Re-Irradiation for Recurrent Cervical Cancer: A State-of-the-Art Review


Abstract
1. Introduction
2. Brachytherapy
2.1. High-Dose-Rate ISBT (HDR-ISBT)
2.1.1. Efficacy
2.1.2. Prognostic Factors
2.1.3. Toxicity
2.1.4. OAR Dose Constraints
2.2. Permanent Radioactive Seed Implantation (PRSI)
3. SBRT

{kind=link}
{kind=link}
| Study | Nature of the Study | Cases with Previous Radiotherapy (Total) | Primary Tumor Site | Recurrent Tumor Site | Treatment Regimen | Median Re-Irradiation Dose (Gy) | Median GTV (cm3) | Local Control Outcomes | Other Outcomes | Toxicities | Prognostic Factors |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Park et al. (2015) [57] | Retrospective | 71 (85) | Cervix | Abdominopelvic lymph nodes | SBRT | Rx: 39 Gy/3 f (BED, 89.7 Gy) (44 cases) BED, 79.2 Gy (re-irradiation group) | n/s | 2-year LPFS 82.5% 5-year LPFS 78.8% | 2-year OS 57.5% 5-year OS 32.9% | Grade 3–4 late toxicity: n = 5 | BED ≥ 89.7 Gy and 69.3 Gy (LC) para-aortic LN vs. pelvic LN (LC) disease-free interval ≥ 36 months (LC, OS) |
| Seo et al. (2016) [55] | Retrospective | 17 (23) | Cervix | Pelvic sidewall | EBRT + SBRT boost + chemotherapy (7) SBRT + chemotherapy (14) SBRT (2) | Rx: 39 Gy (27–45 Gy)/3 f | 40 (2–215) | 2-year LPFS 65% | 2-year OS 43% 3-year OS 27% 2-year DPFS 52% | Grade 3–4 late toxicity: n = 3 | GTV < 50 cm3 (LC) GTV < 30 cm3 (OS) |
| Pontoriero et al. (2016) [58] | Retrospective | 5 (5) | Cervix | Central pelvis | SBRT | Rx: 15–20 Gy/3–4 f | 20 (8.2–47.4) | n/s | CR: n = 1 PR: n = 2 PD: n = 1 OC: n = 1 | Grade 3–4 late toxicity: n = 0 | n/s |
| Ling et al. (2019) [59] | Retrospective | 20 (20) | Cervix (6) Uterus (11) Vagina (1) Ovary (1) Vulva (1) | Pelvis (13) Para-aortic nodes (6) Celiac nodes (1) | SBRT ± chemotherapy (17) EBRT + SBRT boost ± chemotherapy (3) | Rx: 44.5 Gy (33.8–45 Gy) BED10, 82.7 Gy (64.1–85.5 Gy) | 9.7 (4.6–35.9) | 3-year LC 61.4% | 3-year DPFS 44.0% 3-year OS 51.9% | Grade 3–4 late toxicity: n = 3 | n/s |
4. Prospects
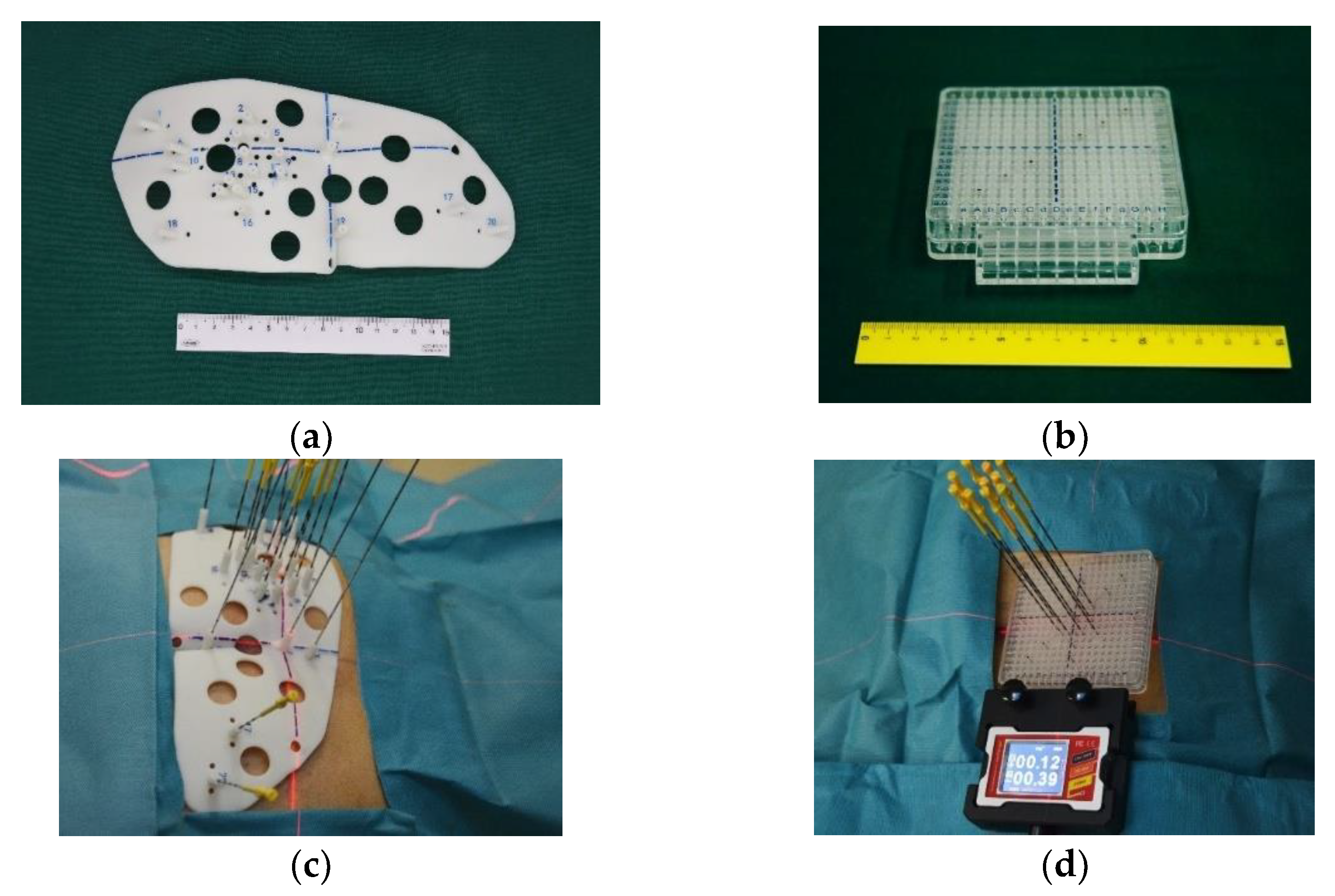
4.1. RISI-Assisted 3D Printed Template (RISI-3DPT)
4.2. Imaging Navigation System-Assisted RISI
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Cohen, P.A.; Jhingran, A.; Oaknin, A.; Denny, L. Cervical cancer. Lancet 2019, 393, 169–182. [Google Scholar] [CrossRef]
- Kasamatsu, T.; Onda, T.; Yamada, T.; Tsunematsu, R. Clinical aspects and prognosis of pelvic recurrence of cervical carcinoma. Int. J. Gynaecol. Obstet. 2005, 89, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Hockel, M.; Sclenger, K.; Hamm, H.; Knapstein, P.G.; Hohenfellner, R.; Rosler, H.P. Five-year experience with combined operative and radiotherapeutic treatment of recurrent gynecologic tumors infiltrating the pelvic wall. Cancer 1996, 77, 1918–1933. [Google Scholar] [CrossRef]
- Webb, M.J.; Symmonds, R.E. Site of recurrence of cervical cancer after radical hysterectomy. Am. J. Obstet. Gynecol. 1980, 138, 813–817. [Google Scholar] [CrossRef]
- Dornhofer, N.; Hockel, M. New developments in the surgical therapy of cervical carcinoma. Ann. N. Y. Acad. Sci. 2008, 1138, 233–252. [Google Scholar] [CrossRef] [PubMed]
- Boussios, S.; Seraj, E.; Zarkavelis, G.; Petrakis, D.; Kollas, A.; Kafantari, A.; Assi, A.; Tatsi, K.; Pavlidis, N.; Pentheroudakis, G. Management of patients with recurrent/advanced cervical cancer beyond first line platinum regimens: Where do we stand? A literature review. Crit. Rev. Oncol. Hematol. 2016, 108, 164–174. [Google Scholar] [CrossRef]
