, J.; Levy, K.; Mayer, C. Implementing screening for distress, the 6th vital sign: A Canadian strategy for changing practice. Psycho-Oncology 2011, 20, 463–469. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Lord, K.; Slattery, J.; Grainger, L.; Symonds, P. How feasible is implementation of distress screening by cancer clinicians in routine clinical care? Cancer 2012, 118, 6260–6269. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Kaar, S.; Coggan, C.; Herdman, J. Acceptability of common screening methods used to detect distress and related mood disorders—Preferences of cancer specialists and non-specialists. Psycho-Oncol. J. Psychol. Soc. Behav. Dimens. Cancer 2008, 17, 226–236. [Google Scholar] [CrossRef]
- Mitchell, A.J. Pooled results from 38 analyses of the accuracy of distress thermometer and other ultra-short methods of detecting cancer-related mood disorders. J. Clin. Oncol. 2007, 25, 4670–4681. [Google Scholar] [CrossRef] [PubMed]
- Vodermaier, A.; Linden, W.; Siu, C. Screening for emotional distress in cancer patients: A systematic review of assessment instruments. J. Natl. Cancer Inst. 2009, 101, 1464–1488. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Meader, N.; Davies, E.; Clover, K.; Carter, G.L.; Loscalzo, M.J.; Linden, W.; Grassi, L.; Johansen, C.; Carlson, L.E. Meta-analysis of screening and case finding tools for depression in cancer: Evidence based recommendations for clinical practice on behalf of the Depression in Cancer Care consensus group. J. Affect. Disord. 2012, 140, 149–160. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Vahabzadeh, A.; Magruder, K. Screening for distress and depression in cancer settings: 10 lessons from 40 years of primary-care research. Psycho-Oncology 2011, 20, 572–584. [Google Scholar] [CrossRef] [PubMed]
- Clover, K.; Carter, G.L.; Mackinnon, A.; Adams, C. Is my patient suffering clinically significant emotional distress? Demonstration of a probabilities approach to evaluating algorithms for screening for distress. Support. Care Cancer 2009, 17, 1455–1462. [Google Scholar] [CrossRef]
- Howell, D.; Keshavarz, H.; Esplen, M.; Hack, T.; Hamel, M.; Howes, J.; Jones, J.; Li, M.; Manii, D.; McLeod, D.; et al. A Pan Canadian Practice Guideline: Screening, Assessment and Care of Psychosocial Distress, Depression, and Anxiety in Adults with Cancer; Canadian Partnership against Cancer and the Canadian Association of Psychosocial Oncology: Toronto, ON, Canada, 2015. [Google Scholar]
