The Impact of the Early COVID-19 Global Pandemic on Children Undergoing Active Cancer Treatment and Their Parents

 , , ,
, , ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Recruitment
2.2. Participants
2.3. Procedure
2.4. Measures
2.4.1. Demographic and Clinical Information
2.4.2. COVID-19 and Cancer Questionnaire
2.4.3. Mental Health Status
2.5. Statistical Analyses
3. Results
3.1. Descriptive and Clinical Characteristics
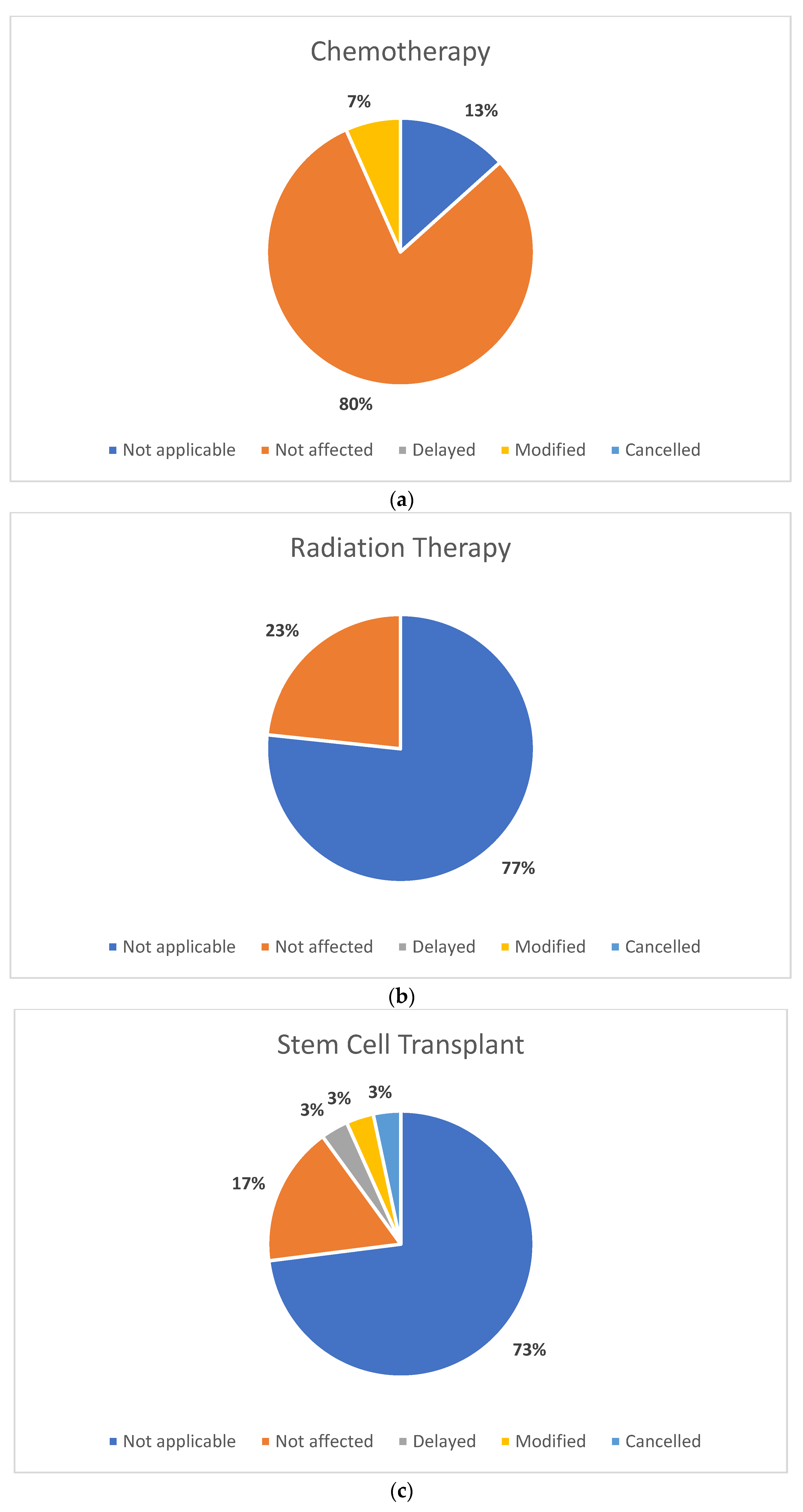
3.2. Objective 1: Changes (Delays, Modifications, Cancellations) to Health Care
3.3. Objective 2: Perceived Utility (Benefit and Effectiveness) of Telemedicine
3.4. Objective 3: Child and Parent Mental Health Status
3.5. Objective 4: Impact of Health Care Changes and Perceived Utility of Telemedicine on Child and Parent Mental Health Status
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Steliarova-Foucher, E.; Colombet, M.; Ries, L.A.G.; Moreno, F.; Dolya, A.; Bray, F.; Hesseling, P.; Shin, H.Y.; Stiller, C.A.; Bouzbid, S.; et al. International incidence of childhood cancer, 2001–2010: A population-based registry study. Lancet Oncol. 2017, 18, 719–731. [Google Scholar] [CrossRef] [PubMed]
- Ikonomidou, C. Chemotherapy and the pediatric brain. Mol. Cell. Pediatr. 2018, 5, 8. [Google Scholar] [CrossRef] [PubMed]
- Alessi, I.; Caroleo, A.M.; de Palma, L.; Mastronuzzi, A.; Pro, S.; Colafati, G.S.; Boni, A.; Della Vecchia, N.; Velardi, M.; Evangelisti, M.; et al. Short and Long-Term Toxicity in Pediatric Cancer Treatment: Central Nervous System Damage. Cancers 2022, 14, 1540. [Google Scholar] [CrossRef] [PubMed]
- Ellison, L.F.; De, P.; Mery, L.S.; Grundy, P.E. Canadian cancer statistics at a glance: Cancer in children. Can. Med. Assoc. J. 2009, 180, 422–424. [Google Scholar] [CrossRef]
- Committee Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics 2021. 2021. Available online: http://cancer.ca/Canadian-Cancer-Statistics-2021-EN (accessed on 14 May 2022).
