Oncologists’ Locus of Control, Compassion Fatigue, Compassion Satisfaction, and the Mediating Role of Helplessness


Abstract
:1. Introduction
2. Method
2.1. Participants and Procedure
2.2. Measures
2.3. Statistical Analysis
3. Results
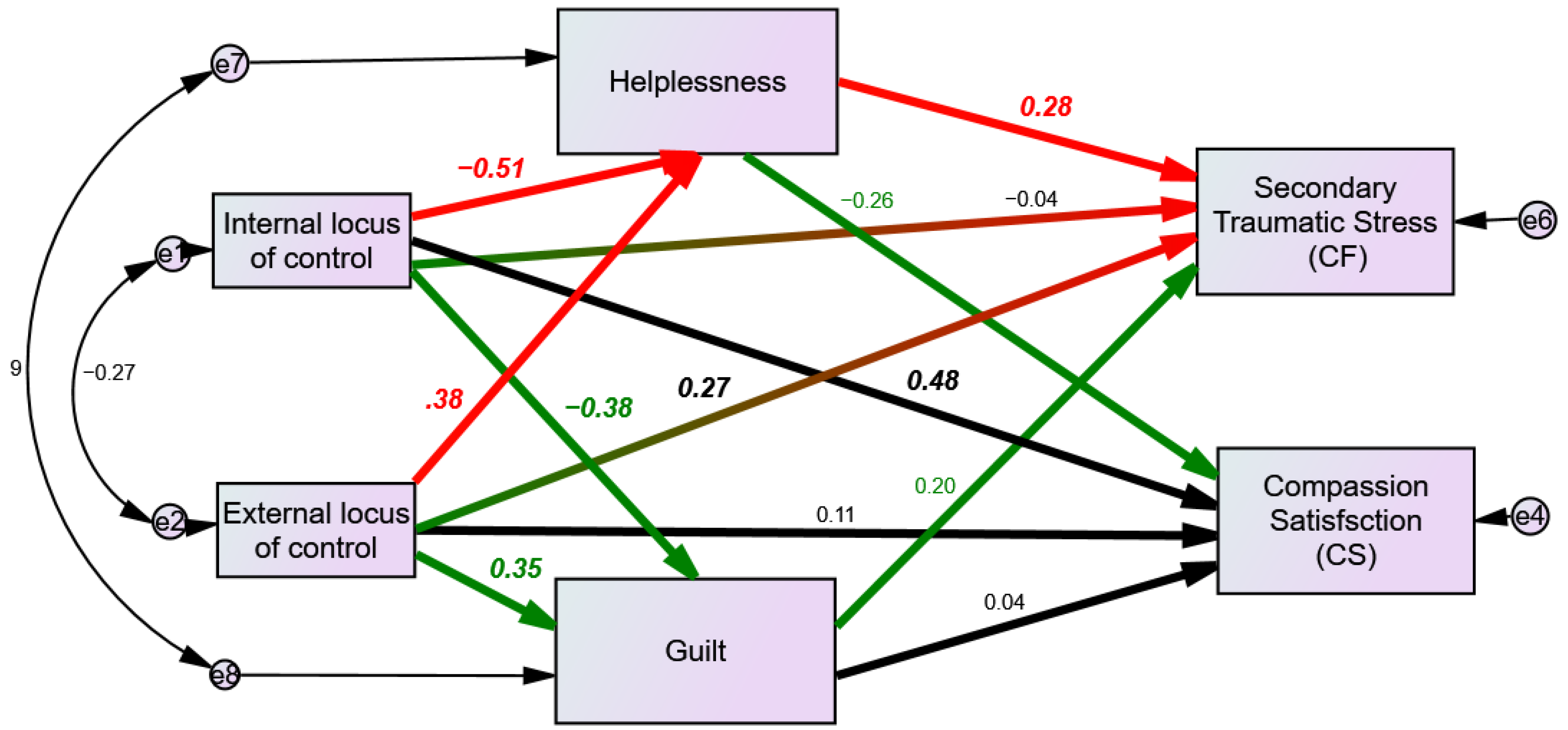
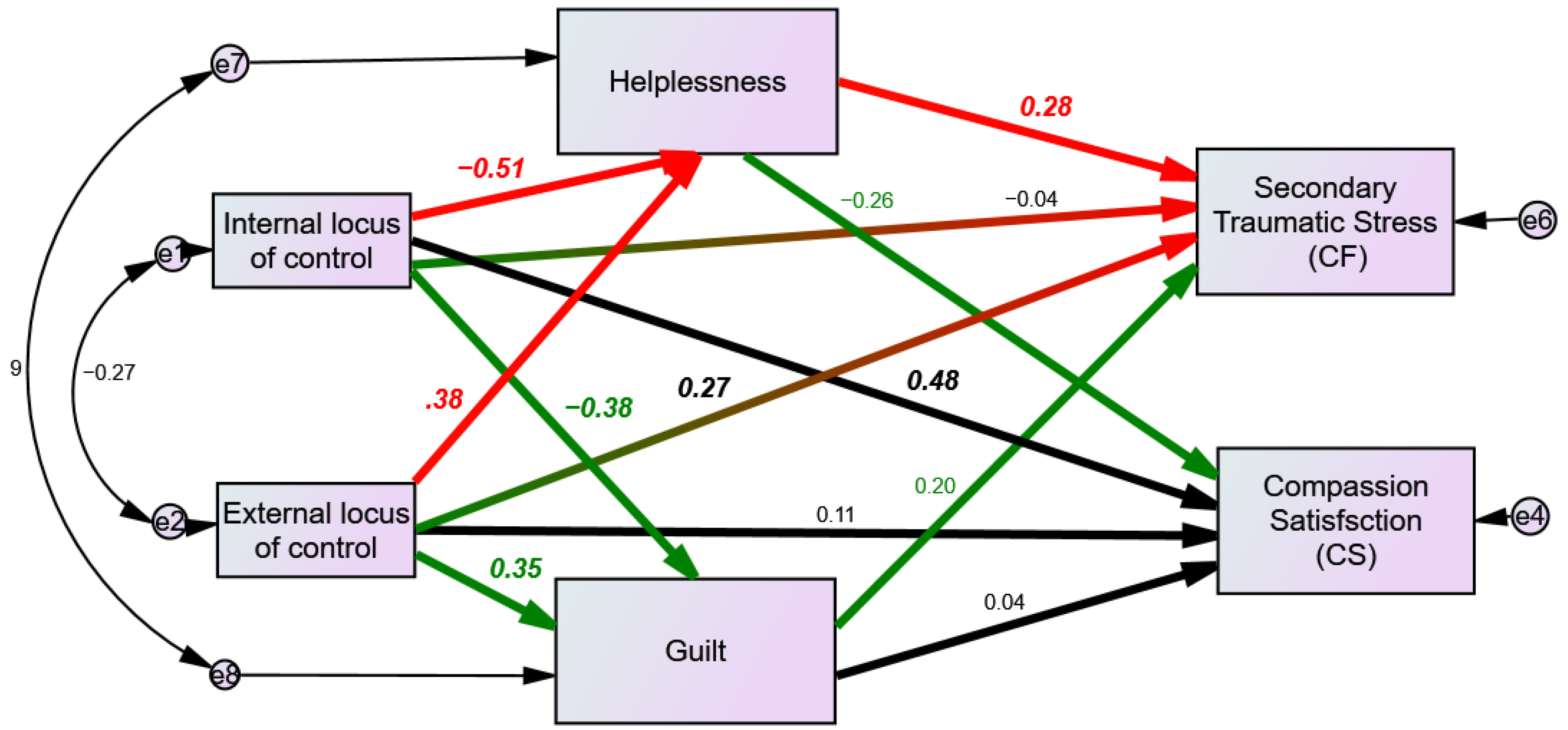
The Mediation Hypotheses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hlubocky, F.J.; Taylor, L.P.; Marron, J.M.; Spence, R.A.; McGinnis, M.M.; Brown, R.F.; Kamal, A.H. A call to action: Ethics committee roundtable recommendations for addressing burnout and moral distress in oncology. JCO Oncol. Pract. 2020, 16, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.; Goh, J.; Sinsky, C. The business case for investing in physician well-being. JAMA Intern. Med. 2017, 177, 1826–1832. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.D.; West, C.P.; Sinsky, C. Changes in burnout and satisfaction with work-life integration in physicians and the general US working population between 2011 and 2017. Mayo Clin. Proc. 2019, 94, 1681–1694. [Google Scholar] [CrossRef] [Green Version]
- Rotenstein, L.S.; Torre, M.; Ramos, M.A.; Rosales, R.C.; Guille, C.; Sen, S.; Mata, D.A. Prevalence of burnout among physicians: A systematic review. JAMA 2018, 320, 1131–1150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shanafelt, T.D.; Gradishar, W.J.; Kosty, M. Burnout and career satisfaction among US oncologists. J. Clin. Oncol. 2014, 32, 678–686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunt, P.; Denieffe, S.; Gooney, M. Running on empathy: Relationship of empathy to compassion satisfaction and compassion fatigue in cancer healthcare professionals. Eur. J. Cancer Care 2019, 28, e13124. [Google Scholar] [CrossRef] [PubMed]
- Hlubocky, F.J.; Back, A.L.; Shanafelt, T.D. Addressing burnout in oncology: Why cancer care clinicians are at risk, what individuals can do, and how organizations can respond. Am. Soc. Clin. Oncol. Educ. Book 2016, 35, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Hlubocky, F.J.; Rose, M.; Epstein, R.M. Mastering resilience in oncology: Learn to thrive in the face of burnout. Am. Soc. Clin. Oncol. Educ. Book 2017, 37, 771–781. [Google Scholar] [CrossRef]