- Zanagnolo, V.; Ming, L.; Gadducci, A.; Maggino, T.; Sartori, E.; Zola, P.; Landoni, F. Surveillance procedures for patients with cervical carcinoma: A review of the literature. Int. J. Gynecol. Cancer 2009, 19, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Llewelyn, M.; Taylor, A. Re-irradiation of cervical and endometrial cancer. Curr. Opin. Oncol. 2017, 29, 343–350. [Google Scholar] [CrossRef]
- Nieder, C.; Milas, L.; Ang, K.K. Tissue tolerance to reirradiation. Semin. Radiat. Oncol. 2000, 10, 200–209. [Google Scholar] [CrossRef] [PubMed]
- Prisciandaro, J.I.; Zhao, X.; Dieterich, S.; Hasan, Y.; Jolly, S.; Al-Hallaq, H.A. Interstitial High-Dose-Rate Gynecologic Brachytherapy: Clinical Workflow Experience from Three Academic Institutions. Semin. Radiat. Oncol. 2020, 30, 29–38. [Google Scholar] [CrossRef]
- Prempree, T.; Amornmarn, R.; Villasanta, U.; Kwon, T.; Scott, R.M. Retreatment of very late recurrent invasive squamous cell carcinoma of the cervix with irradiation. II. Criteria for patients’ selection to achieve the success. Cancer 1984, 54, 1950–1955. [Google Scholar] [CrossRef]
- Haie-Meder, C.; Potter, R.; Van Limbergen, E.; Briot, E.; De Brabandere, M.; Dimopoulos, J.; Dumas, I.; Hellebust, T.P.; Kirisits, C.; Lang, S.; et al. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group (I): Concepts and terms in 3D image based 3D treatment planning in cervix cancer brachytherapy with emphasis on MRI assessment of GTV and CTV. Radiother. Oncol. 2005, 74, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Potter, R.; Haie-Meder, C.; Van Limbergen, E.; Barillot, I.; De Brabandere, M.; Dimopoulos, J.; Dumas, I.; Erickson, B.; Lang, S.; Nulens, A.; et al. Recommendations from gynaecological (GYN) GEC ESTRO working group (II): Concepts and terms in 3D image-based treatment planning in cervix cancer brachytherapy-3D dose volume parameters and aspects of 3D image-based anatomy, radiation physics, radiobiology. Radiother. Oncol. 2006, 78, 67–77. [Google Scholar] [CrossRef]
- Hellebust, T.P.; Kirisits, C.; Berger, D.; Perez-Calatayud, J.; De Brabandere, M.; De Leeuw, A.; Dumas, I.; Hudej, R.; Lowe, G.; Wills, R.; et al. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group: Considerations and pitfalls in commissioning and applicator reconstruction in 3D image-based treatment planning of cervix cancer brachytherapy. Radiother. Oncol. 2010, 96, 153–160. [Google Scholar] [CrossRef]
- Dimopoulos, J.C.; Petrow, P.; Tanderup, K.; Petric, P.; Berger, D.; Kirisits, C.; Pedersen, E.M.; van Limbergen, E.; Haie-Meder, C.; Potter, R. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group (IV): Basic principles and parameters for MR imaging within the frame of image based adaptive cervix cancer brachytherapy. Radiother. Oncol. 2012, 103, 113–122. [Google Scholar] [CrossRef]
- Schmid, M.P.; Fokdal, L.; Westerveld, H.; Chargari, C.; Rohl, L.; Morice, P.; Nesvacil, N.; Mazeron, R.; Haie-Meder, C.; Potter, R.; et al. Recommendations from gynaecological (GYN) GEC-ESTRO working group—ACROP: Target concept for image guided adaptive brachytherapy in primary vaginal cancer. Radiother. Oncol. 2020, 145, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Zolciak-Siwinska, A.; Bijok, M.; Jonska-Gmyrek, J.; Kawczynska, M.; Kepka, L.; Bujko, K.; Michalski, W. HDR brachytherapy for the reirradiation of cervical and vaginal cancer: Analysis of efficacy and dosage delivered to organs at risk. Gynecol. Oncol. 2014, 132, 93–97. [Google Scholar] [CrossRef]