- Miller, K.D.; Siegel, R.L.; Lin, C.C.; Mariotto, A.B.; Kramer, J.L.; Rowland, J.H.; Stein, K.D.; Alteri, R.; Jemal, A. Cancer treatment and survivorship statistics, 2016. CA Cancer J. Clin. 2016, 66, 271–289. [Google Scholar] [CrossRef]
- Love, R.R.; Leventhal, H.; Easterling, D.V.; Nerenz, D.R. Side effects and emotional distress during cancer chemotherapy. Cancer 1989, 63, 604–612. [Google Scholar] [CrossRef]
- Tonorezos, E.S.; Cohn, R.J.; Glaser, A.W.; Lewin, J.; Poon, E.; Wakefield, C.E.; Oeffinger, K.C. Long-term care for people treated for cancer during childhood and adolescence. Lancet 2022, 399, 1561–1572. [Google Scholar] [CrossRef]
- Frederiksen, L.E.; Mader, L.; Feychting, M.; Mogensen, H.; Madanat-Harjuoja, L.; Malila, N.; Tolkkinen, A.; Hasle, H.; Winther, J.F.; Erdmann, F. Surviving childhood cancer: A systematic review of studies on risk and determinants of adverse socioeconomic outcomes. Int. J. Cancer 2019, 144, 1796–1823. [Google Scholar] [CrossRef]
- Nathan, P.C.; Nachman, A.; Sutradhar, R.; Kurdyak, P.; Pole, J.D.; Lau, C.; Gupta, S. Adverse mental health outcomes in a population-based cohort of survivors of childhood cancer. Cancer 2018, 124, 2045–2057. [Google Scholar] [CrossRef]
- Brinkman, T.M.; Recklitis, C.J.; Michel, G.; Grootenhuis, M.A.; Klosky, J.L. Psychological Symptoms, Social Outcomes, Socioeconomic Attainment, and Health Behaviors Among Survivors of Childhood Cancer: Current State of the Literature. J. Clin. Oncol. 2018, 36, 2190–2197. [Google Scholar] [CrossRef]
- Children with Cancer UK. Almost Half of Childhood Cancer Patients Suffer Mental Health Problems. 2018. Available online: https://www.childrenwithcancer.org.uk/stories/almost-half-of-childhood-cancer-patients-suffer-mental-health-problems-due-to-harsh-treatments/ (accessed on 27 June 2022).
