The Effects of Second Primary Malignancies and Frailty on Overall Survival and Mortality in Geriatric Turkish Patients with Multiple Myeloma


Abstract
1. Introduction
2. Materials and Methods
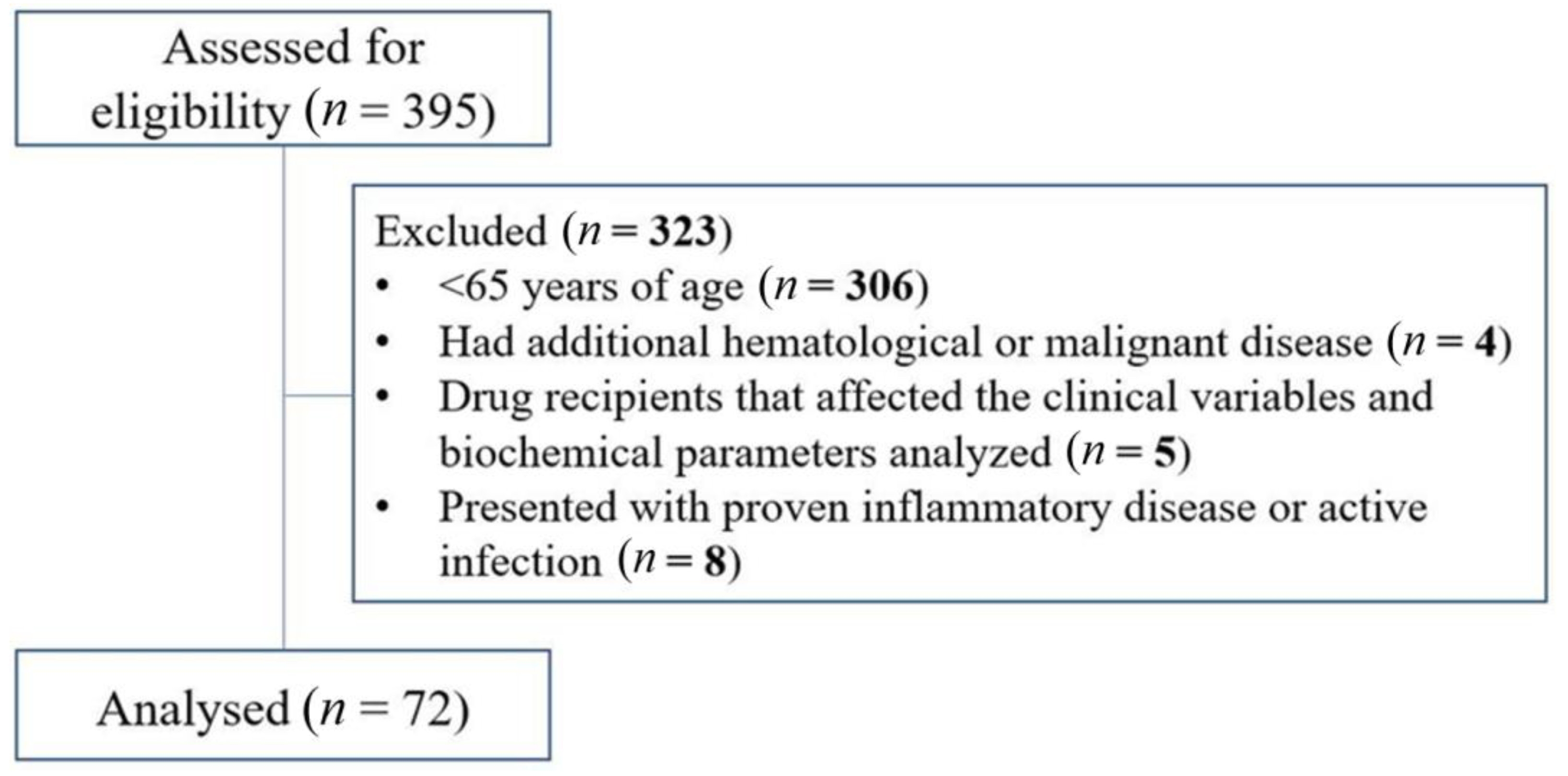
2.1. Study Design
2.2. Data Collection
2.3. Patient Management and Survival-Related Definitions
2.4. Laboratory and Genetic Analyses
2.5. Statistical Analysis
3. Results
3.1. Descriptive & Inferential Analysis
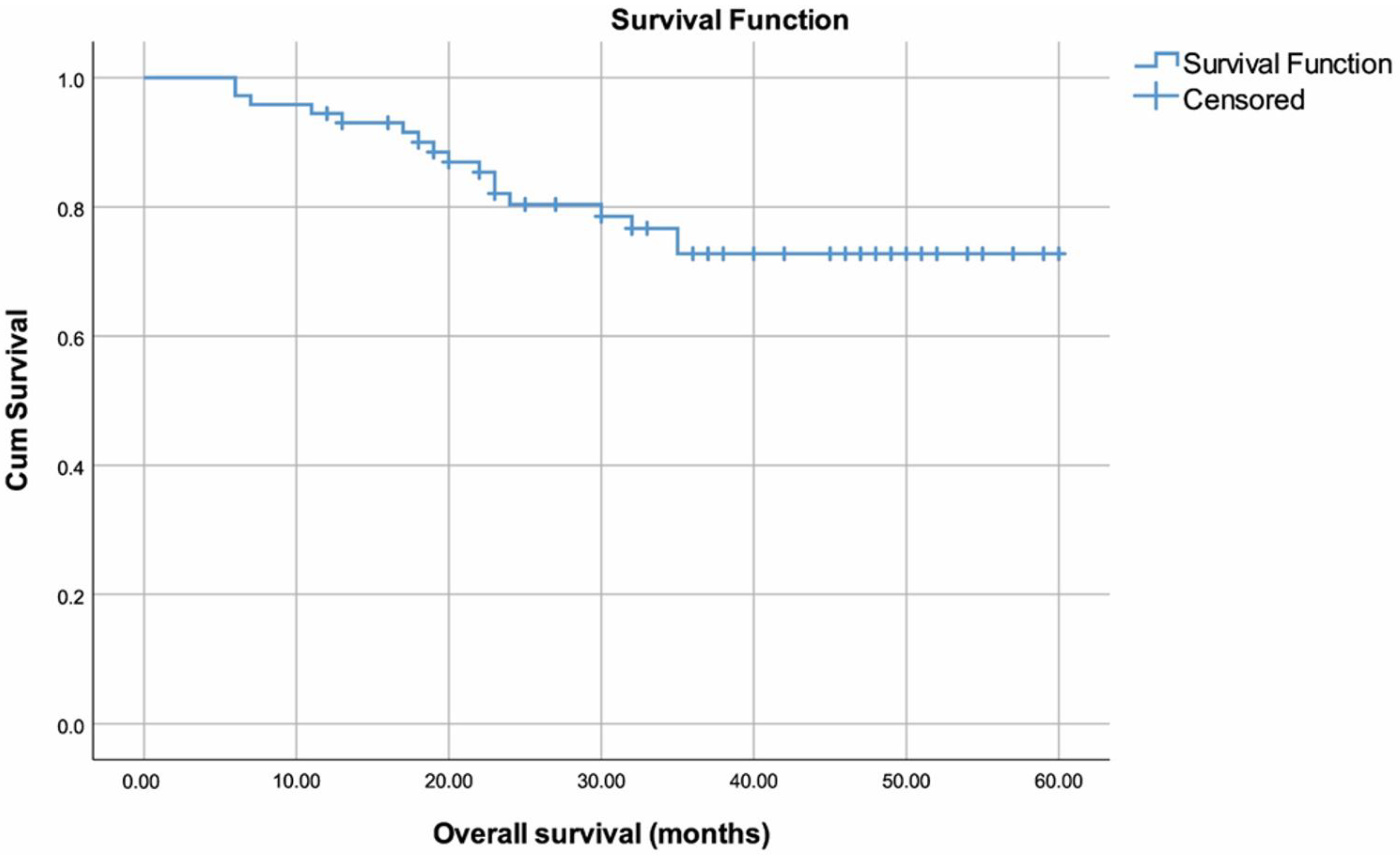
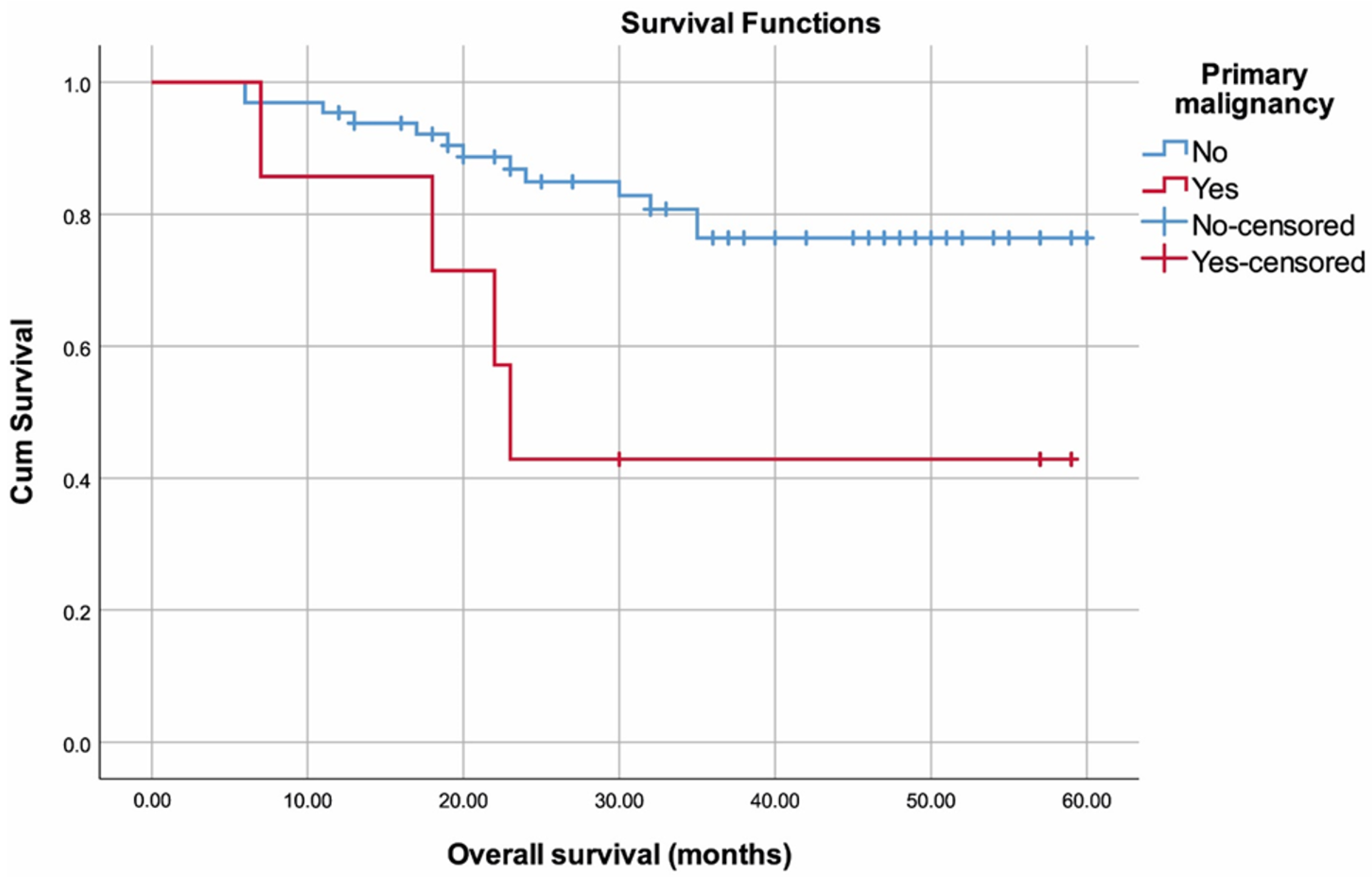
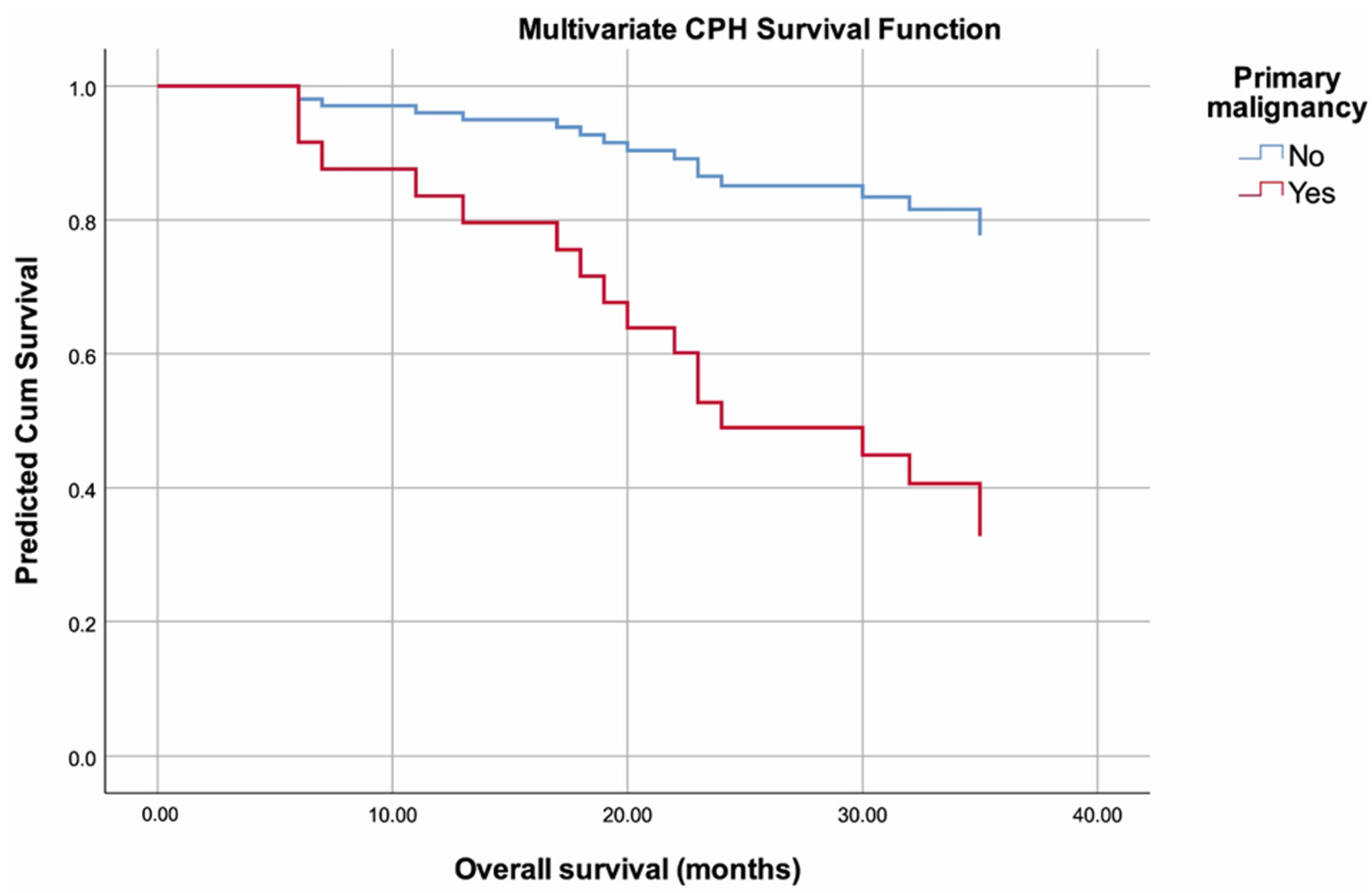
3.2. Survival Analysis
4. Discussion
4.1. Summary and Contributions
4.2. Strengths and Limitations
4.3. Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Padala, S.A.; Barsouk, A.; Barsouk, A.; Rawla, P.; Vakiti, A.; Kolhe, R.; Kota, V.; Ajebo, G.H. Epidemiology, staging, and management of multiple myeloma. Med. Sci. 2021, 9, 3. [Google Scholar] [CrossRef]
- Huang, J.; Chan, S.C.; Lok, V.; Zhang, L.; Lucero-Prisno, D.E.; Xu, W.; Zheng, Z.-J.; Elcarte, E.; Withers, M.; Wong, M.C. The epidemiological landscape of multiple myeloma: A global cancer registry estimate of disease burden, risk factors, and temporal trends. Lancet Haematol. 2022, 9, e670–e677. [Google Scholar] [CrossRef] [PubMed]
- Poh, C.; Keegan, T.; Rosenberg, A.S. Second primary malignancies in multiple myeloma: A review. Blood Rev. 2021, 46, 100757. [Google Scholar] [CrossRef]
- Chakraborty, R.; Majhail, N.S. Treatment and disease-related complications in multiple myeloma: Implications for survivorship. Am. J. Hematol. 2020, 95, 672–690. [Google Scholar] [CrossRef]
- Möller, M.-D.; Gengenbach, L.; Graziani, G.; Greil, C.; Wäsch, R.; Engelhardt, M. Geriatric assessments and frailty scores in multiple myeloma patients: A needed tool for individualized treatment? Curr. Opin. Oncol. 2021, 33, 648–657. [Google Scholar] [CrossRef] [PubMed]
- Engelhardt, M.; Ihorst, G.; Duque-Afonso, J.; Wedding, U.; Spät-Schwalbe, E.; Goede, V.; Kolb, G.; Stauder, R.; Wäsch, R. Structured assessment of frailty in multiple myeloma as a paradigm of individualized treatment algorithms in cancer patients at advanced age. Haematologica 2020, 105, 1183–1188. [Google Scholar] [CrossRef]
- Turgutkaya, A.; Yavaşoğlu, İ.; Şahin, T.; Sargın, G.; Bolaman, A.Z. Multiple myeloma and frequency of synchronous and second primary malignancies. J. Hematop. 2021, 14, 197–203. [Google Scholar] [CrossRef]
- Maclachlan, K.; Diamond, B.; Maura, F.; Hillengass, J.; Turesson, I.; Landgren, C.O.; Kazandjian, D. Second malignancies in multiple myeloma; emerging patterns and future directions. Best Pract. Res. Clin. Haematol. 2020, 33, 101144. [Google Scholar] [CrossRef]
