Rates of Smoking Cessation at 6 and 12 Months after a Clinical Tobacco Smoking Cessation Intervention in Head and Neck Cancer Patients in Northern Ontario, Canada

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Tobacco Use Questionnaires
2.3. Intensive Clinical Tobacco Intervention
2.4. Statistical Analysis
3. Results
3.1. Study Cohort and Sociodemographics
3.2. Smoking Characteristics in the Study Population
3.3. Cessation Rate after an Intensive Clinical Tobacco Intervention
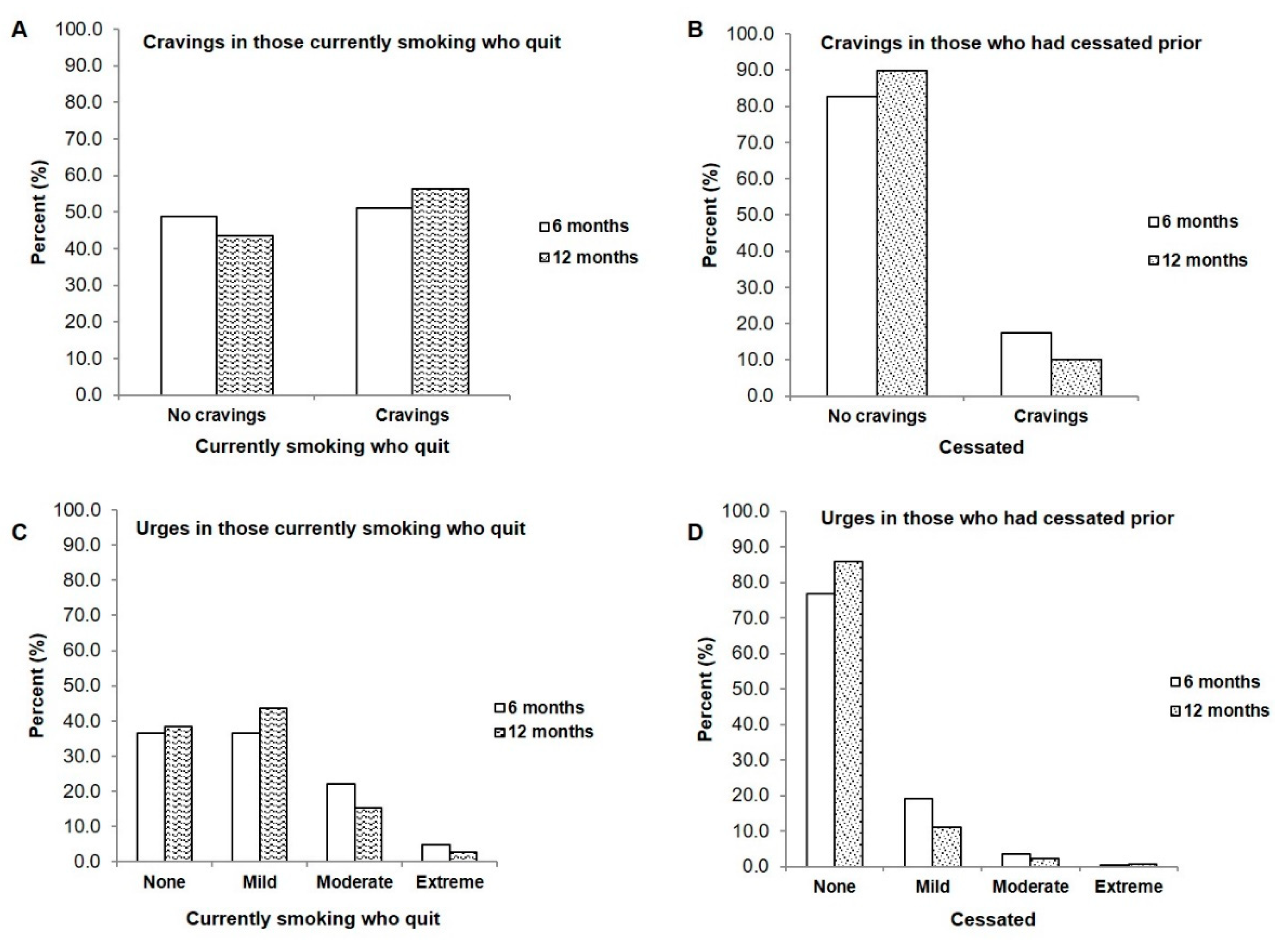
3.4. Cravings and Urges to Smoke on a Regular Basis in Smokers Who Quit and in Those Who Had Been Cessated
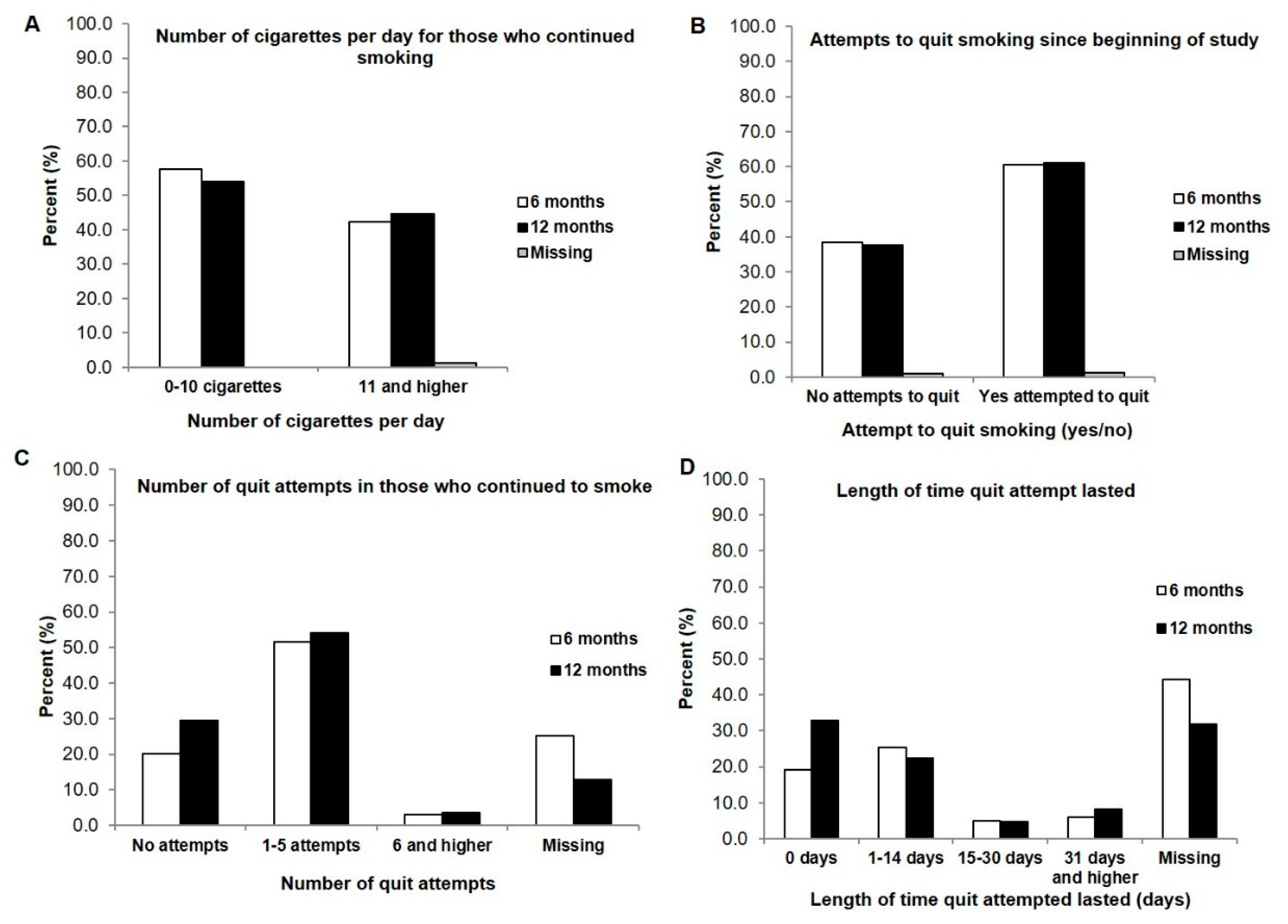
3.5. Participants Who Continued to Smoke
3.6. Comparison of Smoking Characteristics between Current Smokers Who Cessated and Those Who Continued to Smoke
3.7. Participants Who Had Cessated Prior and Resumed Smoking
4. Discussion
4.1. Cessation Rate, Cessation Attempts, and Cessation Methods
4.2. Timing of the Clinical Tobacco Intervention and Motivation to Quit
4.3. Relapse and Longer Time Intervals for Follow-Up
4.4. Smoking Characteristics
4.5. Study Limitations
4.6. Future Directions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khariwala, S.S.; Hatsukami, D.K.; Stepanov, I.; Rubin, N.; Nelson, H.H. Patterns of Tobacco Cessation Attempts and Symptoms Experienced Among Smokers with Head and Neck Squamous Cell Carcinoma. JAMA Otolaryngol. Head Neck Surg. 2018, 144, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.H.E.; Braith, A.; Hitsman, B.; Schnoll, R.A. Treating Nicotine Dependence and Preventing Smoking Relapse in Cancer Patients. Expert Rev. Qual. Life Cancer Care 2017, 2, 23–39. [Google Scholar] [CrossRef] [PubMed]
- Jethwa, A.R.; Khariwala, S.S. Tobacco-related carcinogenesis in head and neck cancer. Cancer Metastasis Rev. 2017, 36, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Symes, Y.R.; Westmaas, J.L.; Mayer, D.K.; Boynton, M.H.; Ribisl, K.M.; Golden, S.D. The impact of psychosocial characteristics in predicting smoking cessation in long-term cancer survivors: A time-to-event analysis. Psychooncology 2018, 27, 2458–2465. [Google Scholar] [CrossRef]
- Conlon, M.S.C.; Santi, S.A.; Meigs, M.L.; Davidson, S.M.; Saunders, D. Cigarette-smoking characteristics and interest in cessation in patients with head-and-neck cancer. Curr. Oncol. 2020, 27, e478–e485. [Google Scholar] [CrossRef]
