Prognostic Significance of Tumor Growth Rate (TGR) in Patients with Huge Hepatocellular Carcinoma Undergoing Transcatheter Arterial Chemoembolization

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Patient Selection
2.2. TACE Procedure
2.3. Follow-Up and TGR Calculation
2.4. Statistical Analysis
3. Results
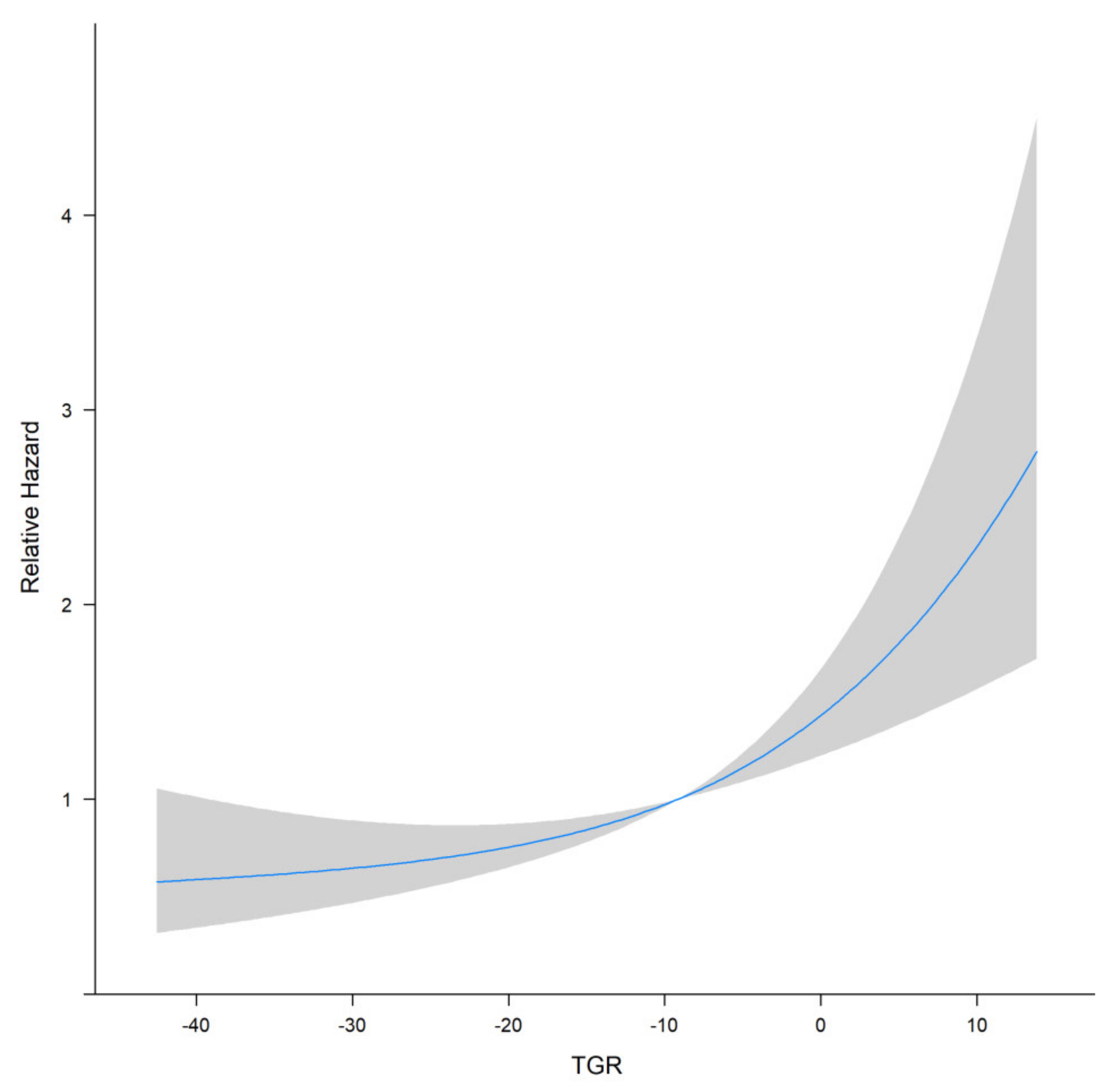
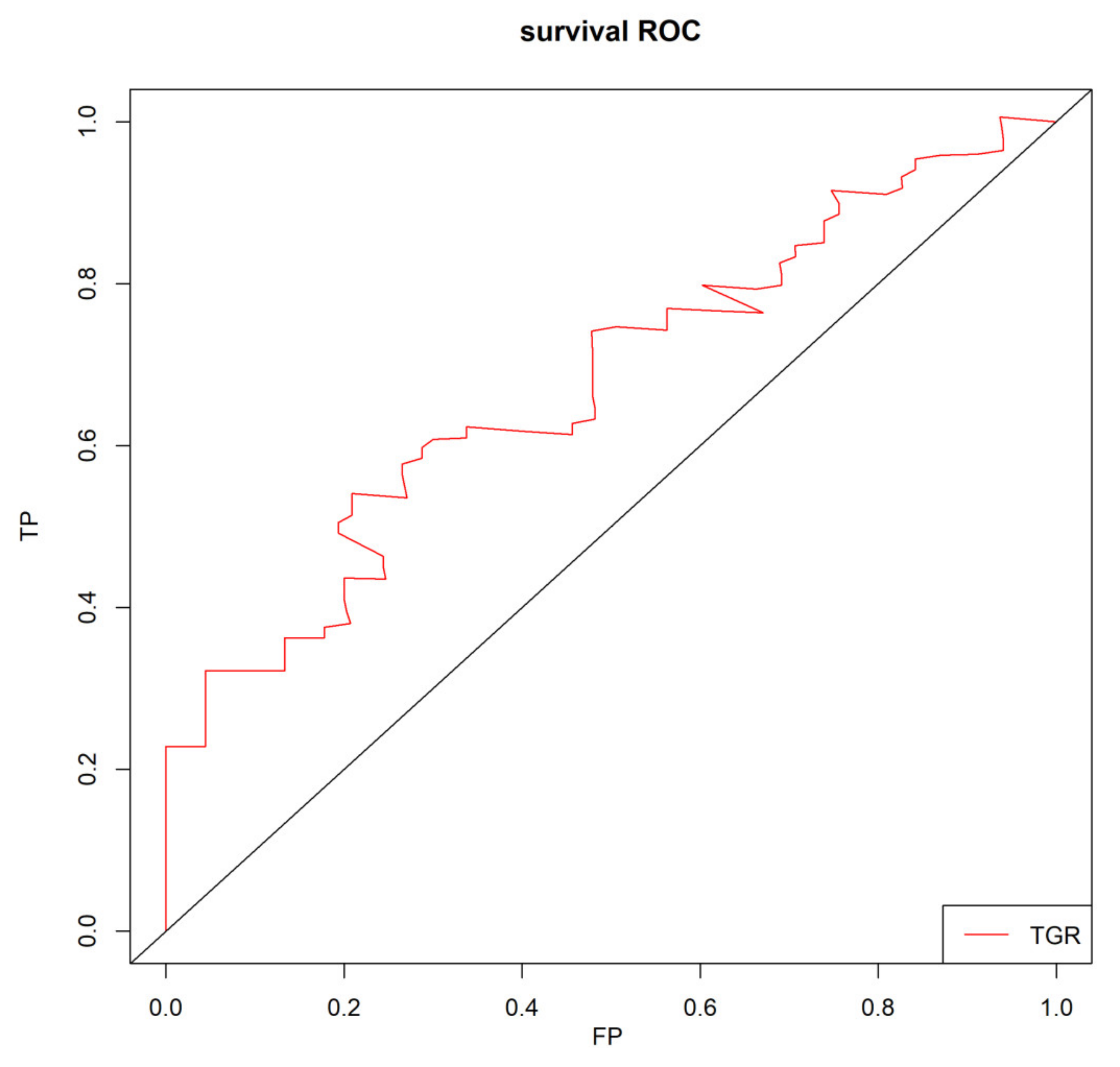
3.1. Optimal Cut-off Value for the TGR
3.2. Patients Characteristics and Overall Survival
3.3. Univariate and Multivariate Analysis
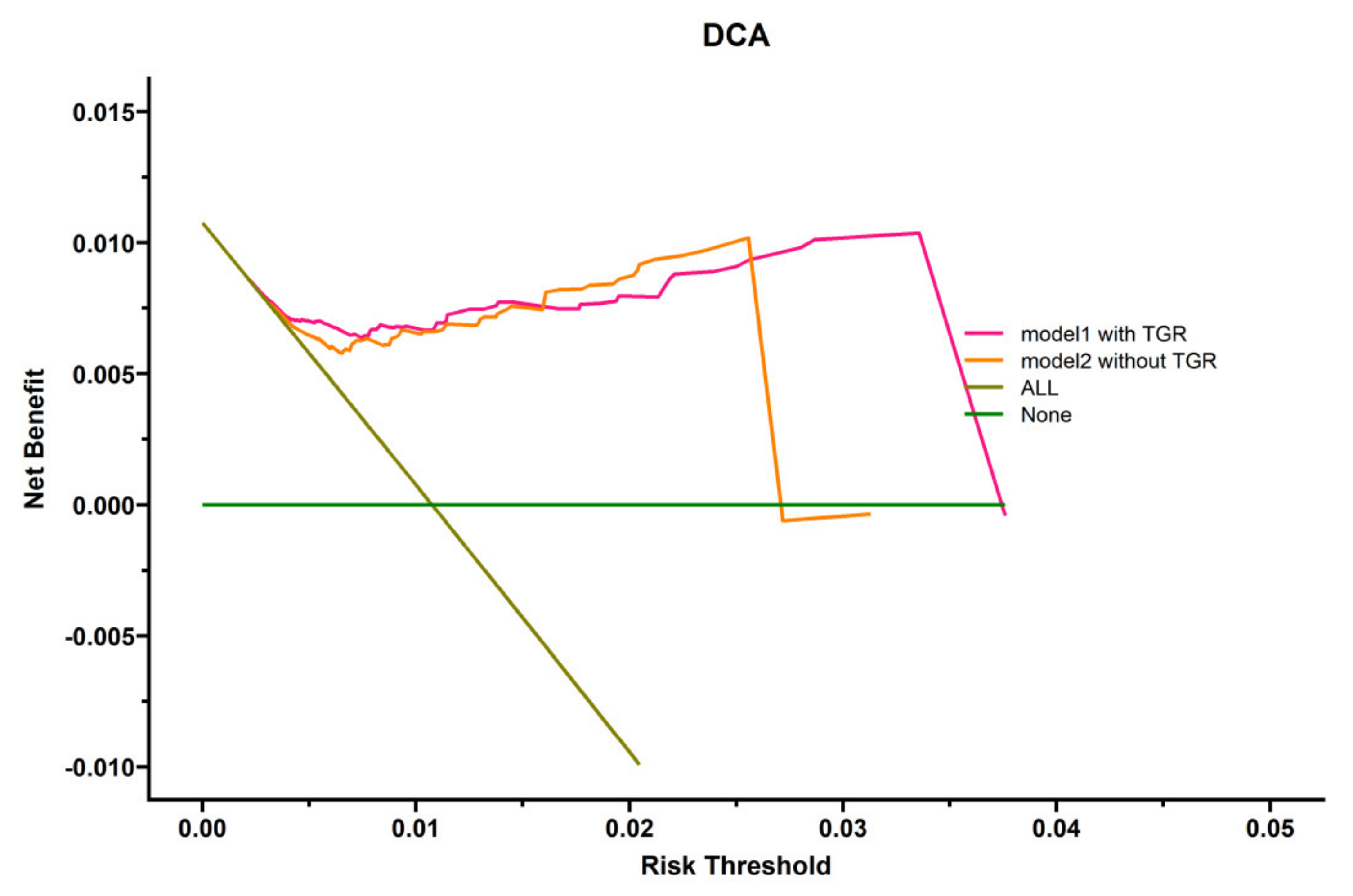
3.4. Clinical Value of TGR and Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Li, C.; Wang, M.D.; Lu, L.; Wu, H.; Yu, J.J.; Zhang, W.G.; Pawlik, T.M.; Zhang, Y.M.; Zhou, Y.H.; Gu, W.M.; et al. Preoperative transcatheter arterial chemoembolization for surgical resection of huge hepatocellular carcinoma (>/=10 cm): A multicenter propensity matching analysis. Hepatol. Int. 2019, 13, 736–747. [Google Scholar] [CrossRef]
- Wei, C.-Y.; Chen, P.-C.; Chau, G.-Y.; Lee, R.-C.; Chen, P.-H.; Huo, T.-I.; Huang, Y.-H.; Su, Y.-H.; Hou, M.-C.; Wu, J.-C.; et al. Comparison of prognosis between surgical resection and transarterial chemoembolization for patients with solitary huge hepatocellular carcinoma. Ann. Transl. Med. 2020, 8, 238. [Google Scholar] [CrossRef]
- Hidaka, T.; Anai, H.; Sakaguchi, H.; Sueyoshi, S.; Tanaka, T.; Yamamoto, K.; Morimoto, K.; Nishiofuku, H.; Maeda, S.; Nagata, T.; et al. Efficacy of combined bland embolization and chemoembolization for huge (>/=10 cm) hepatocellular carcinoma. Minim. Invasive Ther. Allied Technol. 