A Study of Peripheral Blood Parameters to Predict Response to Induction Chemotherapy and Overall Survival in Advanced Laryngeal Squamous Cell Carcinoma

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
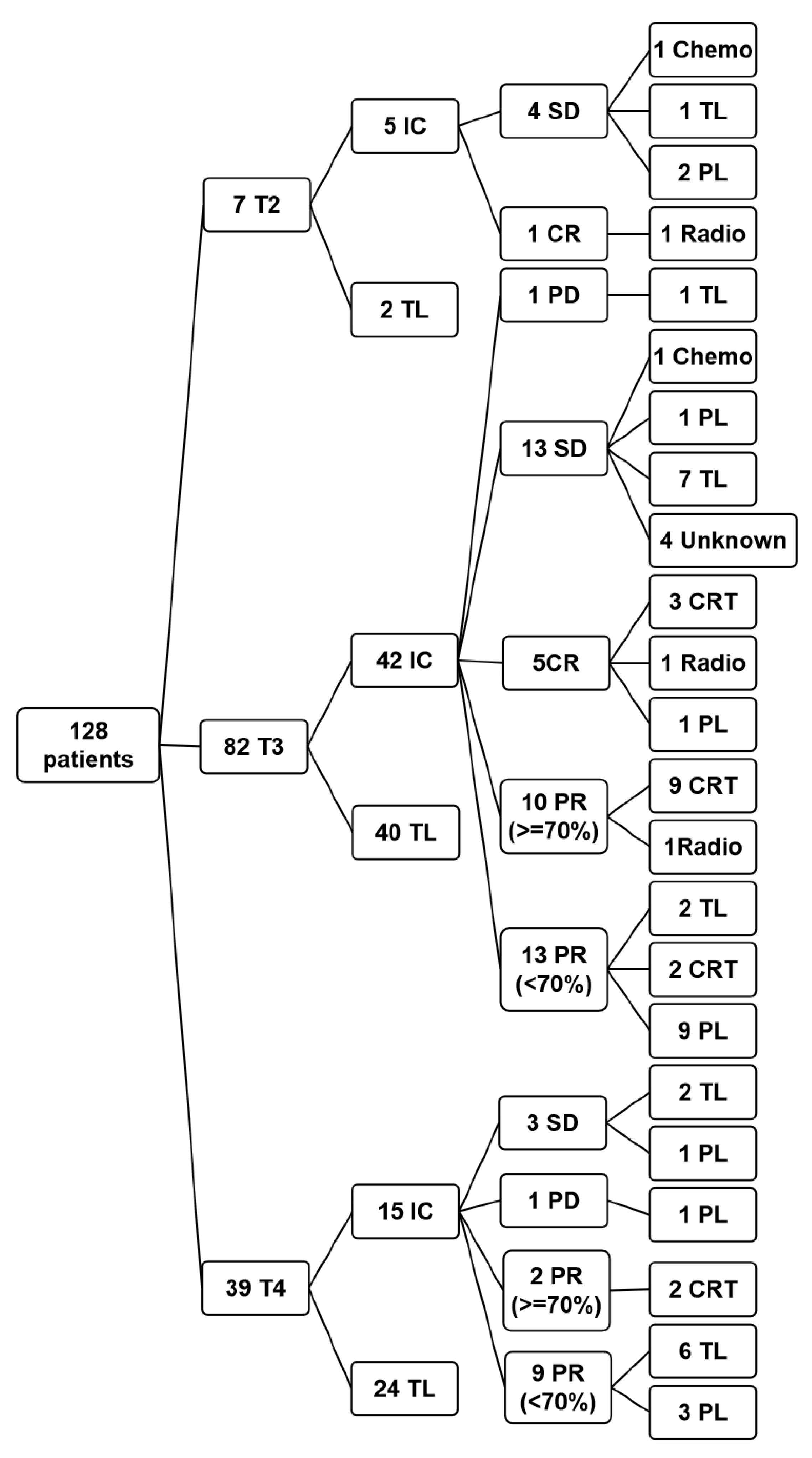
2.1. Patients
2.2. Treatment Protocol
2.3. Statistical Analysis
3. Results
3.1. The Study of Peripheral Blood Parameters to Predict IC Response in Advanced LSCC
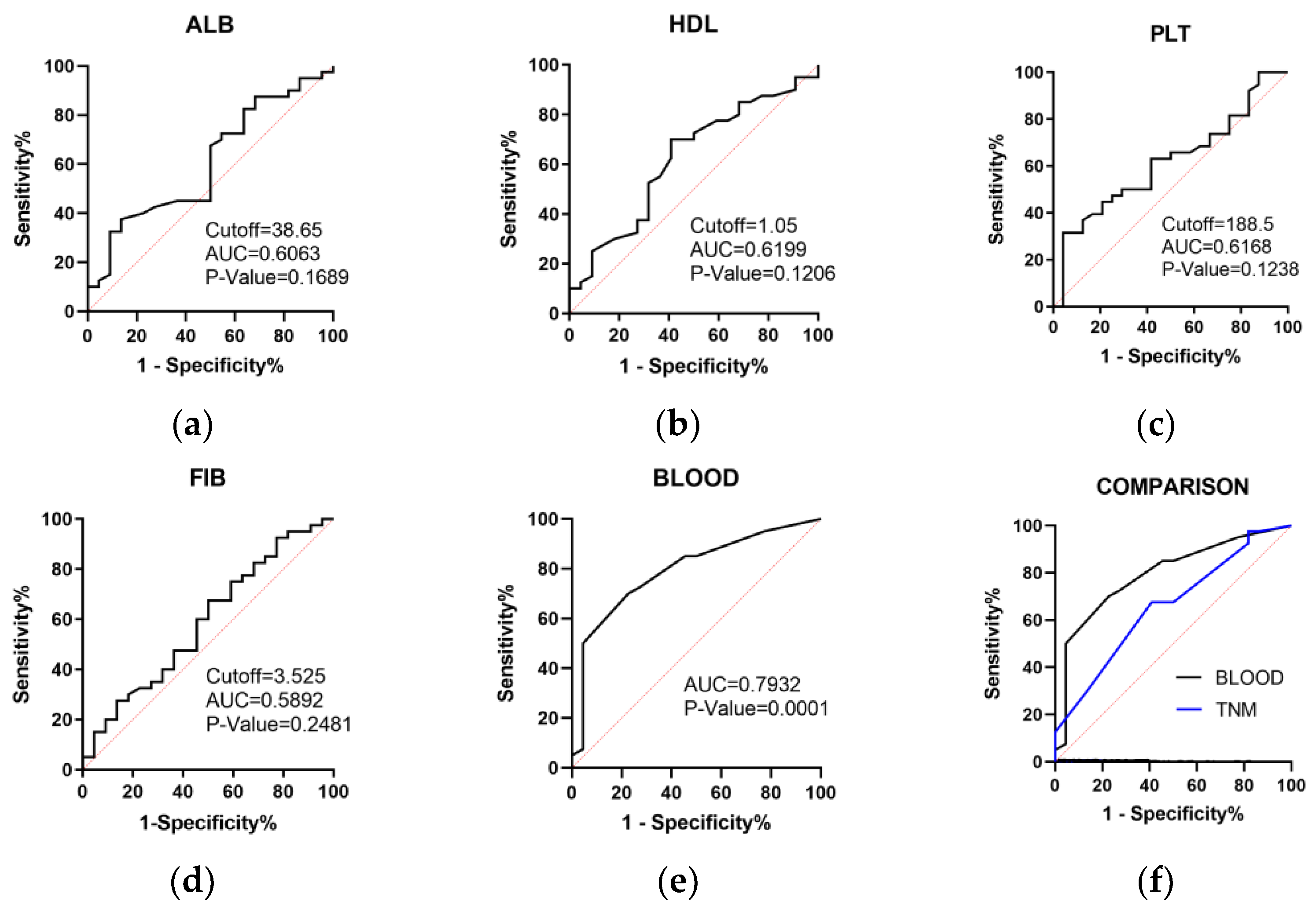
3.1.1. ROC Analysis to Select Potential Peripheral Blood Indicators
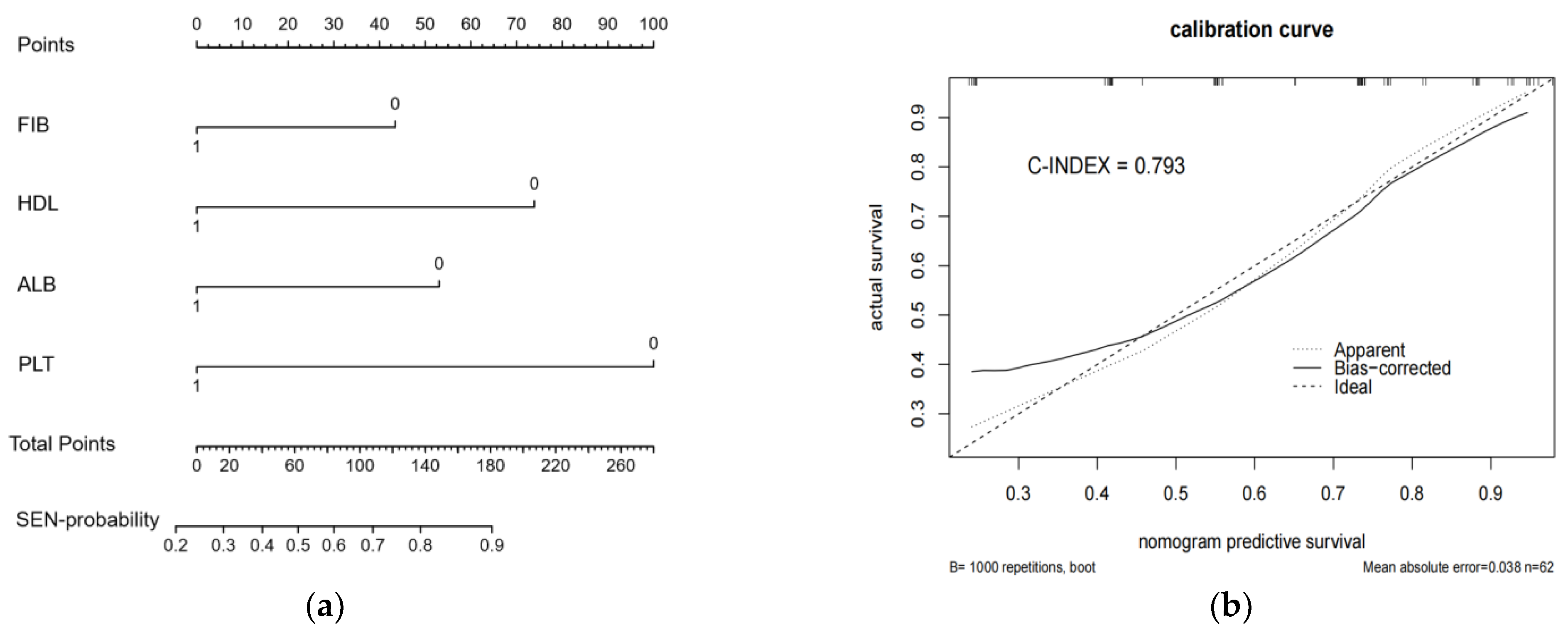
3.1.2. A Nomogram Model of Peripheral Blood Parameters Was Constructed to Predict IC Response
3.2. The Study of Peripheral Blood Parameters to Predict Overall Survival in Advanced LSCC
3.2.1. ROC and K-M Analysis to Select Potential Peripheral Blood Parameters to Predict OS
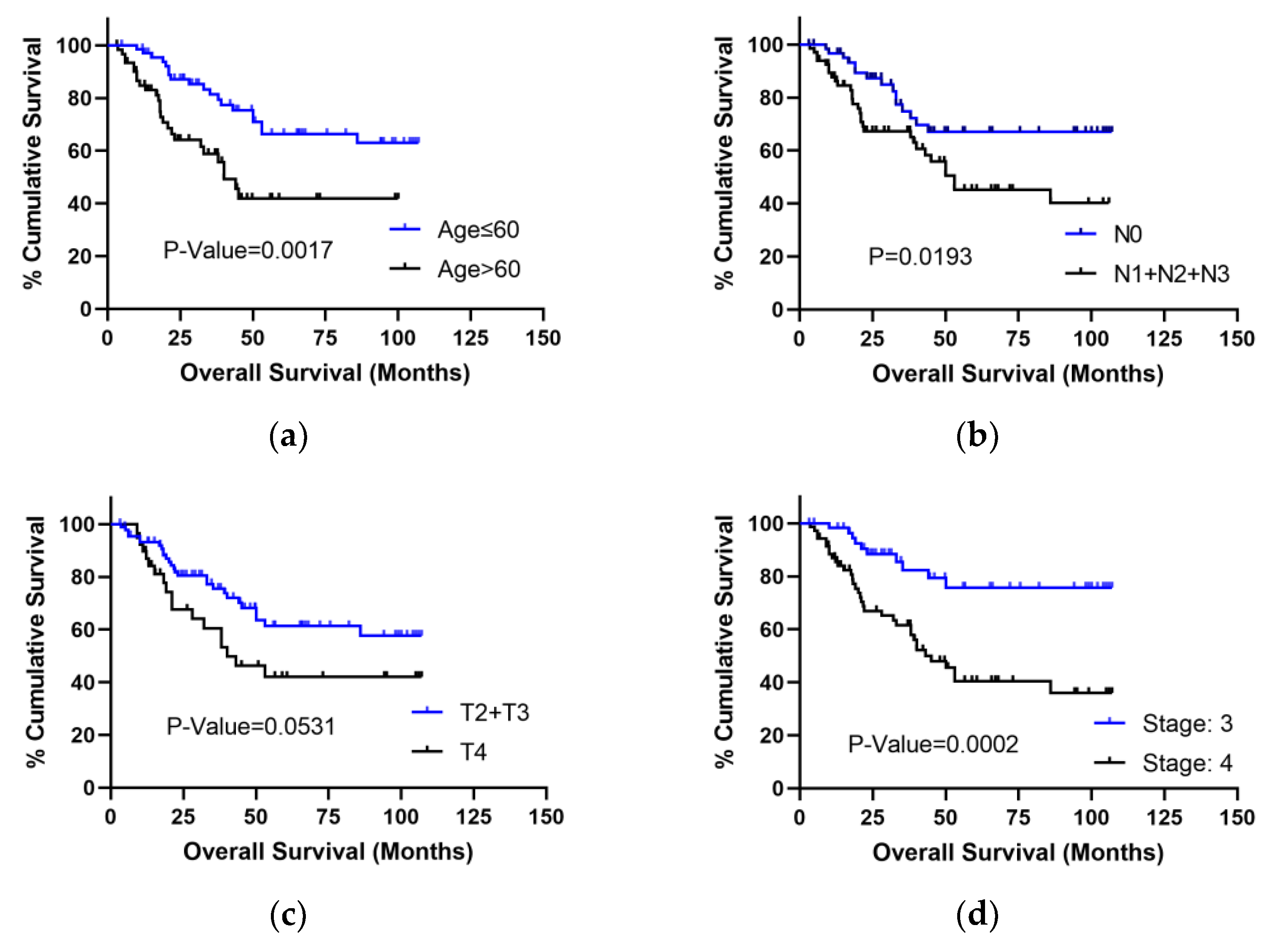
3.2.2. K-M Analysis to Select Clinical Factors Associated with OS
3.2.3. Multivariate COX Analysis to Select Independent Prognostic Factors for Advanced LSCC Patients
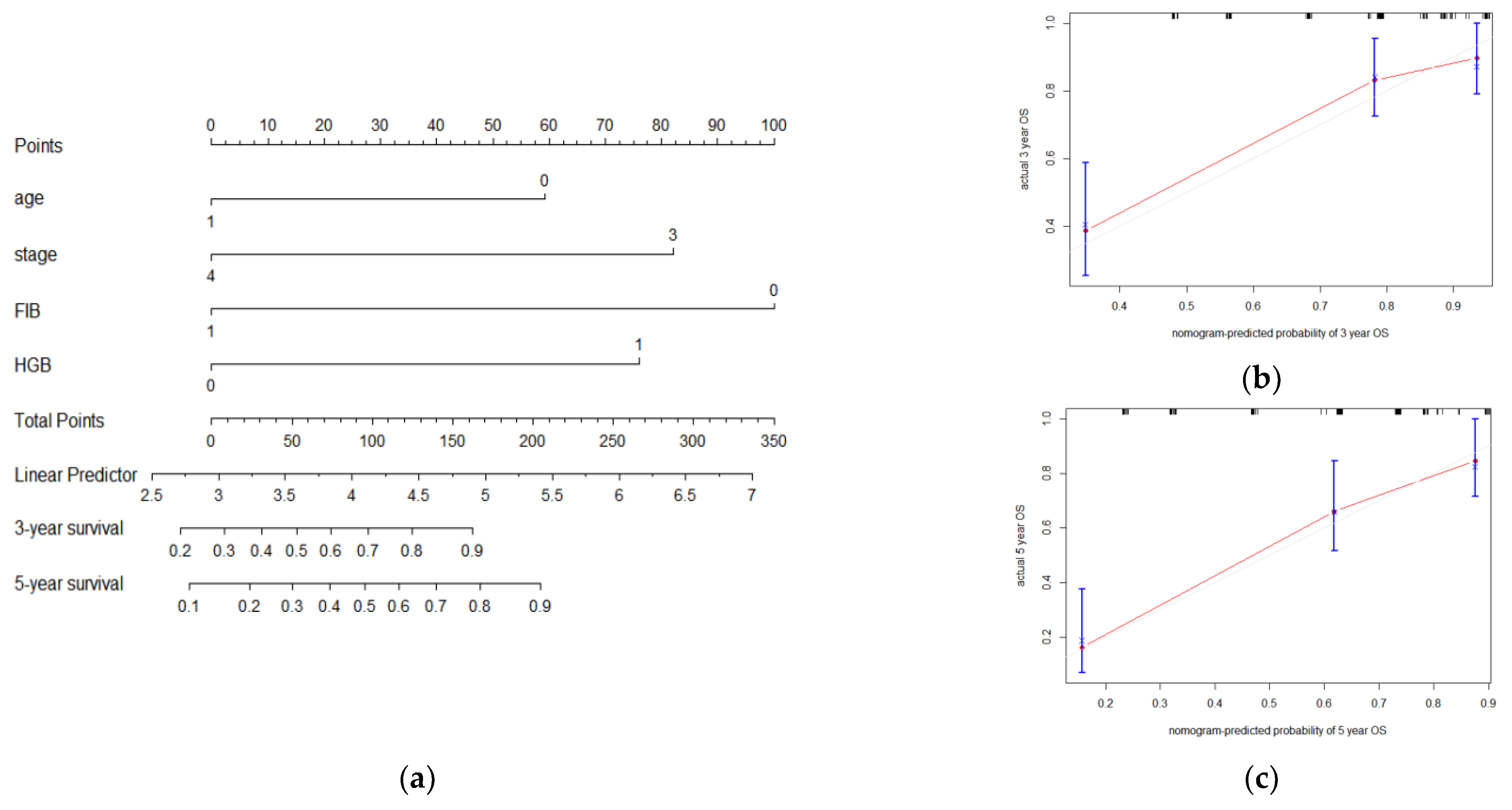
3.2.4. A Nomogram Model Was Constructed to Predict OS in LSCC Patients
3.3. K-M Analysis of OS, PFS, and DSS in Surgery Group and IC Group Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xun, Y.F.; Wang, M.H.; Sun, H.Y.; Shi, S.J.; Guan, B.; Yu, C.J. Prognostic Analysis of Preoperative Inflammatory Biomarkers in Patients With Laryngeal Squamous Cell Carcinoma. Ent-Ear Nose Throat J. 2020, 99, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; Wang, Q.; Yu, Q. The Systemic Immune-Inflammation Index and Albumin as Prognostic Predictors in Laryngeal Carcinoma. Nutr. Cancer 2021, 73, 1916–1923. [Google Scholar] [CrossRef] [PubMed]
