The Transformation of Adolescent and Young Adult Oncological and Supportive Care in Canada: A Mixed Methods Study

 ,
,  ,
,
Abstract
1. Introduction
2. Methods
2.1. Study Participants and Setting
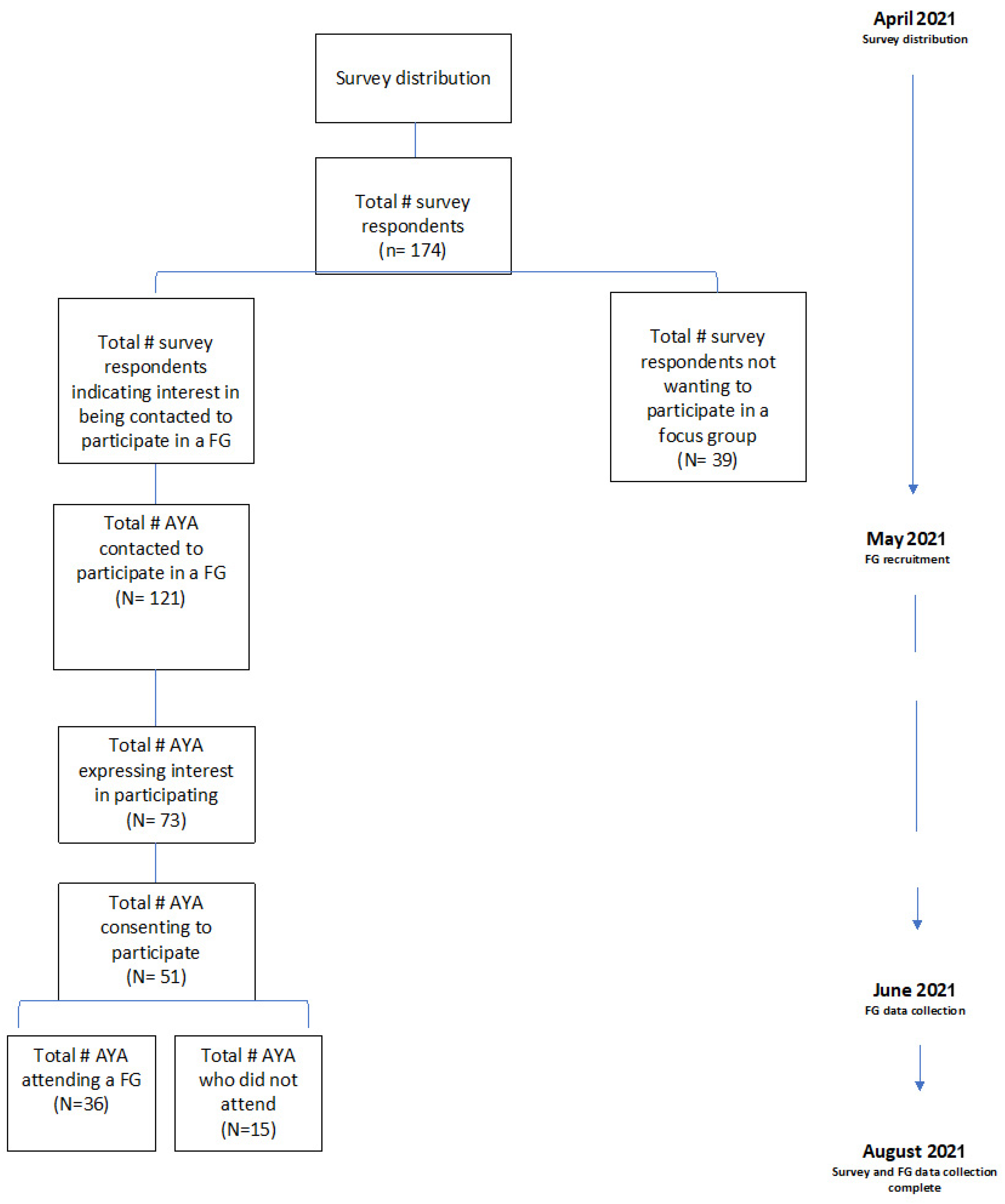
2.2. Survey—Recruitment, Execution, Analysis
2.3. Focus Groups
3. Results
3.1. Theme 1: The Need for AYA Relevant and Timely Information about Future Health Risks
- (a)
- Producing health risk-related content with the AYA life stage in mind
- (b)
- Having a guide to help AYAs anticipate what they may experience next
- (c)
- Providing checklists to help AYAs navigate the experience
3.2. Theme 2: The Need for Tailored and Timely Supportive Care
- (a)
- The need for ongoing check-ins to keep up with shifting needs
- (b)
- Receiving navigation support
3.3. Theme 3: Need for Enhanced Connections
- (a)
- A space to gather, connect, and seek mentorship
- (b)
- A hub to access information
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

References
- Canadian Partnership Against Cancer. Adolescents & Young Adults with Cancer: A Systems Performance Report; Canadian Partnership Against Cancer: Toronto, ON, Canada, 2017. [Google Scholar]
- Schrijvers, D.; Meijnders, P. Palliative care in adolescents. Cancer Treat. Rev. 2007, 33, 616–621. [Google Scholar] [CrossRef] [PubMed]
- Filder, M.M.; Frobisher, C.; Hawkins, M.M.; Nathan, P.C. Challenges and opportunities in the care of survivors of adolescent and young adult cancers. Pediatr. Blood Cancer. 2019, 66, e27668. [Google Scholar]
- Gupta, A.; Papadakos, J.K.; Jones, J.M.; Amin, L.; Chang, E.K.; Korenblum, C.; Santa Mina, D.; McCabe, L.; Mitchell, L.; Giuliani, M.E. Reimagining care for adolescent and young adult cancer programs: Moving with the times. Cancer 2016, 122, 1038–1046. [Google Scholar] [CrossRef] [PubMed]
- Vora, T.; Chapman, S.; Uppal, S.; Shanawaz, S.; Emanuele, C.; Gupta, A.; Avery, J. Preliminary findings of focus group analysis to support the needs of adolescent and young adult patient and survivors of cancer: Steps toward a national adolescent and young adult supportive care program. J. Adolesc. Young Adult Oncol. 2021. online ahead of print. [Google Scholar]
