Breast Volume Is a Predictor of Higher Heart Dose in Whole-Breast Supine Free-Breathing Volumetric-Modulated Arc Therapy Planning

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Simulation and Target Definition
2.3. Treatment Planning
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Correlation Analysis
3.3. Regression Analysis
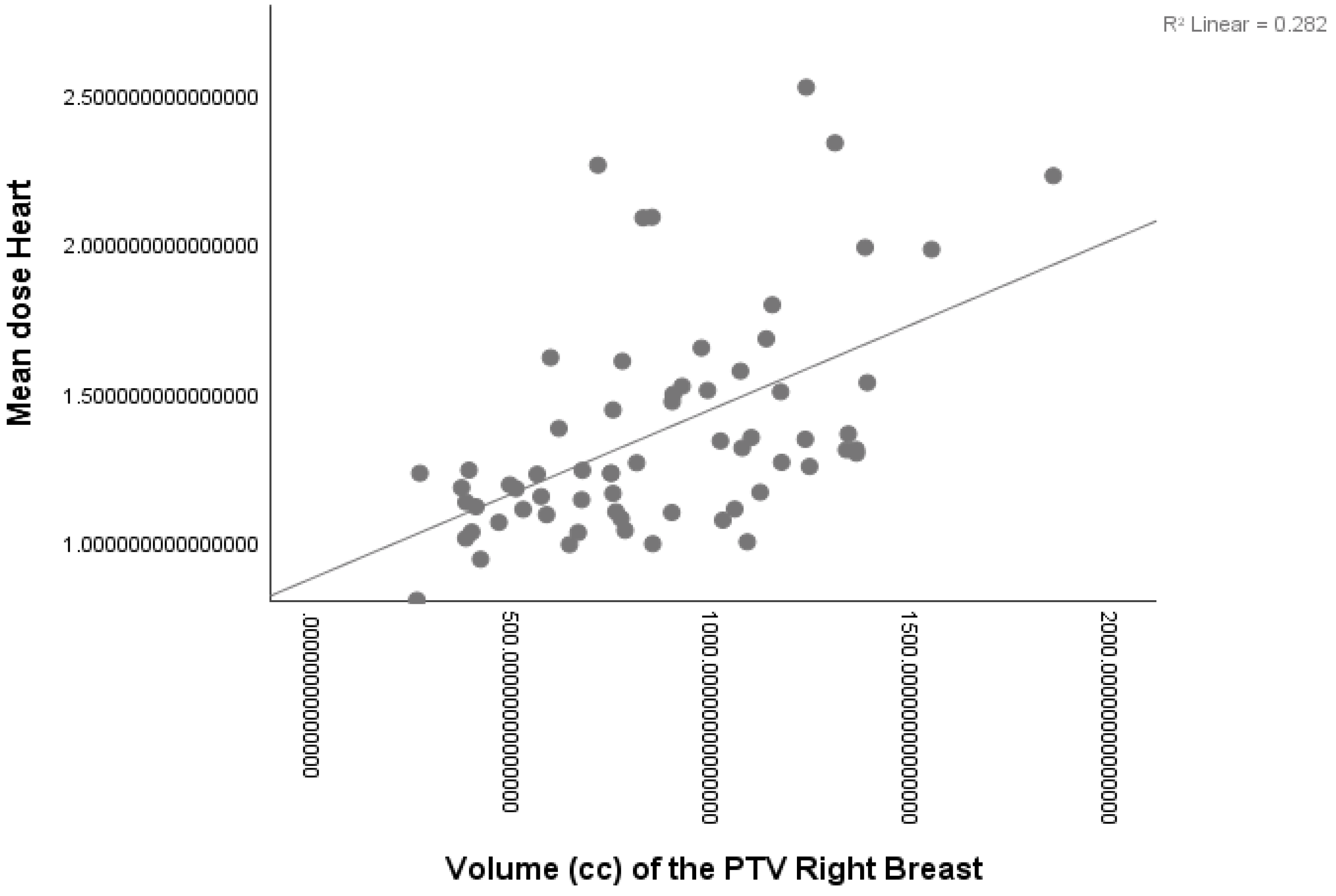
3.3.1. Right-Sided Patients
- (a)
- mHD (Gy) =0.881 + (0.531 × breast volume)
- (b)
- mLAD (Gy) = 0.860 + (0.443 × breast volume)
- (c)
- MLAD (Gy) =1.100 + (0.323 × breast volume)
3.3.2. Left-Sided Patients
- (a)
- mHD (Gy) = 1.705 + (0.208 × breast volume) + (0.312 × heart volume) − (0.411 × lung volume)
- (b)
- mLAD dose (Gy) = 6.528 + (0.281 × heart volume) − (0.565 × lung volume)
- (a)
- MLAD dose (Gy) = 22.812 − (0.639 × lung volume)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG); Darby, S.; McGale, P.; Correa, C.; Taylor, C.; Arriagada, R.; Clarke, M.; Cutter, D.; Davies, C.; Ewertz, M.; et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: Meta-analysis of individual patient data for 10,801 women in 17 randomized trials. Lancet 2011, 378, 1707–1716. [Google Scholar] [CrossRef] [PubMed]
- Yeboa, D.N.; Evans, S.B. Contemporary Breast Radiotherapy and Cardiac Toxicity. Semin. Radiat. Oncol. 2016, 26, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Darby, S.C.; Ewertz, M.; McGale, P.; Bennet, A.M.; Blom-Goldman, U.; Brønnum, D.; Correa, C.; Cutter, D.; Gagliardi, G.; Gigante, B.; et al. Risk of Ischemic Heart Disease in Women after Radiotherapy for Breast Cancer. N. Engl. J. Med. 2013, 368, 987–998. [Google Scholar] [CrossRef] [PubMed]
- Clarke, M.; Collins, R.; Darby, S.; Davies, C.; Elphinstone, P.; Evans, V.; Godwin, J.; Gray, R.; Hicks, C.; James, S.; et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: An overview of the randomized trials. Lancet 2005, 366, 2087–2106. [Google Scholar] [CrossRef] [PubMed]
- Dell’Oro, M.; Giles, E.; Sharkey, A.; Borg, M.; Connell, C.; Bezak, E. A Retrospective Dosimetric Study of Radiotherapy Patients with Left-Sided Breast Cancer; Patient Selection Criteria for Deep Inspiration Breath Hold Technique. Cancers 2019, 11, 259. [Google Scholar] [CrossRef] [PubMed]
- Xin, X.; Li, J.; Zhao, Y.; Wang, P.; Tang, B.; Yao, X.; Liao, X.; Ma, J.; Orlandini, L.C. Retrospective Study on Left-Sided Breast Radiotherapy: Dosimetric Results and Correlation with Physical Factors for Free Breathing and Breath Hold Irradiation Techniques. Technol. Cancer Res. Treat. 2021, 20, 15330338211062429. [Google Scholar] [CrossRef]
- Cao, N.; Kalet, A.M.; Young, L.A.; Fang, L.C.; Kim, J.N.; Mayr, N.A.; Meyer, J. Predictors of cardiac and lung dose sparing in DIBH for left breast treatment. Phys. Med. 2019, 67, 27–33. [Google Scholar] [CrossRef]