- Mabuchi, S.; Takahashi, R.; Isohashi, F.; Yokoi, T.; Okazawa, M.; Sasano, T.; Maruoka, S.; Anzai, M.; Yoshioka, Y.; Ogawa, K.; et al. Reirradiation using high-dose-rate interstitial brachytherapy for locally recurrent cervical cancer: A single institutional experience. Int. J. Gynecol. Cancer 2014, 24, 141–148. [Google Scholar] [CrossRef]
- Mahantshetty, U.; Kalyani, N.; Engineer, R.; Chopra, S.; Jamema, S.; Ghadi, Y.; Deshpande, D.; Shrivastava, S. Reirradiation using high-dose-rate brachytherapy in recurrent carcinoma of uterine cervix. Brachytherapy 2014, 13, 548–553. [Google Scholar] [CrossRef] [PubMed]
- Umezawa, R.; Murakami, N.; Nakamura, S.; Wakita, A.; Okamoto, H.; Tsuchida, K.; Kashihara, T.; Kobayashi, K.; Harada, K.; Takahashi, K.; et al. Image-guided interstitial high-dose-rate brachytherapy for locally recurrent uterine cervical cancer: A single-institution study. Brachytherapy 2018, 17, 368–376. [Google Scholar] [CrossRef] [PubMed]
- da Silva, V.T.M.; Fortuna Diniz, A.P.; Martins, J.; Cursino, K.; Esteves, S.C.B.; Teixeira, J.C. Use of interstitial brachytherapy in pelvic recurrence of cervical carcinoma: Clinical response, survival, and toxicity. Brachytherapy 2019, 18, 146–153. [Google Scholar] [CrossRef]
- Raziee, H.; D’Souza, D.; Velker, V.; Barnes, E.; Taggar, A.; Mendez, L.; Leung, E. Salvage Re-irradiation With Single-modality Interstitial Brachytherapy for the Treatment of Recurrent Gynaecological Tumours in the Pelvis: A Multi-institutional Study. Clin. Oncol. 2020, 32, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Jiang, P.; Qu, A.; Wei, S.; Sun, H.; Zhang, X.; Li, X.; Wang, J. The Preliminary Results of 3-Dimensional Printed Individual Template Assisted 192Ir High-Dose Rate Interstitial Brachytherapy for Central Recurrent Gynecologic Cancer. Technol. Cancer Res. Treat. 2020, 19, 1533033820971607. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.S.; Guo, J.; Zhao, Y.Z.; Lin, X.; Chen, B.; Zhang, M.; Li, J.M.; Ren, X.J.; Zhang, B.Y.; Wang, T.J. Salvage interstitial brachytherapy based on computed tomography for recurrent cervical cancer after radical hysterectomy and adjuvant radiation therapy: Case presentations and introduction of the technique. J. Contemp. Brachytherapy 2016, 8, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Randall, M.E.; Evans, L.; Greven, K.M.; McCunniff, A.J.; Doline, R.M. Interstitial reirradiation for recurrent gynecologic malignancies: Results and analysis of prognostic factors. Gynecol. Oncol. 1993, 48, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Badakh, D.K.; Grover, A.H. Reirradiation with high-dose-rate remote afterloading brachytherapy implant in patients with locally recurrent or residual cervical carcinoma. J. Cancer Res. Ther. 2009, 5, 24–30. [Google Scholar] [CrossRef]
- Charra, C.; Roy, P.; Coquard, R.; Romestaing, P.; Ardiet, J.M.; Gerard, J.P. Outcome of treatment of upper third vaginal recurrences of cervical and endometrial carcinomas with interstitial brachytherapy. Int. J. Radiat. Oncol. Biol. Phys. 1998, 40, 421–426. [Google Scholar] [CrossRef]
- Chopra, S.; Engineer, R.; Shah, S.; Shukla, R.; Dora, T.; Gupta, P.; Paul, S.N.; Popat, P.; Swamidas, J.; Mahantshetty, U.; et al. MRI- and PET-Guided Interstitial Brachytherapy for Postsurgical Vaginal Recurrences of Cervical Cancer: Results of Phase II Study. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 310–319. [Google Scholar] [CrossRef]
- Amsbaugh, M.J.; Bhatt, N.; Hunter, T.; Gaskins, J.; Parker, L.; Metzinger, D.; Amsbaugh, A.; Sowards, K.; El-Ghamry, M. Computed tomography planned interstitial brachytherapy for recurrent gynecologic cancer. Brachytherapy 2015, 14, 600–605. [Google Scholar] [CrossRef]
