Trends in Selective Internal Radiation Therapy (SIRT) for Treating Hepatocellular Carcinoma, Cholangiocarcinoma, and Liver Metastasis: A Total Population Analysis from 2006 to 2021 in Germany

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Database
2.2. German Billing Database (Destatis)
2.3. German Hospitals’ Quality Reports
2.4. Statistical Analysis
2.5. Ethics Statement
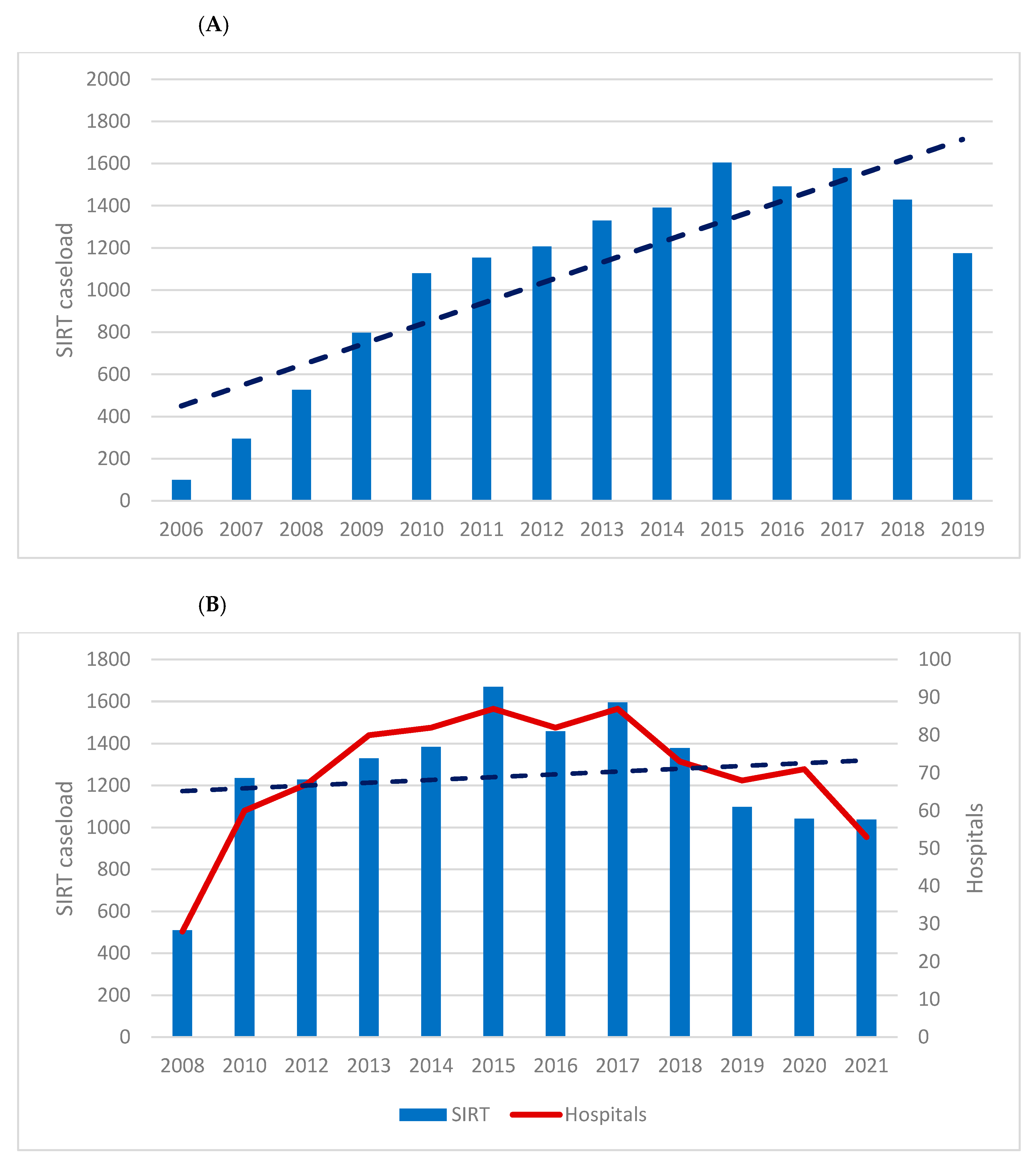
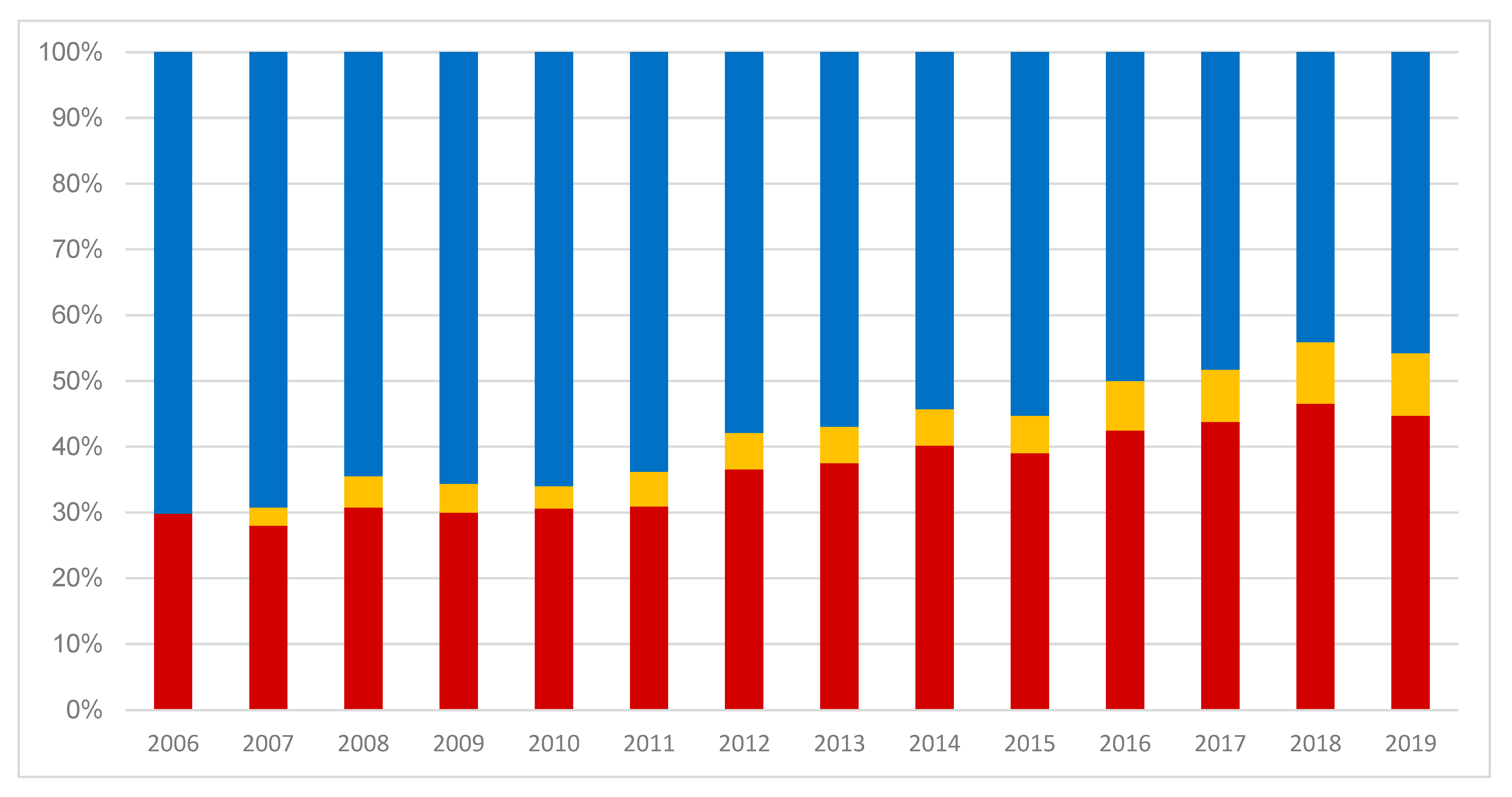
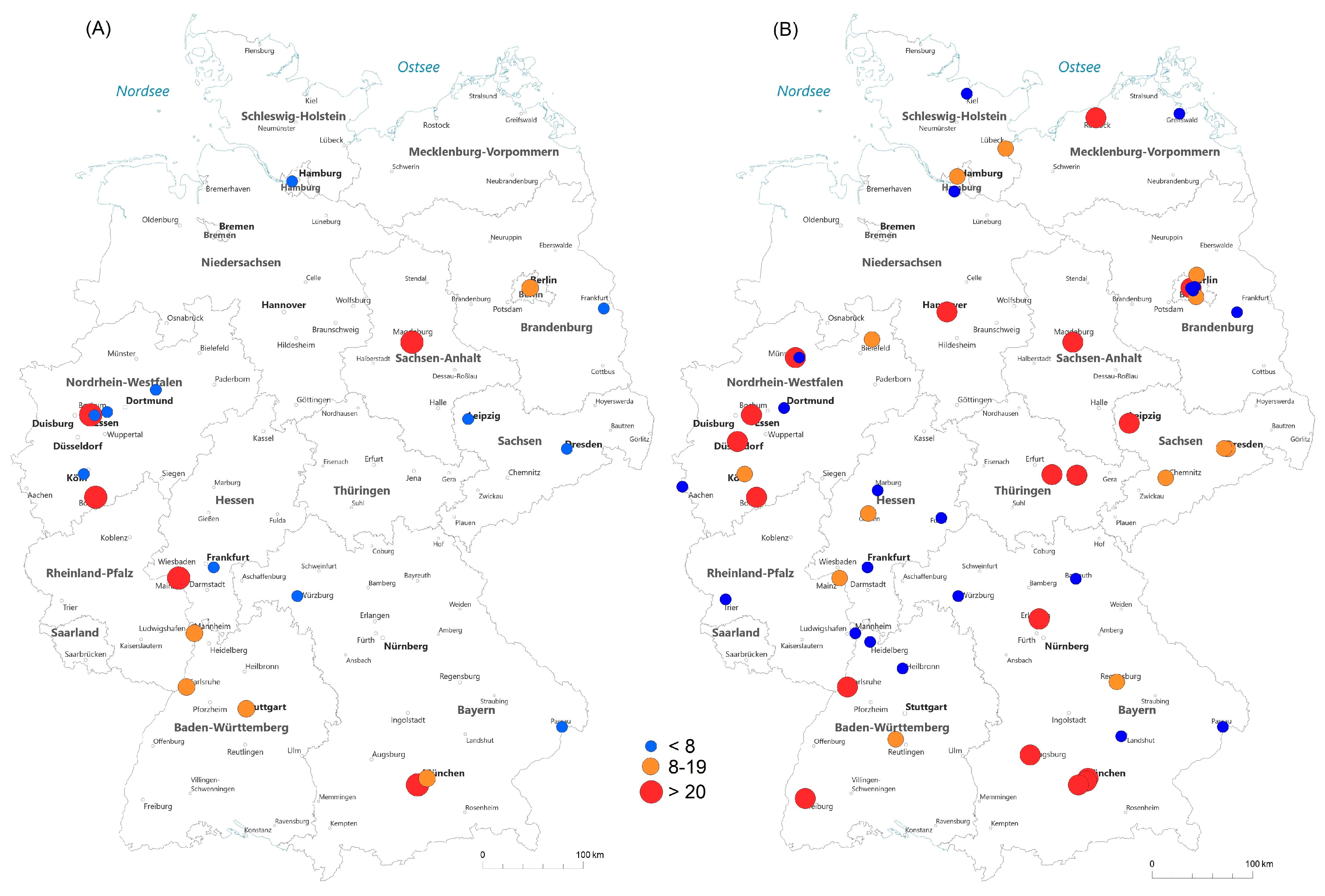
3. Results
4. Discussion
4.1. HCC, CCC, and Liver Metastasis
4.2. Patient’s Age, Caseload Distribution, and University Setting
4.3. In-Hospital Complications and Mortality, Blood Transfusions, and LOS
4.4. Holmium, Rhenium, and Yttrium
4.5. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Helmberger, T.; Arnold, D.; Bilbao, J.I.; de Jong, N.; Maleux, G.; Nordlund, A.; Peynircioglu, B.; Sangro, B.; Sharma, R.A.; Walk, A. Clinical Application of Radioembolization in Hepatic Malignancies: Protocol for a Prospective Multicenter Observational Study. JMIR Res. Protoc. 2020, 9, e16296. [Google Scholar] [CrossRef]
- Spahr, N.; Thoduka, S.; Abolmaali, N.; Kikinis, R.; Schenk, A. Multimodal image registration for liver radioembolization planning and patient assessment. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 215–225. [Google Scholar] [CrossRef]
- Sundram, F.X.; Buscombe, J.R. Selective internal radiation therapy for liver tumours. Clin. Med. 2017, 17, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Cucch Cucchetti, A.; Cappelli, A.; Ercolani, G.; Mosconi, C.; Cescon, M.; Golfieri, R.; Pinna, A.D. Selective Internal Radiation Therapy (SIRT) as Conversion Therapy for Unresectable Primary Liver Malignancies. Liver Cancer 2016, 5, 303–311. [Google Scholar] [CrossRef]