- Nahhas, G.J.; Wilson, D.; Talbot, V.; Cartmell, K.B.; Warren, G.W.; Toll, B.A.; Carpenter, M.J.; Cummings, K.M. Feasibility of Implementing a Hospital-Based “Opt-Out” Tobacco-Cessation Service. Nicotine Tob. Res. 2017, 19, 937–943. [Google Scholar] [CrossRef]
- Statistics Canada. Canadian Tobacco Use Monitoring Survey, Cycle 2, 2007 (CTUMS); [Archived Questionnaire]; Statistics Canada: Ottawa, ON, Canada, 2012. Available online: https://www23.statcan.gc.ca/imdb/p3Instr.pl?Function=getInstrumentList&Item_Id=52109&UL=1V (accessed on 1 November 2019).
- Johnson, K.C.; Hu, J.; Mao, Y. Passive and active smoking and breast cancer risk in Canada, 1994-97. The Canadian Cancer Registries Epidemiology Research Group. Cancer Causes Control 2000, 11, 211–221. [Google Scholar] [CrossRef]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerstrom, K.O. The Fagerstrom Test for Nicotine Dependence: A revision of the Fagerstrom Tolerance Questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Rickert, W.; Robinson, J. Measuring the heaviness of smoking: Using self-reported time to the first cigarette of the day and number of cigarettes smoked per day. Br. J. Addict. 1989, 84, 791–799. [Google Scholar] [CrossRef]
- Baker, T.B.; Piper, M.E.; McCarthy, D.E.; Bolt, D.M.; Smith, S.S.; Kim, S.Y.; Colby, S.; Conti, D.; Giovino, G.A.; Hatsukami, D.; et al. Time to first cigarette in the morning as an index of ability to quit smoking: Implications for nicotine dependence. Nicotine Tob. Res. 2007, 9 (Suppl. 4), S555–S570. [Google Scholar]
- The Clinical Practice Guideline Treating Tobacco Use and Dependence 2008 Update Panel, Liaisons, and Staff. A clinical practice guideline for treating tobacco use and dependence: 2008 update: A U.S. Public Health Service Report. Am. J. Prev. Med. 2008, 35, 158–176. [Google Scholar] [CrossRef] [PubMed]
- Quinn, V.P.; Hollis, J.F.; Smith, K.S.; Rigotti, N.A.; Solberg, L.I.; Hu, W.; Stevens, V.J. Effectiveness of the 5-As tobacco cessation treatments in nine HMOs. J. Gen. Intern. Med. 2009, 24, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Davidson, S.M.; Boldt, R.G.; Louie, A.V. How can we better help cancer patients quit smoking? The London Regional Cancer Program experience with smoking cessation. Curr. Oncol. 2018, 25, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, C.; Nahhas, G.J.; Guille, C.; Cummings, K.M.; Wheeler, C.; McClure, E.A. Tobacco Use Prevalence and Outcomes Among Perinatal Patients Assessed Through an “Opt-out” Cessation and Follow-Up Clinical Program. Matern. Child Health J. 2017, 21, 1790–1797. [Google Scholar] [CrossRef]