- Papadas, T.A.; Alexopoulos, E.C.; Mallis, A.; Jelastopulu, E.; Mastronikolis, N.S.; Goumas, P. Survival after laryngectomy: A review of 133 patients with laryngeal carcinoma. Eur. Arch. Oto-Rhino-Laryngol. 2010, 267, 1095–1101. [Google Scholar] [CrossRef]
- Li, Z.L.; Qu, Y.; Yang, Y.; An, W.; Li, S.Q.; Wang, B.; He, Y.; Li, J.; Shao, Q.; Qin, L.Z. Prognostic value of the neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio and systemic immune-inflammation index in patients with laryngeal squamous cell carcinoma. Clin. Otolaryngol. 2021, 46, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Gadepalli, C.; de Casso, C.; Silva, S.; Loughran, S.; Homer, J.J. Functional results of pharyngo-laryngectomy and total laryngectomy: A comparison. J. Laryngol. Otol. 2012, 126, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Leon, X.; Lopez-Pousa, A.; de Vega, M.; Orus, C.; de Juan, M.; Quer, M. Results of an organ preservation protocol with induction chemotherapy and radiotherapy in patients with locally advanced laryngeal carcinoma. Eur. Arch. Oto-Rhino-Laryngol. 2005, 262, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Leon, X.; Valero, C.; Rovira, C.; Rodriguez, C.; Lopez, M.; Garcia-Lorenzo, J.; Quer, M. Relationship between response to induction chemotherapy and disease control in patients with advanced laryngeal carcinoma included in an organ preservation protocol. Eur. Arch. Oto-Rhino-Laryngol. 2017, 274, 2581–2587. [Google Scholar] [CrossRef]
- Sharma, M.R.; Schilsky, R.L. New standards and a predictive biomarker for adjuvant therapy. Nat. Rev. Clin. Oncol. 2011, 8, 70–72. [Google Scholar] [CrossRef]
- Hu, K.; Harrison, L.B. Impact of anemia in patients with head and neck cancer treated with radiation therapy. Curr. Treat. Options Oncol. 2005, 6, 31–45. [Google Scholar] [CrossRef]
