Adherence to Adjuvant Endocrine Therapy in Breast Cancer Patients

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Study Population
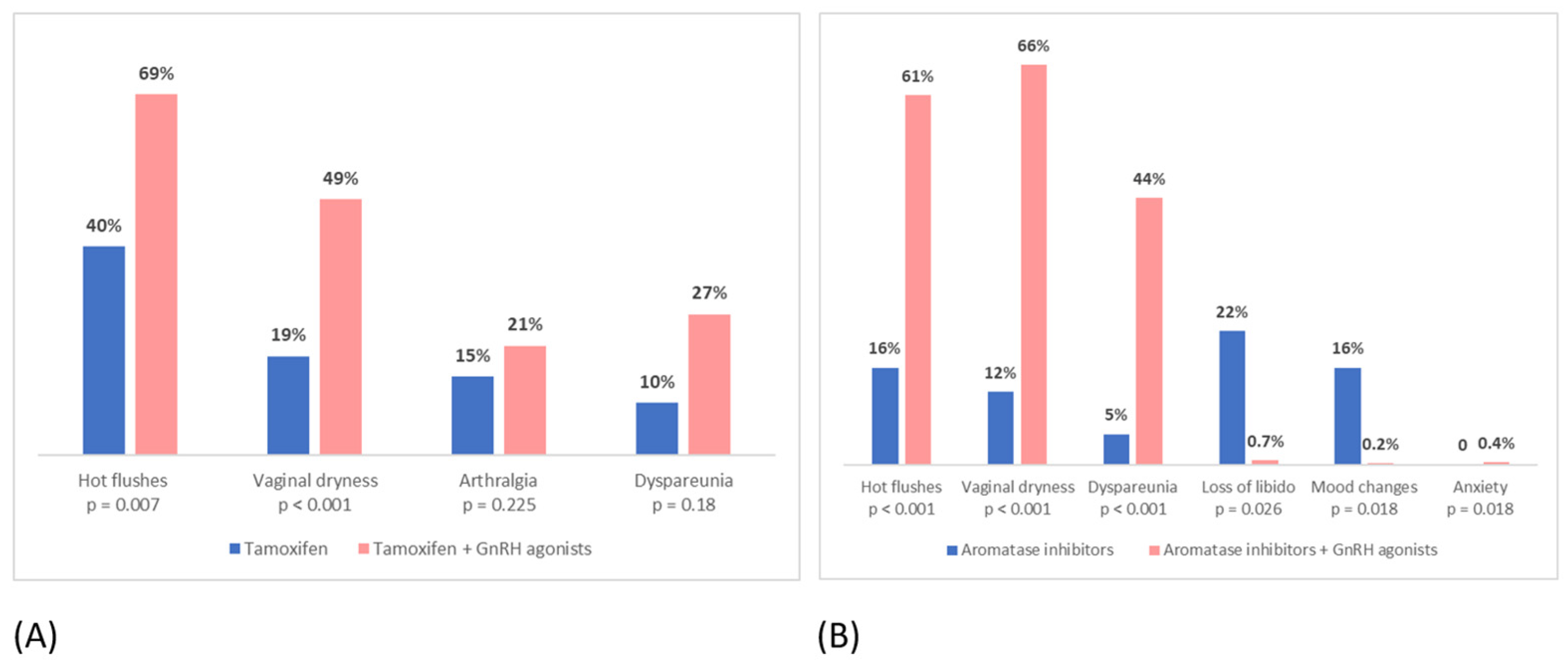
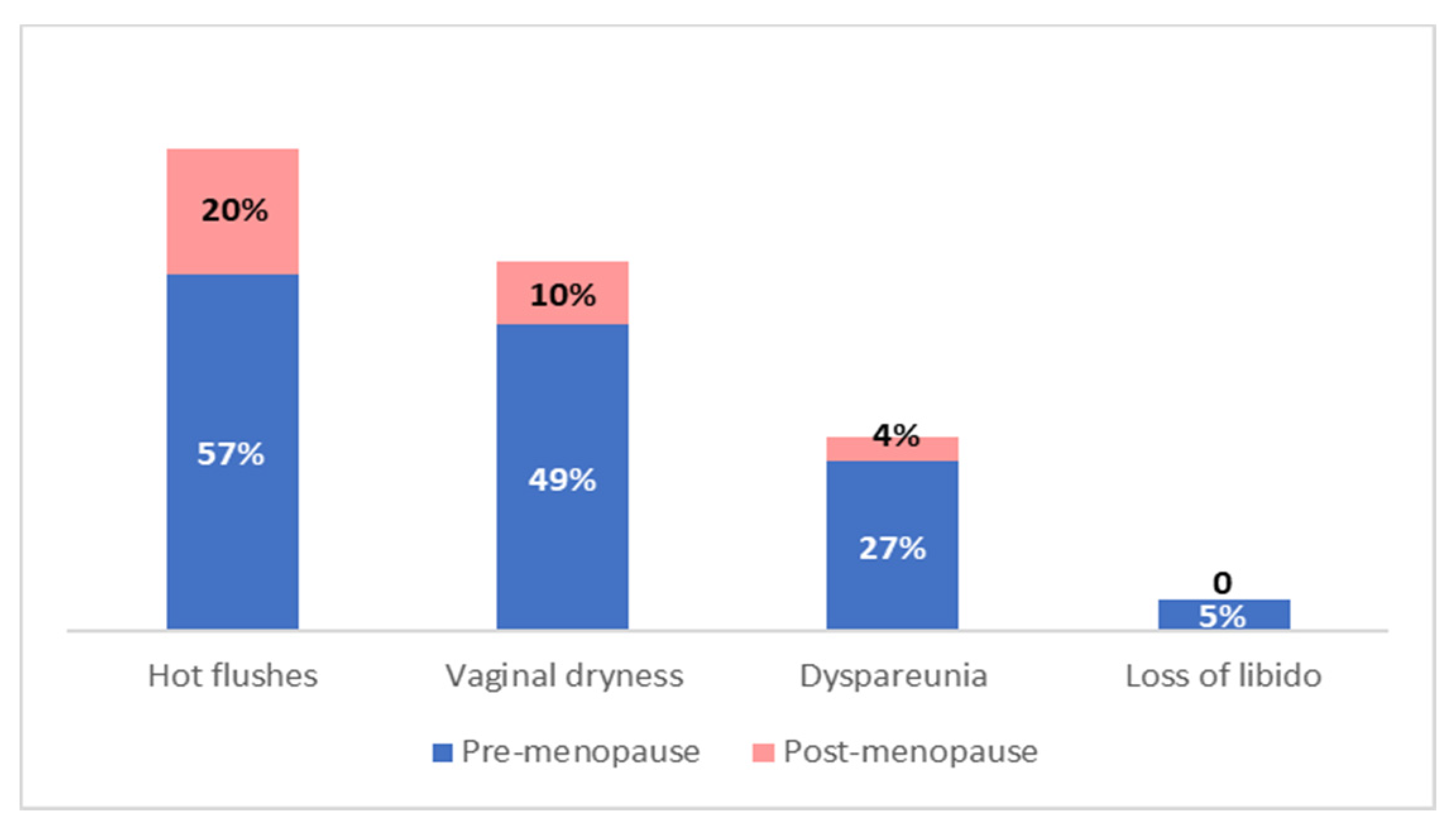
3.2. Incidence of Side Effects
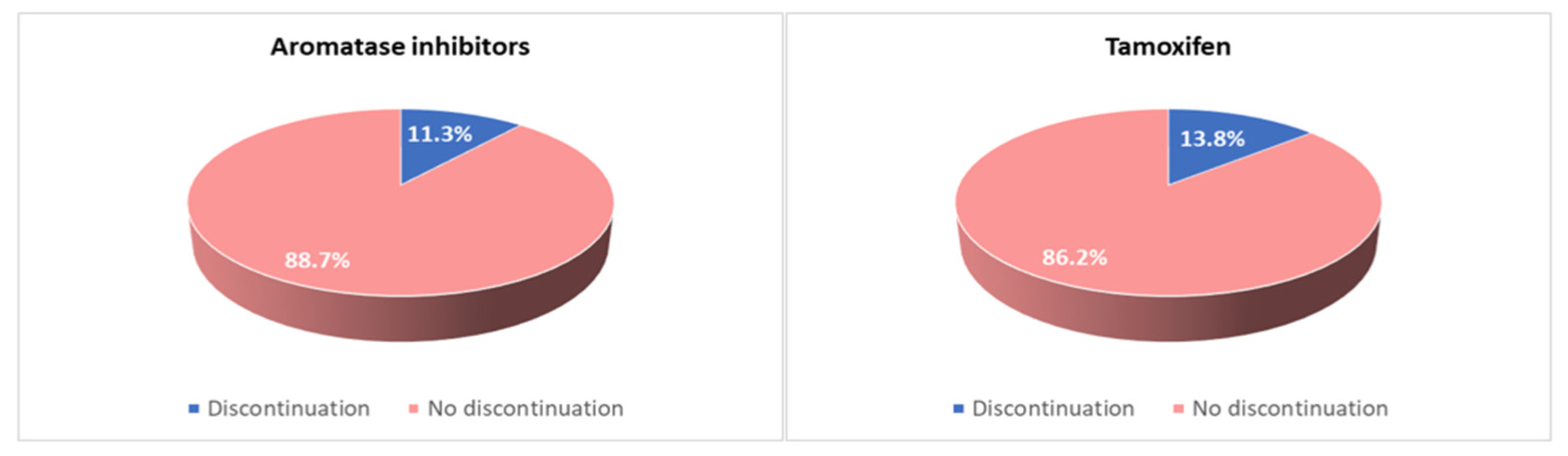
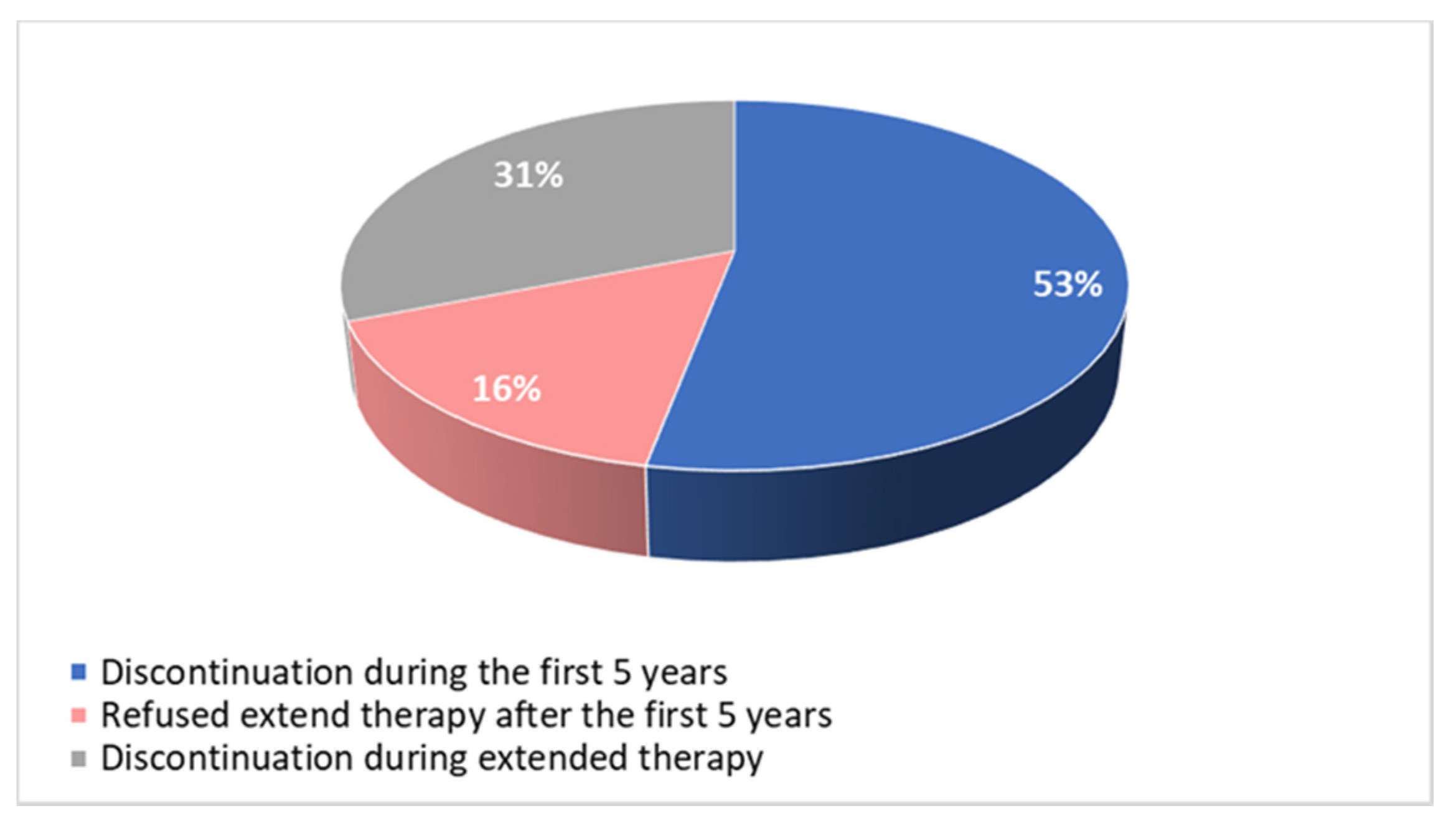
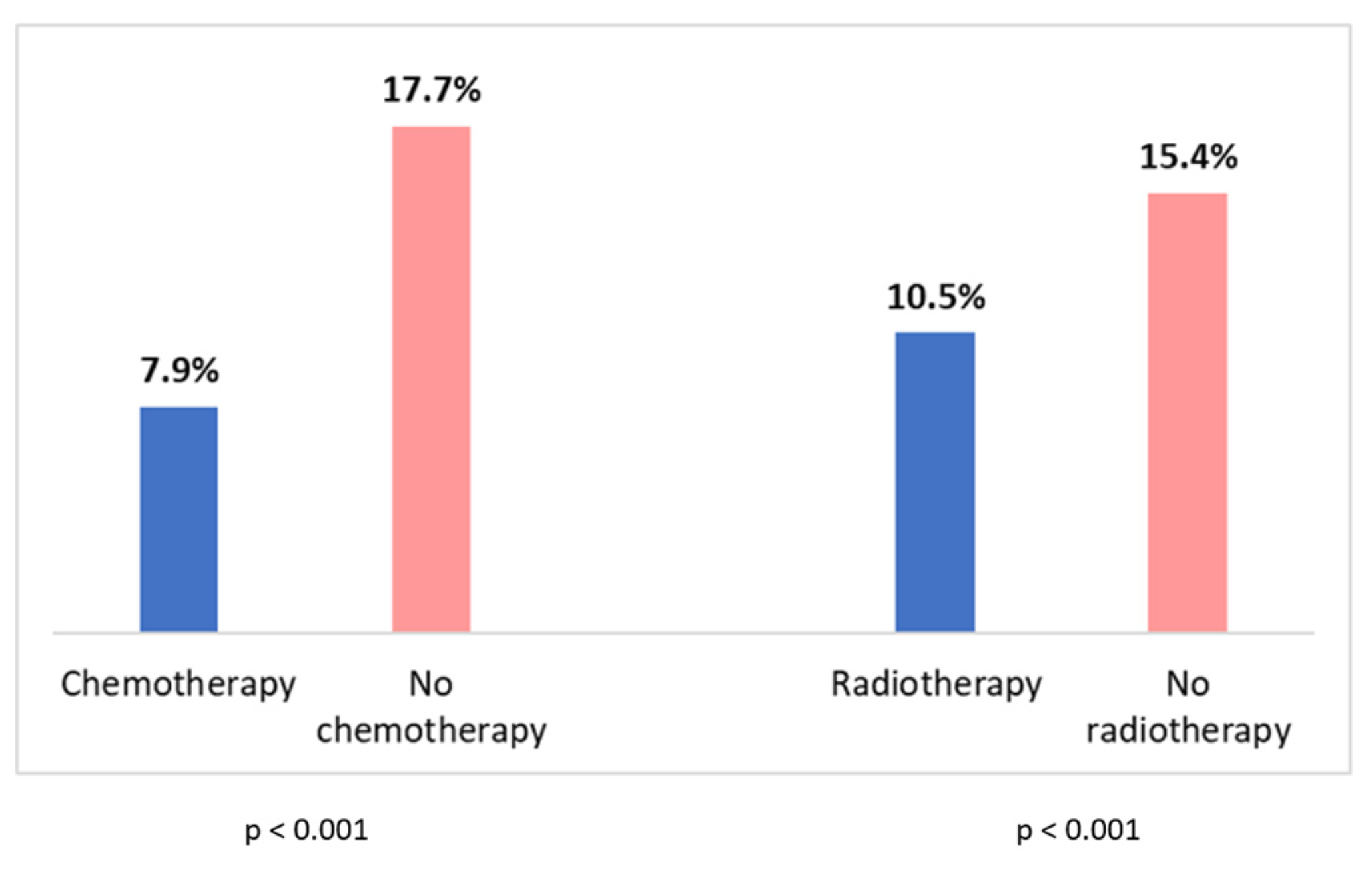
3.3. Adherence to Treatment and Discontinuation
3.4. Patient–Physician Communication and Support Strategies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Questionnaire
|
|
|
|
|
References
- Coates, A.S.; Keshaviah, A.; Thürlimann, B.; Mouridsen, H.; Mauriac, L.; Forbes, J.F.; Paridaens, R.; Castiglione-Gertsch, M.; Gelber, R.D.; Colleoni, M.; et al. Five years of letrozole compared with tamoxifen as initial adjuvant therapy for postmenopausal women with endocrine-responsive early breast cancer: Update of study BIG 1-98. J. Clin. Oncol. 2007, 25, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Forbes, J.F.; Cuzick, J.; Buzdar, A.; Howell, A.; Tobias, J.S.; Baum, M. ATAC/LATTE investigators. Effect of anastrozole and tamoxifen as adjuvant treatment for early-stage breast cancer: 100-month analysis of the ATAC trial. Lancet Oncol. 2008, 9, 45–53. [Google Scholar] [PubMed]
- Aiello Bowles, E.J.; Boudreau, D.M.; Chubak, J.B.; Yu, O.; Fujii, M.; Chestnut, J.; Buist, D.S. Patient-reported discontinuation of endocrine therapy and related adverse effects among women with early-stage breast cancer. J. Oncol. Pract. 2012, 8, e149–e157. [Google Scholar] [CrossRef] [PubMed]
- Pagani, O.; Francis, P.A.; Fleming, G.F.; Walley, B.A.; Viale, G.; Colleoni, M.; Láng, I.; Gómez, H.L.; Tondini, C.; Pinotti, G. SOFT and TEXT Investigators and International Breast Cancer Study Group. Absolute Improvements in Freedom from Distant Recurrence to Tailor Adjuvant Endocrine Therapies for Premenopausal Women: Results from TEXT and SOFT. J. Clin. Oncol. 2020, 38, 1293–1303. [Google Scholar] [CrossRef]