- Rajkumar, S.V.; Dimopoulos, M.A.; Palumbo, A.; Blade, J.; Merlini, G.; Mateos, M.-V.; Kumar, S.; Hillengass, J.; Kastritis, E.; Richardson, P. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014, 15, e538–e548. [Google Scholar] [CrossRef]
- Palumbo, A.; Avet-Loiseau, H.; Oliva, S.; Lokhorst, H.M.; Goldschmidt, H.; Rosinol, L.; Richardson, P.; Caltagirone, S.; Lahuerta, J.J.; Facon, T. Revised international staging system for multiple myeloma: A report from International Myeloma Working Group. J. Clin. Oncol. 2015, 33, 2863–2869. [Google Scholar] [CrossRef]
- Palumbo, A.; Bringhen, S.; Mateos, M.-V.; Larocca, A.; Facon, T.; Kumar, S.K.; Offidani, M.; Mccarthy, P.; Evangelista, A.; Lonial, S. Geriatric assessment predicts survival and toxicities in elderly myeloma patients: An International Myeloma Working Group report. Blood 2015, 125, 2068–2074. [Google Scholar] [CrossRef]
- Kumar, S.; Paiva, B.; Anderson, K.C.; Durie, B.; Landgren, O.; Moreau, P.; Munshi, N.; Lonial, S.; Bladé, J.; Mateos, M.-V. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 2016, 17, e328–e346. [Google Scholar] [CrossRef] [PubMed]
- Larocca, A.; Palumbo, A. Optimizing treatment for elderly patients with newly diagnosed multiple myeloma: A personalized approach. J. Clin. Oncol. 2016, 34, 3600–3604. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, P.S.; Barker, K.A.; Anderson, W.F. Future distribution of multiple myeloma in the United States by sex, age, and race/ethnicity. Blood 2015, 125, 410–412. [Google Scholar] [CrossRef] [PubMed]
- Patel, B.G.; Luo, S.; Wildes, T.M.; Sanfilippo, K.M. Frailty in older adults with multiple myeloma: A study of US veterans. JCO Clin. Cancer Inform. 2020, 4, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Abel, G.A.; Klepin, H.D. Frailty and the management of hematologic malignancies. Blood 2018, 131, 515–524. [Google Scholar] [CrossRef]
- Cook, G.; Larocca, A.; Facon, T.; Zweegman, S.; Engelhardt, M. Defining the vulnerable patient with myeloma—A frailty position paper of the European Myeloma Network. Leukemia 2020, 34, 2285–2294. [Google Scholar] [CrossRef]
- Mian, H.; Mccurdy, A.; Giri, S.; Grant, S.; Rochwerg, B.; Winks, E.; Rosko, A.E.; Engelhardt, M.; Pawlyn, C.; Cook, G. The prevalence and outcomes of frail older adults in clinical trials in multiple myeloma: A systematic review. Blood Cancer J. 2023, 13, 6. [Google Scholar] [CrossRef]
