Métis Peoples and Cancer: A Scoping Review of Literature, Programs, Policies and Educational Material in Canada

 , , ,
, , ,
Abstract
1. Introduction
The Métis Nation
2. Methods
2.1. Sources
2.2. Search Strategy
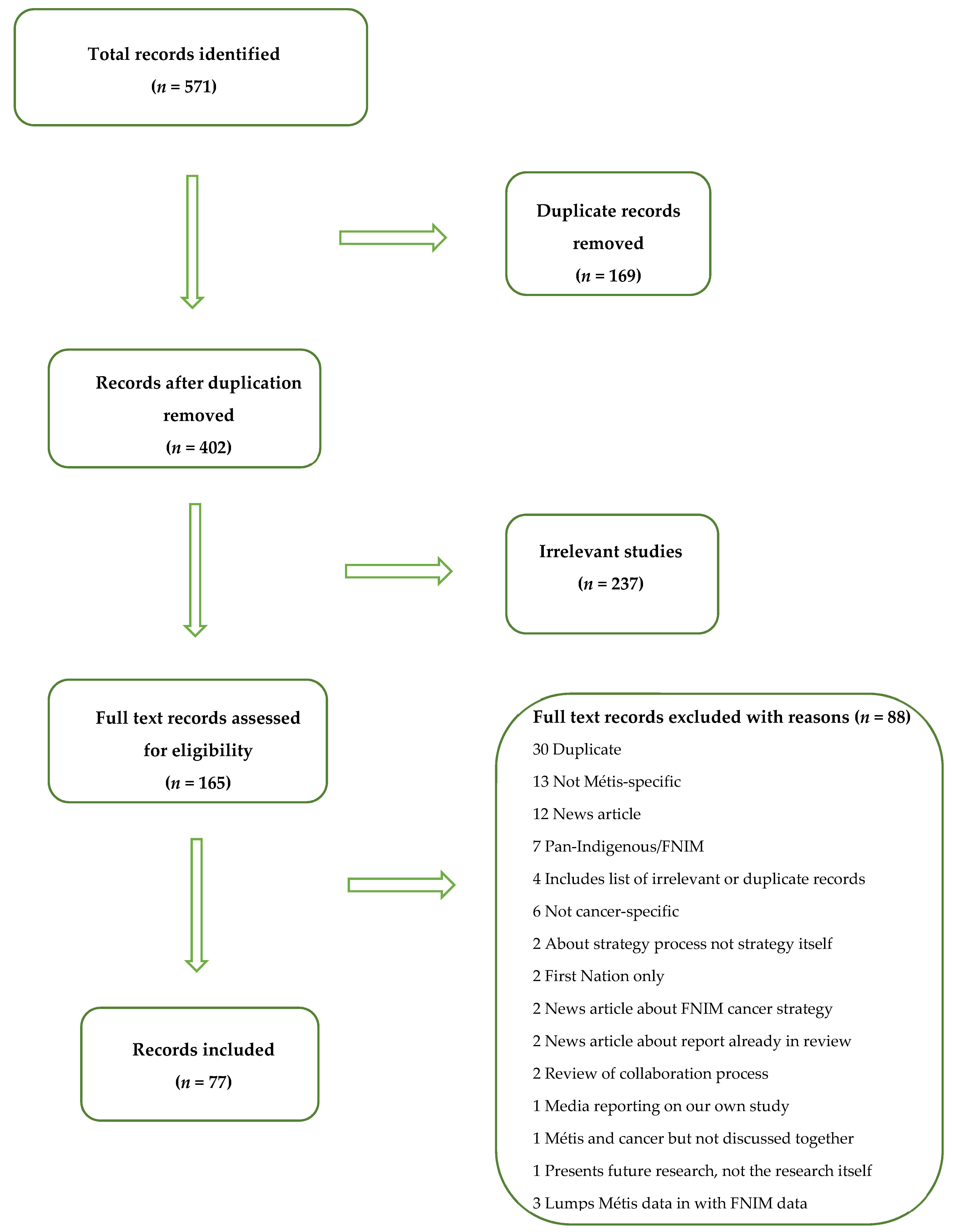
2.3. Record Selection Process
2.4. Data Extraction
2.5. Data Charting
3. Summary of Evidence
3.1. Academic Literature
3.2. Grey Literature
3.3. Material Records
3.4. Programs and Service Records
3.5. Plans and Strategies
- Build productive relationship-building through partnerships and collaboration (Indigenous and non-Indigenous)
- Increase screening participation rates among Indigenous populations
- Increase Indigenous cancer research and surveillance
- Prevention (including the use of culturally appropriate educational materials/outreach)
- Education (for Indigenous peoples as well as health care professionals)
- Health promotion (that is culturally relevant)
- Culturally safe and culturally appropriate cancer-related care (including programs and services)
- Palliative care (also culturally relevant)
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
References
- Reading, C.; Wien, F. Health Inequalities and Social Determinants of Aboriginal Peoples’ Health. National Collaborating Centre for Aboriginal Health, 2009. Available online: https://www.ccnsa-nccah.ca/docs/determinants/RPT-HealthInequalities-Reading-Wien-EN.pdf (accessed on 4 August 2021).
