Investigation of the Incidence and Geographic Distribution of Bone and Soft Tissue Sarcomas in Canada: A National Population-Based Study


 ,
, 
Abstract
1. Introduction
2. Materials and Methods
3. Mandatory Data Rounding
4. Results
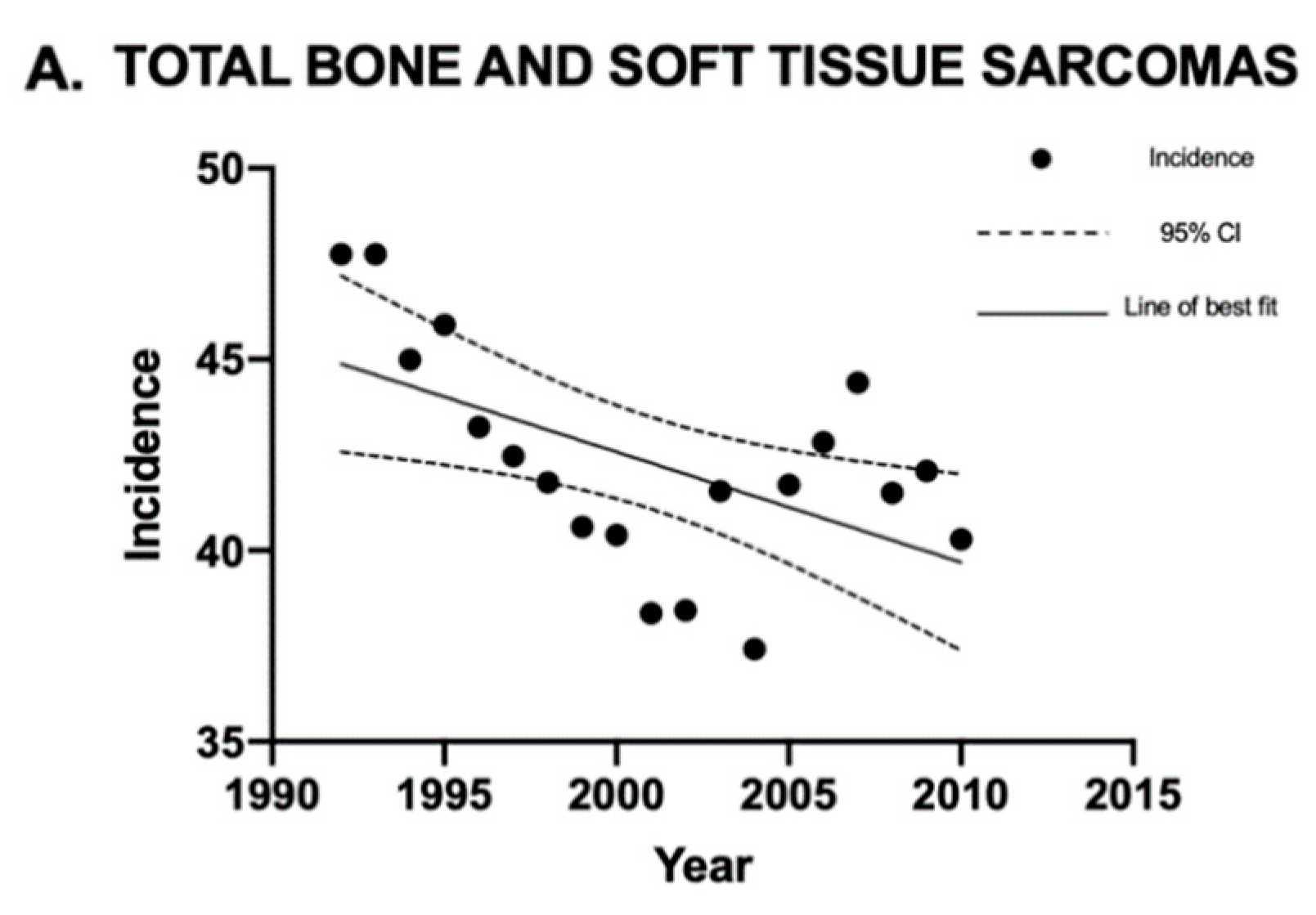
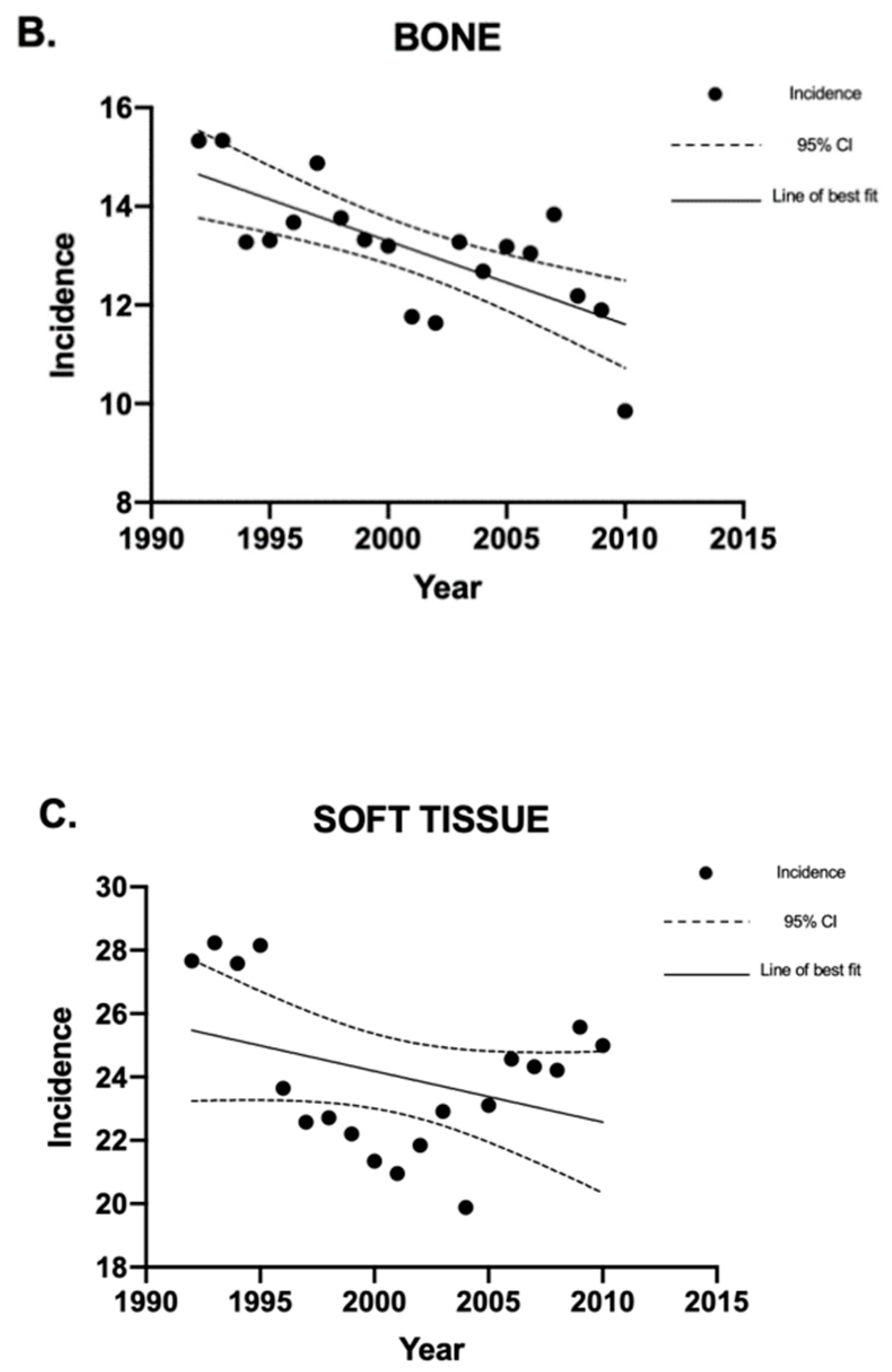
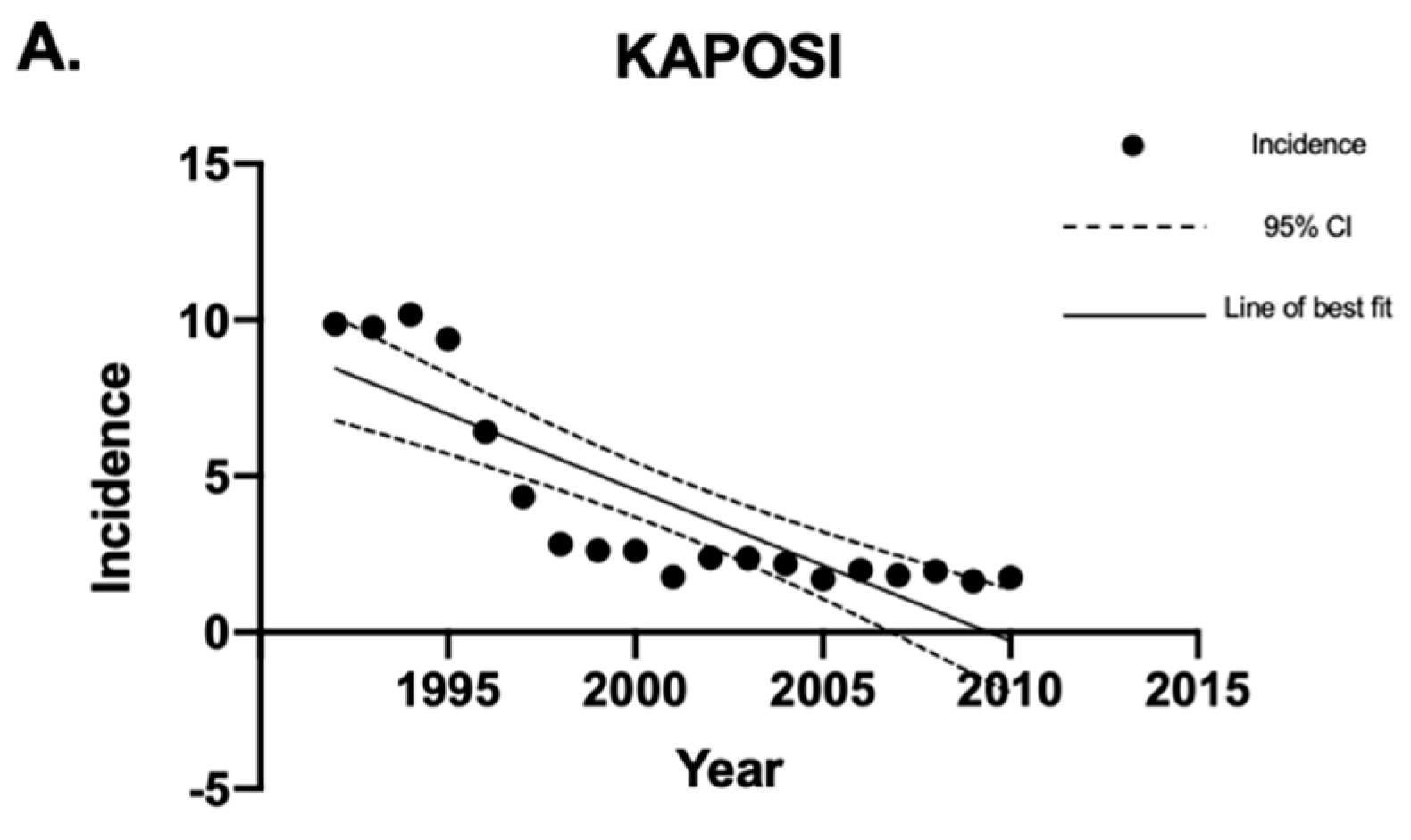
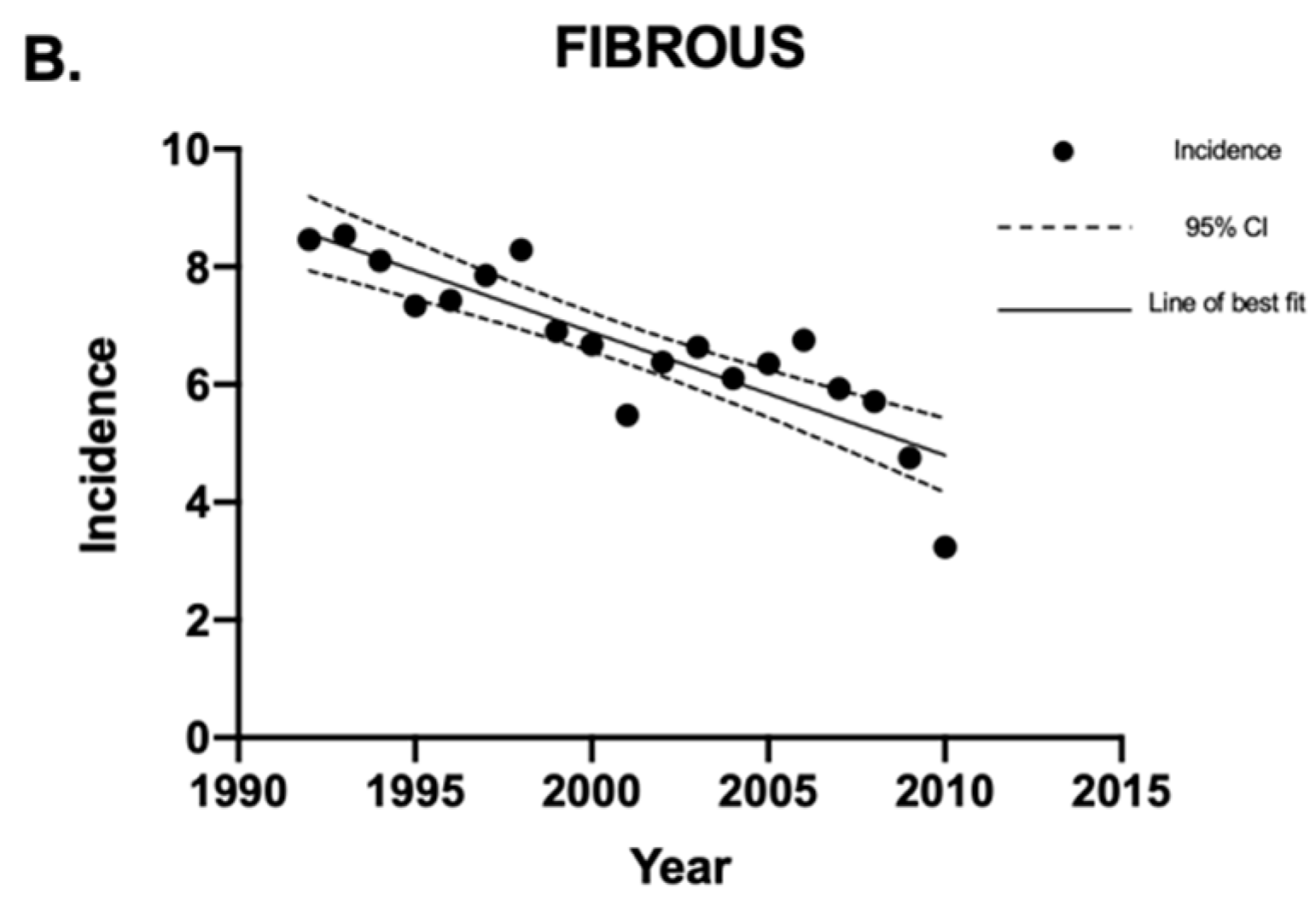
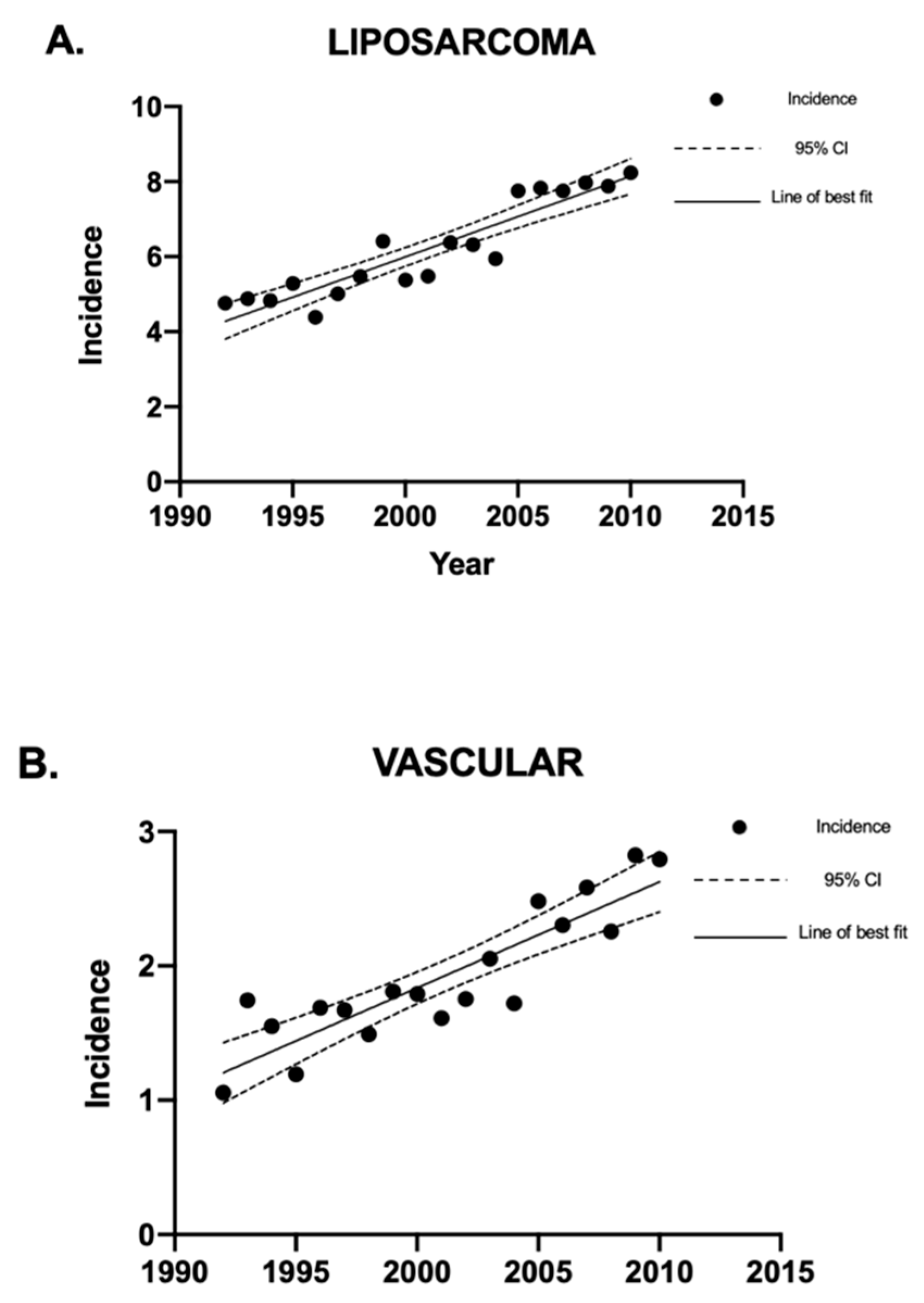
4.1. Incidence of Sarcomas in Canada between 1992 and 2010
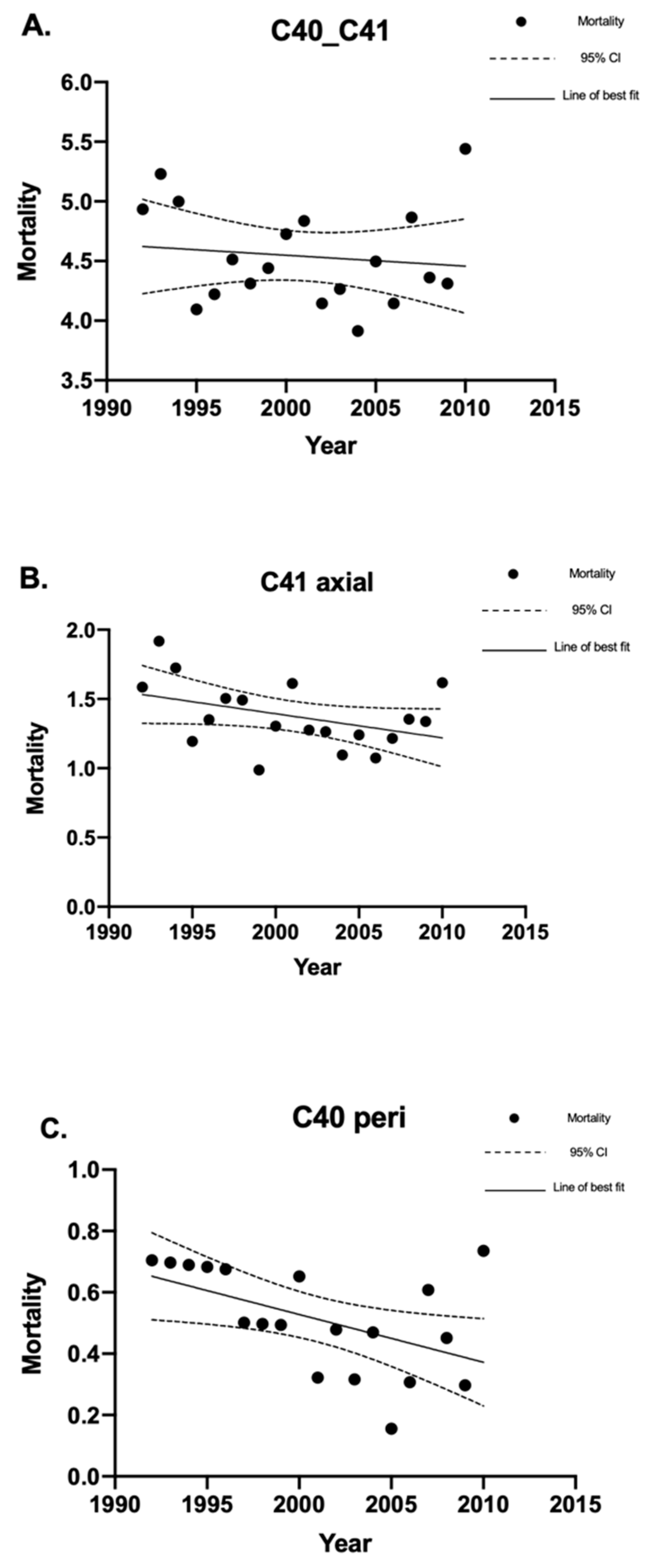
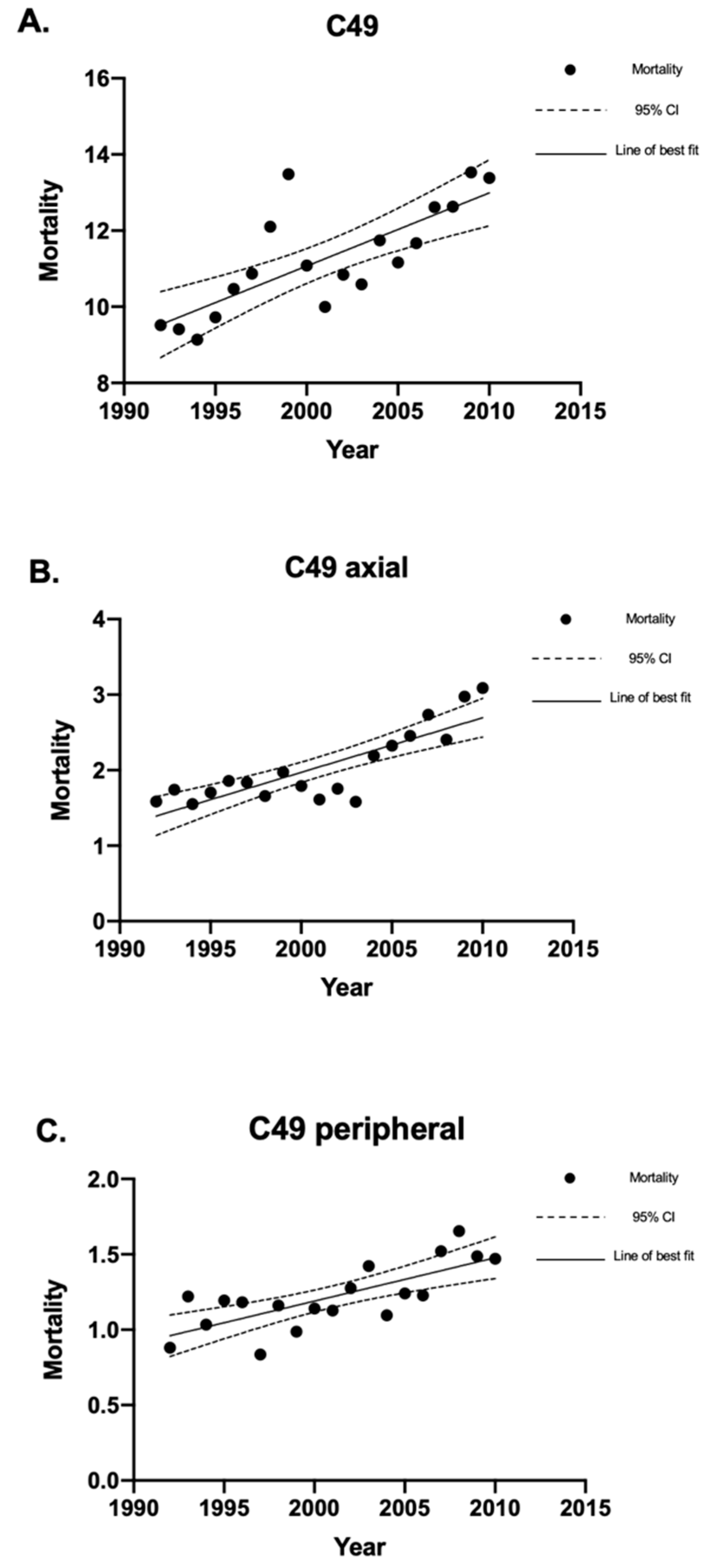
4.2. Mortality of Sarcomas in Canada between 1992 and 2010
4.2.1. Bone Sarcoma Mortality
4.2.2. Soft Tissue Sarcoma Mortality
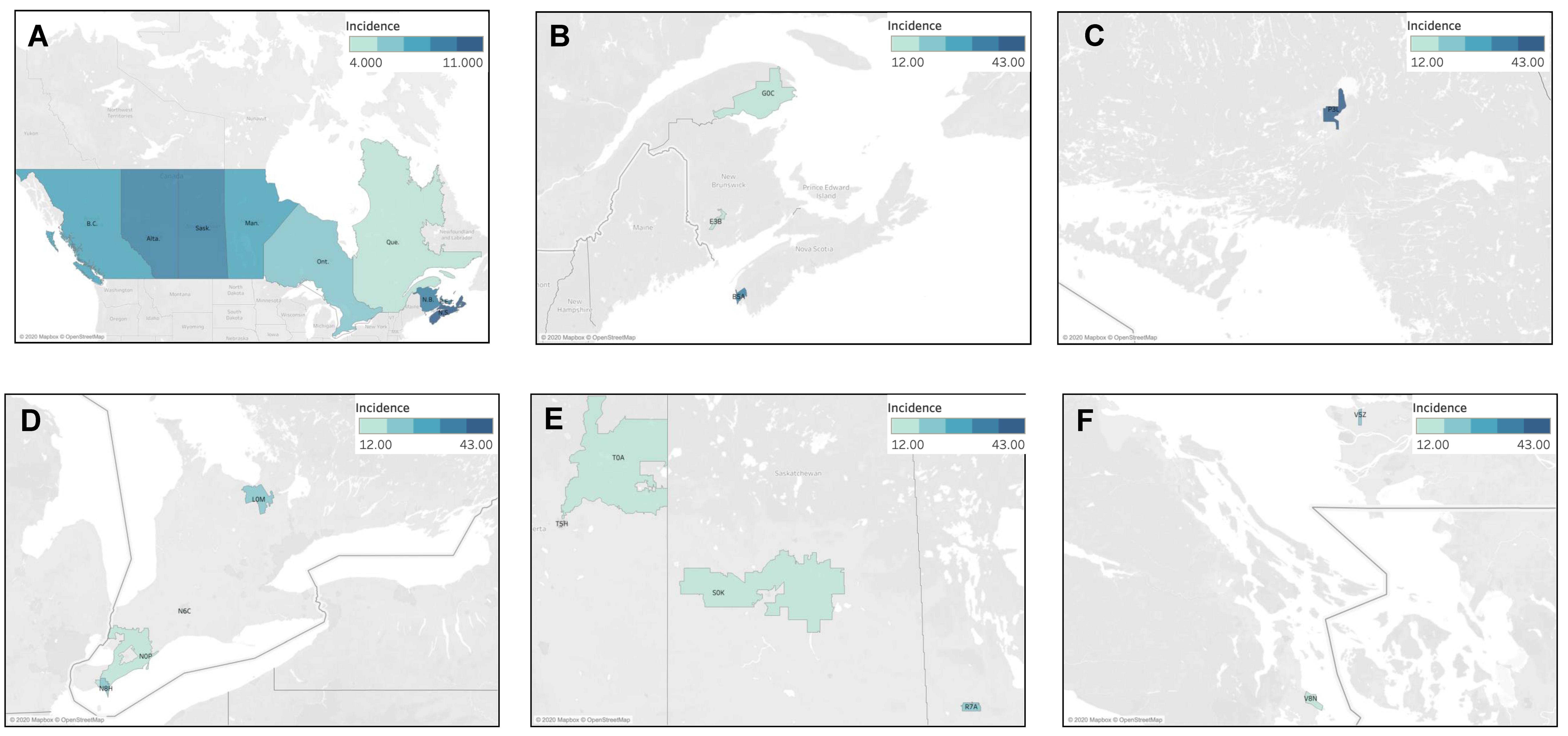
4.3. Geographic Analysis
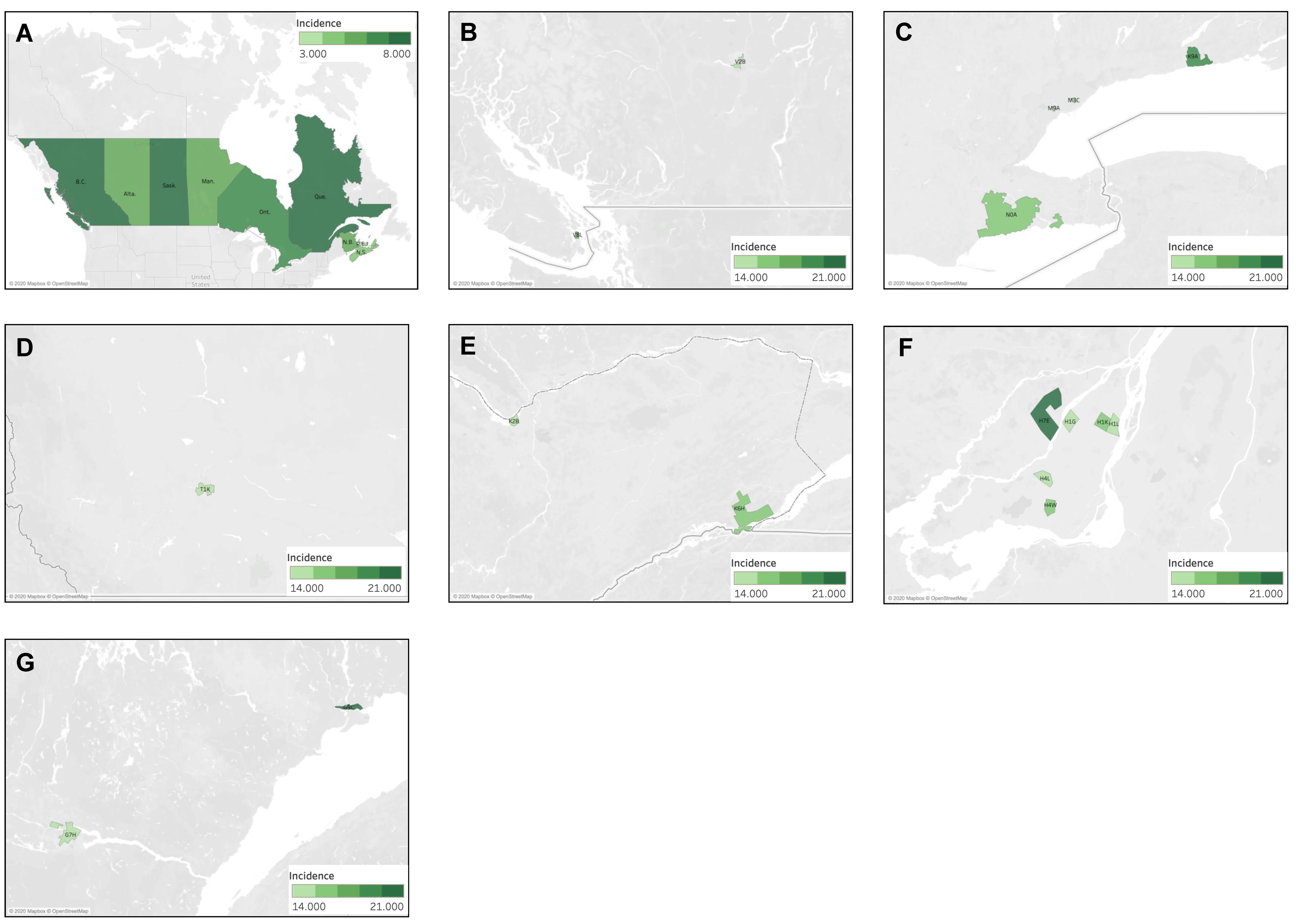
4.3.1. Geographic Distribution of Fibrous Sarcoma Cases
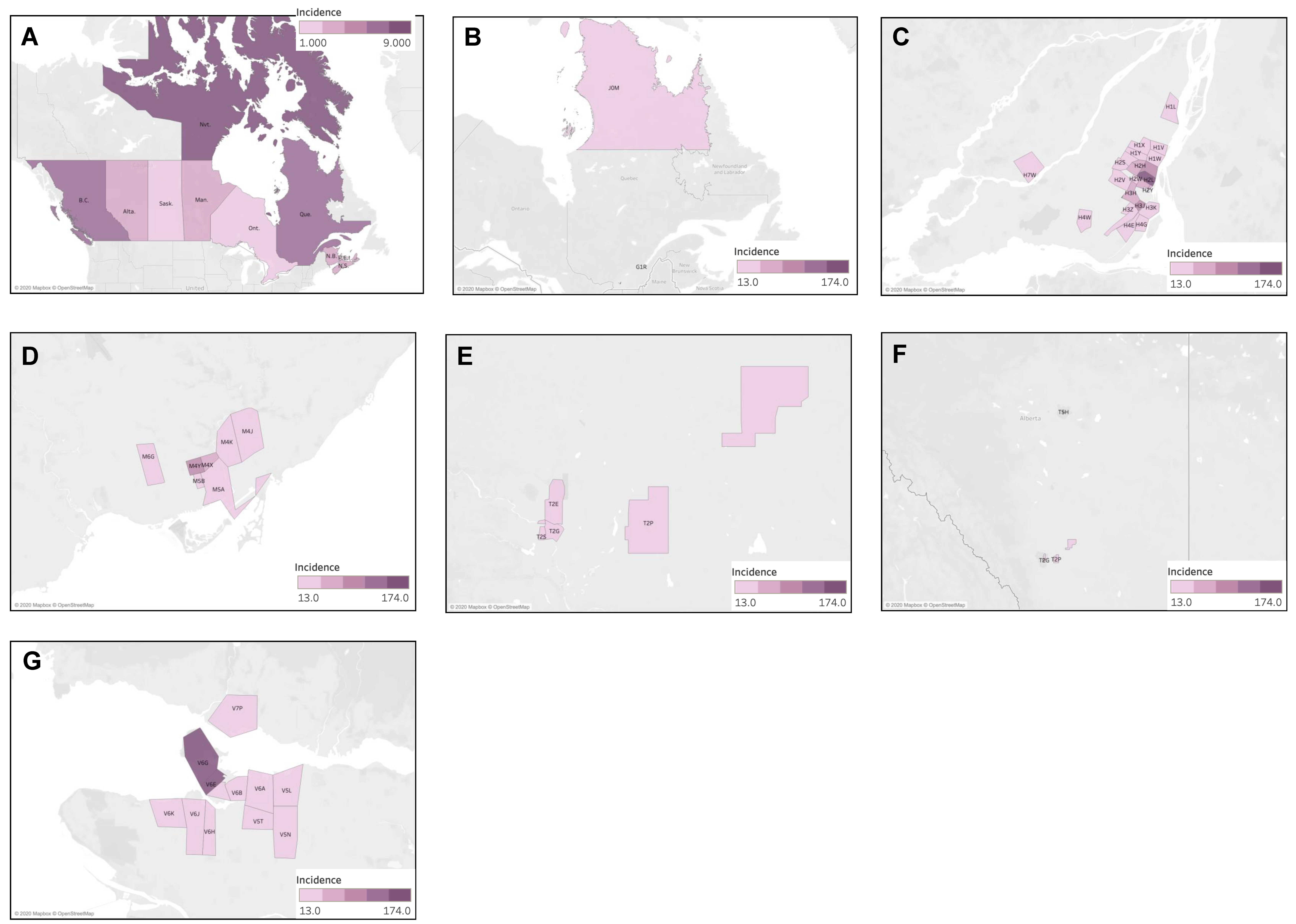
4.3.2. Geographic Distribution of Kaposi Sarcoma Cases
4.3.3. Geographic Distribution of Liposarcoma Cases
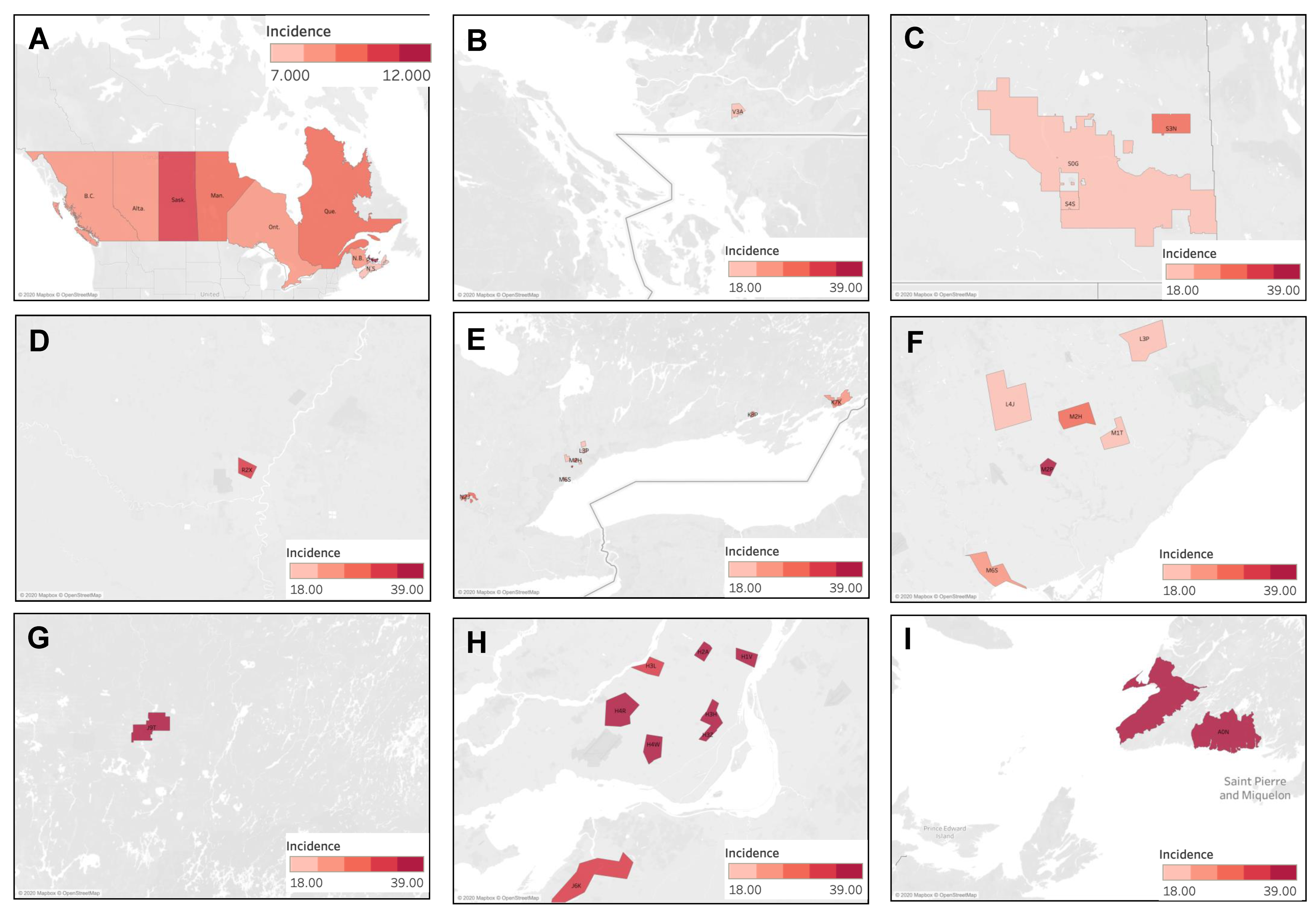
4.3.4. Geographic Distribution of Muscle Sarcoma Cases
4.4. Analysis by Ethnicity and Socioeconomic Status
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lahat, G.; Lazar, A.; Lev, D. Sarcoma epidemiology and etiology: Potential environmental and genetic factors. Surg. Clin. N. Am. 2008, 88, 451–481. [Google Scholar] [CrossRef] [PubMed]
- Burningham, Z.; Hashibe, M.; Spector, L.; Schiffman, J.D. The Epidemiology of Sarcoma. Clin. Sarcoma Res. 2012, 2, 14. [Google Scholar] [CrossRef] [PubMed]
- Stiller, C.A.; Trama, A.; Serraino, D.; Rossi, S.; Navarro, C.; Chirlaque, M.D.; Casali, P.G.; RARECARE Working Group. Descriptive epidemiology of sarcomas in Europe: Report from the RARECARE project. Eur. J. Cancer 2013, 49, 684–695. [Google Scholar] [CrossRef] [PubMed]
