Functional State and Rehabilitation of Patients after Primary Brain Tumor Surgery for Malignant and Nonmalignant Tumors: A Prospective Observational Study

 ,
,
Abstract
1. Introduction
2. Methods
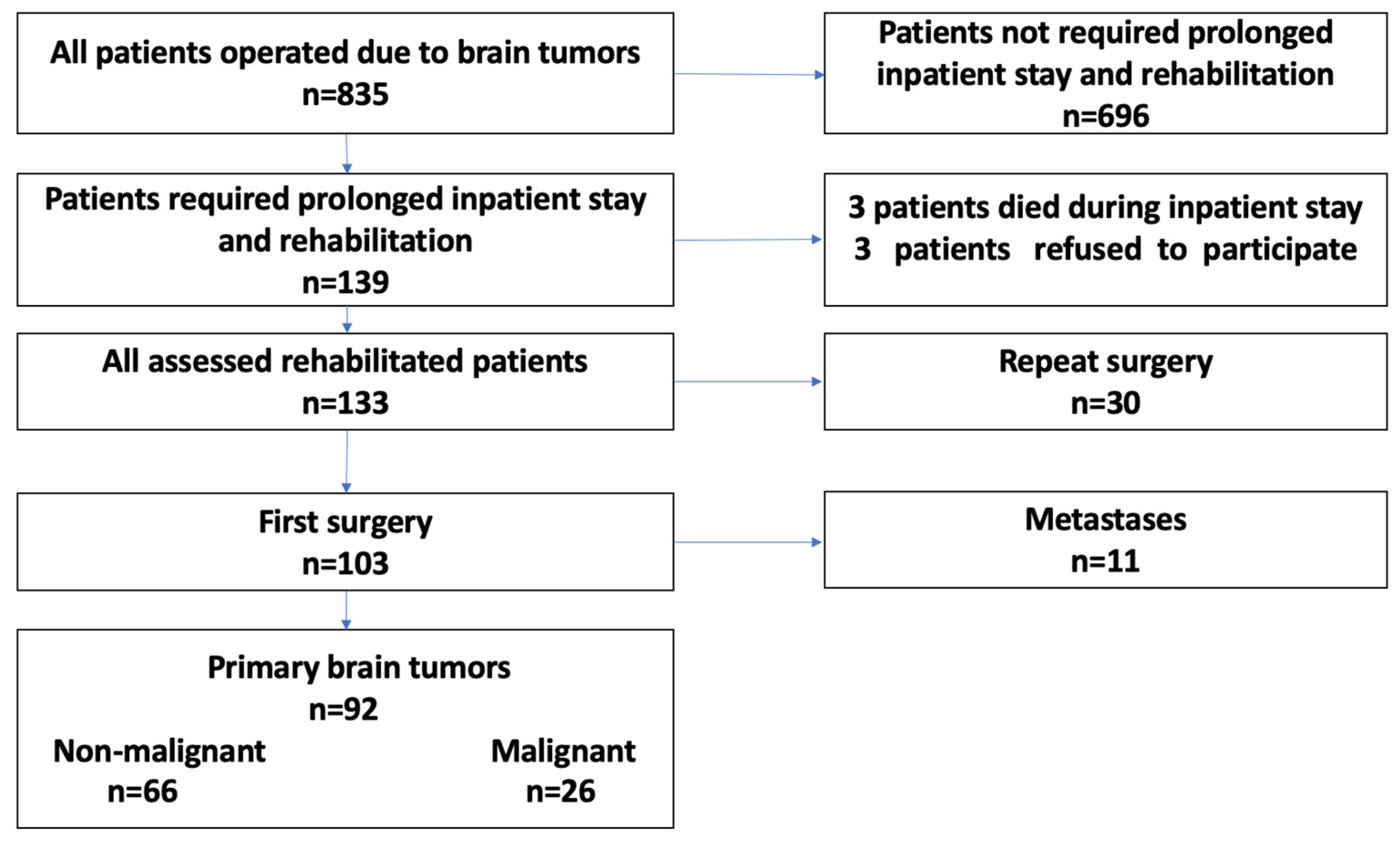
2.1. Patient Cohort
2.2. Patient Assessment
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barnholtz-Sloan, J.S.; Ostrom, Q.T.; Cote, D. Epidemiology of Brain Tumors. Neurol. Clin. 2018, 36, 395–419. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.D.; Ostrom, Q.T.; Kruchko, C.; Patil, N.; Tihan, T.; Cioffi, G.; Fuchs, H.E.; Waite, K.A.; Jemal, A.; Siegel, R.L.; et al. Brain and other central nervous system tumor statistics, 2021. CA Cancer J. Clin. 2021, 71, 381–406. [Google Scholar] [CrossRef] [PubMed]
- Ferroli, P.; Broggi, M.; Schiavolin, S.; Acerbi, F.; Bettamio, V.; Caldiroli, D.; Cusin, A.; La Corte, E.; Leonardi, M.; Raggi, A.; et al. Predicting functional impairment in brain tumor surgery: The Big Five and the Milan Complexity Scale. Neurosurg. Focus 2015, 39, E14. [Google Scholar] [CrossRef]
- Fuentes-Raspall, R.; Solans, M.; Roca-Barcelo, A.; Vilardell, L.; Puigdemont, M.; Del Barco, S.; Comas, R.; Garcia-Velasco, A.; Astudillo, A.; Carmona-Garcia, M.C.; et al. Descriptive epidemiology of primary malignant and non-malignant central nervous tumors in Spain: Results from the Girona Cancer Registry (1994–2013). Cancer Epidemiol. 2017, 50, 1–8. [Google Scholar] [CrossRef]
- Zetterling, M.; Elf, K.; Semnic, R.; Latini, F.; Engstrom, E.R. Time course of neurological deficits after surgery for primary brain tumours. Acta Neurochir. 2020, 162, 3005–3018. [Google Scholar] [CrossRef]
- Bartolo, M.; Zucchella, C.; Pace, A.; Lanzetta, G.; Vecchione, C.; Bartolo, M.; Grillea, G.; Serrao, M.; Tassorelli, C.; Sandrini, G.; et al. Early rehabilitation after surgery improves functional outcome in inpatients with brain tumours. J. Neurooncol. 2012, 107, 537–544. [Google Scholar] [CrossRef]
- Geler-Kulcu, D.; Gulsen, G.; Buyukbaba, E.; Ozkan, D. Functional recovery of patients with brain tumor or acute stroke after rehabilitation: A comparative study. J. Clin. Neurosci. 2009, 16, 74–78. [Google Scholar] [CrossRef]
- Greenberg, E.; Treger, I.; Ring, H. Rehabilitation outcomes in patients with brain tumors and acute stroke: Comparative study of inpatient rehabilitation. Am. J. Phys. Med. Rehabil. 2006, 85, 568–573. [Google Scholar] [CrossRef]
- Han, E.Y.; Chun, M.H.; Kim, B.R.; Kim, H.J. Functional Improvement After 4-Week Rehabilitation Therapy and Effects of Attention Deficit in Brain Tumor Patients: Comparison with Subacute Stroke Patients. Ann. Rehabil. Med. 2015, 39, 560–569. [Google Scholar] [CrossRef]