- Mina, R.; Larocca, A.; Offidani, M.; Innao, V.; Cellini, C.; Galli, M.; Cetani, G.; Grasso, M.; Ciccone, G.; Capra, A. Efficacy and safety of ixazomib induction and maintenance in newly diagnosed multiple myeloma patients according to the IMWG frailty score: A post-hoc analysis of the EMN10-Unito trial. Blood 2020, 136, 44–45. [Google Scholar] [CrossRef]
- Stege, C.A.; Nasserinejad, K.; Van Der Spek, E.; Bilgin, Y.M.; Kentos, A.; Sohne, M.; Van Kampen, R.J.; Ludwig, I.; Thielen, N.; Durdu-Rayman, N. Ixazomib, daratumumab, and low-dose dexamethasone in frail patients with newly diagnosed multiple myeloma: The Hovon 143 study. J. Clin. Oncol. 2021, 39, 2758–2767. [Google Scholar] [CrossRef]
- Stege, C.A.; Nasserinejad, K.; Levin, M.-D.; Klein, S.K.; De Waal, E.; Eeltink, C.; Korst, C.L.; Ypma, P.F.; Dijk, A.C.; Westerman, M. Geriatric impairments and low muscle mass are associated with treatment discontinuation and overall survival in newly diagnosed non-transplant eligible multiple myeloma patients (nte-NDMM) treated with dose-adjusted melphalan-prednisone-bortezomib (MPV)—Results of the Dutch HOVON 123 study. Blood 2018, 132, 1889. [Google Scholar]
- Auner, H.W.; Brown, S.R.; Walker, K.; Kendall, J.; Dawkins, B.; Meads, D.; Morgan, G.J.; Kaiser, M.F.; Cook, M.; Roberts, S. Ixazomib with cyclophosphamide and dexamethasone in relapsed or refractory myeloma: MUKeight phase II randomised controlled trial results. Blood Cancer J. 2022, 12, 52. [Google Scholar] [CrossRef]
- Landgren, O.; Mailankody, S. Update on second primary malignancies in multiple myeloma: A focused review. Leukemia 2014, 28, 1423–1426. [Google Scholar] [CrossRef] [PubMed]
- Ailawadhi, S.; Swaika, A.; Razavi, P.; Yang, D.; Chanan-Khan, A. Variable risk of second primary malignancy in multiple myeloma patients of different ethnic subgroups. Blood Cancer J. 2014, 4, e243. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, A.; Bringhen, S.; Kumar, S.K.; Lupparelli, G.; Usmani, S.; Waage, A.; Larocca, A.; Van Der Holt, B.; Musto, P.; Offidani, M. Second primary malignancies with lenalidomide therapy for newly diagnosed myeloma: A meta-analysis of individual patient data. Lancet Oncol. 2014, 15, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Mccarthy, P.L.; Holstein, S.A.; Petrucci, M.T.; Richardson, P.G.; Hulin, C.; Tosi, P.; Bringhen, S.; Musto, P.; Anderson, K.C.; Caillot, D. Lenalidomide maintenance after autologous stem-cell transplantation in newly diagnosed multiple myeloma: A meta-analysis. J. Clin. Oncol. 2017, 35, 3279–3289. [Google Scholar] [CrossRef]