- Beckingsale, T.B.; Shaw, C. Epidemiology of bone and soft-tissue sarcomas. Orthop. Trauma 2017, 31, 144–150. [Google Scholar] [CrossRef]
- Clark, M.A.; Fisher, C.; Judson, I.; Thomas, J.M. Soft-Tissue Sarcomas in Adults. N. Engl. J. Med. 2005, 353, 701–711. [Google Scholar] [CrossRef] [PubMed]
- Mirabello, L.; Troisi, R.J.; Savage, S.A. International osteosarcoma incidence patterns in children and adolescents, middle ages and elderly persons. Int. J. Cancer 2009, 125, 229–234. [Google Scholar] [CrossRef]
- Eyre, R.; Feltbower, R.G.; James, P.W.; Blakey, K.; Mubwandarikwa, E.; Forman, D.; A McKinney, P.; Pearce, M.S.; McNally, R.J. The epidemiology of bone cancer in 0–39 year olds in northern England, 1981–2002. BMC Cancer 2010, 10, 357. [Google Scholar] [CrossRef]
- Kumamoto, T.; Yamazaki, F.; Nakano, Y.; Tamura, C.; Tashiro, S.; Hattori, H.; Nakagawara, A.; Tsunematsu, Y. Medical guidelines for Li–Fraumeni syndrome 2019, version 1.1. Int. J. Clin. Oncol. 2021, 26, 2161–2178. [Google Scholar] [CrossRef]
- Strauss, S.; Frezza, A.; Abecassis, N.; Bajpai, J.; Bauer, S.; Biagini, R.; Bielack, S.; Blay, J.; Bolle, S.; Bonvalot, S.; et al. Bone sarcomas: ESMO–EURACAN–GENTURIS–ERN PaedCan Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2021, 32, 1520–1536. [Google Scholar] [CrossRef]
- Sampo, M.; Koivikko, M.; Taskinen, M.; Kallio, P.; Kivioja, A.; Tarkkanen, M.; Böhling, T. Incidence, epidemiology and treatment results of osteosarcoma in Finland—A nationwide population-based study. Acta Oncol. 2011, 50, 1206–1214. [Google Scholar] [CrossRef]
- Grønhøj, C.; Hjalgrim, L.; Jakobsen, K.K.; Charabi, B.; Mirian, C.; Laier, G.H.; Kiss, K.; Rechnitzer, C.; Friborg, J.; von Buchwald, C.; et al. Incidence of head and neck cancer in children: A Danish nationwide study from 1978 to 2014. Pediatr. Blood Cancer 2018, 65, e27037. [Google Scholar] [CrossRef]
