Highly Differentiated Follicular Carcinoma of Ovarian Origin: A Systematic Review of the Literature

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Eligibility Criteria
3. Results
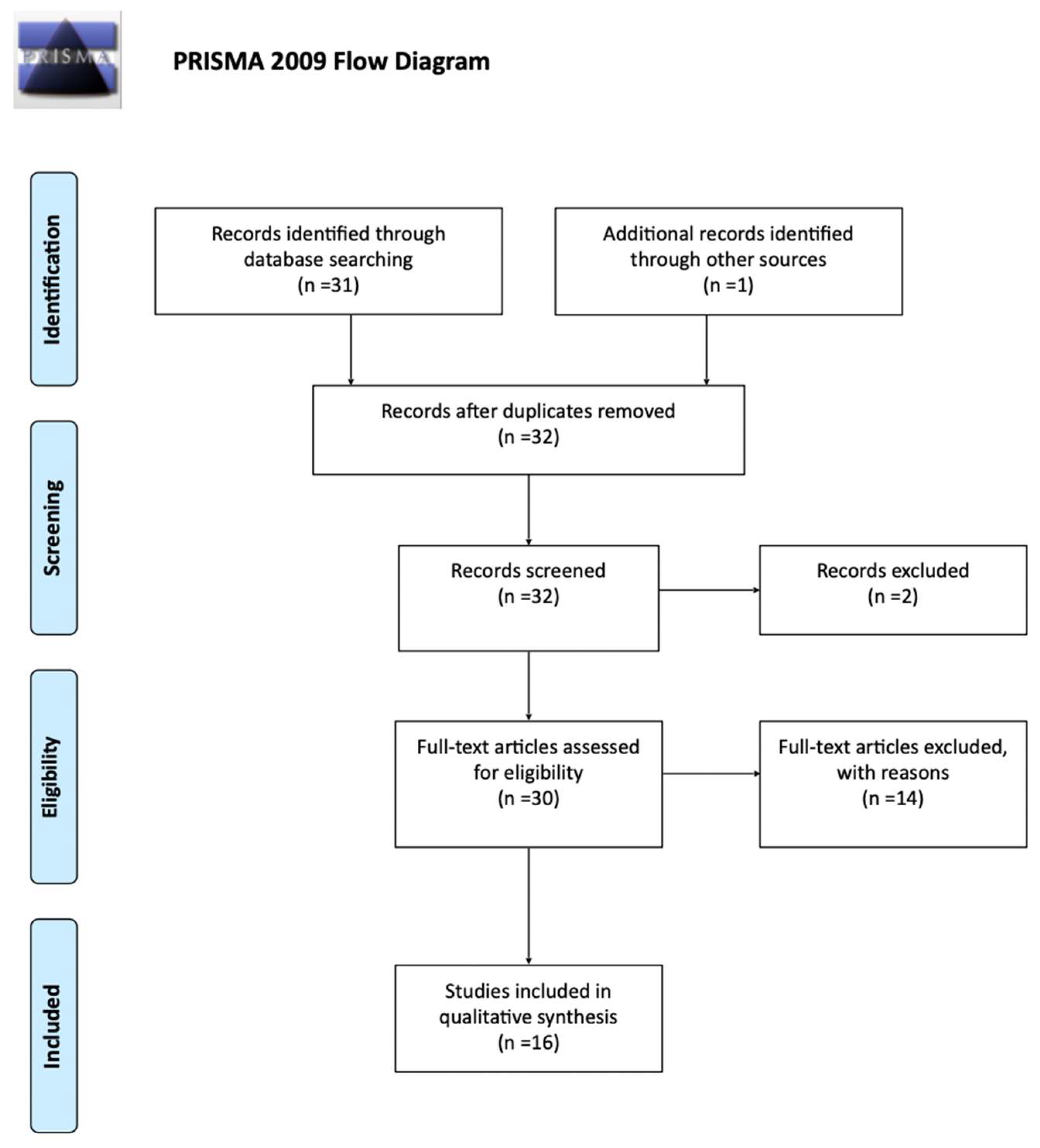
3.1. Included and Excluded Studies
3.2. Case Report
3.3. Characteristics of the Included Patients
3.4. Characteristics of the Lesions (Location, Size)
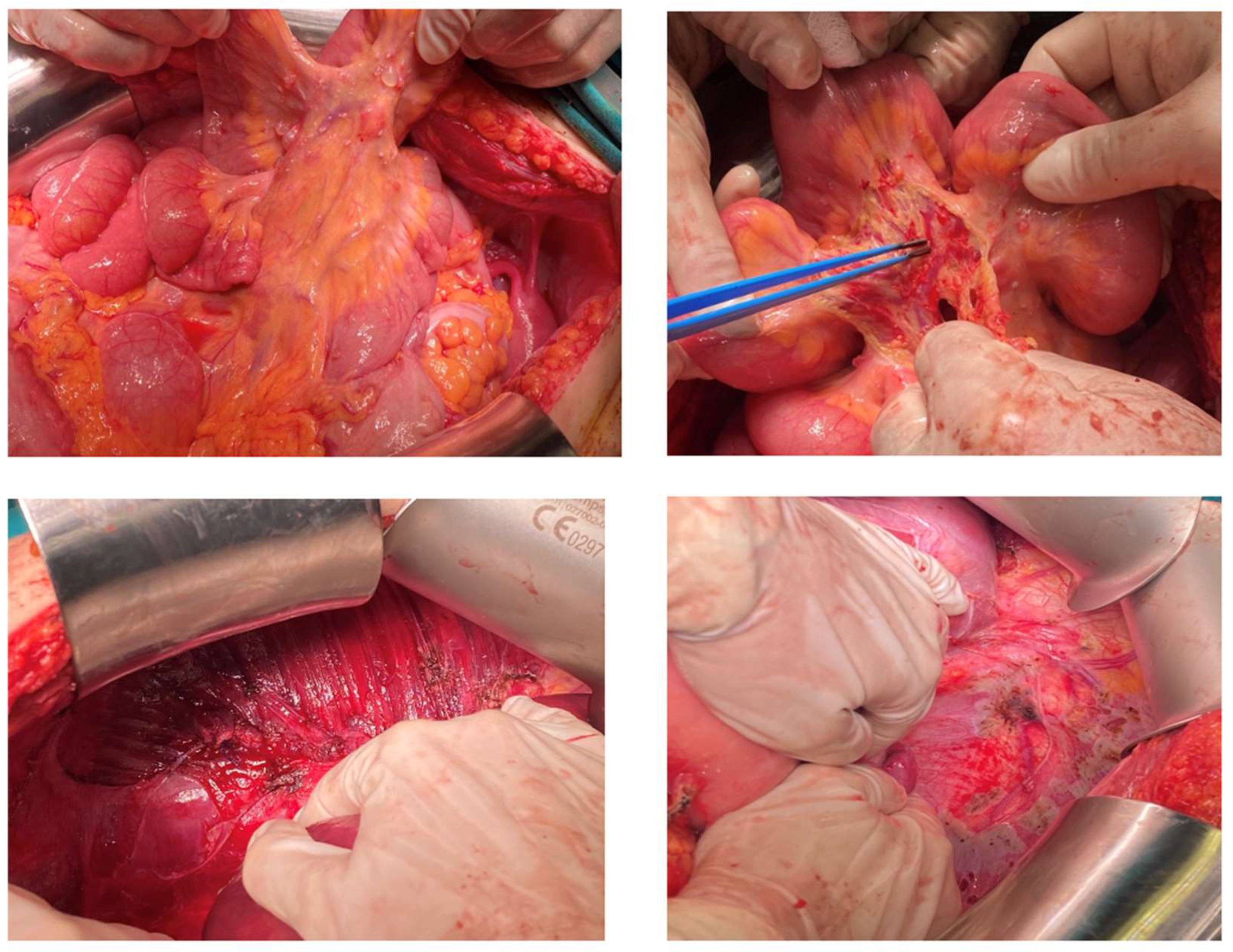
3.5. Surgical Technique and Outcomes
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dunzendorfer, T.; DeLas Morenas, A.; Kalir, T.; Levin, R.M. Struma Ovarii and Hyperthyroidism. Thyroid 1999, 9, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Willemse, P.H.; Oosterhuis, J.W.; Aalsers, J.G.; Piers, D.A.; Sleijfer, D.T.; Vermen, A.; Doorenbos, H. Malignant Struma Ovarii Treated by Ovariectomy, Thyroidectomy, and 131I Administration. Cancer 1987, 60, 178–182. [Google Scholar] [CrossRef]
- Chang, K.H.; Kim, Y.T.; Ryu, H.S.; Kwon, H.C.; Lee, E.J.; Lee, H.C.; Kim, J.W.; Oh, K.S. Clinical Diversity of Struma Ovarii. Korean J. Obstet. Gynecol. 2001, 40, 1683–1689. [Google Scholar]
- Young, R.H. New and Unusual Aspects of Ovarian Germ Cell Tumors. Am. J. Surg. Pathol. 1993, 17, 1210–1224. [Google Scholar] [CrossRef] [PubMed]