- Huang, M.E.; Cifu, D.X.; Keyser-Marcus, L. Functional outcome after brain tumor and acute stroke: A comparative analysis. Arch. Phys. Med. Rehabil. 1998, 79, 1386–1390. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, D.Y.; Chun, M.H.; Lee, S.J. Functional Outcomes and Characteristics of Patients with Brain Tumors after Inpatient Rehabilitation: Comparison with Ischemic Stroke. J. Korean Acad. Rehabil. Med. 2010, 34, 290–296. [Google Scholar]
- Loomis, E.; Wakasa, M. Rehabilitation from meningioma. Handb. Clin. Neurol. 2020, 170, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, P.; Greenwald, B.D.; Patel, P. Rehabilitation of Adult Patients with Primary Brain Tumors: A Narrative Review. Brain Sci. 2020, 10, 492. [Google Scholar] [CrossRef]
- Yu, J.; Jung, Y.; Park, J.; Kim, J.M.; Suh, M.; Cho, K.G.; Kim, M. Intensive Rehabilitation Therapy Following Brain Tumor Surgery: A Pilot Study of Effectiveness and Long-Term Satisfaction. Ann. Rehabil. Med. 2019, 43, 129–141. [Google Scholar] [CrossRef]
- Bilgin, S.; Kose, N.; Karakaya, J.; Mut, M. Traumatic brain injury shows better functional recovery than brain tumor: A rehabilitative perspective. Eur. J. Phys. Rehabil. Med. 2013, 50, 17–23. [Google Scholar] [PubMed]
- Huang, M.E.; Cifu, D.X.; Keyser-Marcus, L. Functional outcomes in patients with brain tumor after inpatient rehabilitation: Comparison with traumatic brain injury. Am. J. Phys. Med. Rehabil. 2000, 79, 327–335. [Google Scholar] [CrossRef]
- Dutta, D.; Vanere, P.; Gupta, T.; Munshi, A.; Jalali, R. Factors influencing activities of daily living using FIM–FAM scoring system before starting adjuvant treatment in patients with brain tumors: Results from a prospective study. J. Neurooncol. 2009, 94, 103–110. [Google Scholar] [CrossRef]
- Torres-Perez, P.; Álvarez-Satta, M.; Arrazola, M.; Egaña, L.; Moreno-Valladares, M.; Villanua, J.; Ruiz, I.; Sampron, N.; Matheu, A. Frailty is associated with mortality in brain tumor patients. Am. J. Cancer Res. 2021, 11, 3294. [Google Scholar]
- Marosi, C.; Hassler, M.; Roessler, K.; Reni, M.; Sant, M.; Mazza, E.; Vecht, C. Meningioma. Crit. Rev. Oncol. Hematol. 2008, 67, 153–171. [Google Scholar] [CrossRef]
- Vargo, M. Brain tumor rehabilitation. Am. J. Phys. Med. Rehabil. 2011, 90, S50–S62. [Google Scholar] [CrossRef]
- Chaichana, K.L.; Martinez-Gutierrez, J.C.; De la Garza-Ramos, R.; Weingart, J.D.; Olivi, A.; Gallia, G.L.; Lim, M.; Brem, H.; Quinones-Hinojosa, A. Factors associated with survival for patients with glioblastoma with poor pre-operative functional status. J. Clin. Neurosci. 2013, 20, 818–823. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.W.; Eves, N.D.; Haykowsky, M.; Freedland, S.J.; Mackey, J.R. Exercise intolerance in cancer and the role of exercise therapy to reverse dysfunction. Lancet Oncol. 2009, 10, 598–605. [Google Scholar] [CrossRef]