- Finkelstein, M.M.; Kreiger, N. Radium in drinking water and risk of bone cancer in Ontario youths: A second study and combined analysis. Occup. Environ. Med. 1996, 53, 305–311. [Google Scholar] [CrossRef]
- Moss, M.E.; Kanarek, M.S.; Anderson, H.A.; Hanrahan, L.P.; Remington, P.L. Osteosarcoma, seasonality, and environmental factors in Wisconsin, 1979–1989. Arch. Environ. Health Int. J. 1995, 50, 235–241. [Google Scholar] [CrossRef]
- Valery, P.C.; Williams, G.; Sleigh, A.C.; Holly, E.A.; Kreiger, N.; Bain, C. Parental occupation and Ewing’s sarcoma: Pooled and meta-analysis. Int. J. Cancer 2005, 115, 799–806. [Google Scholar] [CrossRef]
- Hoar, S.K.; Blair, A.; Holmes, F.F.; Boysen, C.D.; Robel, R.J.; Hoover, R.; Fraumeni, J.F. Agricultural herbicide use and risk of lymphoma and soft-tissue sarcoma. JAMA 1986, 256, 1141–1147. [Google Scholar] [CrossRef]
- Hoppin, J.A.; Tolbert, P.E.; Flanders, W.D.; Zhang, R.H.; Daniels, D.S.; Ragsdale, B.D.; Brann, E.A. Occupational Risk Factors for Sarcoma Subtypes. Epidemiology 1999, 10, 300–306. [Google Scholar] [CrossRef]
- Wiklund, K.; Holm, L.E. Soft tissue sarcoma risk in Swedish agricultural and forestry workers. J. Natl. Cancer Inst. 1986, 76, 229–234. [Google Scholar]
- Merletti, F.; Richiardi, L.; Bertoni, F.; Ahrens, W.; Buemi, A.; Costa-Santos, C.; Eriksson, M.; Guénel, P.; Kaerlev, L.; Jöckel, K.-H.; et al. Occupational factors and risk of adult bone sarcomas: A multicentric case-control study in Europe. Int. J. Cancer 2006, 118, 721–727. [Google Scholar] [CrossRef]
- Hum, L.; Kreiger, N.; Finkelstein, M.M. The relationship between parental occupation and bone cancer risk in offspring. Int. J. Epidemiol. 1998, 27, 766–771. [Google Scholar] [CrossRef]
- Whelan, J.; McTiernan, A.; Cooper, N.; Wong, Y.K.; Francis, M.; Vernon, S.; Strauss, S.J. Incidence and survival of malignant bone sarcomas in England 1979–2007. Int. J. Cancer 2012, 131, E508–E517. [Google Scholar] [CrossRef]