- Rochet, N.; Drake, J.I.; Harrington, K.; Wolfgang, J.A.; Napolitano, B.; Sadek, B.T.; Shenouda, M.N.; Keruakous, A.R.; Niemierko, A.; Taghian, A.G. Deep inspiration breath-hold technique in left-sided breast cancer radiation therapy: Evaluating cardiac contact distance as a predictor of cardiac exposure for patient selection. Pract. Radiat. Oncol. 2015, 5, e127–e134. [Google Scholar] [CrossRef]
- Ferini, G.; Molino, L.; Tripoli, A.; Valenti, V.; Illari, S.I.; Marchese, V.A.; Cravagno, I.R.; Borzi, G.R. Anatomical Predictors of Dosimetric Advantages for Deep-inspiration-breath-hold 3D-conformal Radiotherapy Among Women with Left Breast Cancer. Anticancer Res. 2021, 41, 1529–1538. [Google Scholar] [CrossRef]
- Koide, Y.; Shimizu, H.; Aoyama, T.; Kitagawa, T.; Miyauchi, R.; Watanabe, Y.; Tachibana, H.; Kodaira, T. Preoperative spirometry and BMI in deep inspiration breath-hold radiotherapy: The early detection of cardiac and lung dose predictors without radiation exposure. Radiat. Oncol. 2022, 17, 35. [Google Scholar] [CrossRef]
- Otto, K. Volumetric modulated arc therapy: IMRT in a single gantry arc. Med. Phys. 2008, 35, 310–317. [Google Scholar] [CrossRef]
- Ma, C.; Zhang, W.; Lu, J.; Wu, L.; Wu, F.; Huang, B.; Lin, Y.; Li, D. Dosimetric comparison and evaluation of three radiotherapy techniques for use after modified radical mastectomy for locally advanced left-sided breast cancer. Sci. Rep. 2015, 5, 12274. [Google Scholar] [CrossRef] [PubMed]
- Offersen, B.V.; Boersma, L.J.; Kirkove, C.; Hol, S.; Aznar, M.C.; Biete Sola, A.; Kirova, Y.M.; Pignol, J.P.; Remouchamps, V.; Verhoeven, K.; et al. ESTRO consensus guideline on target volume delineation for elective radiation therapy of early stage breast cancer. Radiother. Oncol. 2015, 114, 3–10. [Google Scholar] [CrossRef]
- Feng, M.; Moran, J.M.; Koelling, T.; Chughtai, A.; Chan, J.L.; Freedman, L.; Hayman, J.A.; Jagsi, R.; Jolly, S.; Larouere, J.; et al. Development and validation of a heart atlas to study cardiac exposure to radiation following treatment for breast cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Piroth, M.D.; Baumann, R.; Budach, W.; Dunst, J.; Feyer, P.; Fietkau, R.; Haase, W.; Harms, W.; Hehr, T.; Krug, D.; et al. Heart toxicity from breast cancer radiotherapy: Current findings, assessment, and prevention. Strahlenther. Onkol. 2019, 195, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Pierce, L.J.; Feng, M.; Griffith, K.A.; Jagsi, R.; Boike, T.; Dryden, D.; Gustafson, G.S.; Benedetti, L.; Matuszak, M.M.; Nurushev, T.S.; et al. Recent Time Trends and Predictors of Heart Dose From Breast Radiation Therapy in a Large Quality Consortium of Radiation Oncology Practices. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 1154–1161. [Google Scholar] [CrossRef] [PubMed]