- Burstein, H.J.; Curigliano, G.; Loibl, S.; Dubsky, P.; Gnant, M.; Poortmans, P.; Colleoni, M.; Denkert, C.; Piccart-Gebhart, M.; Regan, M.; et al. Members of the St. Gallen International Consensus Panel on the Primary Therapy of Early Breast Cancer 2019. Estimating the benefits of therapy for early-stage breast cancer: The St. Gallen International Consensus Guidelines for the primary therapy of early breast cancer 2019. Ann. Oncol. 2019, 30, 1541–1557. [Google Scholar]
- Burstein, H.J.; Lacchetti, C.; Anderson, H.; Buchholz, T.A.; Davidson, N.E.; Gelmon, K.A.; Giordano, S.H.; Hudis, C.A.; Solky, A.J.; Stearns, V.; et al. Adjuvant Endocrine Therapy for Women with Hormone Receptor-Positive Breast Cancer: ASCO Clinical Practice Guideline Focused Update. J. Clin. Oncol. 2019, 37, 423–438. [Google Scholar] [CrossRef]
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Aromatase inhibitors versus tamoxifen in early breast cancer: Patient-level meta-analysis of the randomised trials. Lancet 2015, 386, 1341–1352. [Google Scholar] [CrossRef]
- Gray, R. Early Breast Cancer Trialists’ Collaborative Group. Abstract GS3-03: Effects of prolonging adjuvant aromatase inhibitor therapy beyond five years on recurrence and cause-specific mortality: An EBCTCG meta-analysis of individual patient data from 12 randomised trials including 24,912 women. Cancer Res 2019, 79 (Suppl. 4), GS3-03. [Google Scholar]
- Davies, C.; Pan, H.; Godwin, J.; Gray, R.; Arriagada, R.; Raina, V.; Abraham, M.; Medeiros Alencar, V.H.; Badran, A.; Bonfill, X.; et al. Adjuvant Tamoxifen: Longer Against Shorter (ATLAS) Collaborative Group. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet 2013, 381, 805–816. [Google Scholar] [CrossRef]
- Gray, R.; Rea, D.; Handley, K.; Bowden, S.J.; Perry, P.; Earl, H.M.; Poole, C.J.; Bates, T.; Chetiyawardana, S.; Dewar, J.A.; et al. aTTom Collaborative Group. aTTom: Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years in 6,953 women with early breast cancer. J. Clin. Oncol. 2013, 31 (Suppl. 18), 5. [Google Scholar] [CrossRef]
- Goss, P.E.; Ingle, J.N.; Pritchard, K.I.; Robert, N.J.; Muss, H.; Gralow, J.; Gelmon, K.; Whelan, T.; Strasser-Weippl, K.; Rubin, S.; et al. Extending Aromatase-Inhibitor Adjuvant Therapy to 10 Years. N. Engl. J. Med. 2016, 375, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Tjan-Heijnen, V.C.G.; van Hellemond, I.E.G.; Peer, P.G.M.; Swinkels, A.C.P.; Smorenburg, C.H.; van der Sangen, M.J.C.; Kroep, J.R.; De Graaf, H.; Honkoop, A.H.; Erdkamp, F.L.G.; et al. Dutch Breast Cancer Research Group (BOOG) for the DATA Investigators. Extended adjuvant aromatase inhibition after sequential endocrine therapy (DATA): A randomised, phase 3 trial. Lancet Oncol. 