- Lagacé, F.; Ghazawi, F.M.; Le, M.; Rahme, E.; Savin, E.; Zubarev, A.; Alakel, A.; Sasseville, D.; Moreau, L.; Meterissian, S.; et al. Analysis of incidence, mortality trends, and geographic distribution of breast cancer patients in Canada. Breast Cancer Res. Treat. 2019, 178, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Ghazawi, F.M.; Darwich, R.; Le, M.; Jfri, A.; Rahme, E.; Burnier, J.V.; Sasseville, D.; Burnier, M.N., Jr.; Litvinov, I.V. Incidence trends of conjunctival malignant melanoma in Canada. Br. J. Ophthalmol. 2020, 104, 23–25. [Google Scholar] [CrossRef] [PubMed]
- Ghazawi, F.M.; Lu, J.; Savin, E.; Zubarev, A.; Chauvin, P.; Sasseville, D.; Zeitouni, A.; Litvinov, I.V. Epidemiology and patient distribution of oral cavity and oropharyngeal SCC in Canada. J. Cutan. Med. Surg. 2020, 24, 340–349. [Google Scholar] [CrossRef] [PubMed]
- Darwich, R.; Ghazawi, F.M.; Rahme, E.; Alghazawi, N.; Burnier, J.V.; Sasseville, D.; Burnier, M.N.; Litvinov, I.V. Retinoblastoma incidence trends in Canada: A national comprehensive population-based study. J. Pediatr. Ophthalmol. Strabismus 2019, 56, 124–130. [Google Scholar] [CrossRef]
- Cattelan, L.; Ghazawi, F.M.; Le, M.; Savin, E.; Zubarev, A.; Lagacé, F.; Sasseville, D.; Waschke, K.; Litvinov, I.V. Investigating epidemiologic trends and the geographic distribution of patients with anal squamous cell carcinoma throughout Canada. Curr. Oncol. 2020, 27, 294–306. [Google Scholar] [CrossRef]
- Tsang, M.; Le, M.; Ghazawi, F.; Cyr, J.; Alakel, A.; Rahme, E.; Lagacé, F.; Netchiporouk, E.; Moreau, L.; Zubarev, A.; et al. Multiple myeloma epidemiology and patient geographic distribution in Canada: A population study. Cancer 2019, 125, 2435–2444. [Google Scholar] [CrossRef]