- Martinez-Monge, R.; Cambeiro, M.; Rodriguez-Ruiz, M.E.; Olarte, A.; Ramos, L.I.; Villafranca, E.; Bascon, N.; Jurado, M. Phase II trial of image-based high-dose-rate interstitial brachytherapy for previously irradiated gynecologic cancer. Brachytherapy 2014, 13, 219–224. [Google Scholar] [CrossRef]
- Abusaris, H.; Storchi, P.R.; Brandwijk, R.P.; Nuyttens, J.J. Second re-irradiation: Efficacy, dose and toxicity in patients who received three courses of radiotherapy with overlapping fields. Radiother. Oncol. 2011, 99, 235–239. [Google Scholar] [CrossRef]
- Bockel, S.; Espenel, S.; Sun, R.; Dumas, I.; Gouy, S.; Morice, P.; Chargari, C. Image-Guided Brachytherapy for Salvage Reirradiation: A Systematic Review. Cancers 2021, 13, 1226. [Google Scholar] [CrossRef]
- Sturdza, A.; Viswanathan, A.N.; Erickson, B.; Yashar, C.; Bruggeman, A.; Feddock, J.; Klopp, A.; Beriwal, S.; Gaffney, D.; Han, K.; et al. American Brachytherapy Society working group report on the patterns of care and a literature review of reirradiation for gynecologic cancers. Brachytherapy 2020, 19, 127–138. [Google Scholar] [CrossRef]
- Williamson, J.F. Brachytherapy technology and physics practice since 1950: A half-century of progress. Phys. Med. Biol. 2006, 51, R303–R325. [Google Scholar] [CrossRef]
- Armpilia, C.I.; Dale, R.G.; Coles, I.P.; Jones, B.; Antipas, V. The determination of radiobiologically optimized half-lives for radionuclides used in permanent brachytherapy implants. Int. J. Radiat. Oncol. 2003, 55, 378–385. [Google Scholar] [CrossRef]
- Williamson, J.F.; Butler, W.; DeWerd, L.A.; Huq, M.S.; Ibbott, G.S.; Li, Z.; Mitch, M.G.; Nath, R.; Rivard, M.J.; Todor, D. Recommendations of the American Association of Physicists in Medicine regarding the impact of implementing the 2004 task group 43 report on dose specification for Pd-103 and I-125 interstitial brachytherapy. Med. Phys. 2005, 32, 1424–1439. [Google Scholar] [CrossRef]
- Todor, D.A.; Barani, I.J.; Lin, P.S.; Anscher, M.S. Moving toward focal therapy in prostate cancer: Dual-isotope permanent seed implants as a possible solution. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 297–304. [Google Scholar] [CrossRef]
- Chen, Z.; Nath, R. Biologically effective dose (BED) for interstitial seed implants containing a mixture of radionuclides with different half-lives. Int. J. Radiat. Oncol. Biol. Phys. 2003, 55, 825–834. [Google Scholar] [CrossRef]
- Knaup, C.; Mavroidis, P.; Esquivel, C.; Stathakis, S.; Swanson, G.; Papanikolaou, N. SU-E-T-458: Radiobiological Comparison of Single and Dual-Isotope Prostate Seed Implants. Med. Phys. 2012, 39, 3810. [Google Scholar] [CrossRef][Green Version]
- Cao, Q.; Wang, H.; Meng, N.; Jiang, Y.; Jiang, P.; Gao, Y.; Tian, S.; Liu, C.; Yang, R.; Wang, J.; et al. CT-guidance interstitial 125Iodine seed brachytherapy as a salvage therapy for recurrent spinal primary tumors. Radiat. Oncol. 2014, 9, 301. [Google Scholar] [CrossRef]
- Jiang, P.; Liu, C.; Wang, J.; Yang, R.; Jiang, Y.; Tian, S. Computed tomography (CT)-guided interstitial permanent implantation of 125I seeds for refractory chest wall metastasis or recurrence. Technol. Cancer Res. Treat. 2015, 14, 11–18. [Google Scholar] [CrossRef]
- Chen, Y.; Jiang, Y.; Ji, Z.; Jiang, P.; Xu, F.; Zhang, Y.; Guo, F.; Peng, R.; Li, X.; Sun, H.; et al. Efficacy and safety of CT-guided 125I seed implantation as a salvage treatment for locally recurrent head and neck soft tissue sarcoma after surgery and external beam radiotherapy: A 12-year study at a single institution. Brachytherapy 2020, 19, 81–89. [Google Scholar] [CrossRef]
