Impact of Pre-Treatment NLR and Other Hematologic Biomarkers on the Outcomes of Early-Stage Non-Small-Cell Lung Cancer Treated with Stereotactic Body Radiation Therapy

Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics
3.2. Survival Analysis
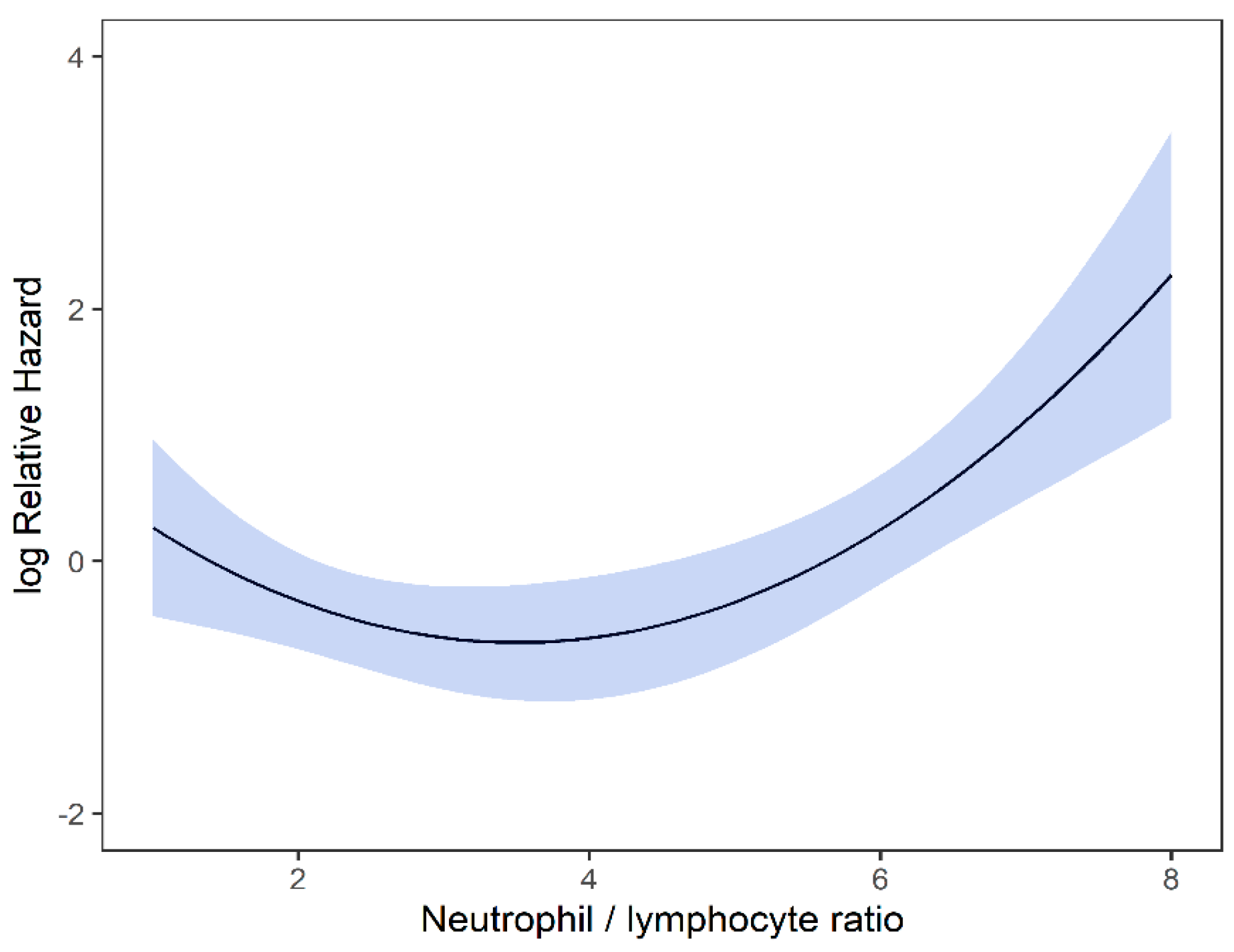
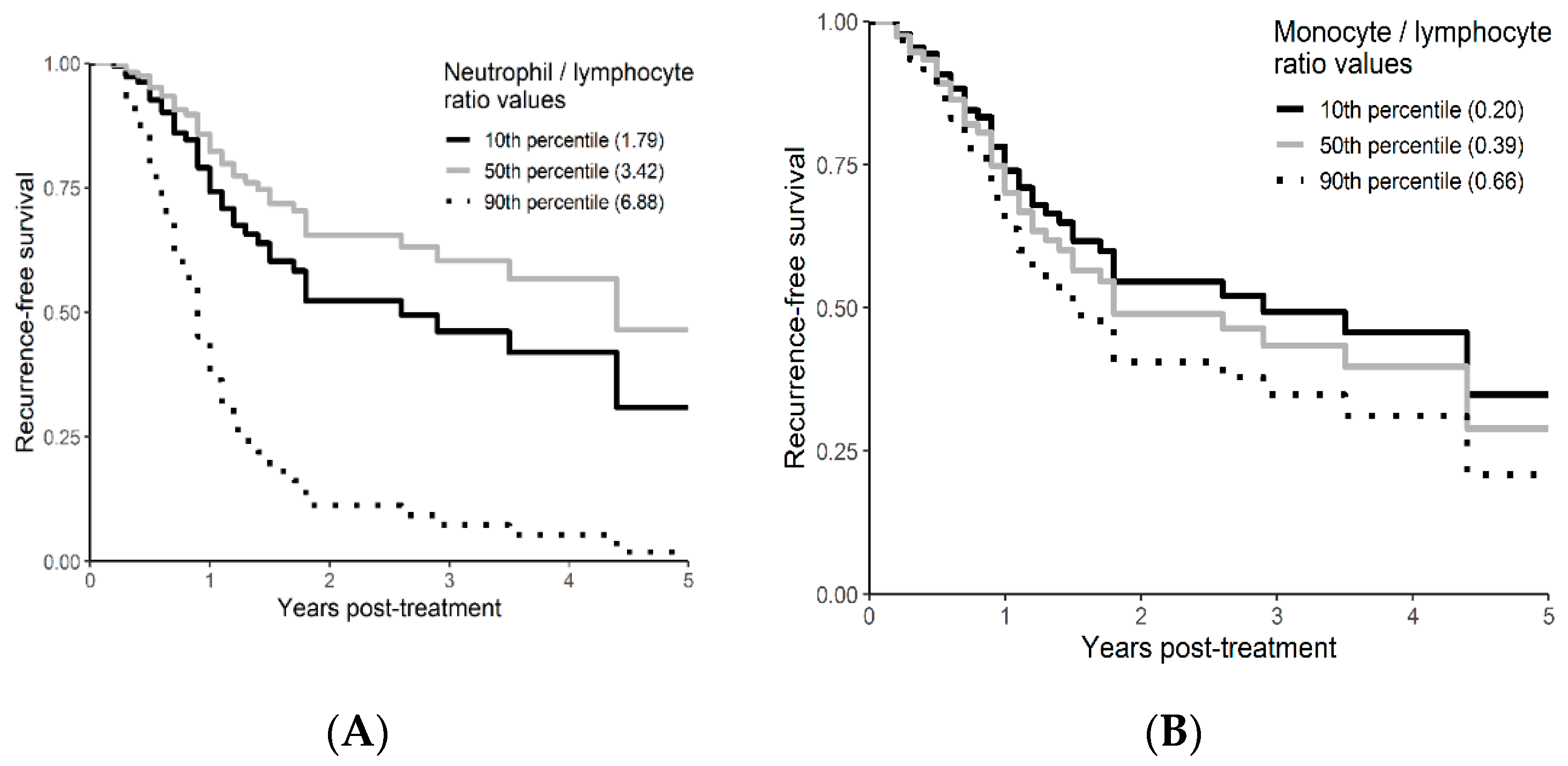
3.3. Recurrence Free Survival Analysis
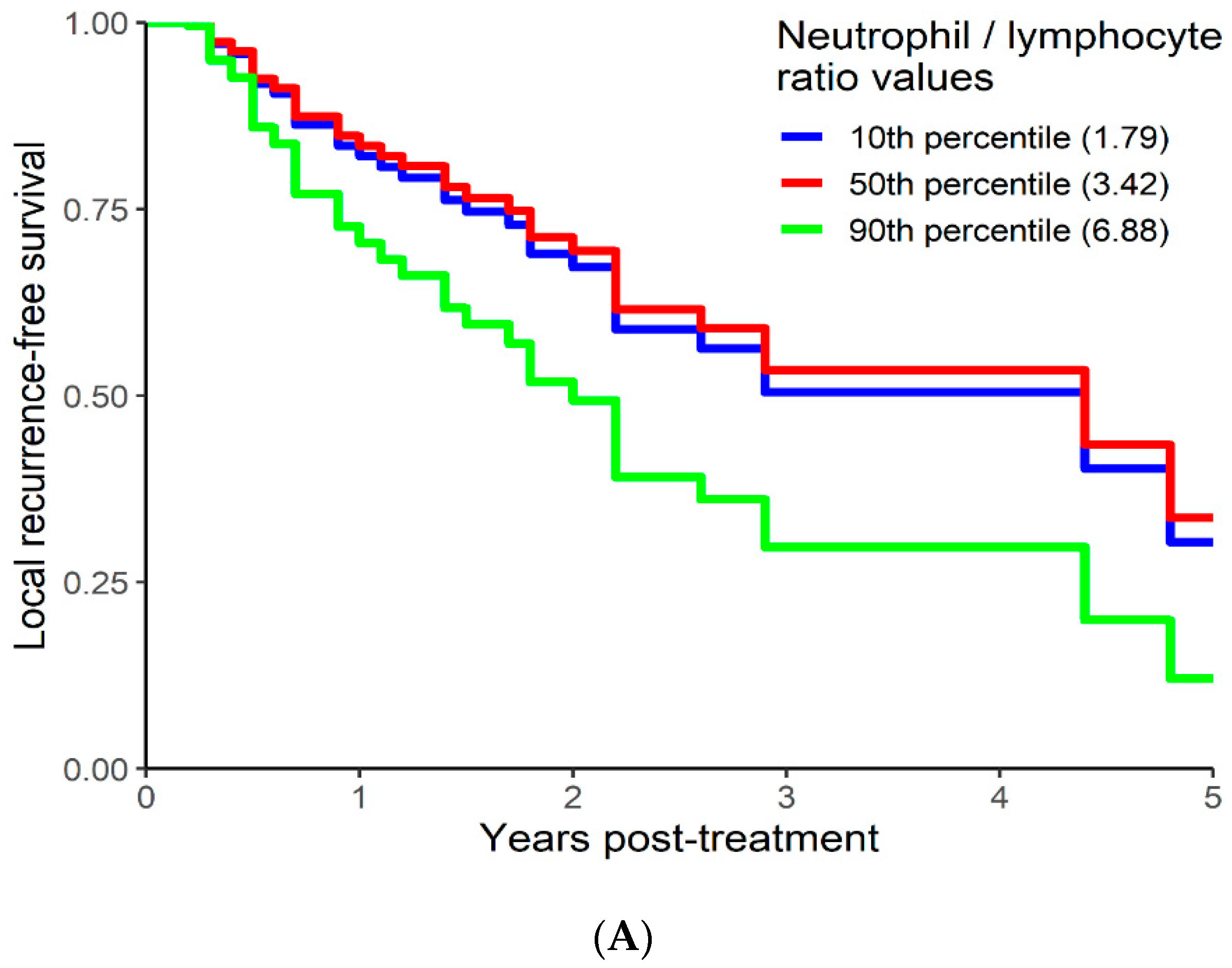
3.4. Local Recurrence Free Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chang, J.Y.; Senan, S.; Paul, M.A.; Mehran, R.J.; Louie, A.V.; Balter, P.; Groen, H.J.M.; E McRae, S.E.; Widder, J.; Feng, L.; et al. Stereotactic ablative radiotherapy versus lobectomy for operable stage I non-small-cell lung cancer: A pooled analysis of two randomised trials. Lancet Oncol. 2015, 16, 630–637. [Google Scholar] [CrossRef]
- Timmerman, R.; Paulus, R.; Galvin, J.; Michalski, J.; Straube, W.; Bradley, J.; Fakiris, A.; Bezjak, A.; Videtic, G.; Johnstone, D.; et al. Stereotactic body radiation therapy for inoperable early stage lung cancer. JAMA 2010, 303, 1070–1076. [Google Scholar] [CrossRef]
- Brown, J.M.; Carlson, D.J.; Brenner, D.J. The Tumor radiobiology of SRS and SBRT: Are more than the 5 Rs involved? Int. J. Radiat. Oncol. 2014, 88, 254–262. [Google Scholar] [CrossRef]
- Reese, A.S.; Feigenberg, S.J.; Husain, A.; Webb, T.; Hausner, P.F.; Edelman, M.; Feliciano, J.; Tkaczuk, K.H.; Sharma, N.K. Stereotactic Ablative Radiotherapy (SABR): Impact on the immune system and potential for future therapeutic modulation. Mol. Cell. Pharmacol. 2013, 5, 19–25. [Google Scholar]
- Song, C.W.; Kim, M.-S.; Cho, L.C.; Dusenbery, K.; Sperduto, P.W. Radiobiological basis of SBRT and SRS. Int. J. Clin. Oncol. 2014, 19, 570–578. [Google Scholar] [CrossRef]
- Gu, X.; Sun, S.; Gao, X.-S.; Xiong, W.; Qin, S.; Qi, X.; Ma, M.; Li, X.; Zhou, D.; Wang, W.; et al. Prognostic value of platelet to lymphocyte ratio in non-small cell lung cancer: Evidence from 3430 patients. Sci. Rep. 2016, 6, 23893. [Google Scholar] [CrossRef]