- Cattelan, L.; Ghazawi, F.M.; Le, M.; Lagacé, F.; Savin, E.; Zubarev, A.; Gantchev, J.; Tomaszewski, M.; Sasseville, D.; Waschke, K.; et al. Epidemiologic trends and geographic distribution of esophageal cancer in Canada: A national population-based study. Cancer Med. 2020, 9, 401–417. [Google Scholar] [CrossRef]
- Gage, M.M.; Nagarajan, N.; Ruck, J.M.; Canner, J.K.; Khan, S.; Giuliano, K.; Gani, F.; Wolfgang, C.; Johnston, F.M.; Ahuja, N. Sarcomas in the United States: Recent trends and a call for improved staging. Oncotarget 2019, 10, 2462–2474. [Google Scholar] [CrossRef]
- Honoré, C.; Méeus, P.; Stoeckle, E.; Bonvalot, S. Soft tissue sarcoma in France in 2015: Epidemiology, classification and organization of clinical care. J. Visc. Surg. 2015, 152, 223–230. [Google Scholar] [CrossRef]
- Bessen, T.; E Caughey, G.; Shakib, S.; Potter, J.A.; Reid, J.; Farshid, G.; Roder, D.; Neuhaus, S.J. A population-based study of soft tissue sarcoma incidence and survival in Australia: An analysis of 26,970 cases. Cancer Epidemiol. 2019, 63, 101590. [Google Scholar] [CrossRef]
- De Pinieux, G.; Karanian, M.; Le Loarer, F.; Le Guellec, S.; Chabaud, S.; Terrier, P.; Bouvier, C.; Batistella, M.; Neuville, A.; Robin, Y.-M.; et al. Nationwide incidence of sarcomas and connective tissue tumors of intermediate malignancy over four years using an expert pathology review network. PLoS ONE 2021, 16, e0246958. [Google Scholar] [CrossRef]
- Zaikova, O.; Hall, K.S.; Styring, E.; Eriksson, M.; Trovik, C.S.; Bergh, P.; Bjerkehagen, B.; Skorpil, M.; Weedon-Fekjaer, H.; Bauer, H.C. Referral patterns, treatment and outcome of high-grade malignant bone sarcoma in Scandinavia—SSG Central Register 25 years’ experience. J. Surg. Oncol. 2015, 112, 853–860. [Google Scholar] [CrossRef]