- Ballestrero, A.; Bedognetti, D.; Ferraioli, D.; Franceschelli, P.; Labidi-Galy, S.I.; Leo, E.; Murai, J.; Pommier, Y.; Tsantoulis, P.; Vellone, V.G.; et al. Report on the first SLFN11 monothematic workshop: From function to role as a biomarker in cancer. J. Transl. Med. 2017, 15, 199. [Google Scholar] [CrossRef]
- Fransawy Alkomos, M.; Rizk, M.; Eskander, G.; Elkheshen, A.; Mahendhar, R.; Shahbaz, A.; Zarghamravanbakhsh, P.; Younan, P.; Golchin, N.; Sachmechi, I. Age Limit and Radiotherapy Option for Sarcomatoid Carcinoma of the Larynx: A Case Report with Literature Review. Cureus 2018, 10, e3023. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Liu, W.W.; OuYang, D.; Yang, A.K.; Zhang, Q. Preoperative Neutrophil-to-lymphocyte Ratio Predicts Long-term Survival in Patients Undergoing Total Laryngectomy With Advanced Laryngeal Squamous Cell Carcinoma A Single-center Retrospective Study. Medicine 2016, 95, e2689. [Google Scholar] [CrossRef] [PubMed]
- Romeo, V.; Iorio, B.; Mesolella, M.; Ugga, L.; Verde, F.; Nicolai, E.; Covello, M. Simultaneous PET/MRI in assessing the response to chemo/radiotherapy in head and neck carcinoma: Initial experience. Med. Oncol. 2018, 35, 112. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Bhalla, A.S.; Thulkar, S.; Kumar, A.; Mohanti, B.K.; Thakar, A.; Sharma, A.; Vishnubhatla, S. Neoadjuvant intra-arterial chemotherapy in advanced laryngeal and hypopharyngeal cancer. Asia-Pac. J. Clin. Oncol. 2016, 12, E97–E104. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Galindo, C.; Hermsen, M.; Garcia-Pedrero, J.M.; Fresno, M.F.; Suarez, C.; Rodrigo, J.P. p27 and BCL2 expression predicts response to chemotherapy in head and neck squamous cell carcinomas. Oral Oncol. 2014, 50, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Ferrandino, R.M.; Roof, S.; Garneau, J.; Haidar, Y.; Bates, S.E.; Park, Y.H.A.; Bauml, J.M.; Genden, E.M.; Miles, B.; Sigel, K. Neutrophil-to-lymphocyte ratio as a prognostic indicator for overall and cancer-specific survival in squamous cell carcinoma of the head and neck. Head Neck-J. Sci. Spec. Head Neck 2020, 42, 2830–2840. [Google Scholar] [CrossRef]
