Combination of Osimertinib and Olaparib Therapy to Treat Non-Small Cell Lung Cancer and High-Grade Serous Ovarian Carcinoma: A Case Report

Abstract
1. Introduction
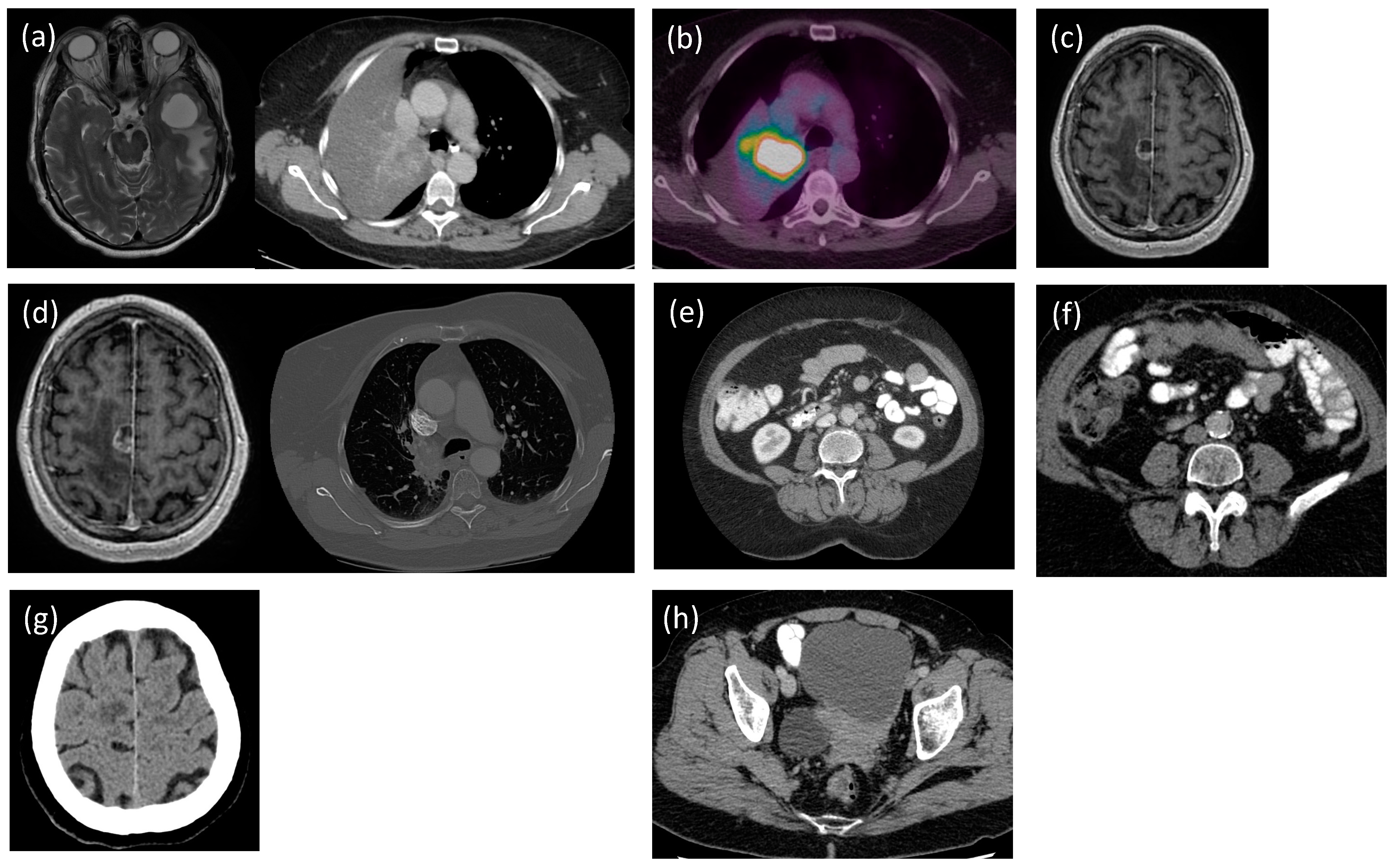
2. Case Presentation
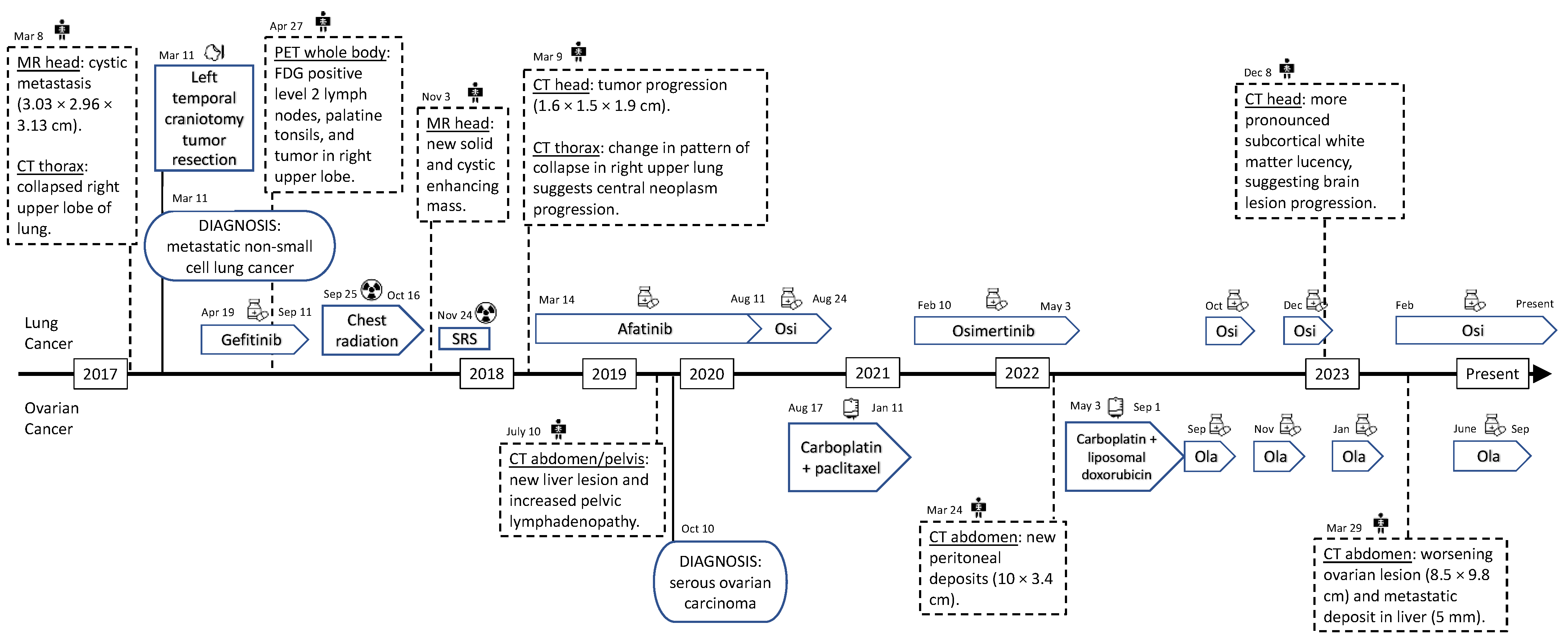
2.1. Non-Small Cell Lung Cancer (NSCLC)
2.1.1. Initial Presentation and Diagnosis
2.1.2. Therapeutic Interventions
2.2. Ovarian Serous Carcinoma
2.2.1. Initial Presentation and Diagnosis
2.2.2. Therapeutic Interventions
2.3. Follow-Up and Outcomes
3. Discussion
3.1. Comparison to Literature
3.2. Alternating and Concurrent Administrations
3.3. Other Drug Combinations
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vogt, A.; Schmid, S.; Heinimann, K.; Frick, H.; Herrmann, C.; Cerny, T.; Omlin, A. Multiple primary tumours: Challenges and approaches, a review. ESMO Open 2017, 2, e000172. [Google Scholar] [CrossRef] [PubMed]
- Mariniello, A.; Ghisoni, E.; Righi, L.; Catino, A.; Chiari, R.; Del Conte, A.; Barbieri, F.; Cecere, F.; Gelibter, A.; Giajlevra, M.; et al. Women with Synchronous or Metachronous Lung and Ovarian Cancer: A Multi-Institutional Report. In Vivo 2019, 33, 2021–2026. [Google Scholar] [CrossRef] [PubMed]
- Ganti, A.K.; Klein, A.B.; Cotarla, I.; Seal, B.; Chou, E. Update of Incidence, Prevalence, Survival, and Initial Treatment in Patients With Non–Small Cell Lung Cancer in the US. JAMA Oncol. 2021, 7, 1824–1832. [Google Scholar] [CrossRef] [PubMed]
- Karachaliou, N.; Fernandez-Bruno, M.; Bracht, J.W.P.; Rosell, R. EGFR first- and second-generation TKIs—There is still place for them in EGFR -mutant NSCLC patients. Transl. Cancer Res. 2019, 8 (Suppl. 1), S23. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-S.; Milone, M.; Seetharamu, N. Osimertinib in EGFR-Mutated Lung Cancer: A Review of the Existing and Emerging Clinical Data. OncoTargets Ther. 2021, 14, 4579–4597. [Google Scholar] [CrossRef] [PubMed]