- Wang, L.; Wang, H.; Jiang, Y.; Ji, Z.; Guo, F.; Jiang, P.; Li, X.; Chen, Y.; Sun, H.; Fan, J.; et al. The efficacy and dosimetry analysis of CT-guided 125I seed implantation assisted with 3D-printing non-co-planar template in locally recurrent rectal cancer. Radiat. Oncol. 2020, 15, 179. [Google Scholar] [CrossRef]
- Sharma, S.K.; Forgione, H.; Isaacs, J.H. Iodine-125 interstitial implants as salvage therapy for recurrent gynecologic malignancies. Cancer 1991, 67, 2467–2471. [Google Scholar] [CrossRef]
- Jiang, P.; Zou, L.; Wei, L.; Cheng, G.; Sun, B.; Zhang, F.; Wang, R.; Wang, T.; Qu, A.; Yuan, X.; et al. Chinese Expert Consensus on Iodine125 Seed Implantation for Recurrent Cervical Cancer in 2021. Front. Oncol. 2021, 11, 700710. [Google Scholar] [CrossRef]
- Tong, L.; Liu, P.; Huo, B.; Guo, Z.; Ni, H. CT-guided 125I interstitial brachytherapy for pelvic recurrent cervical carcinoma after radiotherapy. OncoTargets Ther. 2017, 10, 4081–4088. [Google Scholar] [CrossRef]
- Qu, A.; Jiang, P.; Sun, H.; Jiang, W.; Jiang, Y.; Tian, S.; Wang, J. Efficacy and dosimetry analysis of image-guided radioactive 125I seed implantation as salvage treatment for pelvic recurrent cervical cancer after external beam radiotherapy. J. Gynecol. Oncol. 2019, 30, e9. [Google Scholar] [CrossRef]
- Liu, Y.; Jiang, P.; Zhang, H.; Wang, J. Safety and efficacy of 3D-printed templates assisted CT-guided radioactive iodine-125 seed implantation for the treatment of recurrent cervical carcinoma after external beam radiotherapy. J. Gynecol. Oncol. 2021, 32, e15. [Google Scholar] [CrossRef]
- Han, L.; Li, C.L.; Wang, J.Y.; He, X.Q.; Zhang, X.; Yang, J.D.; Liu, G.F. Iodine-125 radioactive seed tissue implantation as a remedy treatment for recurrent cervical cancer. J. Cancer Res. Ther. 2016, 12, C176–C180. [Google Scholar] [CrossRef]
- Chen, Y.; Jiang, Y.; Ji, Z.; Jiang, P.; Xu, F.; Zhang, Y.; Zhang, P.; Guo, F.; Li, X.; Sun, H.; et al. Dosimetry, efficacy, and safety of three-dimensional printing noncoplanar template-assisted and CT-guided 125I seed implantation for recurrent retroperitoneal lymphatic metastasis after external beam radiotherapy. Brachytherapy 2020, 19, 380–388. [Google Scholar] [CrossRef]
- Guckenberger, M.; Bachmann, J.; Wulf, J.; Mueller, G.; Krieger, T.; Baier, K.; Richter, A.; Wilbert, J.; Flentje, M. Stereotactic body radiotherapy for local boost irradiation in unfavourable locally recurrent gynaecological cancer. Radiother. Oncol. 2010, 94, 53–59. [Google Scholar] [CrossRef]
- Higginson, D.S.; Morris, D.E.; Jones, E.L.; Clarke-Pearson, D.; Varia, M.A. Stereotactic body radiotherapy (SBRT): Technological innovation and application in gynecologic oncology. Gynecol. Oncol. 2011, 120, 404–412. [Google Scholar] [CrossRef]
- Hsieh, C.H.; Tien, H.J.; Hsiao, S.M.; Wei, M.C.; Wu, W.Y.; Sun, H.D.; Wang, L.Y.; Hsieh, Y.P.; Chen, Y.J.; Shueng, P.W. Stereotactic body radiation therapy via helical tomotherapy to replace brachytherapy for brachytherapy-unsuitable cervical cancer patients—A preliminary result. OncoTargets Ther. 2013, 6, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Deodato, F.; Macchia, G.; Grimaldi, L.; Ferrandina, G.; Lorusso, D.; Salutari, V.; Cilla, S.; Valentini, V.; Cellini, N.; Piermattei, A.; et al. Stereotactic radiotherapy in recurrent gynecological cancer: A case series. Oncol. Rep. 2009, 22, 415–419. [Google Scholar] [PubMed]