- Jonsdottir, G.; Lund, S.H.; Björkholm, M.; Turesson, I.; Wahlin, A.; Mailankody, S.; Blimark, C.; Hultcrantz, M.; Porwit, A.; Landgren, O. Survival in multiple myeloma patients who develop second malignancies: A population-based cohort study. Haematologica 2016, 101, e145–e148. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Lv, C.; Zhou, M.; Xu, J.-Y.; Chen, B.; Wan, Y. Second Primary Malignancy Risk in Multiple Myeloma from 1975 to 2018. Cancers 2022, 14, 4919. [Google Scholar] [CrossRef]
- Lu, T.-X.; Wu, S.; Cai, D.-Y.; Hong, T.-T.; Zhang, Y.; Gao, H.-Q.; Hua, H.-Y.; Wu, X.-H. Prognostic significance of serum aspartic transaminase in diffuse large B-cell lymphoma. BMC Cancer 2019, 19, 553. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Apekey, T.A.; Van Hemelrijck, M.; Calori, G.; Perseghin, G. Gamma glutamyltransferase, alanine aminotransferase and risk of cancer: Systematic review and meta-analysis. Int. J. Cancer 2015, 136, 1162–1170. [Google Scholar] [CrossRef]
- Kobayashi, D.; Yamamoto, K.; Kimura, T.; Shimbo, T. Aspartate aminotransferase/alanine aminotransferase ratio and subsequent cancer development. Cancer Med. 2022, 11, 798–814. [Google Scholar] [CrossRef] [PubMed]
- Kyle, R.A. Multiple myeloma: Review of 869 cases. Mayo Clin. Proc. 1975, 50, 29–40. [Google Scholar]
- Poudel, B.; Mittal, A.; Shrestha, R.; Farooqui, M.S.; Yadav, N.K.; Shukla, P.S. Liver involvement in multiple myeloma: A hospital based retrospective study. Asian Pac. J. Cancer Prev. 2012, 13, 2153–2155. [Google Scholar] [CrossRef] [PubMed]
- Walz-Mattmüller, R.; Horny, H.-P.; Ruck, P.; Kaiserling, E. Incidence and pattern of liver involvement in haematological malignancies. Asian Pac. J. Cancer Prev. 1998, 194, 781–789. [Google Scholar] [CrossRef]
- Kiba, T.; Ito, T.; Nakashima, T.; Okikawa, Y.; Kido, M.; Kimura, A.; Kameda, K.; Miyamae, F.; Tanaka, S.; Atsumi, M. Bortezomib and dexamethasone for multiple myeloma: Higher AST and LDH levels associated with a worse prognosis on overall survival. BMC Cancer 2014, 14, 462. [Google Scholar] [CrossRef]
- Wang, F.; Gao, S.; Wu, M.; Zhao, D.; Sun, H.; Yav, S.; Chen, Y.; Zhang, Z.; Yang, M.; Dong, Y. The prognostic role of the AST/ALT ratio in hepatocellular carcinoma patients receiving thermal ablation combined with simultaneous TACE. BMC Gastroenterol. 2023, 23, 80. [Google Scholar] [CrossRef]
- Wu, J.; Chen, L.; Wang, Y.; Tan, W.; Huang, Z. Prognostic value of aspartate transaminase to alanine transaminase (De Ritis) ratio in solid tumors: A pooled analysis of 9400 patients. OncoTargets Ther. 2019, 12, 5201–5213. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Results |