2017, 18, 1502–1511. [Google Scholar] [CrossRef] [PubMed]
- Blok, E.J.; Kroep, J.R.; Meershoek-Klein Kranenbarg, E.; Duijm-de Carpentier, M.; Putter, H.; van den Bosch, J.; Maartense, E.; van Leeuwen-Stok, A.E.; Liefers, G.J.; Nortier, J.W.R.; et al. IDEAL Study Group. Optimal Duration of Extended Adjuvant Endocrine Therapy for Early Breast Cancer; Results of the IDEAL Trial (BOOG 2006-05). J. Natl. Cancer Inst. 2018, 110, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Mamounas, E.P.; Bandos, H.; Lembersky, B.C.; Jeong, J.H.; Geyer, C.E., Jr.; Rastogi, P.; Fehrenbacher, L.; Graham, M.L.; Chia, S.K.; Brufsky, A.M.; et al. Use of letrozole after aromatase inhibitor-based therapy in postmenopausal breast cancer (NRG Oncology/NSABP B-42): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 88–99. [Google Scholar] [CrossRef] [PubMed]
- Garreau, J.R.; Delamelena, T.; Walts, D.; Karamlou, K.; Johnson, N. Side effects of aromatase inhibitors versus tamoxifen: The patients’ perspective. Am. J. Surg. 2006, 192, 496–498. [Google Scholar] [CrossRef]
- Awan, A.; Esfahani, K. Endocrine therapy for breast cancer in the primary care setting. Curr. Oncol. 2018, 25, 285–291. [Google Scholar] [CrossRef]
- Harrow, A.; Dryden, R.; McCowan, C.; Radley, A.; Parsons, M.; Thompson, A.M.; Wells, M. A hard pill to swallow: A qualitative study of women’s experiences of adjuvant endocrine therapy for breast cancer. BMJ Open 2014, 4, e005285. [Google Scholar] [CrossRef]
- Brett, J.; Fenlon, D.; Boulton, M.; Hulbert-Williams, N.J.; Walter, F.M.; Donnelly, P.; Lavery, B.; Morgan, A.; Morris, C.; Watson, E. Factors associated with intentional and unintentional non-adherence to adjuvant endocrine therapy following breast cancer. Eur. J. Cancer Care 2018, 27, e12601. [Google Scholar] [CrossRef]