- Mulita, F.; Verras, G.; Liolis, E.; Tchabashvili, L.; Kehagias, D.; Kaplanis, C.; Perdikaris, I.; Kehagias, I. Recurrent retroperitoneal liposarcoma: A case report and literature review. Clin. Case Rep. 2021, 9, e04717. [Google Scholar] [CrossRef]
- Toro, J.R.; Travis, L.B.; Wu, H.J.; Zhu, K.; Fletcher, C.D.M.; Devesa, S.S. Incidence patterns of soft tissue sarcomas, regardless of primary site, in the surveillance, epidemiology and end results program, 1978–2001: An analysis of 26,758 cases. Int. J. Cancer 2006, 119, 2922–2930. [Google Scholar] [CrossRef]
- Rich, A.J.; Lachowsky, N.J.; Sereda, P.; Cui, Z.; Wong, J.; Wong, S.; Jollimore, J.; Raymond, H.F.; Hottes, T.S.; Roth, E.A.; et al. Estimating the size of the MSM population in Metro Vancouver, Canada, using multiple methods and diverse data sources. J. Urban Health 2018, 95, 188–195. [Google Scholar] [CrossRef]
- Nash, C.J.; Gorman-Murray, A. Recovering the Gay Village: A Comparative Historical Geography of Urban Change and Planning in Toronto and Sydney. Hist. Geogr. 2015, 43, 239–260. [Google Scholar]
- Caron, M.; Bédard, L.; Latreille, J.; Buckeridge, D.L. An exploratory analysis of individuals with multiple episodes of different reportable diseases, Montreal, 1990–2012. Public Health 2016, 131, 49–55. [Google Scholar] [CrossRef]
- Sajan, A.; Corneil, T.; Grzybowski, S. The street value of prescription drugs. Can. Med. Assoc. 1998, 159, 139–142. [Google Scholar]
- Boscoe, F.P.; Johnson, C.J.; Sherman, R.L.; Stinchcomb, D.G.; Lin, G.; Henry, K.A. The relationship between area poverty rate and site-specific cancer incidence in the United States. Cancer 2014, 120, 2191–2198. [Google Scholar] [CrossRef]
- Hsieh, M.-C.; Wu, X.-C.; Andrews, P.A.; Chen, V.W. Racial and ethnic disparities in the incidence and trends of soft tissue sarcoma among adolescents and young adults in the United States, 1995–2008. J. Adolesc. Young Adult Oncol. 2013, 2, 89–94. [Google Scholar] [CrossRef]