- Asher, V.; Lee, J.; Innamaa, A.; Bali, A. Preoperative platelet lymphocyte ratio as an independent prognostic marker in ovarian cancer. Clin. Trans. Oncol. 2011, 13, 499–503. [Google Scholar] [CrossRef]
- Huang, S.H.; Waldron, J.; Milosevic, M.; Shen, X.; Ringash, J.; Su, J.; Tong, L.; Perez-Ordonez, B.; Weinreb, I.; Bayley, A.J.; et al. Prognostic value of pretreatment circulating neutrophils, monocytes, and lymphocytes in oropharyngeal cancer stratified by human papillomavirus status. Cancer 2014, 121, 545–555. [Google Scholar] [CrossRef]
- Kwon, H.-C.; Kim, S.H.; Oh, S.Y.; Lee, S.; Lee, J.H.; Choi, H.-J.; Park, K.-J.; Roh, M.S.; Kim, S.-G.; Kim, H.-J.; et al. Clinical significance of preoperative neutrophil-lymphocyte versus platelet-lymphocyte ratio in patients with operable colorectal cancer. Biomarkers 2012, 17, 216–222. [Google Scholar] [CrossRef]
- Zhou, X.; Du, Y.; Huang, Z.; Xu, J.; Qiu, T.; Wang, J.; Wang, T.; Zhu, W.; Liu, P. Prognostic value of plr in various cancers: A meta-analysis. PLoS ONE 2014, 9, e101119. [Google Scholar] [CrossRef]
- Senthi, S.; Lagerwaard, F.J.; Haasbeek, C.J.; Slotman, B.; Senan, S. Patterns of disease recurrence after stereotactic ablative radiotherapy for early stage non-small-cell lung cancer: A retrospective analysis. Lancet Oncol. 2012, 13, 802–809. [Google Scholar] [CrossRef]
- van den Berg, L.L.; Klinkenberg, T.J.; Groen, H.J.M.; Widder, J. Patterns of recurrence and survival after surgery or stereotactic radiotherapy for early stage NSCLC. J. Thorac. Oncol. 2015, 10, 826–831. [Google Scholar] [CrossRef]
- Brooks, E.D.; Sun, B.; Feng, L.; Verma, V.; Zhao, L.; Gomez, D.R.; Liao, Z.; Jeter, M.; O’Reilly, M.; Welsh, J.W.; et al. Association of long-term outcomes and survival with multidisciplinary salvage treatment for local and regional recurrence after stereotactic ablative radiotherapy for early-stage lung cancer. JAMA Netw. Open 2018, 1, e181390. [Google Scholar] [CrossRef]