- Michel, G.; Brinkman, T.M.; Wakefield, C.E.; Grootenhuis, M. Psychological Outcomes, Health-Related Quality of Life, and Neurocognitive Functioning in Survivors of Childhood Cancer and Their Parents. Pediatr. Clin. N. Am. 2020, 67, 1103–1134. [Google Scholar] [CrossRef] [PubMed]
- Schulte, F.; Forbes, C.; Wurz, A.; Patton, M.; Russell, K.B.; Pluijm, S.; Krull, K.R. Childhood Cancer Survivorship. Pediatr. Clin. N. Am. 2020, 67, 1083–1101. [Google Scholar] [CrossRef]
- World Health Organization. Origin of SARS-CoV-2. 2020. Available online: https://www.who.int/publications/i/item/origin-of-sars-cov-2 (accessed on 14 June 2022).
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. 2022. Available online: https://covid19.who.int/ (accessed on 14 June 2022).
- Children’s Oncology Group. COVID-19 and Your Child, Teen, or Young Adult with Cancer; Children’s Oncology Group: Monrovia, CA, USA, 2021. [Google Scholar]
- Millen, G.C.; Arnold, R.; Cazier, J.B.; Curley, H.; Feltbower, R.G.; Gamble, A.; Glaser, A.W.; Grundy, R.G.; Lee, L.Y.W.; McCabe, M.G.; et al. Severity of COVID-19 in children with cancer: Report from the United Kingdom Paediatric Coronavirus Cancer Monitoring Project. Br. J. Cancer 2021, 124, 754–759. [Google Scholar] [CrossRef] [PubMed]
- Kaspers, G.J.L. COVID-19: How will this impact children with cancer, now and in the future? Expert Rev. Anticancer Ther. 2020, 20, 527–529. [Google Scholar] [CrossRef]
- Auletta, J.J.; Adamson, P.C.; Agin, J.E.; Kearns, P.; Kennedy, S.; Kieran, M.W.; Ludwinski, D.M.; Knox, L.J.; McKay, K.; Rhiner, P.; et al. Pediatric cancer research: Surviving COVID-19. Pediatr. Blood Cancer 2020, 67, e28435. [Google Scholar] [CrossRef]
- Mukkada, S.; Bhakta, N.; Chantada, G.L.; Chen, Y.; Vedaraju, Y.; Faughnan, L.; Homsi, M.R.; Muniz-Talavera, H.; Ranadive, R.; Metzger, M.; et al. Global characteristics and outcomes of SARS-CoV-2 infection in children and adolescents with cancer (GRCCC): A cohort study. Lancet Oncol. 2021, 22, 1416–1426. [Google Scholar] [CrossRef]
- Forster, V.J.; Schulte, F. Unique needs of childhood cancer survivors during the COVID-19 pandemic. Support. Care Cancer 2021, 29, 17–19. [Google Scholar] [CrossRef]
- Gilchrist, L.S.; Tanner, L.R.; Ness, K.K. Short-term recovery of chemotherapy-induced peripheral neuropathy after treatment for pediatric non-CNS cancer. Pediatr. Blood Cancer 2017, 64, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, A.; Rizzo, D.; Catalano, M.; Coccia, P.; Triarico, S.; Attiná, G. Acute chemotherapy-induced nausea and vomiting in children with cancer: Still waiting for a common consensus on treatment. J. Int. Med. Res. 2018, 46, 2149–2156. [Google Scholar] [CrossRef]
- Moreira, D.C.; Millen, G.C.; Sands, S.; Kearns, P.R.; Hawkins, D.S. The Care of Children with Cancer during the COVID-19 Pandemic. Am. Soc. Clin. Oncol. Educ. Book 2021, 41, e305–e314. [Google Scholar] [CrossRef]
- Cheung, A.T.; Li, W.H.C.; Ho, L.L.K.; Chan, G.C.F.; Chung, J.O.K. Health support to pediatric cancer survivors and their families during the COVID-19 pandemic. Pediatr. Blood Cancer 2020, 67, e28441. [Google Scholar] [CrossRef] [PubMed]