2021, 30, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Miyayama, S.; Kikuchi, Y.; Yoshida, M.; Yamashiro, M.; Sugimori, N.; Ikeda, R.; Okimura, K.; Sakuragawa, N.; Ueda, T.; Sanada, T.; et al. Outcomes of conventional transarterial chemoembolization for hepatocellular carcinoma >/=10 cm. Hepatol. Res. 2019, 49, 787–798. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, N.; Fujiwara, Y.; Wang, X.; Ohmoto, A.; Urasaki, T.; Hayashi, N.; Sato, Y.; Nakano, K.; Yunokawa, M.; Ono, M.; et al. Tumor growth rate as a prognostic factor for metastatic or recurrent adenoid cystic carcinoma of the head and neck patients treated with carboplatin plus paclitaxel. Eur. Arch. Oto-Rhino-Laryngol. 2020, 278, 3037–3043. [Google Scholar] [CrossRef] [PubMed]
- He, L.N.; Zhang, X.; Li, H.; Chen, T.; Chen, C.; Zhou, Y.; Lin, Z.; Du, W.; Fang, W.; Yang, Y.; et al. Pre-Treatment Tumor Growth Rate Predicts Clinical Outcomes of Patients With Advanced Non-Small Cell Lung Cancer Undergoing Anti-PD-1/PD-L1 Therapy. Front. Oncol. 2020, 10, 621329. [Google Scholar] [CrossRef] [PubMed]
- Grande, E.; Martínez-Sáez, O.; Gajate-Borau, P.; Alonso-Gordoa, T. Translating new data to the daily practice in second line treatment of renal cell carcinoma: The role of tumor growth rate. World J. Clin. Oncol. 2017, 8, 100–105. [Google Scholar] [CrossRef]