- Kang, Z.; Chen, S.; Shi, L.; He, Y.; Gao, X. Predictors of heart and lung dose in left-sided breast cancer treated with VMAT relative to 3D-CRT: A retrospective study. PLoS ONE 2021, 16, e0252552. [Google Scholar] [CrossRef]
- Duma, M.N.; Baumann, R.; Budach, W.; Dunst, J.; Feyer, P.; Fietkau, R.; Haase, W.; Harms, W.; Hehr, T.; Krug, D.; et al. Heart-sparing radiotherapy techniques in breast cancer patients: A recommendation of the breast cancer expert panel of the German society of radiation oncology (DEGRO). Strahlenther. Onkol. 2019, 195, 861–871. (In English) [Google Scholar] [CrossRef]
- Al-Hammadi, N.; Caparrotti, P.; Naim, C.; Hayes, J.; Benson, K.R.; Vasic, A.; Al-Abdulla, H.; Hammoud, R.; Divakar, S.; Petric, P. Voluntary Deep Inspiration Breath-hold Reduces the Heart Dose without Compromising the Target Volume Coverage during Radiotherapy for Left-Sided Breast Cancer. Radiol. Oncol. 2018, 52, 112–120. [Google Scholar] [CrossRef]
- Kügele, M.; Edvardsson, A.; Berg, L.; Alkner, S.; Ljus, C.A.; Ceberg, S. Dosimetric effects of intrafractional isocenter variation during deep inspiration breath-hold for breast cancer patients using surface-guided radiotherapy. J. Appl. Clin. Med. Phys. 2018, 19, 25–38. [Google Scholar] [CrossRef]
- Koivumäki, T.; Fogliata, A.; Zeverino, M.; Boman, E.; Sierpowska, J.; Moeckli, R.; Vallet, V.; Cozzi, L.; Heikkilä, J.; Väänänen, A.; et al. Dosimetric evaluation of modern radiation therapy techniques for left breast in deep-inspiration breath-hold. Phys. Med. 2018, 45, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Simonetto, C.; Eidemüller, M.; Gaasch, A.; Pazos, M.; Schönecker, S.; Reitz, D.; Kääb, S.; Braun, M.; Harbeck, N.; Niyazi, M.; et al. Does deep inspiration breath-hold prolong life? Individual risk estimates of ischaemic heart disease after breast cancer radiotherapy. Radiother. Oncol. 2019, 131, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Pandeli, C.; Smyth, L.M.L.; David, S.; See, A.W. Dose reduction to organs at risk with deep-inspiration breath-hold during right breast radiotherapy: A treatment planning study. Radiat. Oncol. 2019, 14, 223. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.; Luo, Z.; Hu, H.; Jiang, L.; Wu, J.; Lei, L.; Qu, L.; Wu, Z. SGRT-based DIBH radiotherapy practice for right-sided breast cancer combined with RNI: A retrospective study on dosimetry and setup accuracy. J. Appl. Clin. Med. Phys. 2023, 24, e13998. [Google Scholar] [CrossRef] [PubMed]