- Poli, R.; Scatolini, M.; Grosso, E.; Maletta, F.; Gallo, M.; Liscia, D.; Nelva, A.; Cesario, F.; Forte, G.; Metovic, J.; et al. Malignant Struma Ovarii: Next-Generation Sequencing of Six Cases Revealed Nras, Braf, and Jak3 Mutations. Endocrine 2021, 71, 216–224. [Google Scholar] [CrossRef]
- Anagnostou, E.; Polymeris, A.; Morphopoulos, G.; Travlos, A.; Sarantopoulou, V.; Papaspyrou, I. An Unusual Case of Malignant Struma Ovarii Causing Thyrotoxicosis. Eur. Thyroid. J. 2016, 5, 207–211. [Google Scholar] [CrossRef]
- WHO Classification of Tumours Online. In World Health Organization Classification of Tumours. 5th ed. Female Genital Tumours. Available online: https://tumourclassification.iarc.who.int/welcome/ (accessed on 5 October 2022).
- McCluggage, W.G.; Singh, N.; Gilks, C.B. Key Changes to the World Health Organization (WHO) Classification of Female Genital Tumours Introduced in the 5th Edition (2020). Histopathology 2022, 80, 762–778. [Google Scholar] [CrossRef]
- Hanby, A.M.; Walker, C.; Tavassoli, F.A.; Devilee, P. Pathology and Genetics: Tumours of the Breast and Female Genital Organs; WHO Classification of Tumours Series Publisher IARC: Lyon, France, 2003; 250p. [Google Scholar]