|---|---|
| Age, years, (n = 72) | 68 (66–72) |
| Sex, (n = 72) | |
| Male | 45 (62.5%) |
| Female | 27 (37.5%) |
| Body mass index, kg/m2, (n = 72) | 25.40 ± 3.49 |
| Type of MM, (n = 72) | |
| IgG kappa, (n, %) | 27 (37.5%) |
| IgG lambda, (n, %) | 13 (18.1%) |
| IgA kappa, (n, %) | 17 (23.6%) |
| IgA lambda, (n, %) | 8 (11.1%) |
| Kappa light chain, (n, %) | 3 (4.2%) |
| Lambda light chain, (n, %) | 4 (5.6%) |
| R-ISS, (n = 72) | |
| Stage II, (n, %) | 19 (26.4%) |
| Stage III, (n, %) | 53 (73.6%) |
| Co-morbidities | |
| Chronic renal failure, (n, %) | 17 (23.6%) |
| Congestive heart failure, (n, %) | 13 (18.1%) |
| Hypertension, (n, %) | 44 (61.1%) |
| Thyroid conditions, (n, %) | 10 (13.9%) |
| Diabetes mellitus, (n, %) | 26 (36.1%) |
| Neuropathy, (n, %) | 3 (4.2%) |
| Deep vein thrombosis, (n, %) | 3 (4.2%) |
| Second Primary malignancy, (n, %) | 7 (9.7%) |
| Renal involvement, (n, %) | 21 (29.2%) |
| Bone involvement by FDG-PET, (n, %) | 54 (75.0%) |
| Plasmacytoma, (n,%) | 19 (26.4%) |
| The presence of frailty, (n, %) | 53 (73.6%) |
| The presence of hypercalcemia, (n, %) | 8 (11.1%) |
| The presence of anemia, (n, %) | 63 (87.5%) |
| Follow-up time, months, (n = 72) | 36.5 (22.0–48.5) |
| Final status | |
| Alive, (n, %) | 55 (76.4%) |
| Exitus, (n, %) | 17 (23.6%) |
| Variables | n (%) |
|---|---|
| Induction Therapy | |
| VCD, (n, %) | 72 (100.0%) |
| Number of course, Induction therapy | |
| 4, (n, %) | 64 (88.9%) |
| 6, (n, %) | 8 (11.1%) |
| Response to induction therapy, (n = 72) | |
| Complete response, (n, %) | 9 (12.5%) |
| Very good partial response, (n, %) | 35 (48.6%) |
| Partial response, (n, %) | 19 (26.4%) |
| Stable disease, (n, %) | 9 (12.5%) |
| Progressive disease, (n, %) | 0 (0.0%) |
| Autologous stem cell transplant, (n, %) | 41 (56.9%) |
| Response of prior to ASCT, (n = 41) | |
| Complete response | 5 (12.2%) |
| Very good partial response | 25 (61.0%) |
| Partial response | 11 (26.8%) |
| Response to ASCT, After 100 days, (n = 41) | |
| Complete response, (n, %) | 25 (61.0%) |
| Very good partial response, (n, %) | 15 (36.6%) |
| Partial response, (n, %) | 1 (2.4%) |
| Maintenance treatment after ASCT, (n = 72) | |
| None, (n, %) | 12 (16.7%) |
| Lenalidomide, (n, %) | 60 (83.3%) |
| Consolidation Therapy, (n = 72) | |
| LEN/DEX, (n, %) | 18 (25.0%) |
| KRD, (n, %) | 8 (11.1%) |
| VRD, (n, %) | 9 (12.5%) |
| KD, (n, %) | 13 (18.1%) |
| POM/DEX, (n, %) | 16 (22.2%) |