- Smylie, J. Achieving Strength through Numbers: First Nations, Inuit and Métis Health Information. National Collaborating Centre for Aboriginal Health. Available online: https://www.nccih.ca/docs/context/FS-AchievingStrengthNumbers-Smylie-EN.pdf (accessed on 4 August 2021).
- An Overview of Aboriginal Health in Canada. Available online: https://www.ccnsa-nccah.ca/docs/context/FS-OverviewAbororiginalHealth-EN.pdf (accessed on 4 August 2021).
- Hutchinson, P.; Tobin, P.; Muirhead, A.; Robinson, N. Closing the gaps in cancer screening with First Nations, Inuit and Métis populations: A narrative literature review. Indig. Wellbeing Mauri-Pimatisiwin 2018, 3, 3–17. [Google Scholar]
- About the Métis Nation. Métis National Council, 2021. Available online: https://archive.is/2l5jk (accessed on 8 September 2021).
- Isaac, T. A Matter of National and Constitutional Import: Report to the Minister’s Special Representative on Reconciliation with Métis: Section 35 Métis Rights and the Manitoba Métis Federation Decision. 2016. Available online: http://www.dgwlaw.ca/wp-content/uploads/2016/08/Thomas-Isaac-Reconciliation-Metis-Report.pdf (accessed on 4 August 2021).
- Gracey, M.; King, M. Indigenous health part 1: Determinants and disease patterns. Lancet 2009, 374, 65–75. [Google Scholar] [CrossRef]
- Martens, P.; Barlett, J.; Burland, E.; Priori, H.; Bruchill, C.; Huq, S.; Romphf, L.; Sanguins, J.; Carter, S.; Bailey, A. Profile of Metis Health Status and Healthcare Utilization in Manitoba: A Population-Based Study. 2010. Available online: http://mchp-appserv.cpe.umanitoba.ca/deliverablesList.html (accessed on 4 August 2021).
- Bruce, S.G.; Riediger, N.D.; Lix, L.M. Chronic disease and chronic disease risk factors among First Nations, Inuit and Métis populations of northern Canada. Chronic Dis. Inj. Can. 2014, 34, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Shahid, R.K.; Episkenew, J.A. Disparity in cancer prevention and screening in aboriginal populations: Recommendations for action. Curr. Oncol. 2015, 22, 417–426. [Google Scholar] [CrossRef][Green Version]
- McGahan, C.; Linn, K.; Guno, P.; Johnson, H.; Coldman, A.; Spinelli, J.; Caron, N. Cancer in First Nations people living in British Columbia, Canada: An analysis of incidence and survival from 1993 to 2010. Cancer Causes Control 2017, 28, 1105–1116. [Google Scholar] [CrossRef] [PubMed]
- Garvey, G. Indigenous population with lung cancer. Thoracic. Oncol. 2017, 12, S195–S196. [Google Scholar] [CrossRef][Green Version]
- Horrill, T.C.; Linton, J.; Lavoie, J.G.; Martin, D.; Wiens, A.; Schultz, A.S.H. Access to cancer care among Indigenous peoples in Canada: A scoping review. Soc. Sci. Med. 2019, 238, 112495. [Google Scholar] [CrossRef]
- Kumar, M.; Wesche, S.; McGuire, C. Trends in Métis-related health research (1980–2009): Identification of research gaps. Can. J. Public Health 2012, 103, 23–28. [Google Scholar] [CrossRef]
- Sarfati, D.; Garvey, G.; Robson, B.; Moore, S.; Cunningham, R.; Withrow, D.; Griffiths, K.; Caron, N.; Bray, F. Measuring cancer in Indigenous populations. Ann. Epidemiol. 2018, 28, 335–342. [Google Scholar] [CrossRef]
- Letendre, A.; Garvey, G.; King, A.; King, M.; Crowshow, R.; Bill, L.; Caron, N.R.; Elias, B. Creating a Canadian Indigenous research network against cancer to address Indigenous cancer disparities. JCO Glob. Oncol. 2020, 6, 92–98. [Google Scholar] [CrossRef]