- Wei, S.; Baloch, Z.W.; LiVolsi, V.A. Pathology of Struma Ovarii: A Report of 96 Cases. Endocr. Pathol. 2015, 26, 342–348. [Google Scholar] [CrossRef]
- Checrallah, A.; Medlej, R.; Saadé, C.; Khayat, G.; Halaby, G. Malignant Struma Ovarii: An Unusual Presentation. Thyroid 2001, 11, 889–892. [Google Scholar] [CrossRef]
- Li, S.; Kong, S.; Wang, X.; Zhang, X.; Yin, M.; Yang, J. Survival Outcomes and Prognostic Predictors in Patients With Malignant Struma Ovarii. Front. Med. 2021, 8, 774691. [Google Scholar] [CrossRef]
- Rahma, A.; Mardiyana, L.; Fauziah, D. Malignant Struma Ovarii: Case Report of an Unusual Ovarian Tumor with CT Imaging. Radiol. Case Rep. 2022, 17, 1705–1708. [Google Scholar] [CrossRef] [PubMed]
- Gunasekaran, S.; Kopecka, E.; Maung, K.H.; England, R.J. Struma Ovarii and the Thyroid Surgeon. J. Laryngol. Otol. 2012, 126, 858–860. [Google Scholar] [CrossRef] [PubMed]
- Gottschalk, S. Ein Neuer Typus Einer Kleincystischen Bösartigen Eierstockgeschwulst. Arch. Gynäkol. 1899, 59, 676–698. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Available online: https://www.ncbi.nlm.nih.gov/pubmed/19621072 (accessed on 27 October 2019).