- Sutcliffe, S.B. A Review of Canadian Health Care and Cancer Care Systems. Cancer 2011, 117 (Suppl. S10), 2241–2244. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Hart, R.; Cowie, F.C.; Jesudason, A.B.; Lawton, J. Adolescents and young adults’ (AYA) views on their cancer knowledge prior to diagnosis: Findings from a qualitative study involving AYA receiving cancer care. Health Expect. 2021, 24, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Baird, H.; Patterson PMedlow, S.; Allison, K.R. Understanding and improving survivorship care for adolescents and young adults with cancer. J. Adolesc. Young Adult Oncol. 2019, 8, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Li, W.; Wen, Y.; Wang, H.; Hengwen, S.; Liang, W.; Zhang, B.; Humphris, G. Fear of cancer recurrence in adolescent and young adult cancer survivors: A systematic review of the literature. Psycho-Oncol. 2019, 28, 675–686. [Google Scholar] [CrossRef] [PubMed]
- Kathrine FVandraas, K.F.; Reinertsen, K.V.; Kiserud, C.E.; Lie, H.C. Fear of cancer recurrence among young adult cancer survivors—exploring long-term contributing factors in a large, population-based cohort. J. Cancer Surviv. 2021, 15, 497–508. [Google Scholar]
- Wilder Smith, A.; Keegan, T.; Hamilton, A.; Lynch, C.; Wu, X.C.; Schwartz, S.M.; Kato, I.; Cress, R.; Harlan, L. AYA HOPE Study Collaborative Group. Understanding care and outcomes in adolescents and young adults with cancer: A review of the AYA HOPE study. Pediatr. Blood Cancer 2019, 66, e27486. [Google Scholar] [CrossRef] [PubMed]
- Ryder-Burbidge, C.; Diaz, R.L.; Barr, R.D.; Gupta, S.; Nathan, P.C.; McKillop, S.J.; Fidler-Benaoudia, M.M. The burden of late effects and related risk factors in adolescent and young adult cancer survivors: A scoping review. Cancers 2021, 13, 4870. [Google Scholar] [CrossRef] [PubMed]
- Perez, G.K.; Salsman, J.M.; Fladeboe, K.; Kirchhoff, A.C.; Park, E.R.; Rosenberg, A.R. Taboo Topics in Adolescent and Young Adult Oncology: Strategies for Managing Challenging but Important Conversations Central to Adolescent and Young Adult Cancer Survivorship. Am. Soc. Clin. Oncol. Educ. Book 2020, 40, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Rehberg, K.; Fleischmann, A.; Silber, E.; O’neill, S.C.; Lewis, F.M.; Tercyak, K.P. Facilitators of peer coaching/support engagement and dissemination among women at risk for and surviving with breast cancer. Transl. Behav. Med. 2021, 11, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.; Bruera, E. The Edmonton Symptom Assessment System 25 Years Later: Past, Present, and Future Developments. J. Pain Symptom. Manag. 