- Takenaka, Y.; Oya, R.; Kitamiura, T.; Ashida, N.; Shimizu, K.; Takemura, K.; Yamamoto, Y.; Uno, A. Prognostic role of neutrophil-to-lymphocyte ratio in head and neck cancer: A meta-analysis. Head Neck-J. Sci. Spec. Head Neck 2018, 40, 647–655. [Google Scholar] [CrossRef]
- Bai, Y.Q.; Li, C.; Xia, L.; Gan, F.Y.; Zeng, Z.; Zhang, C.F.; Deng, Y.L.; Xu, Y.Y.; Liu, C.W.; Deng, S.Y.; et al. Identifies Immune Feature Genes for Prediction of Chemotherapy Benefit in Cancer. J. Cancer 2022, 13, 496–507. [Google Scholar] [CrossRef]
- Kim, W.; Park, J.; Sheen, H.; Byun, B.H.; Lim, I.; Kong, C.B.; Lim, S.M.; Woo, S.K. Development of deep learning model for prediction of chemotherapy response using PET images and radiomics features. In Proceedings of the IEEE Nuclear Science Symposium and Medical Imaging Conference (NSS/MIC)/25th International Symposium on Room-Temperature Semiconductor X-Ray and Gamma-Ray Detectors, Sydney, Australia, 10–17 November 2018. [Google Scholar]
- Xu, W.; Ma, Q.C.; Wang, L.Q.; He, C.Y.; Lu, S.; Ni, Z.T.; Hua, Z.C.; Zhu, Z.L.; Yang, Z.Y.; Zheng, Y.A.; et al. Prediction Model of Tumor Regression Grade for Advanced Gastric Cancer After Preoperative Chemotherapy. Front. Oncol. 2021, 11, 607640. [Google Scholar] [CrossRef]
- Cai, H.; Zhang, Z.H.; Zhou, Y.J.; Liu, J.; Chen, H.Q.; Lin, R.Y. The Prognostic Value of Preoperative Plasma Fibrinogen and Neutrophil-to-Lymphocyte Ratio in Patients With Laryngeal Squamous Cell Carcinoma. Ent-Ear Nose Throat J. 2021, 100, 731–736. [Google Scholar] [CrossRef]