- Tang, M.W.; Oakley, R.; Dale, C.; Purushotham, A.; Moller, H.; Gallagher, J.E. A surgeon led smoking cessation intervention in a head and neck cancer centre. BMC Health Serv. Res. 2014, 14, 636. [Google Scholar] [CrossRef]
- Karam-Hage, M.; Oughli, H.A.; Rabius, V.; Beneventi, D.; Wippold, R.C.; Blalock, J.A.; Cinciripini, P.M. Tobacco Cessation Treatment Pathways for Patients with Cancer: 10 Years in the Making. J. Natl. Compr. Cancer Netw. 2016, 14, 1469–1477. [Google Scholar] [CrossRef][Green Version]
- Kashigar, A.; Habbous, S.; Eng, L.; Irish, B.; Bissada, E.; Irish, J.; Brown, D.; Gilbert, R.; Gullane, P.; Xu, W.; et al. Social environment, secondary smoking exposure, and smoking cessation among head and neck cancer patients. Cancer 2013, 119, 2701–2709. [Google Scholar] [CrossRef]
- Cinciripini, P.M.; Karam-Hage, M.; Kypriotakis, G.; Robinson, J.D.; Rabius, V.; Beneventi, D.; Minnix, J.A.; Blalock, J.A. Association of a Comprehensive Smoking Cessation Program with Smoking Abstinence among Patients with Cancer. JAMA Netw. Open. 2019, 2, e1912251. [Google Scholar] [CrossRef]
- Chan, Y.; Irish, J.C.; Wood, S.J.; Sommer, D.D.; Brown, D.H.; Gullane, P.J.; O’Sullivan, B.; Lockwood, G.A. Smoking cessation in patients diagnosed with head and neck cancer. J. Otolaryngol. 2004, 33, 75–81. [Google Scholar] [CrossRef]
- Gritz, E.R.; Carr, C.R.; Rapkin, D.; Abemayor, E.; Chang, L.J.; Wong, W.K.; Belin, T.R.; Calcaterra, T.; Robbins, K.T.; Chonkich, G. Predictors of long-term smoking cessation in head and neck cancer patients. Cancer Epidemiol. Biomark. Prev. 1993, 2, 261–270. [Google Scholar]
- Yeomans, K.; Payne, K.A.; Marton, J.P.; Merikle, E.P.; Proskorovsky, I.; Zou, K.H.; Li, Q.; Willke, R.J. Smoking, smoking cessation and smoking relapse patterns: A web-based survey of current and former smokers in the US. Int. J. Clin. Pract. 2011, 65, 1043–1054. [Google Scholar] [CrossRef] [PubMed]
- Nightingale, C.L.; Sterba, K.R.; Tooze, J.A.; King, J.L.; Weaver, K.E. Cessation Attitudes and Preferences in Head and Neck Cancer Patients and Implications for Cessation Program Design: A Brief Report. Glob Adv. Health Med. 2019, 8, 2164956119847117. [Google Scholar] [CrossRef] [PubMed]