- Cluze, C.; Rey, D.; Huiart, L.; Ben Diane, M.K.; Bouhnik, A.D.; Berenger, C.; Carrieri, M.P.; Giorgi, R. Adjuvant endocrine therapy with tamoxifen in young women with breast cancer: Determinants of interruptions vary over time. Ann. Oncol. 2012, 23, 882–890. [Google Scholar] [CrossRef]
- Freedman, R.A.; Revette, A.C.; Hershman, D.L.; Silva, K.; Sporn, N.J.; Gagne, J.J.; Kouri, E.M.; Keating, N.L. Understanding Breast Cancer Knowledge and Barriers to Treatment Adherence: A Qualitative Study Among Breast Cancer Survivors. Biores. Open Access 2017, 6, 159–168. [Google Scholar] [CrossRef]
- Murphy, C.C.; Bartholomew, L.K.; Carpentier, M.Y.; Bluethmann, S.M.; Vernon, S.W. Adherence to adjuvant hormonal therapy among breast cancer survivors in clinical practice: A systematic review. Breast Cancer Res. Treat. 2012, 134, 459–478. [Google Scholar] [CrossRef] [PubMed]
- Peddie, N.; Agnew, S.; Crawford, M.; Dixon, D.; MacPherson, I.; Fleming, L. The impact of medication side effects on adherence and persistence to hormone therapy in breast cancer survivors: A qualitative systematic review and thematic synthesis. Breast 2021, 58, 147–159. [Google Scholar] [CrossRef] [PubMed]
- Hadji, P.; Ziller, V.; Kyvernitakis, J.; Bauer, M.; Haas, G.; Schmidt, N.; Kostev, K. Persistence in patients with breast cancer treated with tamoxifen or aromatase inhibitors: A retrospective database analysis. Breast Cancer Res. Treat. 2013, 138, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Davies, S.; Voutsadakis, I.A. Adherence to adjuvant hormonal therapy in localised breast cancer. Eur. J. Cancer Care 2022, e13729. [Google Scholar] [CrossRef] [PubMed]
- Hershman, D.L.; Shao, T.; Kushi, L.H.; Buono, D.; Tsai, W.Y.; Fehrenbacher, L.; Kwan, M.; Gomez, S.L.; Neugut, A.I. Early discontinuation and non-adherence to adjuvant hormonal therapy are associated with increased mortality in women with breast cancer. Breast Cancer Res. Treat. 2011, 126, 529–537. [Google Scholar] [CrossRef] [PubMed]
- McCowan, C.; Shearer, J.; Donnan, P.T.; Dewar, J.A.; Crilly, M.; Thompson, A.M.; Fahey, T.P. Cohort study examining tamoxifen adherence and its relationship to mortality in women with breast cancer. Br. J. Cancer 2008, 99, 1763–1768. [Google Scholar] [CrossRef] [PubMed]