- Andersen, B.L.; Lacchetti, C.; Ashing, K.; Berek, J.S.; Berman, B.S.; Bolte, S.; Dizon, D.S.; Given, B.; Nekhlyudov, L.; Pirl, W. Management of anxiety and depression in adult survivors of cancer: ASCO guideline update. J. Clin. Oncol. 2023, 41, 3426–3453. [Google Scholar] [CrossRef]
- Butow, P.; Price, M.A.; Shaw, J.M.; Turner, J.; Clayton, J.M.; Grimison, P.; Rankin, N.; Kirsten, L. Clinical pathway for the screening, assessment and management of anxiety and depression in adult cancer patients: Australian guidelines. Psycho-Oncology 2015, 24, 987–1001. [Google Scholar] [CrossRef]
- Grassi, L.; Caruso, R.; Riba, M.; Lloyd-Williams, M.; Kissane, D.; Rodin, G.; McFarland, D.; Campos-Ródenas, R.; Zachariae, R.; Santini, D. Anxiety and depression in adult cancer patients: ESMO Clinical Practice Guideline. ESMO Open 2023, 8, 101155. [Google Scholar] [CrossRef]
- Whooley, M.A.; Avins, A.L.; Miranda, J.; Browner, W.S. Case-finding instruments for depression: Two questions are as good as many. J. Gen. Intern. Med. 1997, 12, 439–445. [Google Scholar] [CrossRef]
- Henkel, V.; Mergl, R.; Coyne, J.C.; Kohnen, R.; Möller, H.-J.; Hegerl, U. Screening for depression in primary care: Will one or two items suffice? Eur. Arch. Psychiatry Clin. Neurosci. 2004, 254, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Cull, A.; Gould, A.; House, A.; Smith, A.; Strong, V.; Velikova, G.; Wright, P.; Selby, P. Validating automated screening for psychological distress by means of computer touchscreens for use in routine oncology practice. Br. J. Cancer 2001, 85, 1842–1849. [Google Scholar] [CrossRef] [PubMed]
- Fann, J.R.; Berry, D.L.; Wolpin, S.; Austin-Seymour, M.; Bush, N.; Halpenny, B.; Lober, W.B.; McCorkle, R. Depression screening using the Patient Health Questionnaire-9 administered on a touch screen computer. Psycho-Oncol. J. Psychol. Soc. Behav. Dimens. Cancer 2009, 18, 14–22. [Google Scholar] [CrossRef]
- Li, M.; Macedo, A.; Crawford, S.; Bagha, S.; Leung, Y.W.; Zimmermann, C.; Fitzgerald, B.; Wyatt, M.; Stuart-McEwan, T.; Rodin, G. Easier said than done: Keys to successful implementation of the distress assessment and response tool (DART) program. J. Oncol. Pract. 2016, 12, e513–e526. [Google Scholar] [CrossRef]
- Watanabe, S.M.; Nekolaichuk, C.L.; Beaumont, C. The Edmonton Symptom Assessment System, a proposed tool for distress screening in cancer patients: Development and refinement. Psycho-Oncology 2012, 21, 977–985. [Google Scholar] [CrossRef]