- Khariwala, S.S.; Rubin, N.; Stepanov, I.; Nollen, N.; Ahluwalia, J.S.; Nelson, H.H.; Hatsukami, D.K. “Cold turkey” or pharmacotherapy: Examination of tobacco cessation methods tried among smokers prior to developing head and neck cancer. Head Neck 2019, 41, 2332–2339. [Google Scholar] [CrossRef] [PubMed]
- Cooley, M.E.; Wang, Q.; Johnson, B.E.; Catalano, P.; Haddad, R.I.; Bueno, R.; Emmons, K.M. Factors associated with smoking abstinence among smokers and recent-quitters with lung and head and neck cancer. Lung Cancer 2012, 76, 144–149. [Google Scholar] [CrossRef]
- Nayan, S.; Gupta, M.K.; Strychowsky, J.E.; Sommer, D.D. Smoking cessation interventions and cessation rates in the oncology population: An updated systematic review and meta-analysis. Otolaryngol. Head Neck Surg. 2013, 149, 200–211. [Google Scholar] [CrossRef]
- Simmons, V.N.; Litvin, E.B.; Jacobsen, P.; Bs, R.D.P.; McCaffrey, J.C.; Ma, J.A.O.; Sutton, S.; Brandon, T.H. Predictors of smoking relapse in patients with thoracic cancer or head and neck cancer. Cancer 2013, 119, 1420–1427. [Google Scholar] [CrossRef]
- Gritz, E.R.; Fingeret, M.C.; Vidrine, D.J.; Lazev, A.B.; Mehta, N.V.; Reece, G.P. Successes and failures of the teachable moment: Smoking cessation in cancer patients. Cancer 2006, 106, 17–27. [Google Scholar] [CrossRef]
- Gritz, E.R.; Schacherer, C.; Koehly, L.; Nielsen, I.R.; Abemayor, E. Smoking withdrawal and relapse in head and neck cancer patients. Head Neck 1999, 21, 420–427. [Google Scholar] [CrossRef]
- Gritz, E.R. Facilitating smoking cessation in cancer patients. Tob. Control 2000, 9 (Suppl. 1), I50. [Google Scholar] [CrossRef][Green Version]
- Simmons, V.N.; Litvin, E.B.; Patel, R.D.; Jacobsen, P.B.; McCaffrey, J.C.; Bepler, G.; Quinn, G.P.; Brandon, T.H. Patient-provider communication and perspectives on smoking cessation and relapse in the oncology setting. Patient Educ. Couns. 2009, 77, 398–403. [Google Scholar] [CrossRef]
- Schnoll, R.A.; Rothman, R.L.; Newman, H.; Lerman, C.; Miller, S.M.; Movsas, B.; Sherman, E.; Ridge, J.A.; Unger, M.; Langer, C.; et al. Characteristics of cancer patients entering a smoking cessation program and correlates of quit motivation: Implications for the development of tobacco control programs for cancer patients. Psychooncology 2004, 13, 346–358. [Google Scholar] [CrossRef] [PubMed]