2017, 53, 630. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Macedo, A.; Crawford, S.; Bagha, S.; Leung, Y.; Zimmermann, C.; Fitzgerald, B.; Wyatt, M.; Stuart-McEwan, T.; Rodin, G. Easier Said Than Done: Keys to successful implementation of the distress assessment and response tool (DART) program. J. Oncol. Prac. 2016, 12, e513–e526. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.Y.; Hoehn, K.S.; Hanson, C.; Monick, S.; Hlubocky, F.J.; McNeer, J.L. Integration and feasibility of symptom burden assessment and early palliative care into an adolescent and young adult leukemia clinic. J. Clin. Oncol. 2021, 39 (Suppl. S15), 10052. [Google Scholar] [CrossRef]
- Lazard, A.J.; Collins, M.K.R.; Hedrick, A.; Varma, T.; Love, B.; Valle, C.G.; Brooks, E.; Benedict, C. Using social media for peer-to-peer cancer support: Interviews with young adults with cancer. JMIR Cancer 2021, 7, e28234. [Google Scholar] [CrossRef]
- Griffiths, C.; Panteli, N.; Brunton, D.; Marder, B.; Williamson, H. Designing and evaluating the acceptability of Realshare: An online support community for teenagers and young adults with cancer. J. Health Psychol. 2015, 20, 1589–1601. [Google Scholar] [CrossRef] [PubMed]
- Yan, A.; Howden, K.; Mahar, A.L.; Scott, I.; Glidden, C.; Deleemans, J.; Chalifour, K.; Eaton, G.; Gupta, A.; Bolton, J.M.; et al. Experiences of adolescent and young adult cancer survivors during the COVID-19 pandemic. J. Cancer Surviv. 2022. online ahead of print. [Google Scholar]
- Varcoe, C.; Habib, S.; Sinding, C.; Fitch, M.; Gullatte, M.M.; Cummings, G.G. Health disparities in cancer care: Exploring Canadian, American and international perspectives. Can. Oncol. Nurs. J. 2015, 25, 73–92. [Google Scholar] [CrossRef] [PubMed][Green Version]


{kind=link}
{kind=link}
| Part 1—AYA Supportive Care | Questions
|
| Part 2—Types of supportive care currently being accessed Preamble: In terms of delivery of guidelines, appointments, and education, we are going to discuss 3 (2?) different approaches to delivery of supportive and survivorship care information. Hard-copy information vs. online delivery of information. |
|
| Models of care Preamble: In terms of delivery of supportive care, we are going to discuss different approaches to delivery. This includes in person or virtual/online approaches. |
|
| Final comments |
|