- Thekkumpurath, P.; Walker, J.; Butcher, I.; Hodges, L.; Kleiboer, A.; O’Connor, M.; Wall, L.; Murray, G.; Kroenke, K.; Sharpe, M. Screening for major depression in cancer outpatients: The diagnostic accuracy of the 9-item patient health questionnaire. Cancer 2011, 117, 218–227. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L. The PHQ-9: A new depression diagnostic and severity measure. Psychiatr. Ann. 2002, 32, 509–515. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Washington, DC, USA, 2013; Volume 5. [Google Scholar]
- Wright, E.; Kiely, M.; Johnston, C.; Smith, A.; Cull, A.; Selby, P. Development and evaluation of an instrument to assess social difficulties in routine oncology practice. Qual. Life Res. 2005, 14, 373–386. [Google Scholar] [CrossRef]
- Ashbury, F.D.; Findlay, H.; Reynolds, B.; McKerracher, K. A Canadian survey of cancer patients’ experiences: Are their needs being met? J. Pain Symptom Manag. 1998, 16, 298–306. [Google Scholar] [CrossRef]
- Valentine, A.; Brown, J.; Lacourt, T.; Chen, M.; De La Garza, R.; Bruera, E. Frequency of anxiety and depression and screening performance of the Edmonton Symptom Assessment Scale in a psycho-oncology clinic. Psycho-Oncology 2022, 31, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Bagha, S.; Macedo, A.; Jacks, L.; Lo, C.; Zimmermann, C.; Rodin, G.; Li, M. The utility of the Edmonton Symptom Assessment System in screening for anxiety and depression. Eur. J. Cancer Care 2013, 22, 60–69. [Google Scholar] [CrossRef]
- Levis, B.; Benedetti, A.; Levis, A.W.; Ioannidis, J.P.; Shrier, I.; Cuijpers, P.; Gilbody, S.; Kloda, L.A.; McMillan, D.; Patten, S.B. Selective cutoff reporting in studies of diagnostic test accuracy: A comparison of conventional and individual-patient-data meta-analyses of the Patient Health Questionnaire-9 depression screening tool. Am. J. Epidemiol. 2017, 185, 954–964. [Google Scholar] [CrossRef]
- Chau, Y.F.; Zhou, H.; Chen, B.; Ren, H.; Ma, Z.; Zhang, X.; Duan, J. Screening for depression and anxiety in lung cancer patients: A real-world study using GAD-7 and HADS. Thorac. Cancer 2024, 15, 1041–1049. [Google Scholar] [CrossRef] [PubMed]
- Esser, P.; Hartung, T.J.; Friedrich, M.; Johansen, C.; Wittchen, H.U.; Faller, H.; Koch, U.; Härter, M.; Keller, M.; Schulz, H. The Generalized Anxiety Disorder Screener (GAD-7) and the anxiety module of the Hospital and Depression Scale (HADS-A) as screening tools for generalized anxiety disorder among cancer patients. Psycho-Oncology 2018, 27, 1509–1516. [Google Scholar] [CrossRef]