- Lemaire, M.; Lucidi, V.; Bouazza, F.; Katsanos, G.; Vanderlinden, B.; Levillain, H.; Delatte, P.; Garcia, C.A.; Vouche, M.; Galdon, M.G.; et al. Selective internal radiation therapy (SIRT) before partial hepatectomy or radiofrequency destruction for treatment of hepatocellular carcinoma in cirrhotic patients: A feasibility and safety pilot study. HPB 2018, 20, 641–648. [Google Scholar] [CrossRef]
- Yang, B.; Liang, J.; Qu, Z.; Yang, F.; Liao, Z.; Gou, H. Transarterial strategies for the treatment of unresectable hepatocellular carcinoma: A systematic review. PLoS ONE 2020, 15, e0227475, Erratum in PLoS ONE 2020, 15, e0230369. [Google Scholar] [CrossRef]
- Kulik, L.M.; Carr, B.I.; Mulcahy, M.F.; Lewandowski, R.J.; Atassi, B.; Ryu, R.K.; Sato, K.T.; Benson, A., 3rd; Nemcek, A.A., Jr.; Gates, V.L.; et al. Safety and efficacy of 90Y radiotherapy for hepatocellular carcinoma with and without portal vein thrombosis. 2008, 47, 71–81. Hepatology 2008, 47, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, R.S.; Wickremesekera, S.K. Selective internal radiation therapy (SIRT): A new modality for treating patients with colorectal liver metastases. HPB 2004, 6, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Radosa, C.G.; Nadjiri, J.; Mahnken, A.H.; Bücker, A.; Heuser, L.J.; Morhard, D.; Landwehr, P.; Berlis, A.; Katoh, M.; Reimer, P.; et al. Availability of Interventional Oncology in Germany in the Years 2018 and 2019—Results from a Nationwide Database (DeGIR Registry Data). Rofo 2022, 194, 755–761. [Google Scholar] [CrossRef]
- Flegar, L.; Kraywinkel, K.; Zacharis, A.; Aksoy, C.; Koch, R.; Eisenmenger, N.; Groeben, C.; Huber, J. Treatment trends for muscle-invasive bladder cancer in Germany from 2006 to 2019. World J. Urol. 2022, 40, 1715–1721. [Google Scholar] [CrossRef]
- Krieg, S.; Essing, T.; Krieg, A.; Roderburg, C.; Luedde, T.; Loosen, S.H. Recent Trends and In-Hospital Mortality of Transarterial Chemoembolization (TACE) in Germany: A Systematic Analysis of Hospital Discharge Data between 2010 and 2019. Cancers 2022, 14, 2088. [Google Scholar] [CrossRef]