- Chalela, P.; Munoz, E.; Inupakutika, D.; Kaghyan, S.; Akopian, D.; Kaklamani, V.; Lathrop, K.; Ramirez, A. Improving adherence to endocrine hormonal therapy among breast cancer patients: Study protocol for a randomized controlled trial. Contemp. Clin. Trials Commun. 2018, 12, 109–115. [Google Scholar] [CrossRef]
- Bright, E.E.; Petrie, K.J.; Partridge, A.H.; Stanton, A.L. Barriers to and facilitative processes of endocrine therapy adherence among women with breast cancer. Breast Cancer Res. Treat. 2016, 158, 243–251. [Google Scholar] [CrossRef]
- Liu, Y.; Malin, J.L.; Diamant, A.L.; Thind, A.; Maly, R.C. Adherence to adjuvant hormone therapy in low-income women with breast cancer: The role of provider-patient communication. Breast Cancer Res. Treat. 2013, 137, 829–836. [Google Scholar] [CrossRef]
- Stanton, A.L.; Petrie, K.J.; Partridge, A.H. Contributors to nonadherence and nonpersistence with endocrine therapy in breast cancer survivors recruited from an online research registry. Breast Cancer Res. Treat. 2014, 145, 525–534. [Google Scholar] [CrossRef]
- Cahir, C.; Dombrowski, S.U.; Kelly, C.M.; Kennedy, M.J.; Bennett, K.; Sharp, L. Women’s experiences of hormonal therapy for breast cancer: Exploring influences on medication-taking behaviour. Support Care Cancer 2015, 23, 3115–3130. [Google Scholar] [CrossRef] [PubMed]
- Piette, J.D.; Heisler, M.; Krein, S.; Kerr, E.A. The role of patient-physician trust in moderating medication nonadherence due to cost pressures. Arch. Intern. Med. 2005, 165, 1749–1755. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, I.; Sarradon-Eck, A.; Soussan, P.B.; Lacour, A.C.; Largillier, R.; Tallet, A.; Tarpin, C.; Julian-Reynier, C. Women’s perceptions and experience of adjuvant tamoxifen therapy account for their adherence: Breast cancer patients’ point of view. Psychooncology 2010, 19, 472–479. [Google Scholar] [CrossRef]
- Kirk, M.C.; Hudis, C.A. Insight into barriers against optimal adherence to oral hormonal therapy in women with breast cancer. Clin. Breast Cancer 2008, 8, 155–161. [Google Scholar] [CrossRef]