- Ye, J.; Liao, B.; Jiang, X.H.; Dong, Z.H.; Hu, S.H.; Liu, Y.H.; Xiao, M. Prognosis Value of Platelet Counts, Albumin and Neutrophil-Lymphocyte Ratio of Locoregional Recurrence in Patients with Operable Head and Neck Squamous Cell Carcinoma. Cancer Manag. Res. 2020, 12, 731–741. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.F.; Guo, H.S.; Xu, J.C.; Li, B.; Liu, Y.J.; Cheng, C.; Zhou, C.Y.; Zhao, Y.F.; Liu, Y. Activated platelets inhibit hepatocellular carcinoma cell differentiation and promote tumor progression via platelet-tumor cell binding. Oncotarget 2016, 7, 60609–60622. [Google Scholar] [PubMed]
- Hisamatsu, E.; Nagao, M.; Toh, R.; Irino, Y.; Iino, T.; Hara, T.; Tanaka, H.; Satomi-Kobayashi, S.; Ishida, T.; Hirata, K.-I. Fibronectin-containing High-Density Lipoprotein is Associated with Cancer Cell Adhesion and Proliferation. Kobe J. Med. Sci. 2020, 66, E40–E48. [Google Scholar] [PubMed]
- Yu, L.T.; Guo, Y.; Chang, Z.G.; Zhang, D.Y.; Zhang, S.Q.; Pei, H.Z.; Pang, J.; Zhao, Z.J.; Chen, Y. Bidirectional Interaction Between Cancer Cells and Platelets Provides Potential Strategies for Cancer Therapies. Front. Oncol. 2021, 11, 764119. [Google Scholar] [CrossRef]
- Liu, S.Q.; Fang, J.; Jiao, D.C.; Liu, Z.Z. Elevated Platelet Count Predicts Poor Prognosis in Breast Cancer Patients with Supraclavicular Lymph Node Metastasis. Cancer Manag. Res. 2020, 12, 6069–6075. [Google Scholar] [CrossRef]
- Sheng, X.L.; Zhang, H.; Ge, P.J.; Chen, L.S.; Zhang, S.Y. A Retrospective Study of The Prognostic Significance of Preoperative Plasma Fibrinogen, Mean Platelet Volume, and the Neutrophil-to-Lymphocyte Ratio in Patients with Laryngeal Squamous Cell Carcinoma. Med. Sci. Monit. 2019, 25, 4527–4534. [Google Scholar] [CrossRef]
- Han, Y.X.; Ren, Z.Y.; Liu, Y.C.; Liu, Y.A. Diagnostic and Prognostic Value of Fibrinogen, Fibrinogen Degradation Products, and Lymphocyte/Monocyte Ratio in Patients With Laryngeal Squamous Cell Carcinoma. Ent-Ear Nose Throat J. 2021. [Google Scholar] [CrossRef]