- Friedman, D.; Hoffman-Goetz, L. Assessing cultural sensitivity of breast cancer information for older Aboriginal women. Cancer Educ. 2007, 22, 112–118. [Google Scholar] [CrossRef]
- Poudriere, J.; MacLean, R.T. ‘We’ve fallen into the cracks’: Aboriginal women’s experiences with breast cancer through photovoice. Nurs. Inq. 2009, 16, 306–317. [Google Scholar] [CrossRef]
- Demers, A.; Shearer, B.; Totten, S.; Fang, L.; Severini, A.; Kliewer, E.; Mao, Y.; Wong, T.; Jayaraman, G. P1-S2.69 Prevalence of HPV infections in Métis and First Nations living in Manitoba, Canada. Sex. Transm. Infect. 2011, 87, A152. [Google Scholar] [CrossRef]
- Shafer, L.A.; Jeffrey, I.; Elias, B.; Shearer, B.; Canfell, K.; Kliewer, E. Quantifying the impact of dissimilar HPV vaccination uptake among Manitoban school girls by ethnicity using a transmission dynamic model. Vaccine 2013, 31, 4848–4855. [Google Scholar] [CrossRef] [PubMed]
- Randall, J.R.; Harris, A.; Svenson, L.; Voaklander, D.; Parker, S.H. Health Status of Métis Population of Alberta. Métis Nation of Alberta Association and the University of Alberta, 2012. Available online: http://albertametis.com/wp-content/uploads/2014/02/Health-Status-of-the-M--tis-Population-of-Alberta-Report.pdf (accessed on 4 August 2021).
- Wilson, K.; Young, T.K. An overview of Aboriginal health research in the social sciences: Current trends and future directions. Int. J. Circumpolar Health 2008, 67, 179–189. [Google Scholar] [CrossRef]
- Métis Centre of the National Aboriginal Health Organization. Paucity of Métis-Specific Health and Well-Being Data and Information: Underlying Factors. 2011. Available online: https://www.nccahccnsa.ca/docs/fact%20sheets/setting%20the%20context/Paucity%20of%20Metis%20Health%20%28English%29.pdf (accessed on 4 August 2021).
- Young, T.K. Review of research on Aboriginal populations in Canada: Relevance to their health needs. Br. Med. J. 2003, 327, 419–422. [Google Scholar] [CrossRef]
- CPAC-Canadian Partnership Against Cancer. Métis Cancer Control in Canada Baseline Report. 2014. Available online: https://www.partnershipagainstcancer.ca/wp-content/uploads/2017/12/metis-cancer-control-baseline-report.pdf (accessed on 4 August 2021).
- Ahmed, S.; Vaska, M.; Turin, T.C. Conducting a literature review in health research: Basics of the approach, typology and methodology. J. Natl. Heart Found. Bangladesh 2016, 5, 44–51. [Google Scholar]
- Canada-Métis Nation Accord. 2017. Available online: https://pm.gc.ca/en/canada-metis-nation-accord (accessed on 12 November 2021).
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.; Lillie, E.; Zarin, W.; O’Brian, K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.; Horsely, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–486. [Google Scholar] [CrossRef] [PubMed]
- Groot, G. Sakipakawin: Environmental Scan of Provincial Cancer Supports for Indigenous Patients and their Families in Saskatchewan. University of Saskatchewan, 2020. Available online: https://static1.squarespace.com/static/5b22e5239d5abb6a167c048c/t/5f74b62e73f24438327996eb/1601484342696/S%C3%A2kipak%C3%A2win+An+Environmental+Scan+of+Provincial+Cancer+Supports.pdf (accessed on 5 August 2021).