- Plummer, F.; Manea, L.; Trepel, D.; McMillan, D. Screening for anxiety disorders with the GAD-7 and GAD-2: A systematic review and diagnostic metaanalysis. Gen. Hosp. Psychiatry 2016, 39, 24–31. [Google Scholar] [CrossRef]
- Hartung, T.J.; Friedrich, M.; Johansen, C.; Wittchen, H.U.; Faller, H.; Koch, U.; Brähler, E.; Härter, M.; Keller, M.; Schulz, H. The Hospital Anxiety and Depression Scale (HADS) and the 9-item Patient Health Questionnaire (PHQ-9) as screening instruments for depression in patients with cancer. Cancer 2017, 123, 4236–4243. [Google Scholar] [CrossRef] [PubMed]
- Gascon, B.; Leung, Y.; Espin-Garcia, O.; Rodin, G.; Chu, D.; Li, M. Suicide risk screening and suicide prevention in patients with cancer. JNCI Cancer Spectr. 2021, 5, pkab057. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Cao, Y.; Cao, X.; Shi, X.; Lei, M.; Su, X.; Liu, Y. Machine learning-based algorithms to predict severe psychological distress among cancer patients with spinal metastatic disease. Spine J. 2023, 23, 1255–1269. [Google Scholar] [CrossRef]
- Park, J.-H.; Chun, M.; Bae, S.H.; Woo, J.; Chon, E.; Kim, H.J. Factors influencing psychological distress among breast cancer survivors using machine learning techniques. Sci. Rep. 2024, 14, 15052. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristic | All Patients (n = 172) |
|---|---|
| Age | |
| Mean | 52 |
| Median | 53 |
| Standard deviation (SD) | 14.4 |
| Range | 19–87 |
| Unknown | n = 5 |
| Sex—n (%) | |
| Male | 73 (42%) |
| Female | 99 (58%) |
| Marital Status—n (%) | |
| Married | 89 (52%) |
| Single | 46 (27%) |
| Divorced | 22 (13%) |
| Unknown | 7 (4%) |
| Widowed | 6 (3%) |
| Common-law | 2 (1%) |
| Cancer Type—n (%) | |
| Breast | 32 (19%) |
| Gastrointestinal | 24 (14%) |
| Hematologic | 22 (13%) |
| Head and neck | 21 (12%) |
| Gynecologic | 19 (11%) |
| Lung | 11 (6%) |
| Brain | 8 (5%) |
| Lymphoma | 7 (4%) |
| Other | 28 (17%) |
| Anxiety based on psychiatric assessment (reference gold standard)—n (%) | |
| Yes | 39 (23%) |
| No | 133 (77%) |
| Depression based on psychiatric assessment (reference gold standard)—n (%) | |
| Yes | 59 (34%) |
| No | 113 (66%) |
| PHQ Cut-Off | True Positives | True Negatives | False Positives | False Negatives | Sensitivity | Specificity | PPV | NPV | Likelihood Ratios | |
|---|---|---|---|---|---|---|---|---|---|---|