- Henderson, B.B.; Chaubey, A.; Roth, L.M.; Robboy, S.J.; Tarasidis, G.; Jones, J.R.; Sundermann, J.M.; Chou, J.; Craddock, A.L.; Stevenson, L.; et al. Whole-Genome and Segmental Homozygosity Confirm Errors in Meiosis as Etiology of Struma Ovarii. Cytogenet. Genome. Res. 2020, 160, 2–10. [Google Scholar] [CrossRef]
- Balasch, J.; Pahisa, J.; Marquez, M.; Ordi, J.; Fabregues, F.; Puerto, B.; Vanrell, J.A. Metastatic Ovarian Strumosis in an In-Vitro Fertilization Patient. Hum. Reprod. 1993, 8, 2075–2079. [Google Scholar] [CrossRef]
- Karseladze, A.I.; Kulinitch, S.I. Peritoneal Strumosis. Pathol. Res. Pract. 1994, 190, 1082–1085. [Google Scholar] [CrossRef]
- Brogsitter, C.; Wonsak, A.; Wurl, K.; Kotzerke, J. Peritoneal Strumosis. Eur. J. Nucl. Med. Mol. Imaging 2004, 31, 1057. [Google Scholar] [CrossRef]
- Roth, L.M.; Karseladze, A.I. Highly Differentiated Follicular Carcinoma Arising from Struma Ovarii: A Report of 3 Cases, a Review of the Literature, and a Reassessment of so-Called Peritoneal Strumosis. Int. J. Gynecol. Pathol. 2008, 27, 213–222. [Google Scholar] [CrossRef]
- Kim, D.; Cho, H.C.; Park, J.W.; Lee, W.A.; Kim, Y.M.; Chung, P.S.; Park, S.G.; Ahn, W.S.; Han, S.J.; Park, C.H. Struma ovarii and peritoneal strumosis with thyrotoxicosis. Thyroid 2009, 19, 305–308. [Google Scholar] [CrossRef]
- Sibio, S.; Borrini, F.; Sammartino, P.; Accarpio, F.; Biacchi, D.; Caprio, G.; Iafrate, F.; Baccheschi, A.M.; Cornali, T.; di Giorgio, A. Predominant Brenner Tumor Combined with Struma Ovarii Containing a Papillary Microcarcinoma Associated with Benign Peritoneal Strumosis: Report of a Case and Histologic Features. Endocr. Pathol. 2010, 21, 199–203. [Google Scholar] [CrossRef]
- Carey, K.; Jain, M.; Krishna, M.; Accurso, J. Peritoneal and Mediastinal Highly Differentiated Follicular Carcinoma of Ovarian Origin. Indian J. Nucl. Med. 2014, 29, 108–111. [Google Scholar] [CrossRef] [PubMed]
- Ranade, R.; Rachh, S.; Basu, S. Late Manifestation of Struma Peritonei and Widespread Functioning Lesions in the Setting of Struma Ovarii Simulating Highly Differentiated Follicular Carcinoma. J. Nucl. Med. Technol. 2015, 43, 231–233. [Google Scholar] [CrossRef] [PubMed]
- Riggs, M.J.; Kluesner, J.K.; Miller, C.R. Management of Highly Differentiated Thyroid Follicular Carcinoma of Ovarian Origin with a Minimally Invasive Approach. Gynecol. Oncol. Rep. 2018, 24, 87–89. [Google Scholar] [CrossRef] [PubMed]
- Dobi, A.; Kim, S.A.; Zhang, M.; Iames, E.; Lamzabi, I. Highly Differentiated Follicular Carcinoma of Ovary: Use of Imprint Cytology at Intraoperative Consultation. Diagn. Cytopathol. 2020, 48, 360–363. [Google Scholar] [CrossRef] [PubMed]
- Prentice, J.; Panter, K.; Attygalle, A.; Ind, T.; Prentice, M. Pure T3 Thyrotoxicosis from a Struma Ovarii Characterised by a Paradoxical Rise in Thyroxine on Treatment. Endocrinol. Diabetes Metab. Case Rep. 2020, 2020, 1–5. [Google Scholar] [CrossRef]
- Li, Z.; Wang, J.; Chen, Q. Struma Ovarii and Peritoneal Strumosis during Pregnancy. BMC Pregnancy Childbirth 2021, 21, 347. [Google Scholar] [CrossRef] [PubMed]
