Diagnostic and Therapeutic Challenges in a Patient with Ureteral Metastases from a Triple Negative Breast Cancer




 ,
,
Abstract
1. Introduction
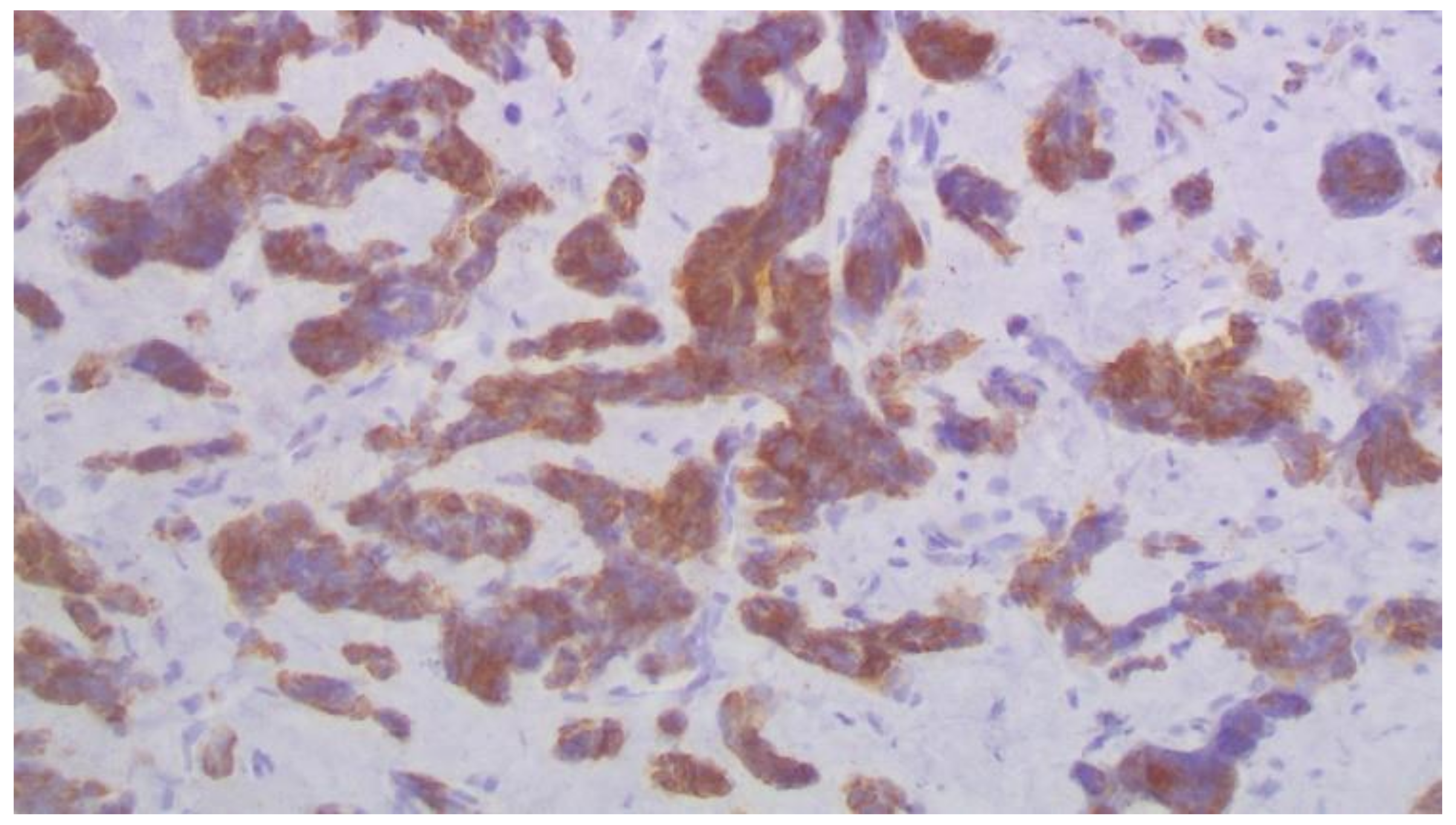
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lei, S.; Zheng, R.; Zhang, S.; Wang, S.; Chen, R.; Sun, K.; Zeng, H.; Zhou, J.; Wei, W. Global Patterns of Breast Cancer Incidence and Mortality: A Population-Based Cancer Registry Data Analysis from 2000 to 2020. Cancer Commun. 2021, 41, 1183–1194. [Google Scholar] [CrossRef] [PubMed]
- Yamamura, J.; Kamigaki, S.; Fujita, J.; Osato, H.; Manabe, H.; Tanaka, Y.; Shinzaki, W.; Hashimoto, Y.; Komoike, Y. New Insights into Patterns of First Metastatic Sites Influencing Survival of Patients with Hormone Receptor-Positive, HER2-Negative Breast Cancer: A Multicenter Study of 271 Patients. BMC Cancer 2021, 21, 476. [Google Scholar] [CrossRef] [PubMed]
- Nathanson, S.D.; Detmar, M.; Padera, T.P.; Yates, L.R.; Welch, D.R.; Beadnell, T.C.; Scheid, A.D.; Wrenn, E.D.; Cheung, K. Mechanisms of Breast Cancer Metastasis. Clin. Exp. Metastasis 2021, 29, 117–137. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Deng, J.; Guo, J.; Fu, B. Ureteral Involvement by Metastatic Malignant Disease. Clin. Exp. Metastasis 2019, 36, 499–509. [Google Scholar] [CrossRef]
- Haddad, F.S. Metastases to the Ureter. Review of the World Literature, and Three New Case Reports. J. Med. Liban. 1999, 47, 265–271. [Google Scholar]
- López-Martínez, R.A.; Stock, J.A.; Gump, F.E.; Rosen, J.S. Carcinoma of the Breast Metastatic to the Ureter Presenting with Flank Pain and Recurrent Urinary Tract Infection. Am. Surg. 1996, 62, 748–752. [Google Scholar]
- Grabstald, H.; Kaufman, R. Hydronephrosis Secondary to Ureteral Obstruction by Metastatic Breast Cancer. J. Urol. 1969, 102, 569–576. [Google Scholar] [CrossRef]
- Talreja, D.; Opfell, R.W. Ureteral Metastasis in Carcinoma of the Breast. West. J. Med. 1980, 133, 252–254. [Google Scholar]
- Richie, J.P.; Withers, G.; Ehrlich, R.M. Ureteral Obstruction Secondary to Metastatic Tumors. Surg. Gynecol. Obstet. 1979, 148, 355–357. [Google Scholar]
- Karaosmanoglu, A.D.; Onur, M.R.; Karcaaltincaba, M.; Akata, D.; Ozmen, M.N. Secondary Tumors of the Urinary System: An Imaging Conundrum. Korean J. Radiol. 2018, 19, 742–751. [Google Scholar] [CrossRef]
- Fröber, R. Surgical Anatomy of the Ureter. BJU Int. 2007, 100, 949–965. [Google Scholar] [CrossRef]
- Gabsi, A.; Yahiaoui, Y.; Zenhani, A.; Herbegue, K.; Meddeb, K.; Mokrani, A.; Letaief, F.; Ayadi, M.; Rais, H.; Chraiet, N.; et al. Ureteral Metastasis in Carcinoma of the Breast. Urology case reports. November 2018, 21, 38–40. [Google Scholar] [CrossRef]
- Jani, K. Ureteric Obstruction Secondary to Metastatic Breast Carcinoma. Pakistan J. Med. Sci. 2006, 22, 197–199. [Google Scholar]