- Warren, G.W.; Arnold, S.M.; Valentino, J.P.; Gal, T.J.; Hyland, A.J.; Singh, A.K.; Rangnekar, V.M.; Cummings, K.M.; Marshall, J.R.; Kudrimoti, M.R. Accuracy of self-reported tobacco assessments in a head and neck cancer treatment population. Radiother. Oncol. 2012, 103, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Abdelmutti, N.; Brual, J.; Papadakos, J.; Fathima, S.; Goldstein, D.; Eng, L.; Liu, G.; Jones, J.; Giuliani, M. Implementation of a comprehensive smoking cessation program in cancer care. Curr. Oncol. 2019, 26, 361–368. [Google Scholar] [CrossRef]
- Kaiser, E.G.; Prochaska, J.J.; Kendra, M.S. Tobacco Cessation in Oncology Care. Oncology 2018, 95, 129–137. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall | Smoking | Cessated | |
|---|---|---|---|
| n = 503 (n%) | n = 186 (n%) | n = 317 (n%) | |
| Sex | |||
| Male | 389 (77.3) | 142 (76.3) | 247 (77.9) |
| Female | 114 (22.7) | 44 (23.7) | 70 (22.1) |
| Age | |||
| Median (Range) | 67 (37–96) | 64 (38–90) | 69 (37–96) |
| Marital Status | |||
| Single | 72 (14.3) | 42 (22.6) | 30 (9.5) |
| Married or Common-Law | 321 (63.8) | 96 (51.6) | 225 (71.0) |
| Separated or Divorced | 21 (4.2) | 13 (7.0) | 8 (2.5) |
| Widow/Widower | 63 (12.5) | 26 (14.0) | 37 (11.7) |
| Data not available | 24 (4.8) | 9 (4.8) | 15 (4.7) |
| ICD Diagnosis | |||
| Oral Cavity (C01–C06) | 186 (37.0) | 82 (44.1) | 104 (32.8) |
| Oropharynx (C09–C10) | 59 (11.7) | 21 (11.3) | 38 (12.0) |
| Larynx (C32) | 91 (18.1) | 34 (18.3) | 57 (18.0) |
| ICD codes not included above | 143 (28.4) | 40 (21.5) | 103 (32.5) |
| D00–D44 | 15 (3.0) | 5 (2.7) | 10 (3.2) |
| Stage | |||
| T1 | 120 (23.9) | 43 (23.1) | 77 (24.3) |
| T2 | 154 (30.6) | 62 (33.3) | 92 (29.0) |
| T3 | 80 (15.9) | 30 (16.1) | 50 (15.8) |
| T4 | 75 (14.9) | 33 (17.7) | 42 (13.2) |
| TX | 9 (1.8) | 5 (2.7) | n/a |
| Missing | 62 (12.3) | 12 (6.5) | 50 (15.8) |
| Physical Comorbidities | |||
| None | 171 (24.2) | 78 (31.8) | 93 (20.1) |
| Diabetes | 75 (10.6) | 17 (6.9) | 58 (12.5) |
| Hypertension | 196 (27.7) | 55 (22.4) | 141 (30.5) |
| Heart problems/heart failure | 82 (11.6) | 25 (10.2) | 57 (12.3) |
| Lung/COPD/Asthma | 52 (7.3) | 23 (9.4) | 29 (6.3) |
| Stroke/circulatory | 19 (2.7) | 7 (2.9) | 12 (2.6) |
| Other cancers | 105 (14.8) | 36 (14.7) | 69 (14.9) |
| Data not available | 8 (1.1) | n/a | n/a |
| n = 501; 708 responses | n = 186; 245 responses | n = 315; 463 responses | |
| Psychiatric Comorbidities | |||