- Seo, Y.; Kim, M.S.; Yoo, H.J.; Jang, W.I.; Rhu, S.Y.; Choi, S.C.; Kim, M.H.; Kim, B.J.; Lee, D.H.; Cho, C.K. Salvage stereotactic body radiotherapy for locally recurrent uterine cervix cancer at the pelvic sidewall: Feasibility and complication. Asia Pac. J. Clin. Oncol. 2016, 12, e280–e288. [Google Scholar] [CrossRef]
- Hasan, S.; Ricco, A.; Jenkins, K.; Lanciano, R.; Hanlon, A.; Lamond, J.; Yang, J.; Feng, J.; Good, M.; Noumoff, J.; et al. Survival and Control Prognosticators of Recurrent Gynecological Malignancies of the Pelvis and Para-aortic Region Treated with Stereotactic Body Radiation Therapy. Front. Oncol. 2016, 6, 249. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Chang, A.R.; Seo, Y.; Cho, C.K.; Jang, W.I.; Kim, M.S.; Choi, C. Stereotactic Body Radiotherapy for Recurrent or Oligometastatic Uterine Cervix Cancer: A Cooperative Study of the Korean Radiation Oncology Group (KROG 14-11). Anticancer Res. 2015, 35, 5103–5110. [Google Scholar]
- Pontoriero, A.; Iati, G.; Aiello, D.; Pergolizzi, S. Stereotactic Radiotherapy in the Retreatment of Recurrent Cervical Cancers, Assessment of Toxicity, and Treatment Response: Initial Results and Literature Review. Technol. Cancer Res. Treat. 2016, 15, 759–765. [Google Scholar] [CrossRef]
- Ling, D.C.; Vargo, J.A.; Burton, S.A.; Heron, D.E.; Beriwal, S. Salvage Curative-Intent Reirradiation Stereotactic Body Radiation Therapy for Isolated Pelvic and/or Paraortic Recurrences of Gynecologic Malignancies. Pr. Radiat Oncol. 2019, 9, 418–425. [Google Scholar] [CrossRef]
- Mendez, L.C.; Leung, E.; Cheung, P.; Barbera, L. The Role of Stereotactic Ablative Body Radiotherapy in Gynaecological Cancers: A Systematic Review. Clin. Oncol. 2017, 29, 378–384. [Google Scholar] [CrossRef]
- Leung, E.; Gladwish, A.; Sahgal, A.; Lo, S.S.; Kunos, C.A.; Lanciano, R.M.; Mantz, C.A.; Guckenberger, M.; Zagar, T.M.; Mayr, N.A.; et al. Survey of current practices from an international task force for gynecological stereotactic ablative radiotherapy. Radiat. Oncol. 2020, 15, 24. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.W.; Palma, D.; D’Souza, D.; Velker, V.; Mendez, L.C. Stereotactic Ablative Radiotherapy for Recurrent or Metastatic Gynecological Cancer: Extending Lives? Curr. Treat. Options Oncol. 2020, 21, 58. [Google Scholar] [CrossRef]
- Chiantera, V.; Rossi, M.; De Iaco, P.; Koehler, C.; Marnitz, S.; Fagotti, A.; Fanfani, F.; Parazzini, F.; Schiavina, R.; Scambia, G.; et al. Morbidity after pelvic exenteration for gynecological malignancies: A retrospective multicentric study of 230 patients. Int. J. Gynecol. Cancer 2014, 24, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhang, F.; Guo, J.; Chai, S.; Zheng, G.; Zhang, K.; Liao, A.; Jiang, P.; Jiang, Y.; Ji, Z. Expert consensus workshop report: Guideline for three-dimensional printing template-assisted computed tomography-guided 125I seeds interstitial implantation brachytherapy. J. Cancer Res. Ther. 2017, 13, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Lu, J.; Chen, K.M.; Wu, Z.Y.; Wang, Q.B.; Liu, J.J.; Gong, J.; Chen, Z.J.; Ding, X.Y.; Wang, Z.M. Preliminary application of 3D-printed coplanar template for iodine-125 seed implantation therapy in patients with advanced pancreatic cancer. World J. Gastroenterol. 2018, 24, 5280–5287. [Google Scholar] [CrossRef] [PubMed]
- Zhao, G.S.; Liu, S.; Yang, L.; Li, C.; Wang, R.Y.; Zhou, J.; Zhang, Y.W. Evaluation of radioactive 125I seed implantation for the treatment of refractory malignant tumours based on a CT-guided 3D template-assisted technique: Efficacy and safety. BMC Cancer 2020, 20, 718. [Google Scholar] [CrossRef]