- Bao, Y.-T.; Wang, C.; Huang, W.; Yao, L.-Q.; Yuan, L. A Rare Case of Highly Differentiated Follicular Carcinoma in Ovary with FGFR4 Gly388Arg Polymorphism: A Case Report and Literature Review. J. Ovarian. Res. 2022, 15, 71. [Google Scholar] [CrossRef]
- Asaturova, A.; Magnaeva, A.; Tregubova, A.; Kometova, V.; Karamurzin, Y.; Martynov, S.; Lipatenkova, Y.; Adamyan, L.; Palicelli, A. Malignant Clinical Course of “Proliferative” Ovarian Struma: Diagnostic Challenges and Treatment Pitfalls. Diagnostics 2022, 12, 1411. [Google Scholar] [CrossRef] [PubMed]
- Roth, L.M.; Czernobilsky, B.; Roth, D.J.; Cheng, L. Highly Differentiated Follicular Thyroid-Type Carcinoma of the Ovary Reconsidered. J. Clin. Pathol. 2021, 74, 553–557. [Google Scholar] [CrossRef]
- Taelman, V.; Boer, M.; Taelman, P. Metastatic Malignant Struma Ovarii: A Case Report and Review of the Literature on the Management of Malignant Struma Ovarii. Acta Clin. Belg. 2022, 77, 721–725. [Google Scholar] [CrossRef]
- Cong, H.; Li, T.; Chen, G.; Liang, Z.; Liang, J.; Lin, Y. Missed Initial Diagnosis of Malignant Struma Ovarii Containing Follicular Thyroid Carcinoma: Metastatic Pulmonary Recurrence 17 Yr After Ovariectomy. Int. J. Gynecol. Pathol. 2015, 34, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Teale, E.; Gouldesbrough, D.R.; Peacey, S.R. Graves’ Disease and Coexisting Struma Ovarii: Struma Expression of Thyrotropin Receptors and the Presence of Thyrotropin Receptor Stimulating Antibodies. Thyroid 2006, 16, 791–793. [Google Scholar] [CrossRef] [PubMed]
- Gobitti, C.; Sindoni, A.; Bampo, C.; Baresic, T.; Giorda, G.; Alessandrini, L.; Canzonieri, V.; Franchin, G.; Borsatti, E. Malignant Struma Ovarii Harboring a Unique NRAS Mutation: Case Report and Review of the Literature. Hormones 2017, 16, 322–327. [Google Scholar] [CrossRef]
- Cui, Y.; Yao, J.; Wang, S.; Zhao, J.; Dong, J.; Liao, L. The Clinical and Pathological Characteristics of Malignant Struma Ovarii: An Analysis of 144 Published Patients. Front. Oncol. 2021, 11, 546. [Google Scholar] [CrossRef] [PubMed]
- Tsukada, T.; Yoshida, H.; Ishikawa, M.; Asami, Y.; Shiraishi, K.; Kato, T. Malignant Struma Ovarii Presenting with Follicular Carcinoma: A Case Report with Molecular Analysis. Gynecol. Oncol. Rep. 2019, 30, 100498. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Axiotis, C. Thyroid-Type Carcinoma of Struma Ovarii. Arch. Pathol. Lab. Med. 2010, 134, 786–791. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author; Year | Age (Years) | Previous Gynecologic Surgery | Diagnosis | Clinical Presentation | Lesion Location | Max Diameter of Ovarian Lesion | Ascites | Surgical Management | Thyroidectomy | RAI | Chemo-therapy | Follow-Up (Months) | Recurrence | Diagnosis |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Balasch et al., 1993 [18] | 36 | RO | SO | Incidental finding during IVF protocol | Left ovary, adnexa (Rt), omentum, large bowel | 8 cm | NO | LSO and local excision | NA (recommended) | NA | NO | NA | NA | Metastatic ovarian strumosis |
| Karselade; 1994 [19] | 49 | RSO | Simple cyst | Incidental finding during laparotomy | Left ovary; omentum | 5 cm | YES | TAH + LSO | NO | NO | YES | 36 | NED | Peritoneal strumosis |