- Bates, A.; Gonzalez-Viana, E.; Cruickshank, G.; Roques, T. Primary and metastatic brain tumours in adults: Summary of NICE guidance. BMJ 2018, 362, k2924. [Google Scholar] [CrossRef]
- Kim, W.J.; Novotna, K.; Amatya, B.; Khan, F. Clinical practice guidelines for the management of brain tumours: A rehabilitation perspective. J. Rehabil. Med. 2019, 51, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.; Amatya, B.; Drummond, K.; Galea, M. Effectiveness of integrated multidisciplinary rehabilitation in primary brain cancer survivors in an Australian community cohort: A controlled clinical trial. J. Rehabil. Med. 2014, 46, 754–760. [Google Scholar] [CrossRef]
- Tang, V.; Rathbone, M.; Park Dorsay, J.; Jiang, S.; Harvey, D. Rehabilitation in primary and metastatic brain tumours: Impact of functional outcomes on survival. J. Neurol. 2008, 255, 820–827. [Google Scholar] [CrossRef] [PubMed]
- Roberts, P.S.; Nuno, M.; Sherman, D.; Asher, A.; Wertheimer, J.; Riggs, R.V.; Patil, C.G. The impact of inpatient rehabilitation on function and survival of newly diagnosed patients with glioblastoma. PM R 2014, 6, 514–521. [Google Scholar] [CrossRef]
- Kushner, D.S.; Amidei, C. Rehabilitation of motor dysfunction in primary brain tumor patients(dagger). Neurooncol. Pract. 2015, 2, 185–191. [Google Scholar] [CrossRef]
- Pace, A.; Parisi, C.; Di Lelio, M.; Zizzari, A.; Petreri, G.; Giovannelli, M.; Pompili, A. Home rehabilitation for brain tumor patients. J. Exp. Clin. Cancer Res. 2007, 26, 297–300. [Google Scholar]
- Piil, K.; Juhler, M.; Jakobsen, J.; Jarden, M. Daily life experiences of patients with a high-grade glioma and their caregivers: A longitudinal exploration of rehabilitation and supportive care needs. J. Neurosci. Nurs. 2015, 47, 271–284. [Google Scholar] [CrossRef] [PubMed]
- Krajewski, S.; Furtak, J.; Zawadka-Kunikowska, M.; Kachelski, M.; Birski, M.; Harat, M. Comparison of the Functional State and Motor Skills of Patients after Cerebral Hemisphere, Ventricular System, and Cerebellopontine Angle Tumor Surgery. Int. J. Environ. Res. Public Health 2022, 19, 2308. [Google Scholar] [CrossRef]
- Krajewski, S.; Furtak, J.; Zawadka-Kunikowska, M.; Kachelski, M.; Birski, M.; Harat, M. Rehabilitation Outcomes for Patients with Motor Deficits after Initial and Repeat Brain Tumor Surgery. Int. J. Environ. Res. Public Health 2022, 19, 10871. [Google Scholar] [CrossRef] [PubMed]