- Figlia, V.; Mazzola, R.; Cuccia, F.; Alongi, F.; Mortellaro, G.; Cespuglio, D.; Cucchiara, T.; Iacoviello, G.; Valenti, V.; Molino, M.; et al. Hypo-fractionated stereotactic radiation therapy for lung malignancies by means of helical tomotherapy: Report of feasibility by a single-center experience. La Radiol. Med. 2018, 123, 406–414. [Google Scholar] [CrossRef]
- Bezjak, A.; Paulus, R.; Gaspar, L.E.; Timmerman, R.D.; Straube, W.L.; Ryan, W.F.; Garces, Y.I.; Pu, A.T.; Singh, A.K.; Videtic, G.M.; et al. Safety and efficacy of a five-fraction stereotactic body radiotherapy schedule for centrally located non–small-cell lung cancer: NRG oncology/RTOG 0813 trial. J. Clin. Oncol. 2019, 37, 1316–1325. [Google Scholar] [CrossRef]
- Royston, P.; Altman, D.G.; Sauerbrei, W. Dichotomizing continuous predictors in multiple regression: A bad idea. Stat. Med. 2006, 25, 127–141. [Google Scholar] [CrossRef]
- Altman, D.G.; Royston, P. The cost of dichotomising continuous variables. BMJ 2006, 332, 1080. [Google Scholar] [CrossRef]
- Califf, R.M.; Phillips, H.R., III; Hindman, M.C.; Mark, B.D.; Lee, K.L.; Behar, V.S.; Johnson, R.A.; Pryor, D.B.; Rosati, R.A.; Wagner, G.S.; et al. Prognostic value of a coronary artery jeopardy score. J. Am. Coll. Cardiol. 1985, 5, 1055–1063. [Google Scholar] [CrossRef]
- Gerds, T.A.; Cai, T.; Schumacher, M. The performance of risk prediction models. Biom. J. 2008, 50, 457–479. [Google Scholar] [CrossRef]
- Burnham, K.P.; Anderson, D.R. Model Selection and Multimodel Inference: A Practical Information-Theoretic Approach, 2nd ed.; Springer: New York, NY, USA, 2002. [Google Scholar]
- Hall, C.A. Logistic Regression Models; CRC Press: Boca Raton, FL, USA, 2009. [Google Scholar]
- Roxburgh, C.S.D.; McMillan, D.C. Cancer and systemic inflammation: Treat the tumour and treat the host. Br. J. Cancer 2014, 110, 1409–1412. [Google Scholar] [CrossRef]
- Cannon, N.A.; Meyer, J.; Iyengar, P.; Ahn, C.; Westover, K.; Choy, H.; Timmerman, R. Neutrophil–lymphocyte and platelet–lymphocyte ratios as prognostic factors after stereotactic radiation therapy for early-stage non–small-cell lung cancer. J. Thorac. Oncol. 2015, 10, 280–285. [Google Scholar] [CrossRef]