- Loap, P.; Vu-Bezin, J.; Monceau, V.; Jacob, S.; Fourquet, A.; Kirova, Y. Dosimetric evaluation of the benefit of deep inspiration breath hold (DIBH) for locoregional irradiation of right breast cancer with volumetric modulated arctherapy (VMAT). Acta Oncol. 2023, 62, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Conway, J.L.; Conroy, L.; Harper, L.; Scheifele, M.; Li, H.; Smith, W.L.; Graham, T.; Phan, T.; Olivotto, I.A. Deep inspiration breath-hold produces a clinically meaningful reduction in ipsilateral lung dose during locoregional radiation therapy for some women with right-sided breast cancer. Pract. Radiat. Oncol. 2017, 7, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Rice, L.; Harris, S.; Green, M.M.L.; Price, P.M. Deep inspiration breath-hold (DIBH) technique applied in right breast radiotherapy to minimize liver radiation. BJR Case Rep. 2015, 1, 20150038. [Google Scholar] [CrossRef]
- Ramella, S.; Trodella, L.; Ippolito, E.; Fiore, M.; Cellini, F.; Stimato, G.; Gaudino, D.; Greco, C.; Ramponi, S.; Cammilluzzi, E.; et al. Whole-breast irradiation: A subgroup analysis of criteria to stratify for prone position treatment. Med. Dosim. 2012, 37, 186–191. [Google Scholar] [CrossRef]
- Wang, X.; Fargier-Bochaton, O.; Dipasquale, G.; Laouiti, M.; Kountouri, M.; Gorobets, O.; Nguyen, N.P.; Miralbell, R.; Vinh-Hung, V. Is prone free breathing better than supine deep inspiration breath-hold for left whole-breast radiotherapy? A dosimetric analysis. Strahlenther. Onkol. 2021, 197, 317–331. [Google Scholar] [CrossRef]
- Fargier-Bochaton, O.; Wang, X.; Dipasquale, G.; Laouiti, M.; Kountouri, M.; Gorobets, O.; Nguyen, N.P.; Miralbell, R.; Vinh-Hung, V. Prone versus supine free-breathing for right-sided whole breast radiotherapy. Sci. Rep. 2022, 12, 525. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Left-Sided Patients | Right-Sided Patients | ||||||
|---|---|---|---|---|---|---|---|---|
| N° Patients | 56 | 65 | ||||||
| Minimum | Maximum | Mean | SD | Minimum | Maximum | Mean | SD | |
| Breast Volume (cc) | 233.48 | 2189.57 | 892.64 | 435.56 | 256.79 | 1852.58 | 864.09 | 348.45 |
| Heart Volume (cc) | 436.78 | 1029.84 | 643.77 | 118.20 | 419.53 | 1359.37 | 637.85 | 150.53 |
| Ipsilateral Lung Volume (cc) | 668.87 | 3076.97 | 1203.13 | 363.65 | 828.87 | 2291.82 | 1502.13 | 336.13 |
| mHD | 0.96 | 5.08 | 2.55 | 0.10 | 0.80 | 2.52 | 1.37 | 0.37 |
| MLAD | 3.78 | 20.15 | 14.29 | 4.03 | 0.97 | 4.53 | 1.59 | 0.62 |
| mLAD | 1.81 | 11.17 | 5.77 | 2.24 | 0.72 | 2.43 | 1.24 | 0.35 |
| Side | Volume | mHD (r, p) | mLAD (r, p) | MLAD (r, p) |
|---|---|---|---|---|
| Right | Breast | 0.531, <0.001 * | 0.443, <0.001 * | 0.323, <0.001 * |
| Heart | 0.243, 0.051 | 0.156, 0.215 | 0.125, 0.323 | |