- Allegra, C.J.; Hall, R.; Yothers, G. Prevalence of burnout in the U.S. oncology community: Results of a 2003 survey. J. Oncol. Pract. 2005, 1, 140–147. [Google Scholar]
- Zhang, B.X.; Li, H.Y.; Jin, X.H.; Peng, W.Q.; Wong, C.L.; Qiu, D.R. Prevalence and factors associated with compassion satisfaction and compassion fatigue among Chinese oncology healthcare professionals: A cross-sectional survey. Asia-Pac. J. Oncol. Nurs. 2021, in press. [Google Scholar] [CrossRef]
- Granek, L.; Nakash, O.; Cohen, M.; Ben-David, M.; Ariad, S. Oncologists’ communication about end of life: The relationship among secondary traumatic stress, compassion satisfaction, and approach and avoidance communication. Psycho-Oncology 2017, 26, 1980–1986. [Google Scholar] [CrossRef]
- HaGani, N.; Yagil, D.; Cohen, M. Burnout among oncologists and oncology nurses: A systematic review and meta-analysis. Health Psychol. 2022, 41, 53. [Google Scholar] [CrossRef]
- Yates, M.; Samuel, V. Burnout in oncologists and associated factors: A systematic literature review and meta-analysis. Eur. J. Cancer Care 2019, 28, e13094. [Google Scholar] [CrossRef]
- Laor-Maayany, R.; Goldzweig, G.; Hasson-Ohayon, I.; Bar-Sela, G.; Engler-Gross, A.; Braun, M. Compassion fatigue among oncologists: The role of grief, sense of failure, and exposure to suffering and death. Supportive Care Cancer 2020, 28, 2025–2031. [Google Scholar] [CrossRef]
- Banerjee, S.; Califano, R.; Corral, J.; De Azambuja, E.; De Mattos-Arruda, L.; Guarneri, V.; Strijbos, M.H. Professional burnout in European young oncologists: Results of the European Society for Medical Oncology (ESMO) young oncologists committee burnout survey. Ann. Oncol. 2017, 28, 1590–1596. [Google Scholar] [CrossRef]
- Stamm, B.H. The proQOL manual. Retrieved July 2005, 16, 2007. [Google Scholar]
- Stamm, B. The Concise ProQOL Manual, 2nd ed.; Publisher Academia: Pocatello, ID, USA, 2010; ID: ProQOL.org. [Google Scholar]
- Rotter, J.B. Generalized expectancies for internal versus external control of reinforcement. Psychol. Monogr. Gen. Appl. 2010, 80, 1–28. [Google Scholar] [CrossRef] [Green Version]
- Levenson, H. Multidimensional locus of control in psychiatric patients. J. Consult. Clin. Psychol. 1973, 41, 397. [Google Scholar] [CrossRef]