- Shaverdian, N.; Veruttipong, D.; Wang, J.; Schaue, D.; Kupelian, P.; Lee, P. Pretreatment immune parameters predict for overall survival and toxicity in early-stage non–small-cell lung cancer patients treated with stereotactic body radiation therapy. Clin. Lung Cancer 2016, 17, 39–46. [Google Scholar] [CrossRef]
- Giuliani, M.; Sampson, L.; Wong, O.; Gay, J.; Le, L.; Cho, B.; Brade, A.; Sun, A.; Bezjak, A.; Hope, A. Prognostic value of pretreatment circulating neutrophils, monocytes, and lymphocytes on outcomes in lung stereotactic body radiotherapy. Curr. Oncol. 2016, 23, 362–368. [Google Scholar] [CrossRef][Green Version]
- Kotha, N.V.; Cherry, D.R.; Bryant, A.K.; Nalawade, V.; Stewart, T.F.; Rose, B.S. Prognostic utility of pretreatment neutrophil-lymphocyte ratio in survival outcomes in localized non-small cell lung cancer patients treated with stereotactic body radiotherapy: Selection of an ideal clinical cutoff point. Clin. Transl. Radiat. Oncol. 2021, 28, 133–140. [Google Scholar] [CrossRef]
- Song, C.W.; Glatstein, E.; Marks, L.B.; Emami, B.; Grimm, J.; Sperduto, P.W.; Kim, M.-S.; Hui, S.; Dusenbery, K.E.; Cho, L.C. Biological principles of Stereotactic Body Radiation Therapy (SBRT) and Stereotactic Radiation Surgery (SRS): Indirect cell death. Int. J. Radiat. Oncol. 2021, 110, 21–34. [Google Scholar] [CrossRef]
- Finkelstein, S.E.; Timmerman, R.; McBride, W.H.; Schaue, D.; Hoffe, S.E.; Mantz, C.A.; Wilson, G. The confluence of stereotactic ablative radiotherapy and tumor immunology. Clin. Dev. Immunol. 2011, 2011, 439752. [Google Scholar] [CrossRef]
- Matsumura, S.; Wang, B.; Kawashima, N.; Braunstein, S.; Badura, M.; Cameron, T.O.; Babb, J.; Schneider, R.; Formenti, S.C.; Dustin, M.; et al. Radiation-induced CXCL16 release by breast cancer cells attracts effector T cells. J. Immunol. 2008, 181, 3099–3107. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Frequency |
|---|---|
| Patients (n) | 61 |
| Sex (n (%)) | |
| Female | 41 (67.2%) |
| Male | 20 (32.8%) |