- Darlington, A.S.E.; Morgan, J.E.; Wagland, R.; Sodergren, S.C.; Culliford, D.; Gamble, A.; Phillips, B. COVID-19 and children with cancer: Parents’ experiences, anxieties and support needs. Pediatr. Blood Cancer 2021, 68, e28790. [Google Scholar] [CrossRef]
- Pacheco, R.L.; Martimbianco, A.L.C.; Roitberg, F.; Ilbawi, A.; Riera, R. Impact of Strategies for Mitigating Delays and Disruptions in Cancer Care Due to COVID-19: Systematic Review. JCO Glob. Oncol. 2021, 7, 342–352. [Google Scholar] [CrossRef]
- Meena, J.P.; Kumar Gupta, A.; Tanwar, P.; Ram Jat, K.; Mohan Pandey, R.; Seth, R. Clinical presentations and outcomes of children with cancer and COVID-19: A systematic review. Pediatr. Blood Cancer 2021, 68, e29005. [Google Scholar] [CrossRef] [PubMed]
- Graetz, D.; Agulnik, A.; Ranadive, R.; Vedaraju, Y.; Chen, Y.; Chantada, G.; Metzger, M.L.; Mukkada, S.; Force, L.M.; Friedrich, P.; et al. Global effect of the COVID-19 pandemic on paediatric cancer care: A cross-sectional study. Lancet Child. Adolesc. Health 2021, 5, 332–340. [Google Scholar] [CrossRef] [PubMed]
- Riera, R.; Bagattini, Â.M.; Pacheco, R.L.; Pachito, D.V.; Roitberg, F.; Ilbawi, A. Delays and Disruptions in Cancer Health Care Due to COVID-19 Pandemic: Systematic Review. JCO Glob. Oncol. 2021, 7, 311–323. [Google Scholar] [CrossRef] [PubMed]
- Connelly, J.A.; Chong, H.; Esbenshade, A.J.; Frame, D.; Failing, C.; Secord, E.; Walkovich, K. Impact of COVID-19 on Pediatric Immunocompromised Patients. Pediatr. Clin. N. Am. 2021, 68, 1029–1054. [Google Scholar] [CrossRef]
- van den Oever, S.R.; Pluijm, S.M.F.; Skinner, R.; Glaser, A.; Mulder, R.L.; Armenian, S.; Bardi, E.; Berger, C.; Ehrhardt, M.J.; Gilleland Marchak, J.; et al. Childhood cancer survivorship care during the COVID-19 pandemic: An international report of practice implications and provider concerns. J. Cancer Surviv. 2022, 16, 1390–1400. [Google Scholar] [CrossRef]
- Arem, H.; Moses, J.; Cisneros, C.; Blondeau, B.; Nekhlyudov, L.; Killackey, M.; Pratt-Chapman, M.L. Cancer Provider and Survivor Experiences with Telehealth during the COVID-19 Pandemic. JCO Oncol. Pract. 2022, 18, e452–e461. [Google Scholar] [CrossRef]
- Geng-Ramos, G.; Taneja, R.; Challa, C.; Vazquez- Colon, C.; Cronin, J.; Campos, A.; Selekman, R.; Rana, M.S.; Melwani, A. Telemedicine for the pediatric preoperative assessment during the COVID-19 pandemic: Evaluating patient and provider satisfaction. Perioper. Care Oper. Room Manag. 2022, 27, 100252. [Google Scholar] [CrossRef]
- McAndrew, N.S.; Strong, Y.; Morris, K.J.; Sannes, T.S.; Pirl, W.F.; Cole, S.; Mohanraj, L.; Knight, J.M. Impact of the COVID-19 pandemic on cancer patients and psycho-oncology providers: Perspectives, observations, and experiences of the American Psychosocial Oncology Society membership. Psychooncology 2022, 31, 1031–1040. [Google Scholar] [CrossRef]
- McLoone, J.; Wakefield, C.E.; Taylor, N.; Johnston, K.; Sansom-Daly, U.M.; Cohen, J.; O’Brien, T.A.; Cohn, R.J.; Signorelli, C. The COVID-19 pandemic: Distance-delivered care for childhood cancer survivors. Pediatr. Blood Cancer 2020, 67, e28715. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.C.; O’Dwyer, L.C.; Badawy, S.M. Telemedicine in Malignant and Nonmalignant Hematology: Systematic Review of Pediatric and Adult Studies. JMIR mHealth uHealth 2021, 9, e29619. [Google Scholar] [CrossRef] [PubMed]