- Ng, T.W.; Sorensen, K.L.; Eby, L.T. Locus of control at work: A meta-analysis. J. Organ. Behav. 2006, 27, 1057–1087. [Google Scholar] [CrossRef]
- Kubany, E.S.; Watson, S.B. Guilt: Elaboration of a multidimensional model. Psychol. Rec. 2003, 53, 51–90. [Google Scholar]
- Ramondetta, L.M.; Urbauer, D.; Brown, A.J.; Richardson, G.; Thaker, P.H.; Koenig, H.G.; Sun, C. Work related stress among gynecologic oncologists. Gynecol. Oncol. 2011, 123, 365–369. [Google Scholar] [CrossRef] [PubMed]
- Granek, L.; Tozer, R.; Mazzotta, P.; Ramjaun, A.; Krzyzanowska, M. Nature and impact of grief over patient loss on oncologists' personal and professional lives. Arch. Intern. Med. 2012, 172, 964–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nowakowski, J.; Borowiec, G.; Zwierz, I.; Jagodzinski, W.; Tarkowski, R. Stress in An Oncologist’s Life: Present but Not Insurmountable. J. Cancer Educ. 2017, 32, 198–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Restivo, L.; Julian-Reynier, C.; Peyla, L.; Apostolidis, T. What makes decision-making difficult for oncologists faced with critical situations? The socio-affective side of the physician–patient relationship. J. Health Psychol. 2020, 25, 1396–1409. [Google Scholar]
- Maier, S.F.; Seligman, M.E. Learned helplessness: Theory and evidence. J. Exp. Psychol. Gen. 1976, 105, 3. [Google Scholar]
- Hayuni, G.; Hasson-Ohayon, I.; Goldzweig, G.; Bar Sela, G.; Braun, M. Between empathy and grief: The mediating effect of compassion fatigue among oncologists. Psycho-Oncology 2019, 28, 2344–2350. [Google Scholar] [CrossRef]
- Amram, Y. Therapist Characteristics Treatment Outcome during Treatment in Therapeutic Communities for Drug Addicts. Ph.D. Thesis, The Hebrew University, Jerusalem, Israel, 1996, unpublished. [Google Scholar]
- Jones, W.H.; Schratter, A.K.; Kugler, K. The guilt inventory. Psychol. Rep. 2000, 87 (Suppl. 3), 1039–1042. [Google Scholar] [CrossRef]
- Quinless, F.W.; Nelson, M.M. Development of a measure of learned helplessness. Nurs. Res. 1988, 37, 11–15. [Google Scholar] [CrossRef]