| Age (years) | |
| Mean (SD) | 77.5 (6.6) |
| Median (Q1, Q3) | 78 (72, 82) |
| Range | 72–82 |
| ECOG (n (%)) | |
| 0 | 11 (18.0%) |
| 1–2 | 37 (60.7%) |
| missing | 13 (21.3%) |
| ITV (cm³) | |
| Mean (SD) | 18.0 (17.7) |
| Median (Q1, Q3) | 11.2 (6.9, 20.8) |
| Range | 1.10–94.80 |
| PET SUV max (SD) | 10.4 (6.2) |
| Histopathological diagnosis (total patients) (n (%)) | 32 (57.4%) |
| Adenocarcinoma | 15 (24.6%) |
| Squamous cell carcinoma | 10 (16.4%) |
| NSCLC | 5 (8.2%) |
| Atypical cells | 1 (1.6%) |
| Tumor size (cm) | |
| Mean (SD) | 2.35 (1.0) |
| Median (Q1, Q3) | 2.1 (1.6, 2.8) |
| Range | 1.1–5.2 |
| Clinical stage (n (%)) | |
| T1A | 50 (82%) |
| T1B | 10 (16.4%) |
| T2A | 1 (1.6%) |
| SBRT dose/fractions (n (%)) | |
| 60 Gy in 8 fractions | 9 (14.8%) |
| 48 Gy in 4 fractions | 50 (82%) |
| 60 Gy in 15 fractions | 2 (3.3%) |
| Baseline neutrophils (×10⁹/L) | |
| Mean (SD) | 5.75 (2.06) |
| Median (Q1, Q3) | 5.40 (4.17, 7.05) |
| Range | 2.07–10.89 |
| Baseline lymphocytes (×10⁹/L) | |
| Mean (SD) | 2.00 (2.46) |
| Median (Q1, Q3) | 1.63 (1.29, 2.10) |
| Range | 0.53–20.10 |
| Baseline platelet (×10⁹/L) | |
| Mean (SD) | 256.5 (85.9) |
| Median (Q1, Q3) | 260.0 (211.0, 302.0) |
| Range | 51.0–588.0 |
| Baseline monocytes (×10⁹/L) | |
| Mean (SD) | 0.67 (0.22) |
| Median (Q1, Q3) | 0.65 (0.54, 0.83) |
| Range | 0.08–1.19 |
| Neutrophil/lymphocytes ratio | |
| Mean (SD) | 3.91 (2.29) |
| Median (Q1, Q3) | 3.42 (2.38, 5.04) |
| Range | 0.27–13.69 |
| Platelet/lymphocyte ratio | |
| Mean (SD) | 169.9 (93.55) |
| Median (Q1, Q3) | 156.4 (117.2, 197.5) |
| Range | 146–534.6 |
| Monocytes/lymphocytes ratio | |
| Mean (SD) | 0.44 (0.22) |
| Median (Q1, Q3) | 0.39 (0.31, 0.53) |
| Range | 0.03–1 |
| Death [n (%)] | 29 (47.5%) |
| Recurrence [n (%)] | 30 (49.1%) |
| Follow-up (years) | |
| Mean (SD) | 2.28 |
| Median | 2.14 |
| Median OS (years) | 3.00 |
| Variables | Univariable | Multivariable | Multivariable + Neutrophil/ Lymphocyte Ratio | Multivariable + Monocyte/ Lymphocyte Ratio | Multivariable + Platelet/ Lymphocyte Ratio | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | ||