- Kermani, F.; Orooji, A.; Sheikhtaheri, A. Teleoncology for children with cancer: A scoping review on applications and outcomes. Int. J. Med. Inform. 2020, 139, 104118. [Google Scholar] [CrossRef] [PubMed]
- Curfman, A.; McSwain, S.D.; Chuo, J.; Yeager-McSwain, B.; Schinasi, D.A.; Marcin, J.; Herendeen, N.; Chung, S.L.; Rheuban, K.; Olson, C.A. Pediatric Telehealth in the COVID-19 Pandemic Era and Beyond. Pediatrics 2021, 148, e2020047795. [Google Scholar] [CrossRef] [PubMed]
- Ng, D.W.L.; Chan, F.H.F.; Barry, T.J.; Lam, C.; Chong, C.Y.; Kok, H.C.S.; Liao, Q.; Fielding, R.; Lam, W.W.T. Psychological distress during the 2019 Coronavirus Disease (COVID-19) pandemic among cancer survivors and healthy controls. Psychooncology 2020, 29, 1380–1383. [Google Scholar] [CrossRef] [PubMed]
- Nekhlyudov, L.; Duijts, S.; Hudson, S.V.; Jones, J.M.; Keogh, J.; Love, B.; Lustberg, M.; Smith, K.C.; Tevaarwerk, A.; Yu, X.; et al. Addressing the needs of cancer survivors during the COVID-19 pandemic. J. Cancer Surviv. 2020, 14, 601–606. [Google Scholar] [CrossRef]
- Hou, S.; Tran, A.; Cho, S.; Forbes, C.; Forster, V.; Stokoe, M.; Allapitan, E.; Wakefield, C.; Wiener, L.; Heathcote, L.; et al. The perceived impact of COVID-19 on the mental health status of adolescent and young adult survivors of childhood cancer and the development of a knowledge translation tool to support their information needs. Front. Psychol. 2022, 13, 2664. [Google Scholar] [CrossRef]
- Košir, U.; Loades, M.; Wild, J.; Wiedemann, M.; Krajnc, A.; Roškar, S.; Bowes, L. The impact of COVID-19 on the cancer care of adolescents and young adults and their well-being: Results from an online survey conducted in the early stages of the pandemic. Cancer 2020, 126, 4414–4422. [Google Scholar] [CrossRef]
- Weaver, M.S.; Robinson, J.E.; Shostrom, V.K.; Hinds, P.S. Telehealth Acceptability for Children, Family, and Adult Hospice Nurses When Integrating the Pediatric Palliative Inpatient Provider during Sequential Rural Home Hospice Visits. J. Palliat. Med. 2020, 23, 641–649. [Google Scholar] [CrossRef]
- Weaver, M.S.; Shostrom, V.K.; Neumann, M.L.; Robinson, J.E.; Hinds, P.S. Homestead together: Pediatric palliative care telehealth support for rural children with cancer during home-based end-of-life care. Pediatr. Blood Cancer 2021, 68, e28921. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.; Bouffet, E.; Rodriguez-Galindo, C.; Luna-Fineman, S.; Khan, M.S.; Kearns, P.; Hawkins, D.S.; Challinor, J.; Morrissey, L.; Fuchs, J.; et al. The COVID-19 pandemic: A rapid global response for children with cancer from SIOP, COG, SIOP-E, SIOP-PODC, IPSO, PROS, CCI, and St Jude Global. Pediatr. Blood Cancer 2020, 67, e28409. [Google Scholar] [CrossRef] [PubMed]