- Birgin, E.; Rasbach, E.; Seyfried, S.; Rathmann, N.; Diehl, S.J.; Schoenberg, S.O.; Reissfelder, C.; Rahbari, N.N. Contralateral Liver Hypertrophy and Oncological Outcome Following Radioembolization with 90Y-Microspheres: A Systematic Review. Cancers 2020, 12, 294. [Google Scholar] [CrossRef]
- Garg, T.; Shrigiriwar, A.; Habibollahi, P.; Cristescu, M.; Liddell, R.P.; Chapiro, J.; Inglis, P.; Camacho, J.C.; Nezami, N. Intraarterial Therapies for the Management of Hepatocellular Carcinoma. Cancers 2022, 14, 3351. [Google Scholar] [CrossRef]
- Craciun, L.; de Wind, R.; Demetter, P.; Lucidi, V.; Bohlok, A.; Michiels, S.; Bouazza, F.; Vouche, M.; Tancredi, I.; Verset, G.; et al. Retrospective analysis of the immunogenic effects of intra-arterial locoregional therapies in hepatocellular carcinoma: A rationale for combining selective internal radiation therapy (SIRT) and immunotherapy. BMC Cancer 2020, 20, 135. [Google Scholar] [CrossRef] [PubMed]
- Vogel, A.; Cervantes, A.; Chau, I.; Daniele, B.; Llovet, J.M.; Meyer, T.; Nault, J.C.; Neumann, U.; Ricke, J.; Sangro, B.; et al. Hepatocellular carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29 (Suppl. 4), iv238–iv255, Erratum in Ann. Oncol. 2019, 30, 871–873; Erratum in Ann. Oncol. 2022, 33, 666. [Google Scholar] [CrossRef] [PubMed]
- Dadrass, F.; Sher, A.; Kim, E. Update on Locoregional Therapies for Liver Cancer: Radiation Segmentectomy. Curr. Oncol. 2023, 30, 10075–10084. [Google Scholar] [CrossRef]
- Edeline, J.; Touchefeu, Y.; Guiu, B.; Farge, O.; Tougeron, D.; Baumgaertner, I.; Ayav, A.; Campillo-Gimenez, B.; Beuzit, L.; Pracht, M.; et al. Radioembolization Plus Chemotherapy for First-line Treatment of Locally Advanced Intrahepatic Cholangiocarcinoma: A Phase 2 Clinical Trial. JAMA Oncol. 2020, 6, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Benguerfi, S.; Estrade, F.; Lescure, C.; Rolland, Y.; Palard, X.; Le Sourd, S.; Pracht, M.; Bourien, H.; Muzellec, L.; Le Du, F.; et al. Selective internal radiation therapy in older patients with hepatocellular carcinoma: A retrospective analysis. Eur. J. Gastroenterol. Hepatol. 