| Neutrophil/lymphocyte ratio | 1.27 | 1.06–1.53 | 0.009 | 1.26 | 1.04–1.53 | 0.017 | ||||||||||
| Monocyte/lymphocyte ratio | 2.92 | 0.62–13.78 | 0.176 | 2.8 | 0.53–14.86 | 0.227 | ||||||||||
| Platelet/lymphocyte ratio | /100 | 1.05 | 0.69–1.59 | 0.833 | 1.02 | 0.66–1.57 | 0.93 | |||||||||
| ECOG | Missing | 0.91 | 0.24–3.47 | 0.609 | 1.11 | 0.29–4.24 | 0.5049 | 1.29 | 0.32–5.13 | 0.3555 | 1.34 | 0.33–5.42 | 0.415 | 1.12 | 0.29–4.28 | 0.5031 |
| 1–2 | 1.42 | 0.48–4.16 | 1.69 | 0.57–5.02 | 2.04 | 0.67–6.25 | 1.98 | 0.64–6.20 | 1.7 | 0.57–5.08 | ||||||
| 0 | (ref) | (ref) | (ref) | (ref) | (ref) | |||||||||||
| ITV (cm) | logged | 1.44 | 0.99–2.10 | 0.06 | 1.47 | 1.01–2.15 | 0.045 | 1.38 | 0.93–2.05 | 0.114 | 1.44 | 0.98–2.13 | 0.064 | 1.47 | 1.01–2.15 | 0.046 |
| Age | /10 years | 1.13 | 0.64–2.01 | 0.664 | ||||||||||||
| Gender | Female | 0.94 | 0.43–2.03 | 0.873 | ||||||||||||
| Male | (ref) | |||||||||||||||
| PET SUV max | /10 | 1.29 | 0.76–2.20 | 0.346 | ||||||||||||
| AIC | 203.3964 | 199.9933 | 204.0053 | 205.38888 | ||||||||||||
| Delta AIC from multivariable | 3.4031 | −0.6089 | −1.99248 | |||||||||||||
| 1 minus index of adequacy | 0.52 | 0.22 | 0 | |||||||||||||
| Scaled Integrated Brier | 0.09 | 0.11 | 0.1 | 0.09 | ||||||||||||
| Scaled Brier change (%) | 17.4 | 1 | −2.5 | |||||||||||||
| Variables | Univariable | Multivariable | Multivariable + Neutrophil/Lymphocyte Ratio | Multivariable + Monocyte/ Lymphocyte Ratio | Multivariable + Platelet/ Lymphocyte Ratio | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | ||
| Neutrophil/lymphocyte ratio | ^1 | 0.55 | 0.28–1.09 | 0.0098 | 0.36 | 0.17–0.78 | 0.0009 | |||||||||
| ^2 | 1.08 | 1.01–1.17 | 1.16 | 1.06–1.26 | ||||||||||||
| Monocyte/lymphocyte ratio | 1.96 | 0.49–7.78 | 0.34 | 2.38 | 0.54–10.43 | 0.252 | ||||||||||
| Platelet/lymphocyte ratio | /100 | 1.13 | 0.80–1.60 | 0.494 | 1.28 | 0.85–1.92 | 0.241 | |||||||||