- Constanze, E.; Uwe, G.; Christoph, T.; Kavitha, D.; Dominik, R.; Urte, S.; Walter, B. The role of trust in the acceptance of adjuvant endocrine therapy in breast cancer patients. Psychooncology 2022, 31, 2122–2131. [Google Scholar] [CrossRef] [PubMed]
- Toivonen, K.I.; Williamson, T.M.; Carlson, L.E.; Walker, L.M.; Campbell, T.S. Potentially Modifiable Factors Associated with Adherence to Adjuvant Endocrine Therapy among Breast Cancer Survivors: A Systematic Review. Cancers 2020, 13, 107. [Google Scholar] [CrossRef] [PubMed]
- Mouridsen, H.T. Incidence and management of side effects associated with aromatase inhibitors in the adjuvant treatment of breast cancer in postmenopausal women. Curr. Med. Res. Opin. 2006, 22, 1609–1621. [Google Scholar] [CrossRef]
- Jones, S.E.; Cantrell, J.; Vukelja, S.; Pippen, J.; O’Shaughnessy, J.; Blum, J.L.; Brooks, R.; Hartung, N.L.; Negron, A.G.; Richards, D.A.; et al. Comparison of menopausal symptoms during the first year of adjuvant therapy with either exemestane or tamoxifen in early breast cancer: Report of a Tamoxifen Exemestane Adjuvant Multicenter trial substudy. J. Clin. Oncol. 2007, 25, 4765–4771. [Google Scholar] [CrossRef]
- Coombes, R.C.; Kilburn, L.S.; Snowdon, C.F.; Paridaens, R.; Coleman, R.E.; Jones, S.E.; Jassem, J.; Van de Velde, C.J.; Delozier, T.; Alvarez, I.; et al. Intergroup Exemestane Study. Survival and safety of exemestane versus tamoxifen after 2-3 years’ tamoxifen treatment (Intergroup Exemestane Study): A randomised controlled trial. Lancet 2007, 369, 559–570. [Google Scholar] [CrossRef]
- Antoine, C.; Vandromme, J.; Fastrez, M.; Carly, B.; Liebens, F.; Rozenberg, S. A survey among breast cancer survivors: Treatment of the climacteric after breast cancer. Climacteric 2008, 11, 322–328. [Google Scholar] [CrossRef]
- Fenlon, D.; Morgan, A.; Khambaita, P.; Carly, B.; Liebens, F.; Rozenberg, S. NCRI CSG Breast Cancer Symptom Working Party. Management of hot flushes in UK breast cancer patients: Clinician and patient perspectives. J. Psychosom. Obstet. Gynaecol. 2017, 38, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Francis, P.A.; Regan, M.M.; Fleming, G.F.; Láng, I.; Ciruelos, E.; Bellet, M.; Bonnefoi, H.R.; Climent, M.A.; Da Prada, G.A.; Burstein, H.J. SOFT Investigators; International Breast Cancer Study Group. Adjuvant ovarian suppression in premenopausal breast cancer. N. Engl. J. Med. 2015, 372, 436–446. [Google Scholar] [CrossRef]