- Banks, J.L.; Marotta, C.A. Outcomes validity and reliability of the modified Rankin scale: Implications for stroke clinical trials: A literature review and synthesis. Stroke 2007, 38, 1091–1096. [Google Scholar] [CrossRef]
- Giga, L.; Petersone, A.; Cakstina, S.; Berzina, G. Comparison of content and psychometric properties for assessment tools used for brain tumor patients: A scoping review. Health Qual. Life Outcomes 2021, 19, 234. [Google Scholar] [CrossRef]
- Grieco, A.; Long, C.J. Investigation of the Karnofsky Performance Status as a measure of quality of life. Health Psychol. 1984, 3, 129. [Google Scholar] [CrossRef] [PubMed]
- Peus, D.; Newcomb, N.; Hofer, S. Appraisal of the Karnofsky Performance Status and proposal of a simple algorithmic system for its evaluation. BMC Med. Inform. Decis. Mak. 2013, 13, 72. [Google Scholar] [CrossRef] [PubMed]
- Schag, C.C.; Heinrich, R.L.; Ganz, P.A. Karnofsky performance status revisited: Reliability, validity, and guidelines. J. Clin. Oncol. 1984, 2, 187–193. [Google Scholar] [CrossRef]
- Wilson, J.T.; Hareendran, A.; Hendry, A.; Potter, J.; Bone, I.; Muir, K.W. Reliability of the modified Rankin Scale across multiple raters: Benefits of a structured interview. Stroke 2005, 36, 777–781. [Google Scholar] [CrossRef]
- Ibañez, F.A.L.; Hem, S.; Ajler, P.; Vecchi, E.; Ciraolo, C.; Baccanelli, M.; Tramontano, R.; Knezevich, F.; Carrizo, A. A new classification of complications in neurosurgery. World Neurosurg. 2011, 75, 709–715. [Google Scholar] [CrossRef]
- Ferroli, P.; Brock, S.; Leonardi, M.; Schiavolin, S.; Acerbi, F.; Broggi, M. Complications in neurosurgery: Application of Landriel Ibanez classification and preliminary considerations on 1000 cases. World Neurosurg. 2014, 82, e576–e577. [Google Scholar] [CrossRef]
- Sarnthein, J.; Stieglitz, L.; Clavien, P.A.; Regli, L. A Patient Registry to Improve Patient Safety: Recording General Neurosurgery Complications. PLoS ONE 2016, 11, e0163154. [Google Scholar] [CrossRef] [PubMed]
- Schiavolin, S.; Broggi, M.; Acerbi, F.; Brock, S.; Schiariti, M.; Cusin, A.; Visintini, S.; Leonardi, M.; Ferroli, P. The Impact of Neurosurgical Complications on Patients’ Health Status: A Comparison Between Different Grades of Complications. World Neurosurg. 2015, 84, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Natsume, K.; Sakakima, H.; Kawamura, K.; Yoshida, A.; Akihiro, S.; Yonezawa, H.; Yoshimoto, K.; Shimodozono, M. Factors Influencing the Improvement of Activities of Daily Living during Inpatient Rehabilitation in Newly Diagnosed Patients with Glioblastoma Multiforme. J. Clin. Med. 2022, 11, 417. [Google Scholar] [CrossRef] [PubMed]