| ECOG | Missing | 1.35 | 0.38–4.81 | 0.1387 | 1.57 | 0.44–5.62 | 0.0738 | 4.13 | 0.93–18.28 | 0.0052 | 1.86 | 0.49–6.99 | 0.0553 | 1.83 | 0.48–6.95 | 0.05 |
| 1–2 | 2.45 | 0.86–7.02 | 2.97 | 1.02–8.58 | 9.24 | 2.25–37.90 | 3.4 | 1.13–10.28 | 3.6 | 1.14–11.42 | ||||||
| 0 | (ref) | (ref) | (ref) | (ref) | (ref) | |||||||||||
| ITV (cm) | logged | 1.33 | 0.95–1.88 | 0.098 | 1.43 | 1.03–2.00 | 0.035 | 1.38 | 0.95–2.01 | 0.089 | 1.42 | 1.01–2.00 | 0.044 | 1.42 | 1.02–1.98 | 0.039 |
| Age | /10 years | 1.03 | 0.62–1.71 | 0.906 | ||||||||||||
| Gender | Female | 1.07 | 0.53–2.13 | 0.853 | ||||||||||||
| Male | (ref) | |||||||||||||||
| PET SUV max | /10 | 1.21 | 0.75–1.95 | 0.443 | ||||||||||||
| AIC | 262.1701 | 245.9663 | 262.9462 | 262.8649 | ||||||||||||
| Delta AIC from multivariable | 16.2038 | −0.7761 | −0.6948 | |||||||||||||
| 1 minus index of adequacy | 0.7 | 0.12 | 0.13 | |||||||||||||
| Scaled integrated Brier | 0.14 | 0.19 | 0.13 | 0.12 | ||||||||||||
| Scaled Brier change (%) | 31.5 | −8.1 | −18.3 | |||||||||||||
| Variables | Univariable | Multivariable | Multivariable + Neutrophil/ Lymphocyte Ratio | Multivariable + Monocyte/ Lymphocyte Ratio | Multivariable + Platelet/ Lymphocyte Ratio | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | ||
| Neutrophil/lymphocyte ratio | ^1 | 0.73 | 0.44–1.21 | 0.001 | 0.74 | 0.44–1.23 | 0.021 | |||||||||
| ^2 | 1.05 | 1.00–1.10 | 1.05 | 1.00–1.10 | ||||||||||||
| Monocyte/lymphocyte ratio | 2.71 | 0.63–11.69 | 0.180 | 2.72 | 0.56–13.14 | 0.212 | ||||||||||
| Platelet/lymphocyte ratio | /100 | 1.01 | 0.68–1.50 | 0.958 | 0.98 | 0.66–1.47 | 0.935 | |||||||||
| ECOG | Missing | 0.90 | 0.24–3.40 | 0.407 | 1.06 | 0.28–4.03 | 0.311 | 1.27 | 0.33–4.95 | 0.239 | 1.27 | 0.32–5.11 | 0.256 | 1.05 | 0.28–4.03 | 0.314 |
| 1–2 | 1.59 | 0.55–4.62 | 1.89 | 0.64–5.57 | 2.22 | 0.74–6.66 | 2.20 | 0.71–6.78 | 1.88 | 0.64–5.57 | ||||||
| 0 | (ref) | (ref) | (ref) | (ref) | (ref) | |||||||||||
| ITV (cm) | logged | 1.37 | 0.93–2 | 0.110 | 1.42 | 0.97–2.09 | 0.074 | 1.30 | 0.86–1.97 | 0.217 | 1.39 | 0.93–2.07 | 0.105 | 1.43 | 0.97–2.10 | 0.074 |