- Lamarca, A.; Ronot, M.; Moalla, S.; Crona, J.; Opalinska, M.; Lopez, C.L.; Pezzutti, D.; Najran, P.; Carvhalo, L.; Bezerra, R.O.F.; et al. Tumor Growth Rate as a Validated Early Radiological Biomarker Able to Reflect Treatment-Induced Changes in Neuroendocrine Tumors: The GREPONET-2 Study. Clin. Cancer Res. 2019, 25, 6692–6699. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.G.; Kim, C.; Yoon, S.E.; Kim, K.H.; Choi, S.J.; Kang, B.; Kim, H.R.; Park, S.-H.; Shin, E.-C.; Kim, Y.-Y.; et al. Hyperprogressive disease during PD-1 blockade in patients with advanced hepatocellular carcinoma. J. Hepatol. 2021, 74, 350–359. [Google Scholar] [CrossRef] [PubMed]
- Ferté, C.; Koscielny, S.; Albiges, L.; Rocher, L.; Soria, J.-C.; Iacovelli, R.; Loriot, Y.; Fizazi, K.; Escudier, B. Tumor Growth Rate Provides Useful Information to Evaluate Sorafenib and Everolimus Treatment in Metastatic Renal Cell Carcinoma Patients: An Integrated Analysis of the TARGET and RECORD Phase 3 Trial Data. Eur. Urol. 2014, 65, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Fang, Q.; Xie, Q.-S.; Chen, J.-M.; Shan, S.-L.; Xie, K.; Geng, X.-P.; Liu, F.-B. Long-term outcomes after hepatectomy of huge hepatocellular carcinoma: A single-center experience in China. Hepatobiliary Pancreat. Dis. Int. 2019, 18, 532–537. [Google Scholar] [CrossRef]
- Jonas, S.; Bechstein, W.O.; Steinmüller, T.; Herrmann, M.; Radke, C.; Berg, T.; Settmacher, U.; Neuhaus, P. Vascular invasion and histopathologic grading determine outcome after liver transplantation for hepatocellular carcinoma in cirrhosis. Hepatology 2001, 33, 1080–1086. [Google Scholar] [CrossRef]