| VEL/DEXA, (n, %) | 8 (11.1%) |
| Number of course, Consolidation Therapy, (n = 72) | 8 (6–12) |
| Response to Consolidation Therapy, (n = 72) | |
| Complete response, (n, %) | 16 (22.2%) |
| Very good partial response, (n, %) | 14 (19.4%) |
| Partial response, (n, %) | 21 (29.2%) |
| Stable disease, (n, %) | 12 (16.7%) |
| Progressive disease, (n, %) | 9 (12.5%) |
| Requiring Radiotherapy, (n, %) | 17 (23.6%) |
| Requiring Zoledronic acid use, (n, %) | 52 (72.2%) |
| Requiring Denosumab use, (n, %) | 15 (20.8%) |
| Variables | Results |
|---|---|
| IgG, g/L | 17.51 (6.97–28.81) |
| IgA, g/L | 2.21 (0.54–9.33) |
| IgM, g/L | 0.36 (0.23–0.49) |
| sFLC Kappa, mg/L | 153 (55–296) |
| sFLC Lambda, mg/L | 38.0 (22.5–163.5) |
| sFLC Kappa to Lambda ratio | 4.75 (0.72–8.09) |
| M-Spike, g/dL | 2.39 ± 1.13 |
| Beta-2 microglobulin, mg/L | 3.25 (2.57–4.95) |
| High plasma cells in bone marrow (≥60%), (n,%) | 18 (25.0%) |
| High serum free light chain ratio (≥100), (n,%) | 26 (36.1%) |
| Total Protein, g/dL | 8.88 ± 1.78 |
| Albumin, g/dL | 3.41 ± 0.71 |
| Creatinine, mg/dL | 1.34 (0.93–2.40) |
| eGFR, mL/min/1.73 m2 | 52 (28–77.5) |
| Calcium, mg/dL | 9.67 ± 0.93 |
| Urea, mg/dL | 42 (32–70) |
| LDH, IU/L | 172.79 ± 45.81 |
| High LDH (>248), (n,%) | 4 (5.6%) |
| ALT, IU/L | 14 (10–24.5) |
| AST, IU/L | 19 (15–24) |
| GGT, IU/L | 31 (19–58) |
| Urinary Protein, mg | 225 (153–1064) |
| Proteinuria (n,%) | 33 (46.5%) |
| Cytogenetic results | |
| del17p, (n,%) | 10 (13.9%) |
| t(4;14), (n,%) | 7 (9.7%) |
| t(14;16), (n,%) | 2 (2.8%) |
| Other, (n,%) | 24 (33.3%) |
| High genetic risk, (n,%) | 19 (26.4%) |
| n | Exitus | Mean (95% CI) | p | |
|---|---|---|---|---|
| Overall survival | 72 | 17 | 49.40 (45.01–53.80) | N/A |
| Second Primary malignancy | ||||
| No | 65 | 13 | 51.05 (46.70–55.40) | 0.018 |
| Yes | 7 | 4 | 35.29 (19.66–50.91) | |
| Frailty | ||||
| No | 19 | 4 | 49.73 (40.92–58.53) | 0.908 |
| Yes | 53 | 13 | 48.49 (43.51–53.48) | |
| Sex | ||||
| Male | 45 | 8 | 52.07 (47.14–57.00) | 0.163 |
| Female | 27 | 9 | 44.63 (36.78–52.47) | |
| Type of heavy protein chain | ||||
| IgG | 40 | 8 | 50.26 (44.28–56.23) | 0.959 |
| IgA | 25 | 6 | 50.05 (43.65–56.44) | |
| Type of light protein chain | ||||
| Kappa | 47 | 12 | 48.16 (42.42–53.90) | 0.473 |
| Lambda | 25 | 5 | 51.03 (44.67–57.39) | |
| Chronic renal failure | ||||
| No | 55 | 13 | 49.48 (44.50–54.47) | 0.975 |
| Yes | 17 | 4 | 48.64 (39.71–57.57) | |
| Congestive heart failure | ||||
| No | 59 | 14 | 49.67 (44.93–54.40) | 0.847 |
| Yes | 13 | 3 | 48.21 (37.50–58.92) | |