| None | 462 (91.8) | 166 (89.2) | 296 (93.4) |
| Depression | 19 (3.8) | 11 (5.9) | 8 (2.5) |
| Anxiety | 9 (1.8) | n/a | 7 (2.2) |
| Depression & Anxiety | 8 (1.6) | 5 (2.7) | n/a |
| Alcohol Consumption | |||
| Yes | 300 (59.6) | 121 (65.1) | 179 (56.5) |
| No | 137 (27.2) | 47 (25.3) | 90 (28.4) |
| Data not available | 64 (12.7) | 18 (9.7) | 46 (14.5) |
| Alcohol Dependency | |||
| Yes | 62 (12.3) | 42 (22.6) | 20 (6.3) |
| No | 374 (74.4) | 125 (67.2) | 249 (78.5) |
| Data not available | 65 (12.9) | 19 (10.2) | 46 (14.5) |
| Drug Use | |||
| Yes | 6 (1.2) | n/a | n/a |
| No | 487 (96.8) | 178 (95.7) | 309 (97.5) |
| Data not available | 7 (1.4) | n/a | n/a |
| Overall | Smoking | Cessated | OR 1 | Adj OR 2 | |
|---|---|---|---|---|---|
| n = 503 (n%) | n = 186 (n%) | n = 317 (n%) | (95% CI) | (95% CI) | |
| Age started to smoke | |||||
| Median (Range) | 16 (4–60) | 15 (4–59) | 16 (4–60) | ||
| Number of years cessated (Ex-Smokers only) | |||||
| 0–1 years | 8 (2.5) | ||||
| 2–5 years | 70 (22.1) | ||||
| 6–10 years | 45 (14.2) | ||||
| 11–20 years | 56 (17.7) | ||||
| 21–30 years | 45 (14.2) | ||||
| 31–40 years | 55 (17.4) | ||||
| 41+ years | 36 (11.4) | ||||
| Missing | 2 (0.6) | ||||
| Duration Smoked (years) | |||||
| 1–30 | 193 (38.4) | 28 (15.1) | 165 (52.1) | 1.0 ref | 1.0 ref |
| 31–43 | 146 (29.0) | 59 (31.7) | 87 (27.4) | 3.97 (2.38–6.72) | 4.22 (2.30–7.74) |
| 44–75 | 163 (32.4) | 98 (52.7) | 65 (20.5) | 8.89 (5.34–14.78) | 19.59 (9.94–38.59) |
| Number of Cigarettes Smoked per Day | |||||
| 10 or less | 83 (16.5) | 15 (8.1) | 68 (21.5) | 1.0 ref | 1.0 ref |
| 11–20 | 199 (39.6) | 83 (44.6) | 116 (36.6) | 3.24 (1.73–6.07) | 3.44 (1.71–6.92) |
| 21–30 | 147 (29.2) | 65 (34.9) | 82 (25.9) | 3.59 (1.88–6.86) | 3.70 (1.79–7.65) |
| 31 or more | 71 (14.1) | 23 (12.4) | 48 (15.1) | 2.17 (1.03–4.59) | 2.18 (0.93–5.12) |
| Smoking Pack Years | |||||
| 25 or less | 181(36.0) | 35 (18.8) | 146 (46.1) | 1.0 ref | 1.0 ref |
| 26–50 | 183 (36.4) | 84 (45.2) | 99 (31.2) | 3.54 (2.21–5.66) | 4.25 (2.47–7.29) |
| 51 or higher | 136 (27.0) | 67 (36.0) | 69 (21.8) | 4.05 (2.46–6.67) | 6.16 (3.34–11.36) |
| Fagerstrom Test for Nicotine Dependence | |||||
| Very Low Dependence (0–2) | 100 (19.9) | 14 (7.5) | 86 (27.1) | 1.0 ref | 1.0 ref |
| Low Dependence (3–4) | 126 (25.0) | 47 (25.3) | 79 (24.9) | 3.66 (1.87–7.15) | 3.73 (1.82–7.65) |