- Bruix, J.; Cheng, A.-L.; Meinhardt, G.; Nakajima, K.; De Sanctis, Y.; Llovet, J. Prognostic factors and predictors of sorafenib benefit in patients with hepatocellular carcinoma: Analysis of two phase III studies. J. Hepatol. 2017, 67, 999–1008. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.H.; Kim, J.H.; Shim, J.H.; Ko, H.-K.; Chu, H.H.; Shin, J.H.; Yoon, H.-K.; Ko, G.-Y.; Gwon, D.I. Chemoembolization for Single Large Hepatocellular Carcinoma with Preserved Liver Function: Analysis of Factors Predicting Clinical Outcomes in a 302 Patient Cohort. Life 2021, 11, 840. [Google Scholar] [CrossRef]
- Purcell, Y.; Sartoris, R.; Paradis, V.; Vilgrain, V.; Ronot, M. Influence of pretreatment tumor growth rate on objective response of hepatocellular carcinoma treated with transarterial chemoembolization. J. Gastroenterol. Hepatol. 2020, 35, 305–313. [Google Scholar] [CrossRef]
- Lencioni, R.; Montal, R.; Torres, F.; Park, J.-W.; Decaens, T.; Raoul, J.-L.; Kudo, M.; Chang, C.; Ríos, J.; Boige, V.; et al. Objective response by mRECIST as a predictor and potential surrogate end-point of overall survival in advanced HCC. J. Hepatol. 2017, 66, 1166–1172. [Google Scholar] [CrossRef] [Green Version]
- Bogdanovic, A.; Bulajic, P.; Masulovic, D.; Bidzic, N.; Zivanovic, M.; Galun, D. Liver resection versus transarterial chemoembolization for huge hepatocellular carcinoma: A propensity score matched analysis. Sci. Rep. 2021, 11, 4493. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Liu, Q.; Xiang, C.; Mao, X.; Yang, B.; Li, Q.; Zhou, Q.; Li, S.; Zhou, Z.; Chen, M. Multi-institutional validation of novel models for predicting the prognosis of patients with huge hepatocellular carcinoma. Int. J. Cancer 