- Atkinson, S.K.; Marlatt, V.L.; Kimpe, L.E.; Lean, D.R.S.; Trudeau, V.L.; Blais, J.M. The occurrence of steroidal estrogens in south-eastern Ontario wastewater treatment plants. Sci. Total Environ. 2012, 430, 119–125. [Google Scholar] [CrossRef]
- Charlier, C.; Foidart, J.-M.; Pitance, F.; Herman, P.; Gaspard, U.; Meurisse, M.; Plomteux, G. Environmental dichlorodiphenyltrichlorethane or hexachlorobenzene exposure and breast cancer: Is there a risk? Clin. Chem. Lab. Med. (CCLM) 2004, 42, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Russo, J.; Fernandez, S.V.; Russo, P.A.; Fernbaugh, R.; Sheriff, F.S.; Lareef, H.M.; Garber, J.; Russo, I.H. 17-Beta-estradiol induces transformation and tumorigenesis in human breast epithelial cells. FASEB J. 2006, 20, 1622–1634. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Yan, Y.; Wen, H.; Jiang, X.; Cao, X.; Zhang, G.; Liu, G. A novel estrogen receptor GPER mediates proliferation induced by 17β-estradiol and selective GPER agonist G-1 in estrogen receptor α (ERα)-negative ovarian cancer cells. Cell Biol. Int. 2014, 38, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Gillis, P.L.; Gagné, F.; McInnis, R.; Hooey, T.M.; Choy, E.S.; André, C.; Hoque, E.; Metcalfe, C.D. The impact of municipal wastewater effluent on field-deployed freshwater mussels in the Grand River (Ontario, Canada). Environ. Toxicol. Chem. 2014, 33, 134–143. [Google Scholar] [CrossRef]
- Palace, V.P.; Evans, R.E.; Wautier, K.; Baron, C.L.; Werner, J.; Klaverkamp, J.F.; Kidd, K.A.; Dick, T.A. Altered distribution of lipid-soluble antioxidant vitamins in juvenile sturgeon exposed to waterborne ethynylestradiol. Environ. Toxicol. Chem. 2001, 20, 2370–2376. [Google Scholar] [CrossRef]
- Statistics Canada. Census Year 2006. 2008. Available online: https://www12.statcan.gc.ca/census-recensement/index-eng.cfm (accessed on 1 May 2022).