- Blanshard, H.J.; Chung, F.; Manninen, P.H.; Taylor, M.D.; Bernstein, M. Awake craniotomy for removal of intracranial tumor: Considerations for early discharge. Anesth. Analg. 2001, 92, 89–94. [Google Scholar] [CrossRef]
- Reponen, E.; Tuominen, H.; Hernesniemi, J.; Korja, M. Modified Rankin Scale and Short-Term Outcome in Cranial Neurosurgery: A Prospective and Unselected Cohort Study. World Neurosurg. 2016, 91, 567–573.e7. [Google Scholar] [CrossRef] [PubMed]
- Reponen, E.; Tuominen, H.; Korja, M. Evidence for the use of preoperative risk assessment scores in elective cranial neurosurgery: A systematic review of the literature. Anesth. Analg. 2014, 119, 420–432. [Google Scholar] [CrossRef]
- Richardson, A.M.; McCarthy, D.J.; Sandhu, J.; Mayrand, R.; Guerrero, C.; Rosenberg, C.; Gernsback, J.E.; Komotar, R.; Ivan, M. Predictors of Successful Discharge of Patients on Postoperative Day 1 After Craniotomy for Brain Tumor. World Neurosurg. 2019, 126, e869–e877. [Google Scholar] [CrossRef]
- Brazil, L.; Thomas, R.; Laing, R.; Hines, F.; Guerrero, D.; Ashley, S.; Brada, M. Verbally administered Barthel Index as functional assessment in brain tumour patients. J. Neurooncol. 1997, 34, 187–192. [Google Scholar] [CrossRef]
- Kreisl, T.N.; Toothaker, T.; Karimi, S.; DeAngelis, L.M. Ischemic stroke in patients with primary brain tumors. Neurology 2008, 70, 2314–2320. [Google Scholar] [CrossRef]
- Sandin, K.J.; Smith, B.S. The measure of balance in sitting in stroke rehabilitation prognosis. Stroke 1990, 21, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Dulaney, C.R.; McDonald, A.M.; Wallace, A.S.; Fiveash, J. Gait Speed and Survival in Patients with Brain Metastases. J. Pain Symptom Manag. 2017, 54, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Lamborn, K.R.; Yung, W.K.; Chang, S.M.; Wen, P.Y.; Cloughesy, T.F.; DeAngelis, L.M.; Robins, H.I.; Lieberman, F.S.; Fine, H.A.; Fink, K.L.; et al. Progression-free survival: An important end point in evaluating therapy for recurrent high-grade gliomas. Neuro Oncol. 2008, 10, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Page, M.; Solheim, K.; Fox, S.; Chang, S.M. Quality of life in adults with brain tumors: Current knowledge and future directions. Neuro Oncol. 2009, 11, 330–339. [Google Scholar] [CrossRef]
- Mackworth, N.; Fobair, P.; Prados, M.D. Quality of life self-reports from 200 brain tumor patients: Comparisons with Karnofsky performance scores. J. Neurooncol. 1992, 14, 243–253. [Google Scholar] [CrossRef]
- Czigleczki, G.; Sinko, D.; Benko, Z.; Bago, A.; Fedorcsak, I.; Sipos, L. He effect of bevacizumab monotherapy on progression free survival in recurrent glioblastoma]. Ideggyogy Sz. 2019, 72, 153–158. [Google Scholar] [CrossRef]