- Logothetis, C.; Assikis, V.; Sarriera, J. Algorithm for the Management of Urinary Obstruction. In Holland-Frei Cancer Medicine, 6th ed.; Kufe, D.W., Pollock, R.E., Weichselbaum, R.R., Best, R.C., Jr., Gansler, T.S., Holland, J.F., Frei, E., Eds.; BC Decker: Hamilton, ON, Canada, 2003. Available online: https://www.ncbi.nlm.nih.gov/books/NBK13333/ (accessed on 10 April 2022).
- Merchan, J.; Jhaveri, K. Chemotherapy Nephrotoxicity and dose Modification in Patients with Kidney Impairment: Conventional Cytotoxic Agents-UpToDate. Available online: https://www.uptodate.com/contents/chemotherapy-nephrotoxicity-and-dose-modification-in-patients-with-kidney-impairment-conventional-cytotoxic-agents#H1991902678 (accessed on 12 March 2022).
- Numakura, K.; Tsuchiya, N.; Obara, T.; Tsuruta, H.; Saito, M.; Narita, S.; Inoue, T.; Horikawa, Y.; Satoh, S.; Habuchi, T. A Case of Ureteral Malignant Lymphoma Diagnosed by Laparoscopic Needle Biopsy. Jpn. J. Clin. Oncol. 2011, 41, 440–442. [Google Scholar] [CrossRef][Green Version]
- Presman, D.; Ehrich, L. Metastatic Tumors of the Ureter. J. Urol. 1948, 59, 312–325. [Google Scholar] [CrossRef]
- Chahin, M.; Chhatrala, H.; Krishnan, N.; Brow, D.; Zuberi, L. Triple-Negative Lobular Breast Cancer Causing Hydronephrosis. J. Investig. Med. High Impact Case Rep. 2020, 8, 2324709620905954. [Google Scholar] [CrossRef]
- Chen, Y.; Wu, J.; Hu, T.; Wang, J.; Su, F. Male Breast Cancer with Ureteral Metastasis: A Case Report. Annals of palliative medicine. China July 2021, 8346–8351. [Google Scholar] [CrossRef]
- Ennishi, D.; Takata, K.; Béguelin, W.; Duns, G.; Mottok, A.; Farinha, P.; Bashashati, A.; Saberi, S.; Boyle, M.; Meissner, B.; et al. Molecular and Genetic Characterization of MHC Deficiency Identifies EZH2 as Therapeutic Target for Enhancing Immune Recognition. Cancer Discov. 2019, 9, 546–563. [Google Scholar] [CrossRef]
- Nie, L.; Wei, Y.; Zhang, F.; Hsu, Y.-H.; Chan, L.-C.; Xia, W.; Ke, B.; Zhu, C.; Deng, R.; Tang, J.; et al. DK2-Mediated Site-Specific Phosphorylation of EZH2 Drives and Maintains Triple-Negative Breast Cancer. Nat. Commun. 2019, 10, 5114. [Google Scholar] [CrossRef]
- Tanaka, H.; Yoshida, S.; Komai, Y.; Sakai, Y.; Urakami, S.; Yuasa, T.; Yamamoto, S.; Masuda, H.; Koizumi, M.; Kohno, A.; et al. Clinical Value of 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in Upper Tract Urothelial Carcinoma: Impact on Detection of Metastases and Patient Management. Urol. Int. 2016, 96, 65–72. [Google Scholar] [CrossRef]
- Wan, X.; Hou, Y.; Yu, Z. Helical CT Diagnosis of the Primary Ureteral Carcinoma and Ureteral Metastatic Carcinoma. J. Clin. Radiol. 2010, 29, 985–987. [Google Scholar]
- Huang, Y.; He, H.; Wei, W.; Li, Q.; Long, X.; Li, Y.; Chen, R.; Yi, X. 18F-FDG PET/CT Features of Ureteral Metastases from Breast Cancer: A Case Report. J. Int. Med. Res. 2021, 49, 3000605211014090. [Google Scholar] [CrossRef]