- Alshahrani, M.; Elyamany, G.; Sedick, Q.; Ibrahim, W.; Mohamed, A.; Othman, M.; Al Thibani, N.; Alsuhaibani, O.; Al Amro, M.; Gharawi, A.; et al. The Impact of COVID-19 Pandemic in Children with Cancer: A Report From Saudi Arabia. Health Serv. Insights 2020, 13, 117863292098416. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Cella, D.; Yount, S.; Rothrock, N.; Gershon, R.; Cook, K.; Reeve, B.; Ader, D.; Fries, J.F.; Bruce, B.; Rose, M. The Patient-Reported Outcomes Measurement Information System (PROMIS). Med. Care 2007, 45, S3–S11. [Google Scholar] [CrossRef]
- Accounts Payable Association. DSM-5-TR Online Assessment Measures; American Psychiatric Association: Washington, DC, USA, 2022. [Google Scholar]
- Hinds, P.S.; Nuss, S.L.; Ruccione, K.S.; Withycombe, J.S.; Jacobs, S.; DeLuca, H.; Faulkner, C.; Liu, Y.; Cheng, Y.I.; Gross, H.E.; et al. PROMIS pediatric measures in pediatric oncology: Valid and clinically feasible indicators of patient-reported outcomes. Pediatr. Blood Cancer 2013, 60, 402–408. [Google Scholar] [CrossRef]
- IBM Corporation. IBM SPSS Statistics for Macintosh, Version 25.0; IBM Corp: Armonk, NY, USA, 2017. [Google Scholar]
- Perkins, N.J.; Cole, S.R.; Harel, O.; Tchetgen, E.J.T.; Sun, B.; Mitchell, E.M.; Schisterman, E.F. Principled Approaches to Missing Data in Epidemiologic Studies. Am. J. Epidemiol. 2018, 187, 568–575. [Google Scholar] [CrossRef]
- Jazieh, A.R.; Akbulut, H.; Curigliano, G.; Rogado, A.; Alsharm, A.A.; Razis, E.D.; Mula-Hussain, L.; Errihani, H.; Khattak, A.; De Guzman, R.B.; et al. Impact of the COVID-19 Pandemic on Cancer Care: A Global Collaborative Study. JCO Glob. Oncol. 2020, 6, 1428–1438. [Google Scholar] [CrossRef]
- Chen-See, S. Disruption of cancer care in Canada during COVID-19. Lancet Oncol. 2020, 21, e374. [Google Scholar] [CrossRef] [PubMed]
- Kenney, L.B.; Vrooman, L.M.; Lind, E.D.; Brace-O’Neill, J.; Mulder, J.E.; Nekhlyudov, L.; Recklitis, C.J. Virtual visits as long-term follow-up care for childhood cancer survivors: Patient and provider satisfaction during the COVID-19 pandemic. Pediatr. Blood Cancer 2021, 68, e28927. [Google Scholar] [CrossRef] [PubMed]
- Hare, N.; Bansal, P.; Bajowala, S.S.; Abramson, S.L.; Chervinskiy, S.; Corriel, R.; Hauswirth, D.W.; Kakumanu, S.; Mehta, R.; Rashid, Q.; et al. Work Group Report: COVID-19: Unmasking Telemedicine. J. Allergy Clin. Immunol. Pract. 2020, 8, 2461–2473.e3. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Duan, M.; Mao, X.; Ge, Y.; Wang, Y.; Huang, H. The effect of digital health technologies on managing symptoms across pediatric cancer continuum: A systematic review. Int. J. Nurs. Sci. 2021, 8, 22–29. [Google Scholar] [CrossRef]
- Holtz, B.E. Patients Perceptions of Telemedicine Visits Before and After the Coronavirus Disease 2019 Pandemic. Telemed. e-Health 2021, 27, 107–112. [Google Scholar] [CrossRef]
- Sansom-Daly, U.M.; Bradford, N. Grappling with the “human” problem hiding behind the technology: Telehealth during and beyond COVID-19. Psychooncology 2020, 29, 1404–1408. [Google Scholar] [CrossRef]
- Badawy, S.M.; Radovic, A. Digital Approaches to Remote Pediatric Health Care Delivery during the COVID-19 Pandemic: Existing Evidence and a Call for Further Research. JMIR Pediatr. Parent. 2020, 3, e20049. [Google Scholar] [CrossRef]