- Long, D.M.; Gordon, T.; Bowman, H.; Etzel, A.; Burleyson, G.; Betchen, S.; Garonzik, I.M.; Brem, H. Outcome and cost of craniotomy performed to treat tumors in regional academic referral centers. Neurosurgery 2003, 52, 1056–1063, discussion 1063–1055. [Google Scholar]
- Groshev, A.; Padalia, D.; Patel, S.; Garcia-Getting, R.; Sahebjam, S.; Forsyth, P.A.; Vrionis, F.D.; Etame, A.B. Clinical outcomes from maximum-safe resection of primary and metastatic brain tumors using awake craniotomy. Clin. Neurol. Neurosurg. 2017, 157, 25–30. [Google Scholar] [CrossRef]
- Kos, N.; Kos, B.; Benedicic, M. Early medical rehabilitation after neurosurgical treatment of malignant brain tumours in Slovenia. Radiol. Oncol. 2016, 50, 139–144. [Google Scholar] [CrossRef]
- Cain, B.T.; Horns, J.J.; Huang, L.C.; McCrum, M.L. Socioeconomic disadvantage is associated with greater mortality after high-risk emergency general surgery. J. Trauma Acute Care Surg. 2022, 92, 691–700. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, A.K.; Unruh, M.A.; Soroka, O.; Shapiro, M. Trends in Medical and Surgical Admission Length of Stay by Race/Ethnicity and Socioeconomic Status: A Time Series Analysis. Health Serv. Res. Manag. Epidemiol. 2021, 8, 23333928211035581. [Google Scholar] [CrossRef] [PubMed]
- Moore, L.; Cisse, B.; Batomen Kuimi, B.L.; Stelfox, H.T.; Turgeon, A.F.; Lauzier, F.; Clement, J.; Bourgeois, G. Impact of socio-economic status on hospital length of stay following injury: A multicenter cohort study. BMC Health Serv. Res. 2015, 15, 285. [Google Scholar] [CrossRef] [PubMed]
- Kasper, G.; Hart, S.; Samuel, N.; Fox, C.; Das, S. Anxiety and depression in patients with intracranial meningioma: A mixed methods analysis. BMC Psychol. 2022, 10, 93. [Google Scholar] [CrossRef] [PubMed]
- Day, J.; Gillespie, D.C.; Rooney, A.G.; Bulbeck, H.J.; Zienius, K.; Boele, F.; Grant, R. Neurocognitive Deficits and Neurocognitive Rehabilitation in Adult Brain Tumors. Curr. Treat. Options Neurol. 2016, 18, 22. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Type of Tumor | Type of Neoplasm | WHO Grade | n | % |
|---|---|---|---|---|
| Hemangioblastoma | 5 | 5.4 | ||
| Benign | Hemangioma cavernosum | 2 | 2.2 | |
| WHO grade I | Meningioma | I | 21 | 22.8 |
| Schwannoma | I | 15 | 16.3 | |
| Other benign tumors | 5 | 5.4 | ||
| Astrocytoma | II | 3 | 3.3 | |
| Low-grade gliomas | Diffuse astrocytoma | II | 7 | 7.6 |
| WHO grade II | Oligodendroglioma | II | 1 | 1.1 |
| Ependymoma | II | 3 | 3.3 | |
| Meningioma atypicum | II | 3 | 3.3 | |
| Central neurocystoma | II | 1 | 1.1 | |