| No. of Correctly Predicted Events | No. of Correctly Predicted Non-Events | No. of Non-Events Predicted as Events | No. of Events Predicted as Non-Events | |||||||
| LR Positive | LR Negative | |||||||||
| ≥0 | 59 | 0 | 113 | 0 | 1.00 | 0.00 | 0.34 | ― | 1.00 | ― |
| ≥1 | 59 | 3 | 110 | 0 | 1.00 | 0.03 | 0.35 | 1.00 | 1.03 | 0.00 |
| ≥2 | 59 | 5 | 108 | 0 | 1.00 | 0.04 | 0.35 | 1.00 | 1.05 | 0.00 |
| ≥3 | 59 | 10 | 103 | 0 | 1.00 | 0.09 | 0.36 | 1.00 | 1.10 | 0.00 |
| ≥4 | 59 | 12 | 101 | 0 | 1.00 | 0.11 | 0.37 | 1.00 | 1.12 | 0.00 |
| ≥5 | 59 | 22 | 91 | 0 | 1.00 | 0.19 | 0.39 | 1.00 | 1.24 | 0.00 |
| ≥6 | 58 | 29 | 84 | 1 | 0.98 | 0.26 | 0.41 | 0.97 | 1.32 | 0.07 |
| ≥7 | 53 | 35 | 78 | 6 | 0.90 | 0.31 | 0.40 | 0.85 | 1.30 | 0.33 |
| ≥8 | 50 | 44 | 69 | 9 | 0.85 | 0.39 | 0.42 | 0.83 | 1.39 | 0.39 |
| ≥9 | 48 | 49 | 64 | 11 | 0.81 | 0.43 | 0.43 | 0.82 | 1.44 | 0.43 |
| ≥10 | 43 | 59 | 54 | 16 | 0.73 | 0.52 | 0.44 | 0.79 | 1.53 | 0.52 |
| ≥11 | 39 | 69 | 44 | 20 | 0.66 | 0.61 | 0.47 | 0.78 | 1.70 | 0.56 |
| ≥12 | 36 | 72 | 41 | 23 | 0.61 | 0.64 | 0.47 | 0.76 | 1.68 | 0.61 |
| ≥13 | 35 | 78 | 35 | 24 | 0.59 | 0.69 | 0.50 | 0.76 | 1.92 | 0.59 |
| ≥14 | 31 | 86 | 27 | 28 | 0.53 | 0.76 | 0.53 | 0.75 | 2.20 | 0.62 |
| ≥15 | 28 | 92 | 21 | 31 | 0.47 | 0.81 | 0.57 | 0.75 | 2.55 | 0.65 |
| ≥16 | 26 | 94 | 19 | 33 | 0.44 | 0.83 | 0.58 | 0.74 | 2.62 | 0.67 |
| ≥17 | 24 | 100 | 13 | 35 | 0.41 | 0.88 | 0.65 | 0.74 | 3.54 | 0.67 |
| ≥18 | 19 | 104 | 9 | 40 | 0.32 | 0.92 | 0.68 | 0.72 | 4.04 | 0.74 |
| ≥19 | 16 | 106 | 7 | 43 | 0.27 | 0.94 | 0.70 | 0.71 | 4.38 | 0.78 |
| ≥20 | 14 | 109 | 4 | 45 | 0.24 | 0.96 | 0.78 | 0.71 | 6.70 | 0.79 |
| ≥21 | 11 | 111 | 2 | 48 | 0.19 | 0.98 | 0.85 | 0.70 | 10.53 | 0.83 |
| ≥22 | 11 | 111 | 2 | 48 | 0.19 | 0.98 | 0.85 | 0.70 | 10.53 | 0.83 |
| ≥23 | 8 | 111 | 2 | 51 | 0.14 | 0.98 | 0.80 | 0.69 | 7.66 | 0.88 |
| ≥24 | 6 | 111 | 2 | 53 | 0.10 | 0.98 | 0.75 | 0.68 | 5.75 | 0.91 |
| ≥25 | 4 | 112 | 1 | 55 | 0.07 | 0.99 | 0.80 | 0.67 | 7.66 | 0.94 |
| ≥26 | 1 | 112 | 1 | 58 | 0.02 | 0.99 | 0.50 | 0.66 | 1.92 | 0.99 |
| ≥27 | 1 | 112 | 1 | 58 | 0.02 | 0.99 | 0.50 | 0.66 | 1.92 | 0.99 |
| Diagnosis of Depression | Not Diagnosed with Depression | ||||||||||
| DART Measure | Mean | Median | SD | Min | Max | Mean | Median | SD | Min | Max | p Value |
| ESAS Depression (ESAS-D) | 6.19 | 7.00 | 2.78 | 0 | 10 | 4.22 | 4.00 | 2.78 | 0 | 10 | <0.0001 |
| PHQ-9 | 14.53 | 14.00 | 6.12 | 5 | 27 | 9.67 | 9.00 | 5.45 | 0 | 27 | <0.0001 |
| Diagnosis of Anxiety | Not Diagnosed with Anxiety | ||||||||||