- Gorphe, P.; Bouhir, S.; Garcia, G.; Alali, A.; Even, C.; Breuskin, I.; Tao, Y.G.; Janot, F.; Bidault, F.; Temam, S. Anemia and neutrophil-to-lymphocyte ratio in laryngeal cancer treated with induction chemotherapy. Laryngoscope 2020, 130, E144–E150. [Google Scholar] [CrossRef]
- Guo, Q.Q.; Wang, H.Y.; Zhao, Y.X.; Wang, H.X.; Zeng, F.; Hua, H.Y.; Xu, Q.; Huang, Y.Z. Cell-penetrating albumin conjugates for enhanced doxorubicin delivery. Polym. Chem. 2013, 4, 4584–4587. [Google Scholar] [CrossRef]
- Wang, K.; Xu, X.; Xiao, R.T.; Du, D.Y.; Wang, L.Q.; Zhang, H.Q.; Lv, Z.H.; Li, X.P.; Li, G. Development and validation of a nomogram to predict cancer-specific survival in patients with hypopharyngeal squamous cell carcinoma treated with primary surgery. J. Int. Med. Res. 2021, 49, 3000605211067414. [Google Scholar] [CrossRef]
- Bussu, F.; Almadori, G.; De Corso, E.; Rizzo, D.; Rigante, M.; Parrilla, C.; Valentini, V.; Paludetti, G. Endoscopic horizontal partial laryngectomy by CO2 laser in the management of supraglottic squamous cell carcinoma. Head Neck 2009, 31, 1196–1206. [Google Scholar] [CrossRef] [PubMed]
- Bussu, F.; Miccichè, F.; Rigante, M.; Dinapoli, N.; Parrilla, C.; Bonomo, P.; Cadoni, G.; Mantini, G.; Galli, J.; Rufini, V.; et al. Oncologic outcomes in advanced laryngeal squamous cell carcinomas treated with different modalities in a single institution: A retrospective analysis of 65 cases. Head Neck 2012, 34, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Bussu, F.; Paludetti, G.; Almadori, G.; De Virgilio, A.; Galli, J.; Miccichè, F.; Tombolini, M.; Rizzo, D.; Gallo, A.; Giglia, V.; et al. Comparison of total laryngectomy with surgical (cricohyoidopexy) and nonsurgical organ-preservation modalities in advanced laryngeal squamous cell carcinomas: A multicenter retrospective