- Wakefield, C.E.; Fardell, J.E.; Doolan, E.L.; Aaronson, N.K.; Jacobsen, P.B.; Cohn, R.J.; King, M. Participation in psychosocial oncology and quality-of-life research: A systematic review. Lancet Oncol. 2017, 18, e153–e165. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Participant Demographics | n (%) | M (SD) | |
|---|---|---|---|
| Participants | |||
| Total N | 30 | ||
| Age (in years) | |||
| Current Age | 8.79 (5.10) | ||
| Age at Diagnosis | 7.23 (5.05) | ||
| Time since Diagnosis | 2.34 (2.27) | ||
| Sex | |||
| Male | 14 (46.7%) | ||
| Female | 16 (53.3%) | ||
| Ethnicity | |||
| White/European | 28 (93.3%) | ||
| Black/African/Caribbean | 2 (6.7%) | ||
| Latin American | 2 (6.7%) | ||
| East Asian | 1 (3.3%) | ||
| South Asian | 1 (3.3%) | ||
| Other | 1 (3.3%) | ||
| Parent’s Education | |||
| Some high school or less | 0 (0%) | ||
| High school | 2 (6.7%) | ||
| Vocational school or training other than college/university | 5 (16.7%) | ||
| Some university/college, no degree | 5 (16.7%) | ||
| University/college, Bachelors degree | 15 (50%) | ||
| Graduate/Professional degree | 3 (10%) | ||
| Household Income | |||
| Low income | 2 (6.7%) | ||
| Low/middle income | 6 (20%) | ||
| Middle income | 13 (43.3%) | ||
| Middle/high income | 4 (13.3%) | ||
| High income | 1 (3.3%) | ||
| Prefer not to answer | 4 (13.3%) | ||
| Has your household’s income changed because of the COVID-19 pandemic? | |||
| No | 14 (46.7) | ||
| Yes, my household income has decreased | 16 (53.3) | ||
| Yes, my household income has increased | 0 (0) | ||
| Has your family had difficulty accessing food or other necessities due to the COVID-19 pandemic? | |||
| No | 25 (83.3) | ||
| Yes | 5 (16.7) |
| Telemedicine Use | n (%) | |
|---|---|---|
| Did you or your child participate in a telemedicine appointment(s)? | ||
| No | 20 (69) | |
| Yes | 9 (31) | |
| Please rate your perception of the benefit of telemedicine | ||
| No benefit | 1 (11.1) | |
| Little benefit | 1 (11.1) | |
| Beneficial | 5 (55.6) | |
| Very beneficial | 2 (22.2) | |
| Did you feel the telemedicine meeting was as effective as a face-to-face meeting? | ||
| Not at all | 2 (22.2) | |
| Somewhat effective | 5 (55.6) | |
| Effective | 2 (22.2) | |
| Very effective, better than face-to-face | 0 (0) |
| Child and Parent Mental Health Status | n (%) |
|---|---|
| Is your child’s current mental health impacted by… | |
| Feelings of isolation from peers | 24 (80) |
| Fears/worries about their cancer and treatment | 15 (50) |
| Difficulties with remote learning | 12 (40) |
| Fears/worries about catching COVID-19 | 9 (30) |
| Fears/worries about the uncertainty related to the COVID-19 pandemic | 9 (30) |
| Fears/worries about the uncertainty related to how COVID-19 might impact them as a survivor of childhood cancer | 6 (20) |
| The media and messaging about the COVID-19 pandemic | 5 (16.7) |
| Not applicable, my child’s mental health has not been impacted by the COVID-19 pandemic | 3 (10) |
| Other | 3 (10) |
| Is your current mental health impacted by… | |
| Fears/worries about your child’s cancer and treatment | 26 (86.7) |
| Fears/worries about the uncertainty related to how COVID-19 might impact them as a child with cancer | 25 (83.3) |
| Fears/worries about catching COVID-19 | 22 (73.3) |