| Characteristics | Total Patients Survey (n, %) N = 174 | Focus Group (n, %) N = 36 | |
|---|---|---|---|
| Age | 19–24 | 17 (9.77) | 1 (2.78) |
| 25–29 | 27 (15.5) | 8 (22.2) | |
| 30–39 | 125 (71.8) | 26 (72.2) | |
| Prefer not to answer | 5 (2.87) | 1 (2.78) | |
| Gender | Woman | 143 (82.2) | 31 (86.1) |
| Man | 27 (15.5) | 5 (13.9) | |
| Non-Binary | 2 (1.15) | - | |
| Transgender | 1 (0.57) | - | |
| Prefer not to answer | 1 (0.57) | - | |
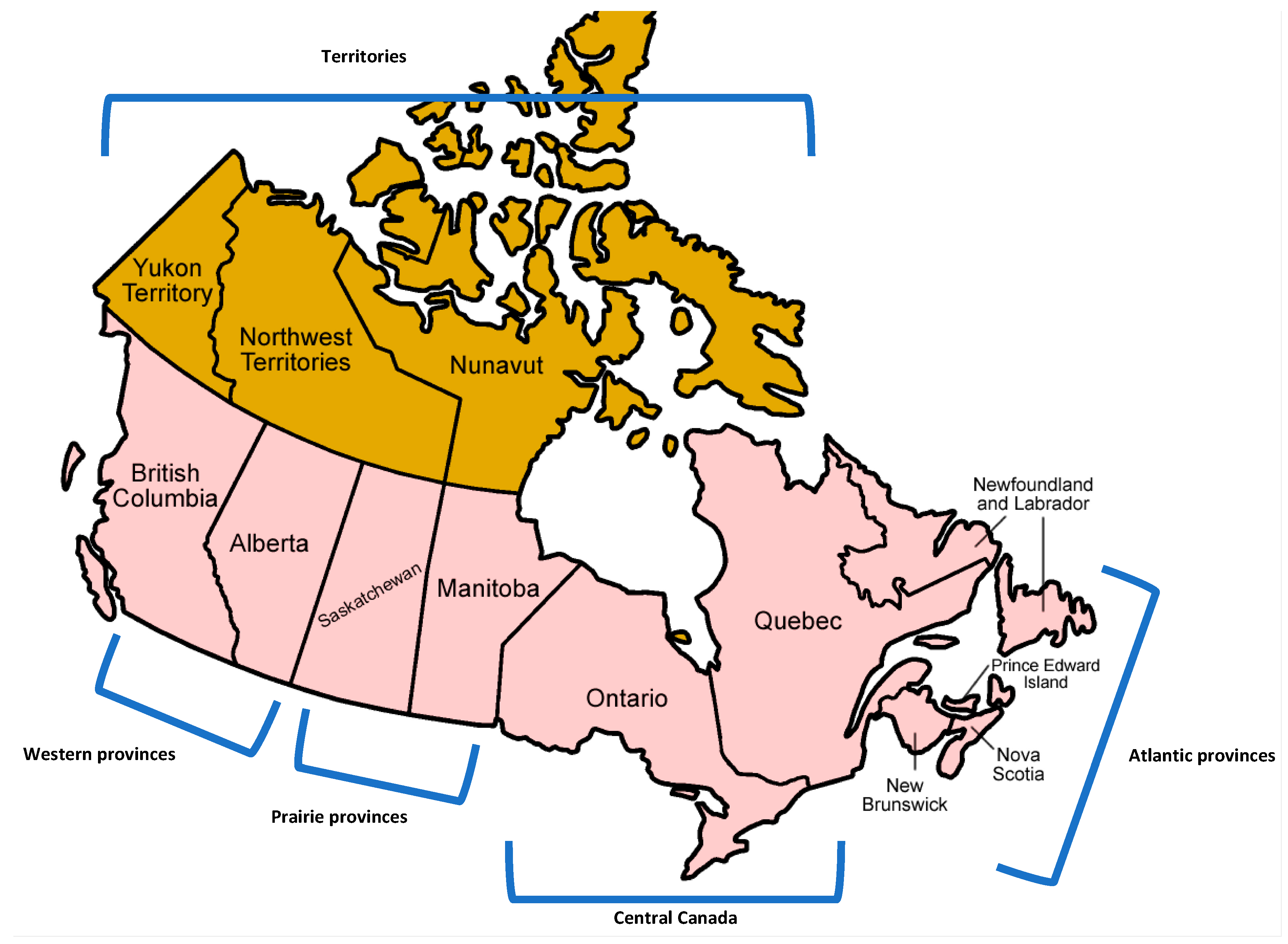
| Region | Central Canada (Ontario and Quebec) | 94 (54.0) | 15 (41.7) |
| Western Canada (British Columbia and Alberta) | 51 (29.3) | 13 (36.1) | |
| Prairie Provinces (Saskatchewan and Manitoba) | 18 (10.3) | 5 (13.9) | |
| Atlantic Provinces (Newfoundland and Labrador, Prince Edward Island, New Brunswick, Nova Scotia) | 11 (6.3) | 3 (8.30) | |
| Territories | 0 (0.00) | 0 (0.00) | |
| Population Centre | Rural (less than 50,000) | 30 (17.2) | 5 (13.9) |
| Small Town (between 50,000–250,000) | 40 (23.0) | 10 (27.8) | |
| Large City (250,000–1 million) | 44 (25.3) | 8 (22.2) | |
| Metropolitan Centre (over 1 million) | 59 (33.9) | 13 (36.1) | |
| Prefer not to answer | 1 (0.57) | - | |
| Cancer Treatment Stage | Yet to start treatment | 2 (1.15) | |
| Currently in Active Treatment | 54 (31.0) | 8 (22.2) | |
| Completed Treatment and in Long-term Follow-up | 95 (54.6) | 23 (63.9) | |
| Discharged from Cancer Centre | 19 (10.9) | 5 (13.9) | |
| Unsure | 4 (2.30) | - | |
| Time of Diagnosis | <1 year | 45 (25.9) | 8 (22.2) |
| 1–3 years ago | 70 (40.2) | 16 (44.4) | |
| 4–6 years ago | 27 (15.5) | 5 (13.9) | |
| ≥6 years ago | 31 (17.8) | 7 (19.4) | |
| Prefer not to answer | 1 (0.56) | - |
| Question | Selection | N (%) |
| When did you receive information about long-term health risks? | Before starting treatment | 116 (66.7) |
| During treatment | 72 (41.4) | |
| Once finished treatment | 43 (24.7) | |
| Not yet received detailed information | 32 (18.4) | |
| Prefer not to answer | 2 (1.15) | |
| From the (health risk) information received, was it? | Not enough | 92 (52.9) |
| Just enough | 54 (31.0) | |
| Too much | 4 (2.30) | |
| Yet to receive detailed information | 21 (12.1) | |
| Prefer not to answer | 3 (1.70) | |
| When did you receive information about supportive care? | Before starting treatment | 76 (43.7) |
| During treatment | 85 (48.9) | |