- Verbrugghe, M.; Verhaeghe, S.; Lauwaert, K.; Beeckman, D.; Van Hecke, A. Determinants and associated factors influencing medication adherence and persistence to oral anticancer drugs: A systematic review. Cancer Treat. Rev. 2013, 39, 610–621. [Google Scholar] [CrossRef] [PubMed]
- Chlebowski, R.T.; Kim, J.; Haque, R. Adherence to endocrine therapy in breast cancer adjuvant and prevention settings. Cancer Prev. Res. 2014, 7, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Hagen, K.B.; Aas, T.; Kvaløy, J.T.; Søiland, H.; Lind, R. Adherence to adjuvant endocrine therapy in postmenopausal breast cancer patients: A 5-year prospective study. Breast 2019, 44, 52–58. [Google Scholar] [CrossRef]
- Fink, A.K.; Gurwitz, J.; Rakowski, W.; Guadagnoli, E.; Silliman, R.A. Patient beliefs and tamoxifen discontinuance in older women with estrogen receptor--positive breast cancer. J. Clin. Oncol. 2004, 22, 3309–3315. [Google Scholar] [CrossRef]
- Horne, R.; Weinman, J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J. Psychosom. Res. 1999, 47, 555–567. [Google Scholar] [CrossRef] [PubMed]
- Hershman, D.L.; Kushi, L.H.; Shao, T.; Buono, D.; Kershenbaum, A.; Tsai, W.Y.; Fehrenbacher, L.; Gomez, S.L.; Miles, S.; Neugut, A.I. Early discontinuation and nonadherence to adjuvant hormonal therapy in a cohort of 8769 early-stage breast cancer patients. J. Clin. Oncol. 2010, 28, 4120–4128. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n = 373 | |
|---|---|
| Mean age (years) | 66.5 (33–90) |
| Mean age at surgery (years) | 59.9 (28–86) |
| Menopausal state at surgery | |
| Premenopausal | 134 (36%) |
| Postmenopausal | 239 (64%) |
| Type of AET at time of administration of questionnaire | |
| Tamoxifen | 81 (21.7%) |
| Aromatase inhibitors | 292 (78.3%) |
| Association with GnRH-agonists | |
| Yes | 73 (19.6%) |
| with tamoxifen | 55 (75%) |
| with AI | 18 (25%) |
| No | 300 (80.4%) |
| Extended therapy | |
| Yes | 79 (21%) |
| No | 294 (79%) |
| Chemotherapy | |
| Yes | 158 (42.4%) |
| No | 215 (57.6%) |
| Radiotherapy | |
| Yes | 256 (68.6%) |