- Bargai, N.; Ben-Shakhar, G.; Shalev, A.Y. Posttraumatic stress disorder and depression in battered women: The mediating role of learned helplessness. J. Fam. Violence 2007, 22, 267–275. [Google Scholar] [CrossRef]
- Karstoft, K.I.; Armour, C.; Elklit, A.; Solomon, Z. The role of locus of control and coping style in predicting longitudinal PTSD-trajectories after combat exposure. J. Anxiety Disord. 2015, 32, 89–94. [Google Scholar] [CrossRef]
- Atilola, O.; Stevanovic, D.; Moreira, P.; Dodig-Ćurković, K.; Franic, T.; Djoric, A.; Knez, R. External locus-of-control partially mediates the association between cumulative trauma exposure and posttraumatic stress symptoms among adolescents from diverse background. Anxiety Stress Coping 2021, 34, 626–644. [Google Scholar] [CrossRef]
- Onyedire, N.G.; Ekoh, A.T.; Chukwuorji, J.C.; Ifeagwazi, C.M. Posttraumatic stress disorder (PTSD) symptoms among firefighters: Roles of resilience and locus of control. J. Workplace Behav. Health 2017, 32, 227–248. [Google Scholar] [CrossRef]
- Black, D.W.; Grant, J.E. DSM-5® Guidebook: The Essential Companion to the Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Pub.: Washington, DC, USA, 2014. [Google Scholar]
- Figley, C.R. Compassion Fatigue: Toward a New Understanding of the Costs of Caring; The Sidran Press: Baltimore, MD, USA, 1995. [Google Scholar]
- Sepúlveda, C.; Marlin, A.; Yoshida, T.; Ullrich, A. Palliative care: The World Health Organization's global perspective. J. Pain Symptom Manag. 1995, 24, 91–96. [Google Scholar] [CrossRef]

{kind=link}
| Variable | N (%) |
|---|---|
| Country of birth | |
| Israel | 50 (68.5) |
| Other | 23 (31.5) |
| Marital status | |
| Married or living with partner | 70 (95.9) |
| Single | 2 (2.7) |
| Divorced | 1 (1.4) |
| Children | |
| Yes | 61 (83.6) |
| No | 10 (13.7) |
| Missing | 2 (2.7) |
| Career status | |
| Intern | 23 (31.5) |
| Fellow | 49 (67.1) |
| Missing | 1 (1.4) |
| Oncology specialty | |
| Clinical oncologist | 58 (79.5) |
| Radiation oncologist | 14 (19.2) |
| Missing | 1 (1.4) |
| Number of work hours | |
| Part-time | 6 (8.2) |
| Full-time | 66 (90.4) |
| Missing | 1 (1.4) |
| Primary practice setting | |
| Hospital | 68 (93.2) |
| Community practice | 3 (4.1) |
| Other | 2 (2.8) |
| Medical specialty | |
| Breast oncologist | 17 (23.3) |