| Brogsitter; 2004 [20] | 50 | NA | NA | NA | Right ovary, peritoneum | NA | NA | RSO and local excision | YES | YES | NO | 6 | NED | Benign strumosis |
| Roth et al., 2008 [21] | 58 | RSO; TAH + LSO | Ectopic pregnancy; SO | Incidental finding during laparotomy | Peritoneum, omentum, para-aortic lymph nodes | NA | NO | Excision of peritoneal/omental nodules and paraaortic lymph node, appendectomy, liver biopsy | YES | YES | NO | 96 | YES/2.5 y Repeat RAI LWD | HDFCO |
| 50 | NA | NA | Incidental finding during laparotomy | Right ovary, omentum, bladder serosa, Douglas pouch | 15 cm | NA | STAH + RSO, omentectomy and excision of peritoneal nodules | YES | YES | NO | 72 | NED | MSO (updated by Roth et al. as HDFCO) | |
| Kim et al., 2009 [22] | 49 | LO | Benign tumor (not specified) | Abdominal discomfort, palpitations, flush | Right ovary, omentum, bladder dome, rectosigmoid mesocolon, Douglas space | 10 cm | YES (300 mL) | TAH—right ovarian tumor excision, implant excision, bilateral pelvic lymphadenectomy | YES | YES | NO | 15 | NED | Peritoneal strumosis |
| Sibio et al., 2010 [23] | 74 | NO | NA | Pelvic pain | Right ovary, peritoneum | 13 cm | NA | TAH + BSO, implant excision, locoregional lymphadenectomy | Thyroidectomy (12 years) | NO | NO | 84 | NED | Brenner’s tumor and malignant struma ovarii with benign strumosis |
| Carey et al., 2014 [24] | 70 | TAH + BSO | Report not available | Asymptomatic | Peritoneal and epicardial nodule | NA | NA | Local excision and partial omentectomy (laparoscopic) | YES | YES | NO | 4 | LWD | Extraovarian struma ovarii |
| Ranade et al., 2014 [25] | 55 | YES (×2) type of surgery NA | Struma ovarii; Struma peritonei | NA | Adnexa, peritoneal nodules, liver, spleen, lungs | NA | NA | Biopsy of peritoneal nodules | YES | YES | NO | NA | LWD | HDFCO |
| Wei et al., 2015 [10] | 35 | NA | NA | NA | Right ovary, fallopian tube, urinary bladder, pelvic peritoneum | NA | NA | Excision of the mass and peritoneal nodules | NA | NA | NA | 204 | NED | HDFCO |
| Riggs et al., 2018 [26] | 32 | RSO; LSO | Mature teratoma (ruptured); simple cyst | Abdominal pain | Uterine serosa (anterior and posterior peritoneal reflections) | NA | NA | Modified hysterectomy and complete pelvic peritoneal resection (robotic-assisted laparoscopy) | No (thyroid preservation) | NO | NO | 12 | NED | HDFCO |
| Dobi et al., 2019 [27] | 52 | NA | N | Abdominal bloating | Uterus, bowel serosa, omentum | 12.5 cm | YES | TAH + BSO, omentectomy, rectosigmoid resection and anastomosis, left pelvic and common iliac lymphadenectomy | NO | NO | NO | 12 | NED | HDFCO |
| Prentice et al., 2020 [28] | 33 | Ovarian cystectomy | SO (piecemeal extraction) | Incidental finding during follow-up | Peritoneum, pelvic sidewall, pararectal spaces, uterosacral ligaments | NA | NA | N/A | YES | YES | NO | NA | NED | HDFCO |
| Henderson, 2020 [17] | 71 | NA | Pelvic dermoid | Right temporomandibular joint discomfort and facial swelling | Face, bones, liver, heart | NA | NA | Biopsy of facial and heart lesions | YES | YES | NO | 18 | NED | Multifocal metastatic struma ovarii |