| Age | /10 years | 1.22 | 0.71–2.11 | 0.477 | ||||||||||||
| Gender | Female | 1.10 | 0.52–2.32 | 0.813 | ||||||||||||
| Male | (ref) | |||||||||||||||
| PET SUV max | /10 | 1.40 | 0.82–2.38 | 0.215 | ||||||||||||
| AIC | 227.69 | 223.60 | 228.23 | 229.69 | ||||||||||||
| Delta AIC from multivariable | 4.09 | −0.54 | −2.00 | |||||||||||||
| 1 minus index of adequacy | 0.61 | 0.22 | 0.00 | |||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aduquaye, M.; Dube, S.; Bashir, B.; Chowdhury, A.; Ahmed, N.; Leylek, A.; Kim, J.; Lambert, P.; Bucher, O.; Hunter, W.; et al. Impact of Pre-Treatment NLR and Other Hematologic Biomarkers on the Outcomes of Early-Stage Non-Small-Cell Lung Cancer Treated with Stereotactic Body Radiation Therapy. Curr. Oncol. 2022, 29, 193-208. https://doi.org/10.3390/curroncol29010019
Aduquaye M, Dube S, Bashir B, Chowdhury A, Ahmed N, Leylek A, Kim J, Lambert P, Bucher O, Hunter W, et al. Impact of Pre-Treatment NLR and Other Hematologic Biomarkers on the Outcomes of Early-Stage Non-Small-Cell Lung Cancer Treated with Stereotactic Body Radiation Therapy. Current Oncology. 2022; 29(1):193-208. https://doi.org/10.3390/curroncol29010019
Chicago/Turabian StyleAduquaye, Marina, Sheen Dube, Bashir Bashir, Amitava Chowdhury, Naseer Ahmed, Ahmet Leylek, Julian Kim, Pascal Lambert, Oliver Bucher, William Hunter, and et al. 2022. "Impact of Pre-Treatment NLR and Other Hematologic Biomarkers on the Outcomes of Early-Stage Non-Small-Cell Lung Cancer Treated with Stereotactic Body Radiation Therapy" Current Oncology 29, no. 1: 193-208. https://doi.org/10.3390/curroncol29010019
APA StyleAduquaye, M., Dube, S., Bashir, B., Chowdhury, A., Ahmed, N., Leylek, A., Kim, J., Lambert, P., Bucher, O., Hunter, W., Sivananthan, G., Koul, R., & Rathod, S. (2022). Impact of Pre-Treatment NLR and Other Hematologic Biomarkers on the Outcomes of Early-Stage Non-Small-Cell Lung Cancer Treated with Stereotactic Body Radiation Therapy. Current Oncology, 29(1), 193-208. https://doi.org/10.3390/curroncol29010019