| ESAS Anxiety (ESAS-A) | 5.77 | 6.00 | 2.90 | 0 | 10 | 5.36 | 6.00 | 2.77 | 0 | 10 | 0.39 |
| GAD-7 | 10.08 | 9.00 | 6.25 | 0 | 21 | 8.53 | 8.00 | 5.83 | 0 | 21 | 0.18 |
| SD = Standard deviation | |||||||||||
| Parameter | Prescribed Medication | Estimate | Standard Error | Chi-Square | Pr > Chi-Square |
|---|---|---|---|---|---|
| PHQ-9 Summed Score | Antidepressant | 0.0671 | 0.0324 | 4.28 | 0.0386 |
| Anxiolytic | 0.0891 | 0.0443 | 4.06 | 0.044 | |
| Both | 0.1817 | 0.0454 | 16.02 | <0.0001 | |
| GAD-7 Summed Score | Antidepressant | −0.00095 | 0.0327 | 0 | 0.9769 |
| Anxiolytic | 0.0817 | 0.0443 | 3.4 | 0.0652 | |
| Both | 0.0938 | 0.0435 | 4.64 | 0.0312 |
| Parameter | DF | Estimate | Standard Error | Wald 95% Confidence Limits Min. | Wald 95% Confidence Limits Max. | Wald Chi-Square | Pr > Chi-Square | |
|---|---|---|---|---|---|---|---|---|
| PHQ Summed Score | 1 | 0.0408 | 0.0053 | 0.0303 | 0.0512 | 58.46 | <0.0001 | |
| Age | 1 | −0.0015 | 0.0027 | −0.0067 | 0.0037 | 0.33 | 0.5682 | |
| Sex | F vs. M | 1 | 0.1054 | 0.0738 | −0.0393 | 0.25 | 2.04 | 0.1533 |
| Advanced Stage | No vs. Yes | 1 | 0.7111 | 0.0915 | 0.5318 | 0.8904 | 60.43 | <0.0001 |
| GAD Summed Score | 1 | 0.0373 | 0.0056 | 0.0264 | 0.0483 | 44.47 | <0.0001 | |
| Age | 1 | −0.0007 | 0.0027 | −0.006 | 0.0046 | 0.07 | 0.7942 | |
| Sex | F vs. M | 1 | 0.0881 | 0.0738 | −0.0566 | 0.2327 | 1.42 | 0.2328 |
| Advanced Stage | No vs. Yes | 1 | 0.7011 | 0.0915 | 0.5217 | 0.8805 | 58.68 | <0.0001 |
| PHQ-9 SUMMED SCORE | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cutoff | ≥11 | ≥12 | ≥13 | ≥14 | ≥15 | ≥16 | ≥17 | ≥18 | |||||||||
| +ve | −ve | +ve | −ve | +ve | −ve | +ve | −ve | +ve | −ve | +ve | −ve | +ve | −ve | +ve | −ve | ||
| ≥1 | 49% | 7% | 49% | 8% | 52% | 8% | 56% | 8% | 59% | 8% | 60% | 9% | 67% | 9% | 70% | 9% | |
| ESAS Depression | ≥2 | 50% | 10% | 50% | 11% | 53% | 11% | 57% | 11% | 60% | 12% | 61% | 12% | 68% | 12% | 71% | 13% |
| ≥3 | 53% | 11% | 52% | 12% | 56% | 11% | 59% | 12% | 63% | 12% | 63% | 13% | 70% | 13% | 73% | 14% | |
| ≥4 | 53% | 13% | 53% | 15% | 56% | 14% | 60% | 15% | 63% | 15% | 64% | 16% | 71% | 16% | 73% | 17% | |
| ≥5 | 58% | 12% | 58% | 13% | 61% | 12% | 64% | 13% | 68% | 13% | 68% | 14% | 74% | 14% | 77% | 15% | |
| ≥6 | 58% | 12% | 58% | 13% | 61% | 12% | 64% | 13% | 68% | 13% | 68% | 14% | 74% | 14% | 77% | 15% | |
| Depression | Anxiety | |||||
|---|---|---|---|---|---|---|
| Performance Index | ESAS-D | PHQ-9 | Two-Step | ESAS-A | GAD-7 | Two-Step |