- Covidence Systematic Review Software, Veritas Health Innovation, Melbourne, Australia. Available online: www.covidence.org (accessed on 20 August 2021).
- Sanchez-Ramirez, D.; Colquhoun, A.; Parker, S.H.; Randall, J.; Svenson, L.; Voaklander, D. Cancer incidence and mortality among the Métis population of Alberta. Intl. J. Circumpolar Health 2016, 75, 30059. [Google Scholar] [CrossRef][Green Version]
- Crouse, A.; Hossein Sadrzadeh, S.M.; de Koning, L.; Naugler, C. Sociodemographic correlates of fecal immunotesting for colorectal cancer screening. Clin. Biochem. 2014, 48, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Fatah, T. Providing a Culturally Sensitive Approach to Support Indigenous Cancer Patients and Their Families: A Nurse Navigator’s Experience. Master’s Thesis, University of Ottawa, Ottawa, ON, Canada, 2019. [Google Scholar]
- Sheppard, A.; Antone, C.; Logan, A.; Kewayosh, A. “In a good way”: Going beyond patient navigation to ensure culturally relevant care in the cancer system for First Nations, Inuit, and Métis patients in Ontario. Int. J. Indigenous Health 2019, 14, 293–306. [Google Scholar] [CrossRef]
- Beben, N.; Muirhead, A. Improving cancer control in First Nations, Inuit and Métis communities in Canada. Eur. J. Cancer Care 2016, 25, 219–221. [Google Scholar] [CrossRef][Green Version]
- Cawley, C.; Mazereeuw, M.; Jamal, S.; Sheppard, A.; Marrett, L. Commercial tobacco exposure in First Nations, Inuit and Métis in Ontario: Results from population-based health surveys and implications for cancer control. Cancer Health Disparities 2018, 2, E1–E12. [Google Scholar]
- Kumar, M.B.; Janz, T. Aboriginal People’s Survey, 2006: Screening for Chronic Diseases among Metis. Ottawa, Canada: Statistics Canada. 2013. Available online: https://www150.statcan.gc.ca/n1/en/pub/89-637-x/89-637-x2013001-eng.pdf?st=GqMBuc13 (accessed on 13 August 2021).
- Mazereeuw, M.; Withrow, D.; Nishri, E.D.; Tjepkema, M.; Vides, E.; Marrett, L. Cancer incidence and survival among Métis adults in Canada: Results from the Canadian census follow-up cohort (1992–2009). CMAJ 2018, 190, E320–E326. [Google Scholar] [CrossRef]
- McDonald, J.T.; Trenholm, R. Cancer-related health behaviours and health service use among Inuit and other residents of Canada’s north. Soc. Sci. Med. 2010, 70, 1396–1403. [Google Scholar] [CrossRef]
- Tjepkema, M.; Wilkins, R.; Pennock, J.; Goedhuis, N. Potential years of life lost at ages 25 to 74 among Métis and non-Status Indians, 1991 to 2001. Stat. Can. Health Rep. 2011, 22, 37–46. [Google Scholar]
- Withrow, D.R.; Amarty, A.; Marrett, L.D. Cancer risk factors and screening in the off-reserve First Nations, Métis and non-Aboriginal populations of Ontario. Chronic Dis. Inj. Can. 2014, 34, 103–112. [Google Scholar] [CrossRef]
- Withrow, D. Cancer Survival in First Nation and Métis Adults in Canada: Follow-Up of the 1991 Census Mortality Cohort. Ph.D. Thesis, University of Toronto, Toronto, ON, Canada, 2016. [Google Scholar]
- Baidoobonso, S. Understanding and Addressing the Cancer Screening Participation Gap in Ontario: A Summary of Cancer Care Ontario’s Initiatives; Prevention and Cancer Control, Cancer Care Ontario: Toronto, ON, Canada, 2017. [Google Scholar]
- Bartlett, J.G.; Sanguins, J.; Carter, S.; Turner, D.; Demers, A.; Kliewer, E.; Mehta, P.; Hoeppner, N.; Musto, G.; Morgan, B. Cancer and Related Health Care Utilization in the Manitoba Metis Population; Manitoba Metis Federation: Winnipeg, MB, Canada, 2011.