analysis. Head Neck 2013, 35, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Forastiere, A.; Goepfert, H.; Maor, M.; Pajak, T.; Weber, R.; Morrison, W.; Glisson, B.; Trotti, A.; Ridge, J.; Chao, C.; et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N. Engl. J. Med. 2003, 349, 2091–2098. [Google Scholar] [CrossRef]
- Wolf, G.; Fisher, S.; Hong, W.; Hillman, R.; Spaulding, M.; Laramore, G.; Endicott, J.; McClatchey, K.; Henderson, W. Induction chemotherapy plus radiation compared with surgery plus radiation in patients with advanced laryngeal cancer. N. Engl. J. Med. 1991, 324, 1685–1690. [Google Scholar]
- Pfister, D.; Spencer, S.; Adelstein, D.; Adkins, D.; Anzai, Y.; Brizel, D.; Bruce, J.; Busse, P.; Caudell, J.; Cmelak, A.; et al. Head and Neck Cancers, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. JNCCN 2020, 18, 873–898. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IC | Surgery | Total | p-Value | |
|---|---|---|---|---|
| Gender | 1 | |||
| Male | 59 | 63 | 122 | |
| Female | 3 | 3 | 6 | |
| Age (years) | 0.607 | |||
| >60 | 31 | 36 | 67 | |
| ≤60 | 31 | 30 | 61 | |
| T stage | 0.135 | |||
| 2 + 3 | 5 + 42 | 2 + 40 | 89 | |
| 4 | 15 | 24 | 39 | |
| N stage | 0.154 | |||
| 0 | 26 | 36 | 62 | |
| 1 | 3 | 17 | 20 | |
| 2 | 31 | 13 | 44 | |
| 3 | 2 | 2 | ||
| M stage | ||||
| 0 | 62 | 66 | ||
| 1 | 0 | 0 | ||
| Differentiation | 0.706 | |||
| High | 15 | 12 | 27 | |
| Moderate | 35 | 40 | 75 | |
| Poor | 12 | 14 | 26 | |
| Position | <0.05 | |||
| Supraglottic | 47 | 26 | 73 | |
| Glottic + Subglottic/Others | 13 + 2 | 36 + 4 | 55 | |
| LFP OR TL | ||||
| LFP 1 (radio + chemo + CRT 7 + PL 8) | 3 + 2 + 16 + 18 | 0 | 39 | |
| TL 2 | 19 | 66 | 85 | |
| Clinical Stage | 0.272 | |||
| 3 | 25 | 33 | 58 | |
| 4 | 37 | 33 | 70 | |
| Response to IC | ||||
| PD 3 + SD 4 | 22 | 22 | ||