| Total nonmalignant tumors | 66 | 71.7 | ||
| Anaplastic astrocytoma | III | 5 | 5.4 | |
| Malignant | Anaplastic oligodendroglioma | III | 1 | 1.1 |
| WHO grade III, IV | Anaplastic ependymoma | III | 2 | 2.2 |
| Glioblastoma | IV | 16 | 17.4 | |
| Meningioma anaplasticum | III | 1 | 1.1 | |
| Supratentorial primitive neuroectodermal tumor | IV | 1 | 1.1 | |
| Total malignant tumors | 26 | 28.3 | ||
| Total tumors | 92 | 100 |
| Malignant n = 26 | Nonmalignant n = 66 | p-Value | |
|---|---|---|---|
| n (%) | n (%) | ||
| Male n (%) | 14 (53.8) | 31 (47.0) | 0.552 |
| Female n (%) | 12 (46.2) | 35 (53.0) | |
| Mean ± SD [range] | Mean ± SD [range] | ||
| Age (years) | 51.9 ± 16.9 [23–82] | 48.1 ± 17.8 [19–83] | 0.352 |
| Overall LoS (days) | 19.1 ± 9.7 [8–40] | 21.3 ± 15.0 [4–92] | 0.491 |
| LoS after surgery (days) | 15.2 ± 8.5 [6–31] | 17.8 ± 14.7 [2–90] | 0.399 |
| Days in ICU after surgery | 0.1 ± 0.3 [0–1] | 1.0 ± 4.1 [0–31] | 0.268 |
| Days of rehabilitation | 11.7 ± 6.9 [3–26] | 13.3 ± 10.6 [1–53] | 0.478 |
| Malignant | Nonmalignant | Total | p-Value | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Patients with complications | 7 | 26.9 | 18 | 27.3 | 25 | 27.2 | 0.973 |
| Grade I | 1 | 3.8 | 3 | 4.5 | 4 | 4.3 | |
| Grade II | 4 | 15.4 | 11 | 16.7 | 15 | 16.3 | 0.944 |
| Grade III | 2 | 7.7 | 4 | 6.1 | 6 | 6.5 | |
| Surgical | 6 | 23.1 | 15 | 22.7 | 21 | 22.8 | 0.884 |
| Medical | 1 | 3.8 | 3 | 4.5 | 4 | 4.3 | |
| Temporary | 4 | 15.4 | 13 | 19.7 | 17 | 18.5 | 0.468 |
| Permanent | 3 | 11.5 | 5 | 9.1 | 8 | 8.7 | |
| Plegia/paresis | |||||||
| Before surgery | 17 | 65.4 | 14 | 21.2 | 31 | 33.7 | <0.001 |
| At discharge | 22 | 84.6 | 38 | 57.6 | 60 | 85.2 | 0.014 |
| Variable | Time | Malignant | Nonmalignant | Source | F | p-Value |
|---|---|---|---|---|---|---|
| Mean ± SE | Mean ± SE | |||||
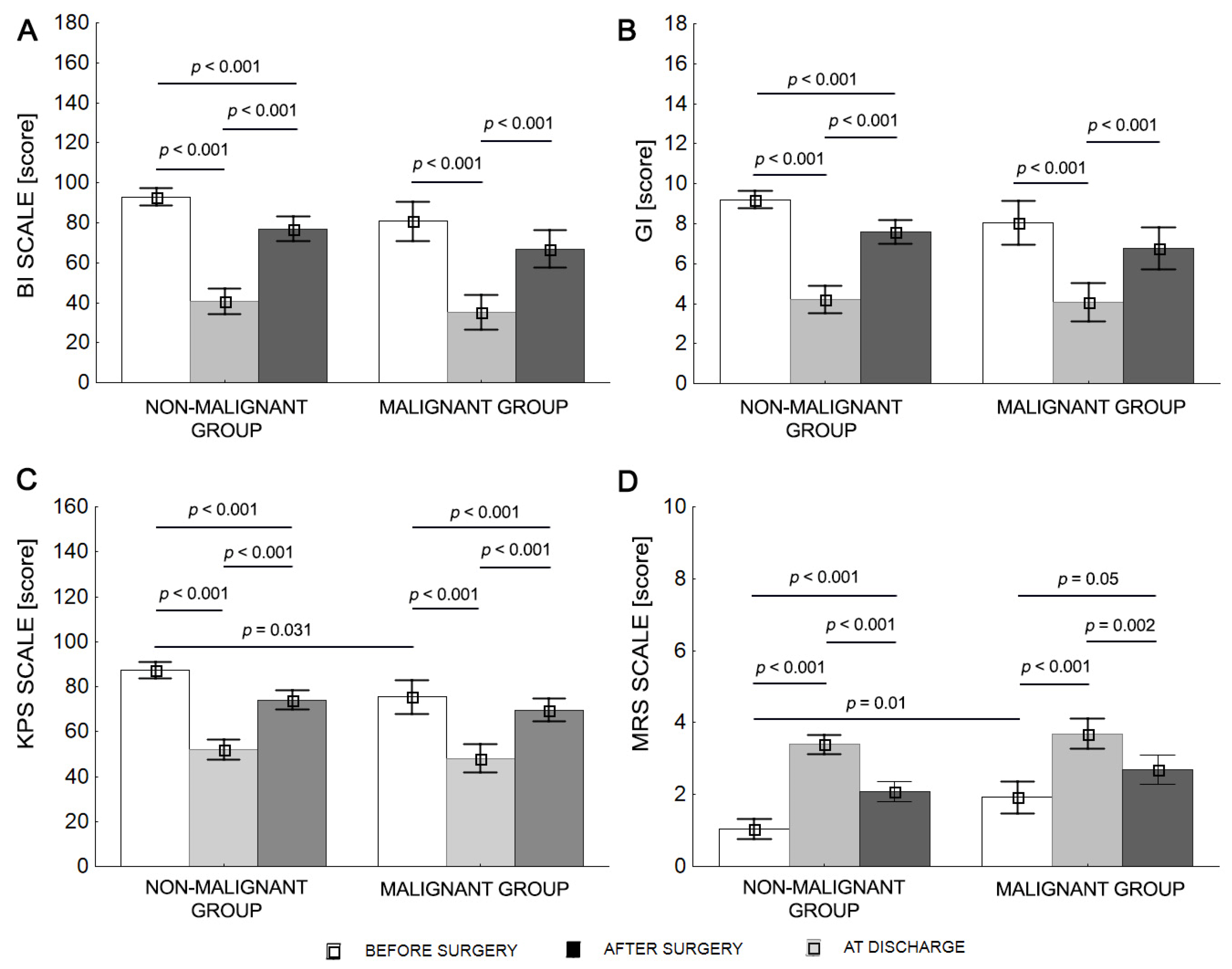
| BI | Before surgery | 80.8 ± 3.97 | 93.0 ± 2.49 | Group | 5.05 | 0.027 |
| After surgery | 35.4 ± 4.91 | 40.8 ± 3.08 | Time | 132.32 | <0.001 | |
| At discharge | 66.9 ± 4.84 | 77.0 ± 3.04 | G × T | 0.63 | 0.535 | |
| KPS | Before surgery | 75.4 ± 3.20 | 87.4 ± 2.01 | Group | 6.01 | 0.016 |
| After surgery | 48.1 ± 3.49 | 52.0 ± 2.19 | Time | 95.74 | <0.001 | |
| At discharge | 69.6 ± 3.11 | 74.1 ± 1.95 | G × T | 1.91 | 0.151 | |
| MRS | Before surgery | 1.9 ± 0.22 | 1.0 ± 014 | Group | 10.70 | 0.002 |
| After surgery | 3.7 ± 0.21 | 3.4 ± 0.13 | Time | 91.62 | <0.001 | |
| At discharge | 2.7 ± 0.22 | 2.1 ± 0.14 | G × T | 1.81 | 0.167 | |
| GI | Before surgery | 8.0 ± 0.41 | 9.2 ± 0.26 | Group | 2.92 | 0.091 |
| After surgery | 4.1 ± 0.53 | 4.2 ± 0.33 | Time | 91.96 | <0.001 | |