- Canadian Partnership Against Cancer. Report on National Forum of First Nations, Inuit and Métis Cancer Control. 2009. Available online: https://s22457.pcdn.co/wp-content/uploads/2018/12/fnim_national_forum_2009_EN.pdf (accessed on 13 August 2021).
- Cancer Care Ontario. Path to Prevention—Recommendations for Reducing Chronic Disease in First Nations, Inuit and Métis. Toronto: Queen’s Printer for Ontario. 2016. Available online: https://www.ccohealth.ca/sites/CCOHealth/files/assets/FNIMPathtoPrevention_0.pdf (accessed on 13 August 2021).
- O’Connor, K. First Nations, Inuit and Metis Cancer Care Priorities: A document Review of First Nations, Inuit and Métis Cancer Care Engagement (2011–2018) to Inform the Refresh of the Canadian Strategy for Cancer Control. Canadian Partnership Against Cancer. 2019. Available online: https://s22457.pcdn.co/wp-content/uploads/2019/05/FNIM-Document-Review-of-Cancer-Control.pdf (accessed on 13 August 2021).
- Métis Nation of Ontario and Cancer Care Ontario. Cancer in the Métis People of Ontario: Risk Factors and Screening Behaviours. Ottawa, ON, Canada, 2015. Available online: https://www.metisnation.org/wp-content/uploads/2015/07/mno-cco-report-screen.pdf (accessed on 13 August 2021).
- Carter, S.; Kosowan, L.; Garner, B.; Sanguins, J. Métis Experience with Chronic Disease in Manitoba: A Discussion Paper. Manitoba Métis Federation & Health and Wellness Department, 2013. Available online: http://www.mmf.mb.ca/docs/Factors%20Influencing%20CDs%20in%20Metis%20Population%20in%20Manitoba%20Canada%20May%202013%20Final.pdf (accessed on 16 August 2021).
- Haver, C. First Nations and Metis Health Service: Navigation Services Literature Review. 2014. Available online: https://www.saskatoonhealthregion.ca/locations_services/Services/fnmh/service/Documents/About-Us%20FNMHS/FNMH_FINAL_Navigation_Services_Literature_Review_Oct_21_2014.pdf (accessed on 16 August 2021).
- Cats, H.C.; Withrow, D.R.; Marrett, L.D. Where There’s a Will, There’s a Way: Environmental Scan and Analysis of Existing Patient Identification Systems for First Nations, Inuit and Métis Peoples—Final Report. Canadian Partnership Against Cancer: Toronto, ON, Canada, 2012. Available online: https://s22457.pcdn.co/wp-content/uploads/2018/12/patient-identification-FNIM-2012-EN.pdf (accessed on 13 August 2021).
- Snelling, S. Working Together: Lessons Learned from the Coalitions Linking Action and Science for Prevention (CLASP) Initiative in Supporting Indigenous Health and Wellness. Canadian Partnership Against Cancer, 2017. Available online: https://s22457.pcdn.co/wp-content/uploads/2018/12/indigenous-lessons-learned-CLASP-EN.pdf (accessed on 13 August 2021).
- Kliewer, E.; Mayer, T.; Wajda, A. The Health of Manitoba’s Metis Population and Their Utilization of Medical Services: A Pilot Study. Canadian Women’s Health Network, 2002. Available online: http://www.mmf.mb.ca/departments_portfolios_and_affiliates_details.php?id=11&type=publications (accessed on 13 August 2021).
- Institute for Clinical Evaluative Sciences and Métis Nation Ontario. Respiratory Disease in the Métis Nation of Ontario: Lay report. 2012. Available online: https://www.metisnation.org/wp-content/uploads/2020/04/respiratory_lay_report16-mar-2012.pdf (accessed on 13 August 2021).
- Klein-Geltink, J.; Saskin, R.; Manno, M.; Urbach, D.; Henry, D. Cancer in the Métis Nation of Ontario: Lay Report. Métis Nation of Ontario and Institute for Clinical Evaluative Sciences, 2012. Available online: https://www.metisnation.org/wp-content/uploads/2020/04/cancer_lay_report_en2019-mar-2012.pdf (accessed on 13 August 2021).
- Métis Centre of the National Aboriginal Health Organization. Métis Women and Disease: A Preliminary Examination. 2012. Available online: https://www.nccih.ca/495/M%C3%A9tis_women_and_disease__A_preliminary_examination.nccih?id=25 (accessed on 13 August 2021).