2022, 34, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Sarwar, A.; Zhou, L.; Novack, V.; Tapper, E.B.; Curry, M.; Malik, R.; Ahmed, M. Hospital volume and mortality after transjugular intrahepatic portosystemic shunt creation in the United States. Hepatology 2018, 67, 690–699. [Google Scholar] [CrossRef]
- Murthy, R.; Brown, D.B.; Salem, R.; Meranze, S.G.; Coldwell, D.M.; Krishnan, S.; Nunez, R.; Habbu, A.; Liu, D.; Ross, W.; et al. Gastrointestinal complications associated with hepatic arterial Yttrium-90 microsphere therapy. J. Vasc. Interv. Radiol. 2007, 18, 553–561; quiz 562. [Google Scholar] [CrossRef] [PubMed]
- Ricke, J.; Schinner, R.; Seidensticker, M.; Gasbarrini, A.; van Delden, O.M.; Amthauer, H.; Peynircioglu, B.; Bargellini, I.; Iezzi, R.; De Toni, E.N.; et al. Liver function after combined selective internal radiation therapy or sorafenib monotherapy in advanced hepatocellular carcinoma. J. Hepatol. 2021, 75, 1387–1396. [Google Scholar] [CrossRef]
- Mertens, A.; Essing, T.; Minko, P.; Möllenhoff, K.; Mattes-György, K.; Giesel, F.L.; Antoch, G.; Luedde, T.; Roderburg, C.; Loosen, S.H. Selective internal radiotherapy in Germany: A review of indications and hospital mortality from 2012 to 2019. J. Clin. Transl. Res. 2023, 9, 123–132. [Google Scholar] [PubMed]
- Kennedy, A.; Brown, D.B.; Feilchenfeldt, J.; Marshall, J.; Wasan, H.; Fakih, M.; Gibbs, P.; Knuth, A.; Sangro, B.; Soulen, M.C.; et al. Safety of selective internal radiation therapy (SIRT) with yttrium-90 microspheres combined with systemic anticancer agents: Expert consensus. J. Gastrointest. Oncol. 2017, 8, 1079–1099. [Google Scholar] [CrossRef] [PubMed]
- Salem, R.; Lewandowski, R.J.; Mulcahy, M.F.; Riaz, A.; Ryu, R.K.; Ibrahim, S.; Atassi, B.; Baker, T.; Gates, V.; Miller, F.H.; et al. Radioembolization for hepatocellular carcinoma using Yttrium-90 microspheres: A comprehensive report of long-term outcomes. Gastroenterology 2010, 138, 52–64. [Google Scholar] [CrossRef] [PubMed]