2021, 149, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, A. Hepatocellular Carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Li, L.; Wang, X.; Zhao, D.; Shan, G.; Wu, X.; Wang, M.; Liu, J.; Li, X. Comparison of Combination Stereotactic Body Radiotherapy Plus High-Intensity Focused Ultrasound Ablation Versus Stereotactic Body Radiotherapy Alone for Massive Hepatocellular Carcinoma. Med. Sci. Monit. 2018, 24, 8298–8305. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; Dai, F.; Zhao, T.; Tao, C.; Wang, L.; Ye, W.; Zhao, W. Transcatheter arterial chemoembolization monotherapy vs combined transcatheter arterial chemoembolization-percutaneous microwave coagulation therapy for massive hepatocellular carcinoma (>/=10 cm). Cancer Manag. Res. 2018, 10, 5273–5282. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | p-Value (OS) |
|---|---|---|
| Age | 55.99 ± 11.988 | 0.823 |
| Sex | ||
| Male | 89 (91.8%) | 0.248 |
| Female | 8 (8.2%) | |
| Hepatic Cirrhosis | ||
| No | 29 (29.9%) | 0.719 |
| Yes | 68 (70.1%) | |
| ECOG performance status | ||
| 0 | 46 (47.4%) | 0.065 |
| 1 | 51 (52.6%) | |
| Diabetes | ||
| No | 84 (86.6%) | 0.337 |
| Yes | 13 (13.4%) | |
| Hypertension | ||
| No | 79 (81.4%) | 0.380 |
| Yes | 18 (18.6%) | |
| HBV | ||
| No | 9 (9.3%) | 0.659 |
| Yes | 88 (90.7%) | |
| Largest tumor diameter (mm) | 130.15 ± 24.523 | 0.429 |
| VI or/and BDI | ||
| No | 46 (47.4%) | 0.657 |
| Yes | 51 (52.6%) | |
| PVTT | ||
| No | 39 (40.2%) | 0.033 |
| Yes | 58 (59.8%) | |
| Distant metastases | ||
| No | 71 (73.2%) | 0.027 |