| Once finished treatment | 54 (31.0) | |
| Not yet received detailed information | 33 (19.0) | |
| Prefer not to answer | 3 (1.70) | |
| From the (supportive care) information received, was it? | Not enough | 100 (57.5) |
| Just enough | 54 (31.0) | |
| Too much | 0 (0.00) | |
| Yet to receive detailed information | 17 (9.77) | |
| Prefer not to answer | 3 (1.70) | |
| Level of concern about each of the following health issue at this time: | Brain fog | |
| Does not apply to me | 6 (3.45) | |
| I am not sure | 3 (1.72) | |
| Not concerned at all | 17 (9.77) | |
| Not very concerned | 34 (19.5) | |
| Somewhat concerned | 69 (39.7) | |
| Very concerned | 45 (25.9) | |
| Fertility | ||
| Does not apply to me | 14 (8.05) | |
| I am not sure | 7 (4.02) | |
| Not concerned at all | 32 (18.4) | |
| Not very concerned | 17 (9.77) | |
| Somewhat concerned | 38 (21.8) | |
| Very concerned | 66 (37.9) | |
| Mental and emotional health | ||
| Does not apply to me | 1 (0.57) | |
| I am not sure | 2 (1.15) | |
| Not concerned at all | 6 (3.45) | |
| Not very concerned | 15 (8.62) | |
| Somewhat concerned | 54 (31.0) | |
| Very concerned | 96 (55.1) | |
| Physical health | ||
| Does not apply to me | 2 (1.15) | |
| I am not sure | 1 (0.57) | |
| Not concerned at all | 6 (3.45) | |
| Not very concerned | 27 (15.5) | |
| Somewhat concerned | 54 (31.0) | |
| Very concerned | 84 (48.3) | |
| Fear of new/different cancer | ||
| Does not apply to me | 2 (1.15) | |
| I am not sure | 5 (2.87) | |
| Not concerned at all | 6 (3.45) | |
| Not very concerned | 11 (6.32) | |
| Somewhat concerned | 41 (23.6) | |
| Very concerned | 109 (62.6) | |
| Fear of cancer recurrence | ||
| Does not apply to me | 6 (3.45) | |
| I am not sure | 1 (0.57) | |
| Not concerned at all | 3 (1.72) | |
| Not very concerned | 8 (4.60) | |
| Somewhat concerned | 36 (20.7) | |
| Very concerned | 120(69.0) | |
| Sexual health | ||
| Does not apply to me | 3 (1.72) | |
| I am not sure | 1 (0.57) | |
| Not concerned at all | 16 (9.20) | |
| Not very concerned | 29 (16.7) | |
| Somewhat concerned | 61 (35.1) | |
| Very concerned | 64 (36.8) | |
| Managing finances | ||
| Does not apply to me | 6 (3.45) | |
| I am not sure | 27 (15.5) | |
| Not concerned at all | 38 (21.8) | |
| Not very concerned | 39 (22.4) | |
| Somewhat concerned | 64 (36.8) | |
| Very concerned | 6 (3.45) | |
| Return to work/career/school | ||