| CR 5 + PR 6 | 40 | 40 |
| Variate | B | Exp(B) | p-Value |
|---|---|---|---|
| Age | 0.869 | 2.384 (1.272–4.466) | 0.007 * |
| T | −0.200 | 0.818 (0.444–1.508) | 0.520 |
| N | −0.042 | 0.958 (0.650–1.413) | 0.830 |
| Stage | 1.581 | 4.861 (1.759–13.427) | 0.002 * |
| FIB | 1.867 | 6.470 (1.522–27.500) | 0.011 * |
| HGB | −1.215 | 0.297 (0.153–0.577) | <0.001 * |
| PDW | −0.641 | 0.527 (0.256–1.083) | 0.081 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, J.; Yang, Y.; Zhong, Q.; Hou, L.; Ma, H.; Zhang, Y.; Feng, L.; He, S.; Lian, M.; Fang, J.; et al. A Study of Peripheral Blood Parameters to Predict Response to Induction Chemotherapy and Overall Survival in Advanced Laryngeal Squamous Cell Carcinoma. Curr. Oncol. 2022, 29, 6472-6484. https://doi.org/10.3390/curroncol29090509
Xu J, Yang Y, Zhong Q, Hou L, Ma H, Zhang Y, Feng L, He S, Lian M, Fang J, et al. A Study of Peripheral Blood Parameters to Predict Response to Induction Chemotherapy and Overall Survival in Advanced Laryngeal Squamous Cell Carcinoma. Current Oncology. 2022; 29(9):6472-6484. https://doi.org/10.3390/curroncol29090509
Chicago/Turabian StyleXu, Jiaqi, Yifan Yang, Qi Zhong, Lizhen Hou, Hongzhi Ma, Yang Zhang, Ling Feng, Shizhi He, Meng Lian, Jugao Fang, and et al. 2022. "A Study of Peripheral Blood Parameters to Predict Response to Induction Chemotherapy and Overall Survival in Advanced Laryngeal Squamous Cell Carcinoma" Current Oncology 29, no. 9: 6472-6484. https://doi.org/10.3390/curroncol29090509
APA StyleXu, J., Yang, Y., Zhong, Q., Hou, L., Ma, H., Zhang, Y., Feng, L., He, S., Lian, M., Fang, J., & Wang, R. (2022). A Study of Peripheral Blood Parameters to Predict Response to Induction Chemotherapy and Overall Survival in Advanced Laryngeal Squamous Cell Carcinoma. Current Oncology, 29(9), 6472-6484. https://doi.org/10.3390/curroncol29090509