| Thoracic oncologist | 7 (9.6) |
| Hematologist oncologist | 14 (19.2) |
| Other | 26(35.6) |
| No medical specialty | 9 (12.3) |
| Training/practice in palliative care (82) | |
| Yes | 43 (58.9) |
| No | 30 (41.1) |
| Secondary Traumatic Stress | Burnout | Compassion Satisfaction | Internal LOC | External LOC—Others | External LOC—Coincidence | Learned Helplessness | Situational Guilt | |
|---|---|---|---|---|---|---|---|---|
| Mean | 17.29 | 26.44 | 36.83 | 23.10 | 10.88 | 10.92 | 1.90 | 2.79 |
| S.D. | 7.35 | 6.42 | 6.98 | 3.91 | 4.36 | 4.02 | 0.35 | 0.73 |
| Beta | Sig. | |
|---|---|---|
| External locus of control—others → Secondary traumatic stress (STS) | 0.27 | * |
| External locus of control—others → Learned helplessness | 0.38 | *** |
| External locus of control—others → Situational guilt | 0.35 | *** |
| Internal locus of control → Compassion satisfaction (CS) | 0.48 | *** |
| Internal locus of control → Learned helplessness | −0.51 | *** |
| Internal locus of control → Situational guilt | −0.38 | *** |
| Learned helplessness → Secondary traumatic stress (STS) | 0.28 | p = 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Braun, M.; Naor, L.; Hasson-Ohayon, I.; Goldzweig, G. Oncologists’ Locus of Control, Compassion Fatigue, Compassion Satisfaction, and the Mediating Role of Helplessness. Curr. Oncol. 2022, 29, 1634-1644. https://doi.org/10.3390/curroncol29030137
Braun M, Naor L, Hasson-Ohayon I, Goldzweig G. Oncologists’ Locus of Control, Compassion Fatigue, Compassion Satisfaction, and the Mediating Role of Helplessness. Current Oncology. 2022; 29(3):1634-1644. https://doi.org/10.3390/curroncol29030137
Chicago/Turabian StyleBraun, Michal, Lee Naor, Ilanit Hasson-Ohayon, and Gil Goldzweig. 2022. "Oncologists’ Locus of Control, Compassion Fatigue, Compassion Satisfaction, and the Mediating Role of Helplessness" Current Oncology 29, no. 3: 1634-1644. https://doi.org/10.3390/curroncol29030137
APA StyleBraun, M., Naor, L., Hasson-Ohayon, I., & Goldzweig, G. (2022). Oncologists’ Locus of Control, Compassion Fatigue, Compassion Satisfaction, and the Mediating Role of Helplessness. Current Oncology, 29(3), 1634-1644. https://doi.org/10.3390/curroncol29030137