| No | 117 (31.4%) |
| Side Effects | Overall | Tamoxifen | Aromatase Inhibitors |
|---|---|---|---|
| 303 (81%) | n = 81 (84%) | n = 235 (80%) | |
| Arthralgia | 200 (53.6%) | 26 (32.1%) | 177 (60.6%) |
| Hot flushes | 123 (33%) | 45 (55.6%) | 57 (19.5%) |
| Vaginal dryness | 85 (23%) | 21 (25.9%) | 45 (15.4%) |
| Hypercholesterolemia | 70 (18.7%) | 3 (3.7%) | 67 (22.9%) |
| Dyspareunia | 45 (12%) | 9 (11.1%) | 23 (7.9%) |
| Asthenia | 43 (11.5%) | 7 (8.6%) | 41 /14%) |
| Alopecia | 33 (8.8%) | 3 (3.7%) | 28 (9.6%) |
| Weight gain | 16 (4.2%) | 7 (8.6%) | 9 (3.2%) |
| CNS alterations | 14 (3.7%) | 3 (3.7%) | 9 (3.1%) |
| Insomnia | 14 (3.7%) | 3 (3.7%) | 10 (3.4%) |
| Itch | 14 (3.7%) | 3 (3.7%) | 10 (3.4%) |
| Mood changes | 11 (2.9%) | 2 (2.5%) | 8 (2.7%) |
| Liver function abnormalities | 10 (2.9%) | 4 (4.9%) | 7 (2.4%) |
| Headache | 10 (2.9%) | 3 (3.7%) | 5 (1.7%) |
| Decreased libido | 9 (2.4%) | 1 (1.2%) | 5 (1.7%) |
| Dry skin | 6 (1.6%) | 2 (2.5%) | 3 (1%) |
| Thromboembolism | 5 (1.3%) | 4 (4.9%) | 1 (0.3%) |
| Anxiety | 5 (1.3%) | 3 (3.7%) | 2 (0.6%) |
| Dizziness | 4 (1.1%) | 0 (0.0%) | 3 (1%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosso, R.; D’Alonzo, M.; Bounous, V.E.; Actis, S.; Cipullo, I.; Salerno, E.; Biglia, N. Adherence to Adjuvant Endocrine Therapy in Breast Cancer Patients. Curr. Oncol. 2023, 30, 1461-1472. https://doi.org/10.3390/curroncol30020112
Rosso R, D’Alonzo M, Bounous VE, Actis S, Cipullo I, Salerno E, Biglia N. Adherence to Adjuvant Endocrine Therapy in Breast Cancer Patients. Current Oncology. 2023; 30(2):1461-1472. https://doi.org/10.3390/curroncol30020112
Chicago/Turabian StyleRosso, Roberta, Marta D’Alonzo, Valentina Elisabetta Bounous, Silvia Actis, Isabella Cipullo, Elena Salerno, and Nicoletta Biglia. 2023. "Adherence to Adjuvant Endocrine Therapy in Breast Cancer Patients" Current Oncology 30, no. 2: 1461-1472. https://doi.org/10.3390/curroncol30020112
APA StyleRosso, R., D’Alonzo, M., Bounous, V. E., Actis, S., Cipullo, I., Salerno, E., & Biglia, N. (2023). Adherence to Adjuvant Endocrine Therapy in Breast Cancer Patients. Current Oncology, 30(2), 1461-1472. https://doi.org/10.3390/curroncol30020112