| Cutoff | ≥2 | ≥15 | ≥2 → ≥15 | ≥2 | ≥15 | ≥2 → ≥15 |
| Sensitivity | 0.92 | 0.47 | - | 0.92 | 0.26 | - |
| Specificity | 0.21 | 0.81 | - | 0.13 | 0.80 | - |
| Likelihood ratio positive | 1.16 | 2.55 | - | 1.06 | 1.31 | - |
| Likelihood ratio negative | 0.40 | 0.65 | - | 0.60 | 0.92 | - |
| Post-test probability positive | 37% | 57% | 60% | 24% | 28% | 29% |
| Post-test probability negative | 17% | 25% | 12% | 15% | 22% | 14% |
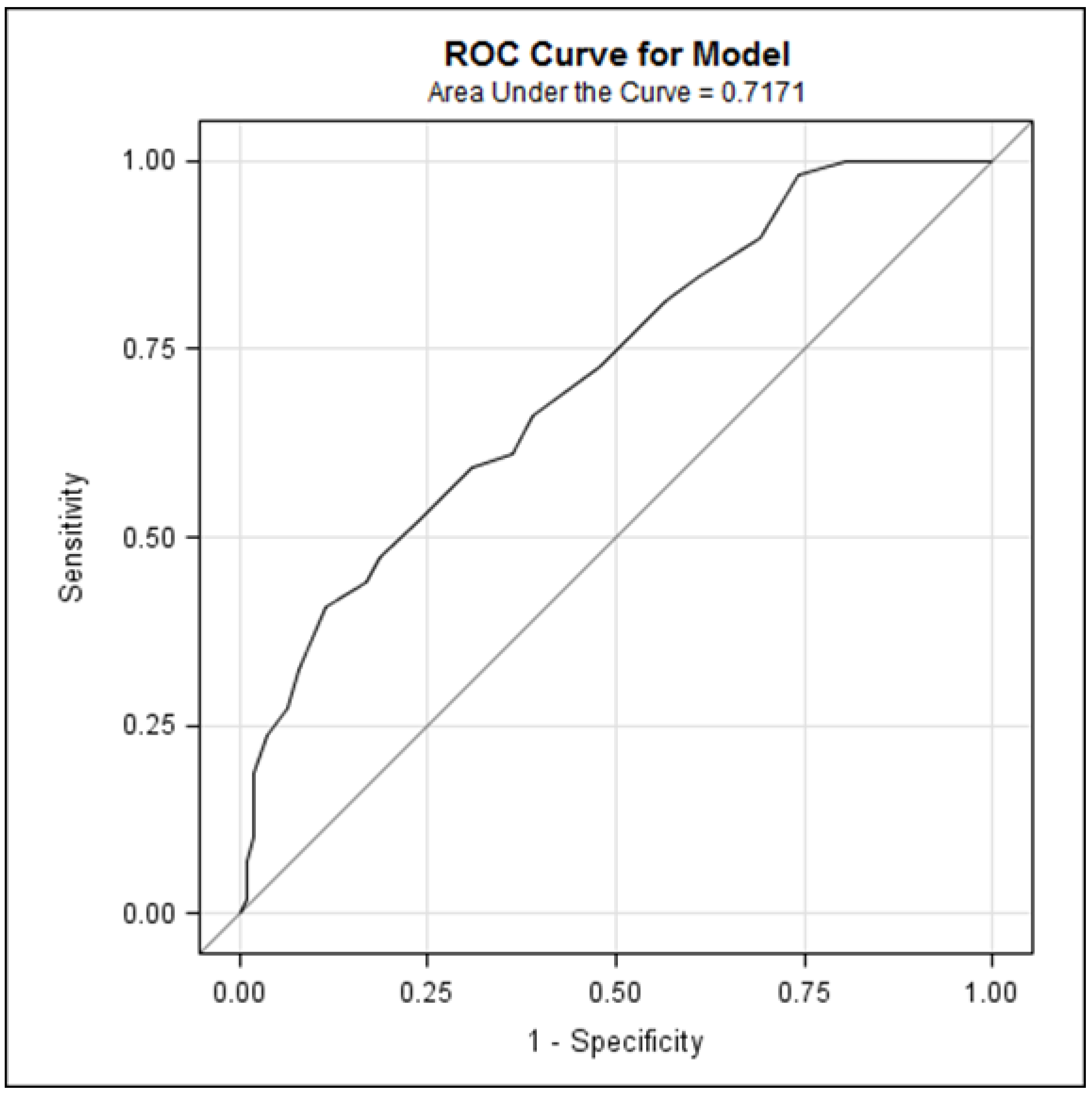
| Outcome = Diagnosis of depression | Area Under the Curve (AUC) | −2 Log likelihood | Deviance | p value |
| ESAS Depression Score | 0.70 | 202.69 | 8.87 | Top of Form |
| ESAS Depression Score + PHQ Summed Score | 0.73 | 193.82 | 0.003 | |
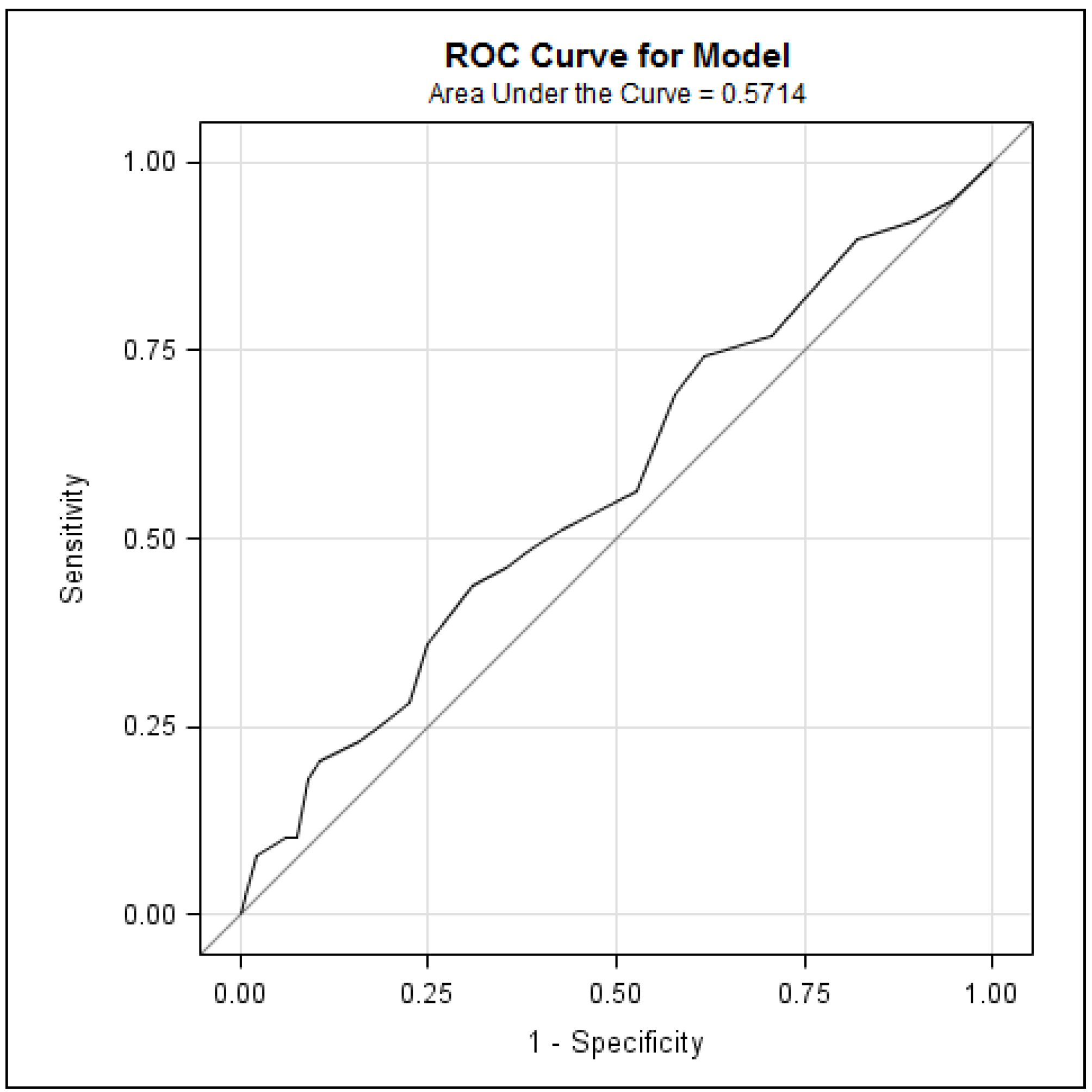
| Outcome = Diagnosis of anxiety | AUC | −2 Log likelihood | Deviance | p value |
| ESAS Anxiety Score | 0.55 | 183.50 | 1.51 | Top of Form |
| ESAS Anxiety Score + GAD Summed Score | 0.57 | 181.98 | 0.22 |
| GAD-7 Cutoff | True Positives | True Negatives | False Positives | False Negatives | Sensitivity | Specificity | PPV | NPV | Likelihood Ratios | |
|---|---|---|---|---|---|---|---|---|---|---|
| No. of Correctly Predicted Events | No. of Correctly Predicted Non-Events | No. of Non-Events Predicted as Events | No. of Events Predicted as Non-Events | LR Positive | LR Negative | |||||
| ≥0 | 39 | 0 | 133 | 0 | 1.00 | 0.00 | 0.23 | ― | 1.00 | ― |
| ≥1 | 37 | 7 | 126 | 2 | 0.95 | 0.05 | 0.23 | 0.78 | 1.00 | 0.97 |
| ≥2 | 36 | 14 | 119 | 3 | 0.92 | 0.11 | 0.23 | 0.82 | 1.03 | 0.73 |
| ≥3 | 35 | 24 | 109 | 4 | 0.90 | 0.18 | 0.24 | 0.86 | 1.10 | 0.57 |
| ≥4 | 33 | 30 | 103 | 6 | 0.85 | 0.23 | 0.24 | 0.83 | 1.09 | 0.68 |
| ≥5 | 30 | 39 | 94 | 9 | 0.77 | 0.29 | 0.24 | 0.81 | 1.09 | 0.79 |
| ≥6 | 29 | 51 | 82 | 10 | 0.74 | 0.38 | 0.26 | 0.84 | 1.21 | 0.67 |
| ≥7 | 27 | 56 | 77 | 12 | 0.69 | 0.42 | 0.26 | 0.82 | 1.20 | 0.73 |
| ≥8 | 22 | 63 | 70 | 17 | 0.56 | 0.47 | 0.24 | 0.79 | 1.07 | 0.92 |
| ≥9 | 20 | 76 | 57 | 19 | 0.51 | 0.57 | 0.26 | 0.80 | 1.20 | 0.85 |
| ≥10 | 19 | 81 | 52 | 20 | 0.49 | 0.61 | 0.27 | 0.80 | 1.25 | 0.84 |
| ≥11 | 18 | 86 | 47 | 21 | 0.46 | 0.65 | 0.28 | 0.80 | 1.31 | 0.83 |
| ≥12 | 17 | 92 | 41 | 22 | 0.44 | 0.69 | 0.29 | 0.81 | 1.41 | 0.82 |
| ≥13 | 14 | 100 | 33 | 25 | 0.36 | 0.75 | 0.30 | 0.80 | 1.45 | 0.85 |
| ≥14 | 11 | 103 | 30 | 28 | 0.28 | 0.77 | 0.27 | 0.79 | 1.25 | 0.93 |
| ≥15 | 10 | 107 | 26 | 29 | 0.26 | 0.80 | 0.28 | 0.79 | 1.31 | 0.92 |