- Jiang, W.; Jiang, P.; Wei, S.; Jiang, Y.; Ji, Z.; Sun, H.; Fan, J.; Li, W.; Shao, Y.; Wang, J. The accuracy and safety of CT-guided iodine-125 seed implantation assisted by 3D non-coplanar template for retroperitoneal recurrent carcinoma. World J. Surg. Oncol. 2020, 18, 307. [Google Scholar] [CrossRef]
- Chen, E.; Zhang, Y.; Zhang, H.; Jia, C.; Liang, Y.; Wang, J. Dosimetry study of three-dimensional print template for 125I implantation therapy. Radiat. Oncol. 2021, 16, 115. [Google Scholar] [CrossRef] [PubMed]
- Qu, A.; Jiang, P.; Wei, S.; Jiang, Y.; Ji, Z.; Sun, H.; Li, W.; Shao, Y.; Fan, J.; Wang, J. Accuracy and dosimetric parameters comparison of 3D-printed non-coplanar template-assisted computed tomography-guided iodine-125 seed ablative brachytherapy in pelvic lateral recurrence of gynecological carcinomas. J. Contemp. Brachytherapy 2021, 13, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.H.; Lv, X.M.; Wu, W.J.; Wu, Z.Y.; Zheng, L.; Huang, M.W.; Wang, Y.; Zhang, J.G. Evaluation of the accuracy of computer-assisted techniques in the interstitial brachytherapy of the deep regions of the head and neck. Brachytherapy 2019, 18, 217–223. [Google Scholar] [CrossRef]
- Wei, S.; Li, C.; Li, M.; Xiong, Y.; Jiang, Y.; Sun, H.; Qiu, B.; Lin, C.J.; Wang, J. Radioactive Iodine-125 in Tumor Therapy: Advances and Future Directions. Front. Oncol. 2021, 11, 717180. [Google Scholar] [CrossRef] [PubMed]
- Ji, Z.; Jiang, Y.; Sun, H.; Chen, Y.; Guo, F.; Fan, J.; Wang, J. 3D-printed template and optical needle navigation in CT-guided iodine-125 permanent seed implantation. J. Contemp. Brachytherapy 2021, 13, 410–418. [Google Scholar] [CrossRef] [PubMed]


| Study | Cases with Previous RT (Total) | Primary Tumor Site (Case Number) | Treatment Regimen | Delivered Dose (Gy) | Local Control Outcomes | Other Outcomes | Toxicities | Prognostic Factors |
|---|---|---|---|---|---|---|---|---|
| Zolciak-Siwinska et al. (2014) [17] | 20 (20) | Cervix (19) + Vagina (1) | HDR BT alone (17) HDR BT + EBRT (2) HDR BT + EBRT + chemotherapy (1) | Re-irradiation EQD2: 48.8 Gy (16–91 Gy) Cumulative EQD2: 133.5 Gy (96.8–164.2 Gy) | 3-year LC 45% | 3-year OS 68% 3-year DFS 45% | Grade 3 late toxicity: n = 3 | Interval between radiations ≤ 12 months (LC, OS, DFS) Tumor diameter> 3 cm (LC, OS, DFS) |
| Mabuchi et al. (2014) [18] | 52 (52) | Cervix | HDR ISBT | Rx: 42 Gy/7 f | Response rate 76.9% | Median OS 32 m Estimated 5-year OS 52.6% | Grade 3–4 late toxicity: n = 13 | Tumor diameter ≥ 4 cm (OS) Primary tumor FIGO staging III–IV (OS) DFI ≤ 6 months (OS) |
| Mahantshetty et al. (2014) [19] | 30 (30) | Cervix | HDR ISBT alone (24) Intracavitary HDR BT alone (6) | EQD2: 42 Gy (37–46 Gy) | 2-year LC 44% | 2-year DFS 42% 2-year OS 52% | 2-year Grade 3 toxicity rate: 23% | Re-irradiation dose < 40 Gy EQD2 (LC) |
| Umezawa et al. (2018) [20] | 18 (18) | Cervix | HDR ISBT alone (13) EBRT + HDR ISBT (5) | EQD2: 62.5 Gy (48.6–82.5 Gy) | 2-year LC 51.8% | 2-year PFS 20% 2-year OS 60.8% | Grade 3–4 late toxicity: n = 3 | Hemoglobin level < 12.5 g/dL (LC) Tumor diameter ≥ 40 mm (LC) |
| Silva et al. (2019) [21] | 45 (45) | Cervix | HDR ISBT ± EBRT (4) ± chemotherapy (13) | Rx: 40–60 Gy/4–6 f | CR rate 67% | 1-year OS 71% 5-year OS 52% 5-year DFS (patients with CR) 45% | Grade 3–4 late toxicity: n = 15 | - |