- Kitajima, K.; Yamamoto, S.; Fukushima, K.; Minamimoto, R.; Kamai, T.; Jadvar, H. Update on Advances in Molecular PET in Urological Oncology. Jpn. J. Radiol. 2016, 34, 470–485. [Google Scholar] [CrossRef]
- Peart, O. Metastatic Breast Cancer. Radiol. Technol. 2017, 88, 519M–539M. [Google Scholar]
- Lin, N.U.; Thomssen, C.; Cardoso, F.; Cameron, D.; Cufer, T.; Fallowfield, L.; Francis, P.A.; Kyriakides, S.; Pagani, O.; Senkus, E.; et al. International Guidelines for Management of Metastatic Breast Cancer (MBC) from the European School of Oncology (ESO)-MBC Task Force: Surveillance, Staging, and Evaluation of Patients with Early-Stage and Metastatic Breast Cancer. Breast 2013, 22, 203–210. [Google Scholar] [CrossRef]
- Pagani, O.; Senkus, E.; Wood, W.; Colleoni, M.; Cufer, T.; Kyriakides, S.; Costa, A.; Winer, E.P.; Cardoso, F. International Guidelines for Management of Metastatic Breast Cancer: Can Metastatic Breast Cancer Be Cured? J. Natl. Cancer Inst. 2010, 102, 456–463. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author and Year {Ref} | Patient’s Characteristics | Clinical Findings | Laboratory Findings | Treatment |
|---|---|---|---|---|
| Chahin et al., 2020 [18] | 54-year-old female Invasive lobular carcinoma, G I, ER-PR-HER2-negative | Hydronephrosis | CT scan: Hemi-pelvic mass | Ureteral stent |
| Chen et al., 2021 [19] | 60-year-old male Invasive ductal carcinoma, GIII, ER-PR-HER2-negative | Hematuria | CT scan: Ureteral mass and dilated ureter | Middle ureter dissection and anastomosis |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saranti, G.; Zolota, V.; Kalogeropoulou, C.; Papathanasiou, N.; Katsila, T.; Kitsou, K.; Haliassos, I.; Kardamakis, D. Diagnostic and Therapeutic Challenges in a Patient with Ureteral Metastases from a Triple Negative Breast Cancer. Curr. Oncol. 2022, 29, 4791-4798. https://doi.org/10.3390/curroncol29070380
Saranti G, Zolota V, Kalogeropoulou C, Papathanasiou N, Katsila T, Kitsou K, Haliassos I, Kardamakis D. Diagnostic and Therapeutic Challenges in a Patient with Ureteral Metastases from a Triple Negative Breast Cancer. Current Oncology. 2022; 29(7):4791-4798. https://doi.org/10.3390/curroncol29070380
Chicago/Turabian StyleSaranti, Georgia, Vasiliki Zolota, Christina Kalogeropoulou, Nikolaos Papathanasiou, Theodora Katsila, Konstantina Kitsou, Ilias Haliassos, and Dimitrios Kardamakis. 2022. "Diagnostic and Therapeutic Challenges in a Patient with Ureteral Metastases from a Triple Negative Breast Cancer" Current Oncology 29, no. 7: 4791-4798. https://doi.org/10.3390/curroncol29070380
APA StyleSaranti, G., Zolota, V., Kalogeropoulou, C., Papathanasiou, N., Katsila, T., Kitsou, K., Haliassos, I., & Kardamakis, D. (2022). Diagnostic and Therapeutic Challenges in a Patient with Ureteral Metastases from a Triple Negative Breast Cancer. Current Oncology, 29(7), 4791-4798. https://doi.org/10.3390/curroncol29070380