| ≥16 | 9 | 112 | 21 | 30 | 0.23 | 0.84 | 0.30 | 0.79 | 1.46 | 0.91 |
| ≥17 | 8 | 119 | 14 | 31 | 0.21 | 0.89 | 0.36 | 0.79 | 1.95 | 0.89 |
| ≥18 | 7 | 121 | 12 | 32 | 0.18 | 0.91 | 0.37 | 0.79 | 1.99 | 0.90 |
| ≥19 | 4 | 123 | 10 | 35 | 0.10 | 0.92 | 0.29 | 0.78 | 1.36 | 0.97 |
| ≥20 | 4 | 125 | 8 | 35 | 0.10 | 0.94 | 0.33 | 0.78 | 1.71 | 0.95 |
| ≥21 | 3 | 130 | 3 | 36 | 0.08 | 0.98 | 0.50 | 0.78 | 3.41 | 0.94 |
| GAD-7 Summed Score | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cutoff | ≥11 | ≥12 | ≥13 | ≥14 | ≥15 | ≥16 | ≥17 | ≥18 | |||||||||
| +ve | −ve | +ve | −ve | +ve | −ve | +ve | −ve | +ve | −ve | +ve | −ve | +ve | −ve | +ve | −ve | ||
| ≥1 | 29% | 8% | 31% | 8% | 31% | 8% | 28% | 9% | 29% | 9% | 32% | 9% | 38% | 8% | 39% | 8% | |
| ESAS Anxiety | ≥2 | 29% | 13% | 31% | 13% | 31% | 13% | 28% | 14% | 29% | 14% | 32% | 14% | 38% | 14% | 39% | 14% |
| ≥3 | 26% | 28% | 28% | 27% | 28% | 28% | 25% | 30% | 26% | 30% | 28% | 30% | 35% | 29% | 35% | 29% | |
| ≥4 | 28% | 19% | 30% | 19% | 31% | 19% | 28% | 21% | 29% | 21% | 31% | 21% | 37% | 20% | 38% | 20% | |
| ≥5 | 29% | 18% | 31% | 17% | 32% | 18% | 29% | 19% | 30% | 19% | 32% | 19% | 38% | 19% | 39% | 19% | |
| ≥6 | 29% | 18% | 31% | 17% | 32% | 18% | 29% | 19% | 30% | 19% | 32% | 19% | 38% | 19% | 39% | 19% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gascon, B.; Elman, J.; Macedo, A.; Leung, Y.; Rodin, G.; Li, M. Two-Step Screening for Depression and Anxiety in Patients with Cancer: A Retrospective Validation Study Using Real-World Data. Curr. Oncol. 2024, 31, 6488-6501. https://doi.org/10.3390/curroncol31110481
Gascon B, Elman J, Macedo A, Leung Y, Rodin G, Li M. Two-Step Screening for Depression and Anxiety in Patients with Cancer: A Retrospective Validation Study Using Real-World Data. Current Oncology. 2024; 31(11):6488-6501. https://doi.org/10.3390/curroncol31110481
Chicago/Turabian StyleGascon, Bryan, Joel Elman, Alyssa Macedo, Yvonne Leung, Gary Rodin, and Madeline Li. 2024. "Two-Step Screening for Depression and Anxiety in Patients with Cancer: A Retrospective Validation Study Using Real-World Data" Current Oncology 31, no. 11: 6488-6501. https://doi.org/10.3390/curroncol31110481
APA StyleGascon, B., Elman, J., Macedo, A., Leung, Y., Rodin, G., & Li, M. (2024). Two-Step Screening for Depression and Anxiety in Patients with Cancer: A Retrospective Validation Study Using Real-World Data. Current Oncology, 31(11), 6488-6501. https://doi.org/10.3390/curroncol31110481