| Fears/worries about the uncertainty related to the COVID-19 pandemic | 22 (73.3) |
| Fears/worries about other factors in your life (i.e., boredom, feeling stuck at home) | 21 (70) |
| Feelings of isolation from peers | 19 (63.3) |
| Difficulties with remote learning | 11 (36.7) |
| The media and messaging about the COVID-19 pandemic | 8 (26.7) |
| Other | 5 (16.7) |
| Not applicable, my mental health has not been impacted by the COVID-19 pandemic | 0 (0) |
| Delayed, Modified, Cancelled Treatment | No Change to Treatment | 95% Confidence Interval | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | M (SD) | n | M (SD) | t-Test | df | p | Cohen’s d | LL | UL | |
| Child Anxiety | 10 | 61.33 (6.80) | 18 | 50.40 (12.26) | −3.04 | 25.99 | 0.005 | 1.02 | −18.33 | −3.53 |
| Child Depression | 10 | 61.55 (6.21) | 18 | 55.88 (12.83) | −1.57 | 25.72 | 0.128 | 0.52 | −13.09 | 1.74 |
| Parent Anxiety | 9 | 58.56 (6.71) | 18 | 61.26 (9.18) | 0.78 | 25 | 0.441 | 0.32 | −4.41 | 9.82 |
| Parent Depression | 9 | 53.21 (8.46) | 18 | 55.51 (10.44) | 0.57 | 25 | 0.572 | 0.23 | −5.98 | 10.58 |
| Telemedicine Is as Effective as Face-to-Face | Telemedicine Is not as Effective | 95% Confidence Interval | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | M (SD) | n | M (SD) | t-test | df | p | Cohen’s d | LL | UL | |
| Child Anxiety | 7 | 52.87 (12.36) | 2 | 74.35 (1.77) | 2.34 | 7 | 0.052 | 1.87 | −0.25 | 43.21 |
| Child Depression | 7 | 54.80 (8.46) | 2 | 75.85 (1.91) | 3.34 | 7 | 0.012 | 2.68 | 6.14 | 35.96 |
| Parent Anxiety | 7 | 57.63 (6.94) | 2 | 75.60 (3.25) | 3.43 | 7 | 0.011 | 2.75 | 5.58 | 30.37 |
| Parent Depression | 7 | 49.99 (8.83) | 2 | 69.35 (2.62) | 5.07 | 6.55 | 0.002 | 2.35 | 10.21 | 28.52 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tran, A.; Hou, S.H.J.; Forbes, C.; Cho, S.; Forster, V.J.; Stokoe, M.; Wakefield, C.E.; Wiener, L.; Heathcote, L.C.; Michel, G.; et al. The Impact of the Early COVID-19 Global Pandemic on Children Undergoing Active Cancer Treatment and Their Parents. Curr. Oncol. 2023, 30, 2441-2456. https://doi.org/10.3390/curroncol30020186
Tran A, Hou SHJ, Forbes C, Cho S, Forster VJ, Stokoe M, Wakefield CE, Wiener L, Heathcote LC, Michel G, et al. The Impact of the Early COVID-19 Global Pandemic on Children Undergoing Active Cancer Treatment and Their Parents. Current Oncology. 2023; 30(2):2441-2456. https://doi.org/10.3390/curroncol30020186
Chicago/Turabian StyleTran, Andrew, Sharon H. J. Hou, Caitlin Forbes, Sara Cho, Victoria J. Forster, Mehak Stokoe, Claire E. Wakefield, Lori Wiener, Lauren C. Heathcote, Gisela Michel, and et al. 2023. "The Impact of the Early COVID-19 Global Pandemic on Children Undergoing Active Cancer Treatment and Their Parents" Current Oncology 30, no. 2: 2441-2456. https://doi.org/10.3390/curroncol30020186
APA StyleTran, A., Hou, S. H. J., Forbes, C., Cho, S., Forster, V. J., Stokoe, M., Wakefield, C. E., Wiener, L., Heathcote, L. C., Michel, G., Patterson, P., Reynolds, K., & Schulte, F. S. M. (2023). The Impact of the Early COVID-19 Global Pandemic on Children Undergoing Active Cancer Treatment and Their Parents. Current Oncology, 30(2), 2441-2456. https://doi.org/10.3390/curroncol30020186