- Spahr, N.; Schilling, P.; Thoduka, S.; Abolmaali, N.; Schenk, A. Predictive SIRT dosimetry based on a territorial model. EJNMMI Phys. 2017, 4, 25. [Google Scholar] [CrossRef]
- Smits, M.L.; Elschot, M.; van den Bosch, M.A.; van de Maat, G.H.; van het Schip, A.D.; Zonnenberg, B.A.; Seevinck, P.R.; Verkooijen, H.M.; Bakker, C.J.; de Jong, H.W.; et al. In vivo dosimetry based on SPECT and MR imaging of 166Ho-microspheres for treatment of liver malignancies. J. Nucl. Med. 2013, 54, 2093–2100. [Google Scholar] [CrossRef]
- Radosa, C.G.; Radosa, J.C.; Grosche-Schlee, S.; Zöphel, K.; Plodeck, V.; Kühn, J.P.; Kotzerke, J.; Hoffmann, R.T. Holmium-166 Radioembolization in Hepatocellular Carcinoma: Feasibility and Safety of a New Treatment Option in Clinical Practice. Cardiovasc. Interv. Radiol. 2019, 42, 405–412. [Google Scholar] [CrossRef]
- Drescher, R.; Seifert, P.; Gühne, F.; Aschenbach, R.; Kühnel, C.; Freesmeyer, M. Radioembolization With Holmium-166 Polylactic Acid Microspheres: Distribution of Residual Activity in the Delivery Set and Outflow Dynamics During Planning and Treatment Procedures. J. Endovasc. Ther. 2021, 28, 452–462. [Google Scholar] [CrossRef]
- Shukla, J.; Goyal, A.; Chhabra, A.; Rathore, Y.; Bansal, K.; Pandey, S.; Parmar, M.; Singhal, S.; Kalra, N.; Duseja, A.; et al. Cold kit for Rhenium-188 microspheres based selective intra-arterial therapy (SIRT): Preparation, characterization and feasibility study. Appl. Radiat. Isot. 2022, 190, 110423. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source of data | Nationwide hospital billing database of the German Federal Statistical Office (Destatis database) | German hospitals’ quality reports (reimbursement.INFO tool) |
| Details | Age and gender Diagnosis code in combination with OPS code Surgical access route Hospital characteristics (teaching status, size, annual surgery/procedure caseload, approaches for surgery/procedure) | Age and gender Diagnosis code or OPS code (no combination possible) Hospital characteristics (teaching status, annual surgery/procedure caseload) Geographical localization of respective hospitals |