| Does not apply to me | 16 (9.20) | |
| I am not sure | 2 (1.15) | |
| Not concerned at all | 26 (14.9) | |
| Not very concerned | 27 (15.5) | |
| Somewhat concerned | 41 (23.6) | |
| Very concerned | 62 (35.6) | |
| Making/maintaining social connections | ||
| Does not apply to me | 2 (1.15) | |
| I am not sure | 3 (1.72) | |
| Not concerned at all | 35 (20.1) | |
| Not very concerned | 36 (20.7) | |
| Somewhat concerned | 64 (36.8) | |
| Very concerned | 34 (19.5) | |
| Support for caregivers, (i.e., my parents/spouse/siblings) | ||
| Does not apply to me | 15 (8.62) | |
| I am not sure | 4 (2.30) | |
| Not concerned at all | 37 (21.3) | |
| Not very concerned | 32 (18.4) | |
| Somewhat concerned | 56 (32.1) | |
| Very concerned | 30 (17.2) | |
| Child-care support | ||
| Does not apply to me | 69 (39.7) | |
| I am not sure | 1 (0.57) | |
| Not concerned at all | 46 (26.4) | |
| Not very concerned | 24 (13.8) | |
| Somewhat concerned | 18 (10.3) | |
| Very concerned | 16 (9.20) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Avery, J.; Wong, E.; Harris, C.; Chapman, S.; Uppal, S.; Shanawaz, S.; Edwards, A.; Burnett, L.; Vora, T.; Gupta, A.A. The Transformation of Adolescent and Young Adult Oncological and Supportive Care in Canada: A Mixed Methods Study. Curr. Oncol. 2022, 29, 5126-5138. https://doi.org/10.3390/curroncol29070406
Avery J, Wong E, Harris C, Chapman S, Uppal S, Shanawaz S, Edwards A, Burnett L, Vora T, Gupta AA. The Transformation of Adolescent and Young Adult Oncological and Supportive Care in Canada: A Mixed Methods Study. Current Oncology. 2022; 29(7):5126-5138. https://doi.org/10.3390/curroncol29070406
Chicago/Turabian StyleAvery, Jonathan, Emily Wong, Christine Harris, Stacy Chapman, Serena Uppal, Shaayini Shanawaz, Annemarie Edwards, Laura Burnett, Tushar Vora, and Abha A. Gupta. 2022. "The Transformation of Adolescent and Young Adult Oncological and Supportive Care in Canada: A Mixed Methods Study" Current Oncology 29, no. 7: 5126-5138. https://doi.org/10.3390/curroncol29070406
APA StyleAvery, J., Wong, E., Harris, C., Chapman, S., Uppal, S., Shanawaz, S., Edwards, A., Burnett, L., Vora, T., & Gupta, A. A. (2022). The Transformation of Adolescent and Young Adult Oncological and Supportive Care in Canada: A Mixed Methods Study. Current Oncology, 29(7), 5126-5138. https://doi.org/10.3390/curroncol29070406