- Niwa, H.; Nakahara, Y.; Sasaki, J.; Masuda, N. A promising response to osimertinib in a patient with erlotinib-resistant lung adenocarcinoma with an uncommon EGFR mutation. Case Rep. 2018, 2018, bcr-2017. [Google Scholar] [CrossRef] [PubMed]
- Soria, J.-C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in Untreated EGFR-Mutated Advanced Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Trabert, B.; DeSantis, C.E.; Miller, K.D.; Samimi, G.; Runowicz, C.D.; Gaudet, M.M.; Jemal, A.; Siegel, R.L. Ovarian Cancer Statistics, 2018. CA Cancer J. Clin. 2018, 68, 284–296. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.; Colombo, N.; Scambia, G.; Kim, B.-G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; Sonke, G.S.; et al. Maintenance Olaparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2018, 379, 2495–2505. [Google Scholar] [CrossRef] [PubMed]
- Poveda, A.; Floquet, A.; Ledermann, J.A.; Asher, R.; Penson, R.T.; Oza, A.M.; Korach, J.; Huzarski, T.; Pignata, S.; Frielander, M.; et al. Olaparib tablets as maintenance therapy in patients with platinum-sensitive relapsed ovarian cancer and a BRCA1/2 mutation (SOLO2/ENGOT-Ov21): A final analysis of a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol. 2021, 22, 620–631. [Google Scholar] [CrossRef] [PubMed]
- Eide, I.J.Z.; Helland, A.; Ekman, S.; Mellemgaard, A.; Hansen, K.H.; Cicenas, S.; Koivunen, J.; Grønberg, B.H.; Brustugen, O.T. Osimertinib in T790M-positive and -negative patients with EGFR-mutated advanced non-small cell lung cancer (the TREM-study). Lung Cancer 2020, 143, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Rodier, T.; Puszkiel, A.; Cardoso, E.; Balakirouchenane, D.; Narjoz, C.; Arrondeau, J.; Fallet, V.; Khoudour, N.; Guidi, M.; Vidal, M.; et al. Exposure–Response Analysis of Osimertinib in Patients with Advanced Non-Small-Cell Lung Cancer. Pharmaceutics 2022, 14, 1844. [Google Scholar] [CrossRef] [PubMed]