| Yes | 26 (26.8%) | |
| Tumor number | ||
| Single | 55 (56.7%) | 0.999 |
| Multiple | 42 (43.3%) | |
| Subsequent combination therapy | ||
| No | 41 (42.3%) | 0.026 |
| Yes | 56 (57.7%) | |
| Baseline AFP | ||
| ≤400 | 39 (40.2%) | 0.735 |
| >400 | 53 (54.6%) | |
| Unknown | 5 (5.2%) | |
| Baseline TB (umol/l) | 17.56 ± 33.355 | 0.353 |
| Baseline ALB (g/l) | 40.44 ± 5.013 | 0.042 |
| Baseline ALT (U/L) | 50.01 ± 70.696 | 0.821 |
| Baseline AST (U/L) | 84.30 ± 103.765 | 0.662 |
| Baseline LDH (U/L) | 253.58 ± 101.547 | 0.072 |
| Baseline INR | 1.25 ± 1.634 | 0.051 |
| Baseline NLR | 4.12 ± 2.620 | 0.223 |
| Baseline PLR | 190.53 ± 91.734 | 0.779 |
| Baseline ALBI | −2.66 ± 0.579 | 0.326 |
| Baseline CRP | 29.19 ± 41.321 | 0.062 |
| Continuous TGR | −12.52 ± 19.186 | <0.001 |
| Categorical TGR | ||
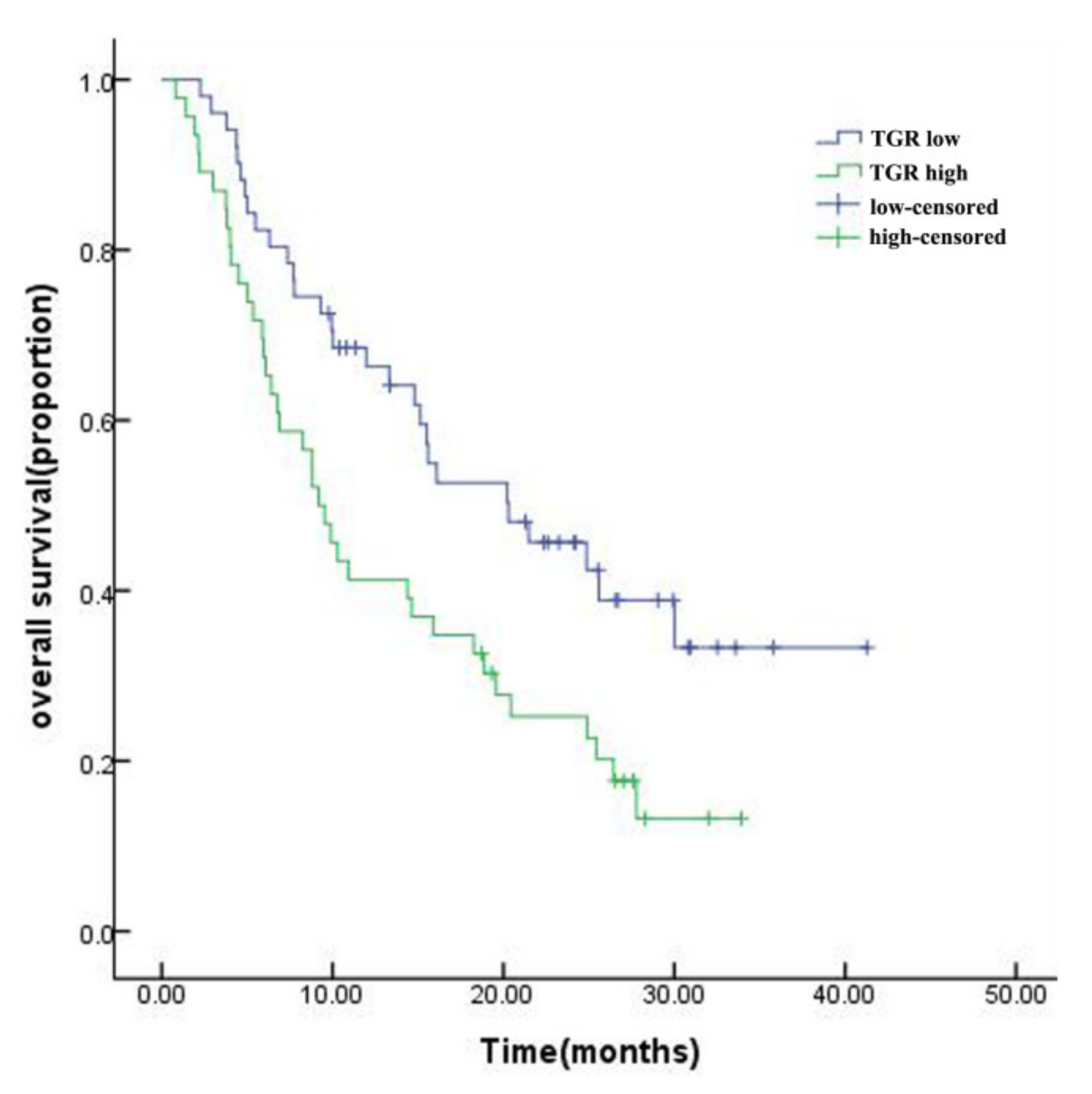
| Low (<−8.6) | 51 (52.6%) | 0.007 |
| High (≥−8.6) | 46 (47.4%) | |
| mRECIST evaluation | ||
| PR | 11 (11.4%) | 0.071 |
| SD | 69 (71.1%)) | |
| PD | 17 (17.5%) | |
| Characteristics | HR (95%CI) | p-Value |
|---|---|---|
| Categorical TGR | ||
| Low (<−8.6) | 1.00 (Ref) | 0.006 |
| High (≥−8.6) | 2.06 (1.23, 3.43) | |
| PVTT | ||
| No | 1.00 (Ref) | 0.016 |
| Yes | 1.93 (1.13, 3.27) | |
| Distant metastases | ||
| No | 1.00 (Ref) | 0.126 |
| Yes | 1.51 (0.89, 2.55) | |
| Subsequent combination therapy | ||
| No | 1.00 (Ref) | 0.047 |
| Yes | 0.59 (0.35, 0.99) | |
| Baseline ALB (g/l) | 0.96 (0.91, 1.00) | 0.071 |
| Categorical TGR | Subsequent Combination Therapy | Number | mOS | Log-Rank | p-Value | AIT | p-Value |