| Ipsilateral Lung | −0.280, 0.024 * | −0.125, 0.320 | −0.130, 0.301 | |
| Left | Breast | 0.392, 0.003 * | 0.327, 0.014 * | 0.180, 0.183 |
| Heart | 0.378, 0.004 * | 0.345, 0.090 | 0.332, 0.012 * | |
| Ipsilateral Lung | −0.524, <0.001 * | −0.597, <0.001 * | −0.639, <0.001 * |
| Univariate | Multivariate | ||||||
|---|---|---|---|---|---|---|---|
| Side RIGHT | mHD | R2 | F | p | R2 | F | p |
| Breast Volume | 0.282 | 24.790 | <0.001 * | ||||
| Lung Volume | 0.085 | 5.359 | 0.024 | ||||
| mLAD | |||||||
| Breast Volume | 0.196 | 15.395 | <0.001 * | ||||
| MLAD | |||||||
| Breast Volume | 0.104 | 7.331 | 0.009 * | ||||
| Side LEFT | mHD | R2 | F | p | R2 | F | p |
| Breast Volume | 0.154 | 9.800 | 0.003 * | 0.483 | 16.165 | 0.349 | |
| Heart Volume | 0.143 | 9.024 | 0.004 * | 0.005 | |||
| Lung Volume | 0.274 | 20.429 | <0.001 * | <0.001 | |||
| mLAD | |||||||
| Breast Volume | 0.107 | 6.462 | 0.014 | ||||
| Heart Volume | 0.119 | 7.301 | 0.009 * | 0.434 | 20.350 | 0.009 | |
| Lung Volume | 0.356 | 29.893 | <0.001 * | <0.001 | |||
| MLAD | |||||||
| Heart Volume | 0.110 | 6.706 | 0.012 | ||||
| Lung Volume | 0.408 | 37.213 | <0.001 * | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alaimo, R.; Ippolito, E.; Falconi, R.; Perrone Congedi, F.; Sciommari, C.; Silipigni, S.; Pellegrini, R.; Carnevale, A.; Greco, C.; Fiore, M.; et al. Breast Volume Is a Predictor of Higher Heart Dose in Whole-Breast Supine Free-Breathing Volumetric-Modulated Arc Therapy Planning. Curr. Oncol. 2023, 30, 10530-10538. https://doi.org/10.3390/curroncol30120768
Alaimo R, Ippolito E, Falconi R, Perrone Congedi F, Sciommari C, Silipigni S, Pellegrini R, Carnevale A, Greco C, Fiore M, et al. Breast Volume Is a Predictor of Higher Heart Dose in Whole-Breast Supine Free-Breathing Volumetric-Modulated Arc Therapy Planning. Current Oncology. 2023; 30(12):10530-10538. https://doi.org/10.3390/curroncol30120768
Chicago/Turabian StyleAlaimo, Rita, Edy Ippolito, Rita Falconi, Francesca Perrone Congedi, Cecilia Sciommari, Sonia Silipigni, Roberto Pellegrini, Alessia Carnevale, Carlo Greco, Michele Fiore, and et al. 2023. "Breast Volume Is a Predictor of Higher Heart Dose in Whole-Breast Supine Free-Breathing Volumetric-Modulated Arc Therapy Planning" Current Oncology 30, no. 12: 10530-10538. https://doi.org/10.3390/curroncol30120768
APA StyleAlaimo, R., Ippolito, E., Falconi, R., Perrone Congedi, F., Sciommari, C., Silipigni, S., Pellegrini, R., Carnevale, A., Greco, C., Fiore, M., D’Angelillo, R. M., & Ramella, S. (2023). Breast Volume Is a Predictor of Higher Heart Dose in Whole-Breast Supine Free-Breathing Volumetric-Modulated Arc Therapy Planning. Current Oncology, 30(12), 10530-10538. https://doi.org/10.3390/curroncol30120768