| Hypertension | ||||
| No | 28 | 4 | 53.40 (47.51–59.28) | 0.169 |
| Yes | 44 | 13 | 46.19 (40.28–52.09) | |
| Thyroid conditions | ||||
| No | 62 | 17 | 47.71 (42.75–52.67) | 0.073 |
| Yes | 10 | 0 | (1) | |
| Diabetes mellitus | ||||
| No | 46 | 8 | 52.65 (48.05–57.26) | 0.070 |
| Yes | 26 | 9 | 43.16 (34.76–51.55) | |
| Neuropathy | ||||
| No | 69 | 17 | 48.92 (44.36–53.48) | 0.344 |
| Yes | 3 | 0 | (1) | |
| Deep vein thrombosis | ||||
| No | 69 | 16 | 49.65 (45.20–54.11) | 0.534 |
| Yes | 3 | 1 | 24.00 (22.61–25.39) | |
| Hypercalcemia | ||||
| No | 64 | 16 | 48.64 (43.83–53.44) | 0.373 |
| Yes | 8 | 1 | 49.57 (41.54–57.61) | |
| Renal involvement | ||||
| No | 51 | 13 | 47.90 (42.26–53.54) | 0.361 |
| Yes | 21 | 4 | 52.36 (46.43–58.28) | |
| Anemia | ||||
| No | 9 | 0 | (1) | 0.090 |
| Yes | 63 | 17 | 47.87 (42.96–52.78) | |
| Bone involvement by FDG-PET | ||||
| No | 18 | 6 | 46.16 (37.37–54.95) | 0.440 |
| Yes | 54 | 11 | 50.52 (45.55–55.49) | |
| High plasma cells in bone marrow (≥60%) | ||||
| No | 54 | 14 | 47.51 (42.33–52.69) | 0.412 |
| Yes | 18 | 3 | 52.83 (45.49–60.18) | |
| High serum free light chain ratio (≥100) | ||||
| No | 46 | 13 | 47.17 (41.27–53.07) | 0.200 |
| Yes | 26 | 4 | 52.66 (46.94–58.37) | |
| Plasmacytoma | ||||
| No | 53 | 10 | 51.84 (47.28–56.40) | 0.069 |
| Yes | 19 | 7 | 39.08 (30.29–47.86) | |
| LDH | ||||
| Normal | 68 | 17 | 48.67 (44.03–53.32) | 0.241 |
| High | 4 | 0 | (1) | |
| Proteinuria | ||||
| No | 38 | 8 | 50.39 (44.49–56.28) | 0.663 |
| Yes | 33 | 9 | 47.75 (41.37–54.13) | |
| Genetic risk | ||||
| Low | 53 | 14 | 47.63 (42.15–53.12) | 0.254 |
| High | 19 | 3 | 49.00 (42.80–55.20) | |
| Frailty | ||||
| No | 19 | 4 | 49.73 (40.92–58.53) | 0.908 |
| Yes | 53 | 13 | 48.49 (43.51–53.48) | |
| Requiring Radiotherapy | ||||
| No | 55 | 13 | 49.69 (44.81–54.56) | 0.920 |
| Yes | 17 | 4 | 44.35 (35.94–52.77) | |
| Requiring Zoledronic acid use | ||||
| No | 20 | 3 | 52.72 (46.21–59.24) | 0.232 |
| Yes | 52 | 14 | 47.60 (42.08–53.11) | |
| Requiring Denosumab use | ||||
| No | 57 | 15 | 48.06 (42.89–53.23) | 0.270 |
| Yes | 15 | 2 | 53.36 (46.13–60.59) | |
| Number of course, Induction Therapy | ||||
| 4 | 64 | 17 | 47.14 (42.35–51.94) | 0.084 |
| 6 | 8 | 0 | (1) | |
| Response to Induction Therapy | ||||
| Complete response | 9 | 2 | 54.44 (47.65–61.24) | 0.334 |
| Very good partial response | 35 | 8 | 34.95 (30.67–39.23) | |
| Partial response | 19 | 3 | 49.68 (44.14–55.23) | |
| Stable disease | 9 | 4 | 34.11 (25.51–42.71) | |
| Autologous stem cell transplant | ||||