| Medium Dependence (5) | 87 (17.3) | 44 (23.7) | 43 (13.6) | 6.29 (3.11–12.71) | 5.45 (2.57–11.52) |
| High Dependence (6–7) | 147 (29.2) | 63 (33.9) | 84 (26.5) | 4.61 (2.40–8.85) | 3.91 (1.92–7.95) |
| Very High Dependence (8–10) | 38 (7.6) | 18 (9.7) | 20 (6.3) | 5.53 (2.36–12.95) | 3.98 (1.55–10.25) |
| Missing | 5 (1.0) | 5 (1.6) | |||
| Heaviness of Smoking Index | |||||
| Very Low Dependence | 139 (27.6) | 27 (14.5) | 112 (35.3) | 1.0 ref | 1.0 ref |
| Low–Moderate Dependence | 116 (23.1) | 56 (30.1) | 60 (18.9) | 3.87 (2.22–6.75) | 3.52 (1.92–6.44) |
| Moderate Dependence | 114 (22.7) | 47 (25.3) | 67 (12.1) | 2.91 (1.66–5.10) | 2.57 (1.38–4.77) |
| Very High Dependence | 132 (26.2) | 56 (30.1) | 76 (24.0) | 3.06 (1.77–5.27) | 2.59 (1.42–4.75) |
| Time to First Cigarette | |||||
| 31 or more min | 145 (28.8) | 29 (15.6) | 116 (36.6) | 1.0 ref | 1.0 ref |
| 30 min or less | 356 (70.8) | 157 (84.4) | 199 (62.8) | 3.16 (2.00–4.99) | 2.67 (1.62–4.40) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santi, S.A.; Conlon, M.S.C.; Meigs, M.L.; Davidson, S.M.; Mispel-Beyer, K.; Saunders, D.P. Rates of Smoking Cessation at 6 and 12 Months after a Clinical Tobacco Smoking Cessation Intervention in Head and Neck Cancer Patients in Northern Ontario, Canada. Curr. Oncol. 2022, 29, 1544-1558. https://doi.org/10.3390/curroncol29030130
Santi SA, Conlon MSC, Meigs ML, Davidson SM, Mispel-Beyer K, Saunders DP. Rates of Smoking Cessation at 6 and 12 Months after a Clinical Tobacco Smoking Cessation Intervention in Head and Neck Cancer Patients in Northern Ontario, Canada. Current Oncology. 2022; 29(3):1544-1558. https://doi.org/10.3390/curroncol29030130
Chicago/Turabian StyleSanti, Stacey A., Michael S. C. Conlon, Margaret L. Meigs, Stacey M. Davidson, Kyle Mispel-Beyer, and Deborah P. Saunders. 2022. "Rates of Smoking Cessation at 6 and 12 Months after a Clinical Tobacco Smoking Cessation Intervention in Head and Neck Cancer Patients in Northern Ontario, Canada" Current Oncology 29, no. 3: 1544-1558. https://doi.org/10.3390/curroncol29030130
APA StyleSanti, S. A., Conlon, M. S. C., Meigs, M. L., Davidson, S. M., Mispel-Beyer, K., & Saunders, D. P. (2022). Rates of Smoking Cessation at 6 and 12 Months after a Clinical Tobacco Smoking Cessation Intervention in Head and Neck Cancer Patients in Northern Ontario, Canada. Current Oncology, 29(3), 1544-1558. https://doi.org/10.3390/curroncol29030130