| At discharge | 6.8 ± 0.49 | 7.6 ± 0.31 | G × T | 1.23 | 0.294 |
| Motor Skills | Malignant | Nonmalignant | p-Value |
|---|---|---|---|
| n (%) | n (%) | ||
| Before surgery | |||
| Passive sitting | 26 (100%) | 66 (100%) | 1.000 |
| Active sitting | 25 (96.2%) | 66 (100%) | 0.109 |
| Standing | 23 (88.5%) | 64 (97.0%) | 0.105 |
| Independent gait | 21 (80.8%) | 63 (95.5%) | 0.024 |
| Week after surgery | |||
| Passive sitting | 24 (92.3%) | 60 (90.1%) | 0.830 |
| Active sitting | 19 (73.1%) | 55 (83.3%) | 0.264 |
| Standing | 15 (58.7%) | 41 (62.1%) | 0.695 |
| Independent gait | 7 (26.9%) | 28 (42.4%) | 0.168 |
| At discharge | |||
| Passive sitting | 26 (100%) | 66 (100%) | 1.000 |
| Active sitting | 24 (92.3%) | 63 (95.5%) | 0.548 |
| Standing | 22 (84.7%) | 60 (90.1%) | 0.382 |
| Independent gait | 13 (50.0%) | 44 (66.7%) | 0.138 |
| After Surgery | Malignant | Nonmalignant | p-Value |
|---|---|---|---|
| (Days) | Mean ± SD [Range] | Mean ± SD [Range] | |
| Passive sitting | 3.9 ± 4.5 [1–18] | 4.3 ± 8.5 [1–66] | 0.820 |
| Active sitting | 4.3 ± 5.3 [1–21] | 4.0 ± 4.8 [1–32] | 0.793 |
| Independent standing | 7.5 ± 8.2 [1–27] | 7.5 ± 8.0 [1–45] | 1.000 |
| Independent gait | 8.3 ± 7.4 [1–26] | 8.5 ± 8.0 [1–32] | 0.912 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krajewski, S.; Furtak, J.; Zawadka-Kunikowska, M.; Kachelski, M.; Soboń, J.; Harat, M. Functional State and Rehabilitation of Patients after Primary Brain Tumor Surgery for Malignant and Nonmalignant Tumors: A Prospective Observational Study. Curr. Oncol. 2023, 30, 5182-5194. https://doi.org/10.3390/curroncol30050393
Krajewski S, Furtak J, Zawadka-Kunikowska M, Kachelski M, Soboń J, Harat M. Functional State and Rehabilitation of Patients after Primary Brain Tumor Surgery for Malignant and Nonmalignant Tumors: A Prospective Observational Study. Current Oncology. 2023; 30(5):5182-5194. https://doi.org/10.3390/curroncol30050393
Chicago/Turabian StyleKrajewski, Stanisław, Jacek Furtak, Monika Zawadka-Kunikowska, Michał Kachelski, Jakub Soboń, and Marek Harat. 2023. "Functional State and Rehabilitation of Patients after Primary Brain Tumor Surgery for Malignant and Nonmalignant Tumors: A Prospective Observational Study" Current Oncology 30, no. 5: 5182-5194. https://doi.org/10.3390/curroncol30050393
APA StyleKrajewski, S., Furtak, J., Zawadka-Kunikowska, M., Kachelski, M., Soboń, J., & Harat, M. (2023). Functional State and Rehabilitation of Patients after Primary Brain Tumor Surgery for Malignant and Nonmalignant Tumors: A Prospective Observational Study. Current Oncology, 30(5), 5182-5194. https://doi.org/10.3390/curroncol30050393