|---|---|---|---|---|---|---|---|
| TGR (<−8.6) | No | 18 (35.3%) | 15.5 ± 2.7 | 0.507 | 0.477 | ||
| Yes | 33 (64.7%) | 21.5 ± 5.3 | 2.06 ± 2.74 | 0.55 | |||
| TGR (≥−8.6) | No | 23 (50%) | 6.9 ± 2.9 | 4.312 | 0.038 | ||
| Yes | 23 (50%) | 9.9 ± 5.6 | 1.83 ± 2.08 | 0.59 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, G.; Xie, X.; Wang, M.; Guo, X.; Zhang, Z.; Zhang, L.; Zhang, B. Prognostic Significance of Tumor Growth Rate (TGR) in Patients with Huge Hepatocellular Carcinoma Undergoing Transcatheter Arterial Chemoembolization. Curr. Oncol. 2022, 29, 423-432. https://doi.org/10.3390/curroncol29020038
Chen G, Xie X, Wang M, Guo X, Zhang Z, Zhang L, Zhang B. Prognostic Significance of Tumor Growth Rate (TGR) in Patients with Huge Hepatocellular Carcinoma Undergoing Transcatheter Arterial Chemoembolization. Current Oncology. 2022; 29(2):423-432. https://doi.org/10.3390/curroncol29020038
Chicago/Turabian StyleChen, Guobin, Xiaoying Xie, Meixia Wang, Xinkun Guo, Zhenzhen Zhang, Lan Zhang, and Boheng Zhang. 2022. "Prognostic Significance of Tumor Growth Rate (TGR) in Patients with Huge Hepatocellular Carcinoma Undergoing Transcatheter Arterial Chemoembolization" Current Oncology 29, no. 2: 423-432. https://doi.org/10.3390/curroncol29020038
APA StyleChen, G., Xie, X., Wang, M., Guo, X., Zhang, Z., Zhang, L., & Zhang, B. (2022). Prognostic Significance of Tumor Growth Rate (TGR) in Patients with Huge Hepatocellular Carcinoma Undergoing Transcatheter Arterial Chemoembolization. Current Oncology, 29(2), 423-432. https://doi.org/10.3390/curroncol29020038