- Velev, M.; Puszkiel, A.; Blanchet, B.; de Percin, S.; Delanoy, N.; Medioni, J.; Gervais, C.; Balakirouchenane, D.; Khoudour, N.; Pautier, P.; et al. Association between Olaparib Exposure and Early Toxicity in BRCA-Mutated Ovarian Cancer Patients: Results from a Retrospective Multicenter Study. Pharmaceuticals 2021, 14, 804. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Wang, Y.; Wu, H.; Zhou, S.; Li, S.; Meng, X.; Tao, R.; Yu, J. Olaparib Combined with Dacomitinib in Osimer-Tinib-Resistant Brain and Leptomeningeal Metastases from Non-Small Cell Lung Cancer: A Case Report and Systematic Review. Front. Oncol. 2023, 12, 877279. Available online: https://www.frontiersin.org/articles/10.3389/fonc.2022.877279 (accessed on 3 September 2023). [CrossRef]

{kind=link}
{kind=link}
| Name | Target | Start Date | End Date | Cycles | Dose | Side Effects | |
|---|---|---|---|---|---|---|---|
| Targeted Drug Therapy | Gefitinib | Lung cancer | 19 April 2017 | 11 September 2017 | 4 | 250 mg/day, daily | Rash, diarrhea, dysuria, hematuria |
| Afatinib | Lung cancer | 14 March 2018 | 11 August 2020 | 32 | 20–30 mg/day, daily | Rash, diarrhea, anaphylaxis | |
| Osimertinib | Lung cancer | 10 August 2020 | Present | 31 | 80 mg/day, daily | None | |
| Olaparib | Ovarian cancer | 1 September 2022 | 21 September 2023 | 6 | 2 × 150 mg BID, total 300 mg/day | Nausea, vomiting, taste distortion, poor appetite, fatigue | |