- Cancer Control Alberta. Supportive Care Framework Report. 2016. Available online: https://albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-supportive-care-framework-report.pdf (accessed on 16 August 2021).
- Cancer Care Ontario. Aboriginal Cancer Strategy II. 2011. Available online: https://www.cancercareontario.ca/sites/ccocancercare/files/assets/CCOACS2.pdf (accessed on 20 August 2021).
- Cancer Care Ontario. First Nations, Inuit, Metis and Urban Indigenous Cancer Strategy 2019–2023. 2019. Available online: https://www.cancercareontario.ca/en/cancer-care-ontario/programs/aboriginal-programs/indigenous-cancer-strategy (accessed on 20 August 2021).
- Cancer Care Ontario. 2015–2019 Southeast Aboriginal Cancer Strategy. 2015. Available online: http://cancercaresoutheast.ca/south-east-aboriginal-cancer-strategy-2015-19-0 (accessed on 20 August 2021).
- Cancer Care Ontario. 2015–2019 Northeast Aboriginal Cancer Plan. 2015. Available online: https://www.hsnsudbury.ca/portalen/Portals/3/NE%20Aboriginal%20Cancer%20Plan%202015-19%20Sept_2016%20v5.pdf?ver=2017-01-27-135448-827 (accessed on 20 August 2021).
- Canadian Partnership against Cancer. First Nations, Inuit and Metis Action Plan on Cancer Control. 2011. Available online: https://www.partnershipagainstcancer.ca/wp-content/uploads/2017/12/fnim-action-plan-cancer-control.pdf (accessed on 20 August 2021).
- Canadian Partnership against Cancer. 2019–2029 Canadian Strategy for Cancer Control: Doing Together What Cannot Be Done Alone. 2019. Available online: https://www.partnershipagainstcancer.ca/wp-content/uploads/2019/06/Canadian-Strategy-Cancer-Control-2019-2029-EN.pdf (accessed on 19 August 2021).
- First Nations Health Authority; Métis Nation BC; BC Association of Aboriginal Friendship Centres; BC Cancer. Improving Indigenous Cancer Journeys in BC: A Road Map. 2017. Available online: https://www.fnha.ca/WellnessSite/WellnessDocuments/improving-indigenous-cancer-journeys-in-bc.pdf (accessed on 20 August 2021).
- Government of Alberta. Changing Our Future: Alberta’s Cancer Plan to 2030. 2013. Available online: https://open.alberta.ca/dataset/09e65e85-2796-456e-ac52-353b533450fd/resource/0c184a3f-e897-4794-a40a-a71b86ff91a5/download/6153402-2013-Changing-Our-Future-Albertas-Cancer-Plan-2030.pdf (accessed on 20 August 2021).
- Jones, J.; Cunsolo, A.; Harper, S.L. Who is research serving? A systematic realist review of circumpolar environment-related Indigenous health literature. PLoS ONE 2018, 13, e0196090. [Google Scholar] [CrossRef]
- ICES. ICES and Métis Nation of Ontario Partner on New Agreement. 2016. Available online: https://www.ices.on.ca/Newsroom/Announcements-and-Events/2016/ICES-and-Metis-Nation-of-Ontario-partner-on-new-agreement (accessed on 12 November 2021).