| 58 | NA | SO | NA | Not specified para-aortic lymph node | NA | NA | NA | NA | NA | NA | NA | NA | Extraovarian struma ovarii | |
| 31 | RSO | SO | NA | Not specified peritoneum | 8 cm | NA | NA | NA | NA | NA | NA | NA | Extraovarian struma ovarii | |
| Li et al., 2021 [29] | 39 | Bilateral ovarian cystectomy (LAP) | SO (intact extraction) | Incidental finding during follow-up | Ovary, fallopian tube, uterus, urinary bladder, pelvic wall, sigmoid colon | NA | NO | Open surgery (during caesarian section), resection of ovarian mass, and local lesion excision | NO | NO | NO | NA | NA | Peritoneal strumosis |
| Bao et al., 2022 [30] | 38 | Ovarian cystectomy Rt; ovarian cystectomy Rt; ovarian cystectomy Rt and lesion excision | OMCT; SO; HDFCO | NA | Ovary, peritoneum, rectus abdominis, rectum, para-aortic lymph nodes | 2 cm | NA | TLH + BSO, omentectomy, pelvic and para-aortic lymphadenectomy, local excision | YES | YES | NO | 10 | NED | HDFCO |
| Asaturova et al., 2022 [31] | 38 | Ovarian cystectomy during CS | SO | Lower back pain | Ovary, lumbar vertebra, omentum, Sigmoid | 3.5 cm | NA | Laparoscopic LO, omentectomy and local excision | NO (patient’s refusal) | NO | NO | 17 | NED | HDFCO |
| Giovannopoulou et al., 2022 | 25 | Ovarian cystectomy; RSO | Mature teratoma; struma ovarii | Asymptomatic | Left ovary, peritoneum, mesentery, bowel serosa, subdiaphragmatic peritoneum | 6 cm | NO | Optimal debulking uterine preservation, LSO, omentectomy, Pelvic, paracolic, subdiaphragmatic, and bladder peritoneum, appendectomy | YES | YES | NO | 15 | NED | HDFCO |
| Total | 47.15 (25–74) | 92.9% previous gynecologic surgery | 62.5 % previous diagnosis of SO | 57.1% asymptomatic | 60% ovarian 15% extraperitoneal disease | 8.3 (2–15) cm | 42.9% | 35.3% uterine-sparing, 41.2% radical, 11.8% biopsies, 11.8% local excision (previous TAH + BSLO) | 62.5%% combined thyroidectomy and RA, 31.3% no additional therapy, 6.3% chemotherapy | 42.9 months (4–204) | 81.25% NED 12.5% LWD 6.25% recurrence | 50% HDFCO 50% other terminology | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giovannopoulou, E.; Saliaris, K.; Kavoura, E.; Pavlakis, K.; Lathouras, K. Highly Differentiated Follicular Carcinoma of Ovarian Origin: A Systematic Review of the Literature. Curr. Oncol. 2022, 29, 9105-9116. https://doi.org/10.3390/curroncol29120712
Giovannopoulou E, Saliaris K, Kavoura E, Pavlakis K, Lathouras K. Highly Differentiated Follicular Carcinoma of Ovarian Origin: A Systematic Review of the Literature. Current Oncology. 2022; 29(12):9105-9116. https://doi.org/10.3390/curroncol29120712
Chicago/Turabian StyleGiovannopoulou, Eirini, Konstantinos Saliaris, Evangelia Kavoura, Kitty Pavlakis, and Konstantinos Lathouras. 2022. "Highly Differentiated Follicular Carcinoma of Ovarian Origin: A Systematic Review of the Literature" Current Oncology 29, no. 12: 9105-9116. https://doi.org/10.3390/curroncol29120712
APA StyleGiovannopoulou, E., Saliaris, K., Kavoura, E., Pavlakis, K., & Lathouras, K. (2022). Highly Differentiated Follicular Carcinoma of Ovarian Origin: A Systematic Review of the Literature. Current Oncology, 29(12), 9105-9116. https://doi.org/10.3390/curroncol29120712