| Raziee et al. (2020) [22] | 26 (26) | Endometrium (20) Cervix (4) Vulva (1) Vagina (1) | HDR ISBT | EQD2: 29.1 Gy (16.1–64.6 Gy) | 2-year LC 50% | 2-year PFS 38% 2-year OS 78% | Grade 3 late toxicity: n = 2 | - |
| Jiang et al. (2020) [23] | 27 (32) | Cervix (17) Endometrium (5) Vagina (6) Ovary (3) Vulva (1) | HDR ISBT | Rx: 10–36 Gy, 5–6 Gy/f, 2–6 f | 1-year LC 51.7% | Median TTF 15.4 months | Grade 3–4 late toxicity: n = 3 | - |
| Study | Cases with Previous RT (Total) | Primary Tumor Site | Recurrent Tumor Site | Interval between Radiations (Month) | Treatment Regimen | Re-Irradiation Dose (Gy) | Tumor Size | Median Seeds Number | Median Follow-Up Time | Local Control Outcomes | Other Outcomes | Toxicities | Prognostic Factors |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lei et al. (2017) [49] | 17 (17) | Cervix | Cervix Vaginal cuff Pelvic LNs Extra-pelvis | n/s | CT-guided 125I seed implantation ± chemotherapy | Matched peripheral dose: 145 Gy | 0.5 × 0.5 cm–5 × 6 cm | 20 (6–68) | 9.5 (4–18) | Overall response rate 58% | 1-year OS 18.3% | Grade 3–4 late toxicity: n = 0 | n/s |
| Tong et al. (2017) [46] | 33 (33) | Cervix | Cervix | n/s | CT-guided 125I seed implantation + chemotherapy | Rx: 90–150 Gy | n/s | 50 (20–95) | 16 | 1-year LC 55.5% | 1-year OS 65.5% 2-year OS 43.6% | Grade 3–4 late toxicity: n = 2 | Tumor diameter < 4 cm (LC) D90 ≥ 130 Gy (LC) Good performance status (OS) |
| Qu et al. (2019) [47] | 36 (36) | Cervix | Pelvic Sidewall (21) Central Pelvis (15) | 12 (2–60) | CT-guided 125I seed implantation | GTV D90: 128.5 ± 47.4 Gy | 59.2 cm3 (2.5–116.5 cm3) | 62.5 (10–140) | 11.5 (2–30) | 1-year LPFS 34.9% 2-year LPFS 20% | 1-year OS 52% 2-year OS 19.6% | Grade 3–4 late toxicity: n = 1 | Pathological type (OS) recurrence site (OS, LPFS) lesion volume (LPFS) D90 ≥ 105 Gy (LPFS) |
| Liu et al. (2019) [48] | 103 (103) | Cervix | Pelvic Sidewall (75) Central Pelvis (8) Extra Pelvis | 11 (2–70) | 3D-PNCT assisted CT-guided 125I seed implantation | Rx: 120 Gy (100–180 Gy) | GTV 37.7 cm3 (2.6–237.8 cm3) | 63 (8–186) | 12 (2–43) | 1-year LC 87.4% 3-year LC 75.1% | 1-year OS 68.1% 3-year OS 20.8% | Grade 3–4 late toxicity: n = 2 | Pathological type (LC, OS) Hemoglobin level (LC, OS) D90 ≥ 130 Gy (LC, OS) Recurrence site (OS) |
| Chen et al. (2020) [50] | 23 (32) | Cervix (11) Non-Cervix (21) | Retroperitoneal lymph nodes | n/s | 3D-PNCT assisted CT-guided 125I seed implantation | Rx: 140 Gy (115–160 Gy) | n/s | 62.5 (15–197) | 15.3 (9.2–33.5) | 1-year LC 66.2% 2-year LC 43.2% | 1-year OS 74.1% | Grade 3–4 late toxicity: n = 0 | Univariate analysis: Tumor size ≤ 49.8 cm3, D90 < 130 Gy or D100 < 63 Gy (LC) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, Z.; Qu, A.; Jiang, P.; Jiang, Y.; Sun, H.; Wang, J. Re-Irradiation for Recurrent Cervical Cancer: A State-of-the-Art Review. Curr. Oncol. 2022, 29, 5262-5277. https://doi.org/10.3390/curroncol29080418
Shen Z, Qu A, Jiang P, Jiang Y, Sun H, Wang J. Re-Irradiation for Recurrent Cervical Cancer: A State-of-the-Art Review. Current Oncology. 2022; 29(8):5262-5277. https://doi.org/10.3390/curroncol29080418
Chicago/Turabian StyleShen, Zongyan, Ang Qu, Ping Jiang, Yuliang Jiang, Haitao Sun, and Junjie Wang. 2022. "Re-Irradiation for Recurrent Cervical Cancer: A State-of-the-Art Review" Current Oncology 29, no. 8: 5262-5277. https://doi.org/10.3390/curroncol29080418
APA StyleShen, Z., Qu, A., Jiang, P., Jiang, Y., Sun, H., & Wang, J. (2022). Re-Irradiation for Recurrent Cervical Cancer: A State-of-the-Art Review. Current Oncology, 29(8), 5262-5277. https://doi.org/10.3390/curroncol29080418