| Number of patients | 13,981 | 14,165 |
| Proportion of population | 100% | 100% |
| Years | 2006–2019 | 2008–2021 (missing: 2006, 2007, 2009, 2011) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thoduka, S.G.; Flegar, L.; Groeben, C.; Huber, J.; Eisenmenger, N.; Paulus, T.; Vogt, K.; Luster, M.; Abolmaali, N. Trends in Selective Internal Radiation Therapy (SIRT) for Treating Hepatocellular Carcinoma, Cholangiocarcinoma, and Liver Metastasis: A Total Population Analysis from 2006 to 2021 in Germany. Curr. Oncol. 2023, 30, 10325-10335. https://doi.org/10.3390/curroncol30120752
Thoduka SG, Flegar L, Groeben C, Huber J, Eisenmenger N, Paulus T, Vogt K, Luster M, Abolmaali N. Trends in Selective Internal Radiation Therapy (SIRT) for Treating Hepatocellular Carcinoma, Cholangiocarcinoma, and Liver Metastasis: A Total Population Analysis from 2006 to 2021 in Germany. Current Oncology. 2023; 30(12):10325-10335. https://doi.org/10.3390/curroncol30120752
Chicago/Turabian StyleThoduka, Smita George, Luka Flegar, Christer Groeben, Johannes Huber, Nicole Eisenmenger, Tobias Paulus, Katharina Vogt, Markus Luster, and Nasreddin Abolmaali. 2023. "Trends in Selective Internal Radiation Therapy (SIRT) for Treating Hepatocellular Carcinoma, Cholangiocarcinoma, and Liver Metastasis: A Total Population Analysis from 2006 to 2021 in Germany" Current Oncology 30, no. 12: 10325-10335. https://doi.org/10.3390/curroncol30120752
APA StyleThoduka, S. G., Flegar, L., Groeben, C., Huber, J., Eisenmenger, N., Paulus, T., Vogt, K., Luster, M., & Abolmaali, N. (2023). Trends in Selective Internal Radiation Therapy (SIRT) for Treating Hepatocellular Carcinoma, Cholangiocarcinoma, and Liver Metastasis: A Total Population Analysis from 2006 to 2021 in Germany. Current Oncology, 30(12), 10325-10335. https://doi.org/10.3390/curroncol30120752