| Chemotherapy | Carboplatin + Paclitaxel | Ovarian cancer | 17 August 2020 | 11 January 2021 | 6 | Carboplatin: 5 AUC Paclitaxel: 175 mg/m2 | Fatigue, nausea, diaphoresis, constipation, diarrhea, dysgeusia, neuropathy |
| Carboplatin + Liposomal doxorubicin | Ovarian cancer | 3 May 2022 | 1 September 2022 | 4 | Carboplatin: 5 AUC Liposomal doxorubicin: 30 mg/m2 | Fatigue, nausea, vomiting, heartburn, diarrhea, dysgeusia, neuropathy | |
| Radiation Therapy | Chest radiation therapy | Lung cancer | 25 September 2017 | 16 October 2017 | - | 45 Gy in 15 fractions | None |
| Stereotactic radiosurgery | Brain metastasis from primary lung cancer | 24 November 2017 | 24 November 2017 | - | 18 Gy in 1 fraction | Weakness |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, J.; Welch, S.; Sanatani, M.; Ramadan, S. Combination of Osimertinib and Olaparib Therapy to Treat Non-Small Cell Lung Cancer and High-Grade Serous Ovarian Carcinoma: A Case Report. Curr. Oncol. 2024, 31, 558-565. https://doi.org/10.3390/curroncol31010039
Lin J, Welch S, Sanatani M, Ramadan S. Combination of Osimertinib and Olaparib Therapy to Treat Non-Small Cell Lung Cancer and High-Grade Serous Ovarian Carcinoma: A Case Report. Current Oncology. 2024; 31(1):558-565. https://doi.org/10.3390/curroncol31010039
Chicago/Turabian StyleLin, Jane, Stephen Welch, Michael Sanatani, and Sherif Ramadan. 2024. "Combination of Osimertinib and Olaparib Therapy to Treat Non-Small Cell Lung Cancer and High-Grade Serous Ovarian Carcinoma: A Case Report" Current Oncology 31, no. 1: 558-565. https://doi.org/10.3390/curroncol31010039
APA StyleLin, J., Welch, S., Sanatani, M., & Ramadan, S. (2024). Combination of Osimertinib and Olaparib Therapy to Treat Non-Small Cell Lung Cancer and High-Grade Serous Ovarian Carcinoma: A Case Report. Current Oncology, 31(1), 558-565. https://doi.org/10.3390/curroncol31010039