- Stacchiotti, S.; Frezza, A.M.; Blay, J.; Baldini, E.H.; Bonvalot, S.; Bovée, J.V.M.G.; Callegaro, D.; Casali, P.G.; Chiang, R.C.; Demetri, G.D.; et al. Ultra-rare sarcomas: A consensus paper from the Connective Tissue Oncology Society community of experts on the incidence threshold and the list of entities. Cancer 2021, 127, 2934–2942. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subtype | Incidence | 95% CI |
|---|---|---|
| Muscle Sarcoma * | 10.43 | 10.17–10.69 |
| Fibrous Sarcoma | 6.63 | 6.42–6.84 |
| Liposarcoma | 6.27 | 6.07–6.48 |
| Sarcoma, NOS | 4.30 | 4.13–4.47 |
| Kaposi Sarcoma | 3.94 | 3.79–4.11 |
| Chondrosarcoma | 3.13 | 2.99–3.28 |
| Osteosarcoma | 2.97 | 2.83–3.11 |
| Vascular Sarcoma | 1.93 | 1.82–2.05 |
| Ewing’s Sarcoma | 1.63 | 1.54–1.74 |
| Synovial Sarcoma | 0.92 | 0.85–1.00 |
| Notochordal Sarcoma | 0.86 | 0.79–0.94 |
| Unknown Sarcoma | 0.80 | 0.73–0.87 |
| Dermatological Sarcoma | 0.47 | 0.41–0.52 |
| Sarcoma Subtype | Total No. a | % of Total Sarcomas b | % Male | % Female | Mean Age at Diagnosis ± SD, Years c |
|---|---|---|---|---|---|
| Muscle Sarcoma | 6165 | 24 | 41 | 59 | 53.9 ± 22.1 |
| Fibrous Sarcoma | 3910 | 15 | 59 | 41 | 62.8 ± 19.3 |
| Liposarcoma | 3705 | 14 | 58 | 42 | 58.3 ± 16.4 |
| Sarcoma, NOS | 2560 | 10 | 48 | 52 | 61.4 ± 19.3 |
| Kaposi Sarcoma | 2330 | 9 | 92 | 8 | 46.0 ± 15.6 |
| Chondrosarcoma | 1860 | 7 | 58 | 42 | 52.4 ± 18.4 |
| Osteosarcoma | 1435 | 6 | 53 | 47 | 37.2 ± 25.4 |
| Vascular Sarcoma | 1145 | 4 | 49 | 51 | 61.8 ± 18.4 |
| Ewing’s Sarcoma | 965 | 4 | 58 | 42 | 22.0 ± 14.8 |
| Synovial Sarcoma | 550 | 2 | 53 | 47 | 43.2 ± 20.5 |
| Notochordal Sarcoma | 520 | 2 | 57 | 43 | 55.6 ± 20.5 |
| Unknown Sarcoma | 480 | 2 | 49 | 51 | 38.1 ± 20.7 |
| Dermatological Sarcoma | 270 | 1 | 53 | 47 | 46.0 ± 22.6 |
| Total No. a | <40 y a | 40–59 y a | ≥60 y a | Mean age at diagnosis ± SD, years | |
| Total Sarcomas | 25,895 | 6480 | 7915 | 11,240 | 53.6 ± 21.7 |
| Age Group (Years) | Total Sarcoma Cases a | Most Common Type of Sarcoma |
|---|---|---|
| 0–9 | 845 | Muscle Sarcoma |
| 10–19 | 1520 | Osteosarcoma |
| 20–29 | 1365 | Ewing’s Sarcoma |
| 30–39 | 2750 | Kaposi Sarcoma |
| 40–49 | 3840 | Muscle Sarcoma |
| 50–59 | 4075 | Muscle Sarcoma |
| 60–69 | 4170 | Muscle Sarcoma |
| 70–79 | 4290 | Muscle Sarcoma |
| 80–89 | 2450 | Fibrous Sarcoma |
| 90–99 | 330 | Fibrous Sarcoma |
| ICD Code | Study Code | Sarcoma Mortality |
|---|---|---|
| C40 | C40 peripheral | Bone, joints, and articular cartilages of limbs located peripherally |
| C41 | C41 axial | Bones, joints, and articular cartilages of other and unspecified sites located axially |
| C40–41 | C40_41 | Bones, joints, and articular cartilages of all locations combined |
| C49 | C49 peripheral | Connective, subcutaneous, and other soft tissues located peripherally |
| C49 | C49 axial | Connective, subcutaneous, and other soft tissues located axially |
| C49 | C49 | Connective, subcutaneous, and other soft tissues of all locations combined |
| Sarcoma | Mortality Rate |
|---|---|
| Axial Bone Sarcoma Peripheral Bone Sarcoma | 1.35 (95% CI 1.25–1.44) 0.52 (95% CI 0.47–0.59) |
| Axial Soft Tissue Sarcoma Peripheral Soft Tissue Sarcoma | 2.06 (95% CI 1.94–2.18) 1.21 (95% CI 1.12–1.30) |
| Quintile 1 | Quintile 2 | Quintile 3 | Quintile 4 | Quintile 5 | |
|---|---|---|---|---|---|
| Annual income | <CAD 20,000 | CAD 20,000–25,000 | CAD 25,000–30,000 | CAD 30,000–35,000 | >CAD 35,000 |
| Cases a | 620 | 360 | 215 | 40 | 0 |
| Incidence rate per million | 3.40 | 1.67 | 1.64 | 0.89 | 0.00 |
| Incidence rate ratio compared to Q1 (95% CI) | - | 0.49 (0.43–0.56) | 0.48 (0.41–0.56) | 0.26 (0.19–0.36) | - |
| Quintile 1 | Quintile 2 | Quintile 3 | Quintile 4 | Quintile 5 | |
|---|---|---|---|---|---|
| Percentage of African Canadian individuals | <5.00% | 5.00–9.99% | 10.00–14.99% | 15.00–19.99% | >20.00% |
| Cases a | 1045 | 95 | 35 | 30 | 20 |
| Incidence rate per million | 2.13 | 2.00 | 1.77 | 4.55 | 3.75 |
| Incidence rate ratio compared to Q1 (95% CI) | - | 0.94 (0.76–1.16) | 0.83 (0.59–1.16) | 2.14 (1.49–3.07) | 1.76 (1.13–2.74) |
| Quintile 1 | Quintile 2 | Quintile 3 | Quintile 4 | Quintile 5 | |
|---|---|---|---|---|---|
| Percentage of Hispanic individuals | <1.00% | 1.00–1.99% | 2.00–2.99% | 3.00–3.99% | >4.00% |
| Cases a | 220 | 480 | 310 | 155 | 60 |
| Incidence rate per million | 0.54 | 4.70 | 9.48 | 14.67 | 3.80 |
| Incidence rate ratio compared to Q1 (95% CI) | - | 8.74 (7.45–10.25) | 17.61 (14.81–20.93) | 27.25 (22.19–33.47) | 7.06 (5.31–9.39) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alkazemi, B.; Ghazawi, F.M.; Lagacé, F.; Nechaev, V.; Zubarev, A.; Litvinov, I.V. Investigation of the Incidence and Geographic Distribution of Bone and Soft Tissue Sarcomas in Canada: A National Population-Based Study. Curr. Oncol. 2023, 30, 5631-5651. https://doi.org/10.3390/curroncol30060424
Alkazemi B, Ghazawi FM, Lagacé F, Nechaev V, Zubarev A, Litvinov IV. Investigation of the Incidence and Geographic Distribution of Bone and Soft Tissue Sarcomas in Canada: A National Population-Based Study. Current Oncology. 2023; 30(6):5631-5651. https://doi.org/10.3390/curroncol30060424
Chicago/Turabian StyleAlkazemi, Badria, Feras M. Ghazawi, François Lagacé, Vladimir Nechaev, Andrei Zubarev, and Ivan V. Litvinov. 2023. "Investigation of the Incidence and Geographic Distribution of Bone and Soft Tissue Sarcomas in Canada: A National Population-Based Study" Current Oncology 30, no. 6: 5631-5651. https://doi.org/10.3390/curroncol30060424
APA StyleAlkazemi, B., Ghazawi, F. M., Lagacé, F., Nechaev, V., Zubarev, A., & Litvinov, I. V. (2023). Investigation of the Incidence and Geographic Distribution of Bone and Soft Tissue Sarcomas in Canada: A National Population-Based Study. Current Oncology, 30(6), 5631-5651. https://doi.org/10.3390/curroncol30060424