| No | 31 | 9 | 46.70 (39.95–53.44) | 0.397 |
| Yes | 41 | 8 | 50.94 (45.31–56.58) | |
| Response to ASCT, After 100 days | ||||
| No ASCT | 31 | 9 | 46.70 (39.95–53.44) | 0.672 |
| Complete response | 25 | 5 | 50.27 (42.71–57.84) | |
| VGPR & PR | 16 | 3 | 47.75 (40.36–55.15) | |
| R-ISS | ||||
| Stage II | 19 | 3 | 51.81 (44.29–59.32) | 0.382 |
| Stage III | 53 | 14 | 48.32 (43.08–53.56) | |
| Maintenance treatment after ASCT | ||||
| No | 12 | 4 | 39.32 (31.29–47.36) | 0.484 |
| Yes | 60 | 13 | 50.08 (45.32–54.84) | |
| Consolidation Therapy | ||||
| LEN/DEX | 18 | 2 | 49.85 (43.37–56.33) | 0.893 |
| KRD | 8 | 2 | 48.86 (35.78–61.93) | |
| VRD | 9 | 3 | 42.11 (30.41–53.81) | |
| KD | 13 | 3 | 48.37 (38.11–58.63) | |
| POM/DEX | 16 | 4 | 47.37 (37.40–57.34) | |
| VEL/DEXA | 8 | 3 | 37.98 (28.38–47.58) | |
| Response to Consolidation Therapy | ||||
| Complete response | 16 | 0 | (1) | 0.203 |
| Very good partial response | 14 | 3 | 48.71 (38.74–58.69) | |
| Partial response | 21 | 4 | 49.85 (41.82–57.87) | |
| Stable disease | 12 | 5 | 36.61 (27.89–45.33) | |
| Progressive disease | 9 | 5 | 32.30 (22.43–42.18) | |
| β Coefficient | Standard Error | p | HR | 95.0% CI for HR | ||
|---|---|---|---|---|---|---|
| Second Primary malignancy | 1.486 | 0.597 | 0.013 | 4.420 | 1.371 | 14.246 |
| ALT | 0.017 | 0.008 | 0.038 | 1.017 | 1.001 | 1.033 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ipek, Y.; Karademir, N.; Yilmazer, O.; Yilmaz, G. The Effects of Second Primary Malignancies and Frailty on Overall Survival and Mortality in Geriatric Turkish Patients with Multiple Myeloma. Curr. Oncol. 2023, 30, 5615-5630. https://doi.org/10.3390/curroncol30060423
Ipek Y, Karademir N, Yilmazer O, Yilmaz G. The Effects of Second Primary Malignancies and Frailty on Overall Survival and Mortality in Geriatric Turkish Patients with Multiple Myeloma. Current Oncology. 2023; 30(6):5615-5630. https://doi.org/10.3390/curroncol30060423
Chicago/Turabian StyleIpek, Yildiz, Nevra Karademir, Onur Yilmazer, and Guven Yilmaz. 2023. "The Effects of Second Primary Malignancies and Frailty on Overall Survival and Mortality in Geriatric Turkish Patients with Multiple Myeloma" Current Oncology 30, no. 6: 5615-5630. https://doi.org/10.3390/curroncol30060423
APA StyleIpek, Y., Karademir, N., Yilmazer, O., & Yilmaz, G. (2023). The Effects of Second Primary Malignancies and Frailty on Overall Survival and Mortality in Geriatric Turkish Patients with Multiple Myeloma. Current Oncology, 30(6), 5615-5630. https://doi.org/10.3390/curroncol30060423