- Letendre, A. Aboriginal Female Sexual Health in a Context of Cervical Cancer and Cytology Screening with Reference to the Cree and Cree-Métis of Northern Alberta. Ph.D. Thesis, University of Alberta, Edmonton, AB, Canada, 2008. [Google Scholar]


{kind=link}
| Academic Search | Grey Search |
|---|---|
| MedLine Embase iPortal (University of Saskatchewan’ s Indigenous Studies Portal) Proquest Theses & Dissertations (first 30 results) Google Scholar (first 50 results) | Google (first 50 results) Canadian Partnership Against Cancer website National Collaborating Centre for Aboriginal Health website Cancer Care Ontario website Cancer Care Alberta website Cancer Care Manitoba website BC Cancer website Métis Nation of Alberta website Métis Nation of Ontario website Manitoba Métis Federation website Métis Nation of British Colombia website |
| Academic Searches | Grey Searches |
|---|---|
| (Cancer OR breast cancer OR colon cancer OR cervical cancer OR lung cancer) AND (Métis OR Michif) AND (care OR experience OR support) AND Canada | We used website search functions to search for ‘Métis/Aboriginal/Indigenous’ OR ‘cancer’ depending on the nature of the website. We explored Indigenous/Aboriginal/First Nations, Inuit, and Métis tabs when available on cancer agency websites. |
| (Cancer OR breast cancer OR colon cancer OR cervical cancer OR lung cancer) AND (Métis OR Michif) AND (policy OR strategy) AND Canada | |
| (Cancer OR breast cancer OR colon cancer OR cervical cancer OR lung cancer) AND (Métis OR Michif) AND community support AND patients AND Canada |
| Academic Records | Grey Records | ||
|---|---|---|---|
| Inclusion Criteria | Exclusion Criteria | Inclusion Criteria | Exclusion Criteria |
| Discuss Métis and cancer together | Pan-Indigenous/FNIM approach to data and analysis (i.e., cite Indigenous when data is from First Nation studies, or lumping First Nation, Inuit or Métis data together) | Target Métis cancer patients, survivors or caregivers/family | Addresses cancer in the general public |
| Target First Nation, Inuit and Métis people experiencing cancer | |||
| English or French language | Other | English language | Other |
| Canada | Other | Canada | Other |
| Authors | Jurisdiction | Datasets | Qual | Quant | Focus Area | Key Findings |
|---|---|---|---|---|---|---|
| Abdul-Fatah, 2019 [34] | Ottawa, Ontario | NA | X | Patient navigation | Nurse Navigators in Ottawa use a patient-centered, land-based, culturally appropriate approach to provide culturally safe health care to Indigenous cancer patients. Indigenous-specific cancer care services are an effective method to reduce care inequities. | |
| Beben & Muirhead, 2016 [36] | Canada | NA | X | Cancer control | Cancer care needs to address distinct needs of FNIM as separate groups of Indigenous peoples, rather than a pan-Indigenous approach. There needs to be more data collected that is specific to each group (FNIM) and urban/rural communities. | |
| Cawley et al., 2018 [37] | Ontario | Canadian Community Health Survey 2007–2014 | X | Behavioral risk factors | Prevalence of smoking is higher in Métis adults and adolescents than non-Indigenous adults and adolescents. Métis adolescents are more likely to be exposed to second-hand smoke than their non-Indigenous peers. | |
| Crouse et al., 2014 [33] | Calgary, Alberta | Alberta Cancer Registry Alberta Laboratory Information System Canadian Census (1991–2011) Mortality Cohort | X | Screening rates & sociodemographic variables | Métis population in Calgary, Alberta is less likely to be screened for colorectal cancer than other ethnic groups. Having a family doctor led to higher screening participation. Sociodemographic variables seem to play a role in screening participation. | |
| Hutchinson et al., 2018 [6] | Canada | NA | X | Screening barriers & facilitators | Screening facilitators include using culturally relevant educational materials, integrating screening opportunities with other FNIM health services, positive relationships with care providers, access to female health providers and communicating in plain language. | |
| Kumar & Janz, 2013 [38] | Canada | Aboriginal Peoples Survey 2006 | X | Screening rates & sociodemographic variable | Having a family doctor led to higher screening participation. | |
| Mazereeuw et al., 2018 [39] | Canada | Canadian Census (1991–2011) Health and Environment Cohort; Canadian Mortality Database; Canadian Cancer Registry | X | Cancer incidence & survival | Cancer incidence among Métis populations and non-Indigenous adults is similar for many cancers. Higher incidence rates among Métis adults for female breast, liver, lung, gallbladder and cervical cancers compared to non-Indigenous adults. | |
| McDonald & Trenholm, 2010 [40] | Northern Canada | Aboriginal Peoples Survey 2001 & 2006 Canadian Community Health Survey 2000–2002 & 2004–2005 | X | Behavioral risk factors & sociodemographic variables | Prevalence of smoking is higher in Métis adults and adolescents than non-Indigenous adults and adolescents. Métis people in northern regions are twice as likely to be obese than non-Indigenous people. Métis are not significantly more likely to have binged on alcohol than non-Indigenous people. Sociodemographic variables impact behavioural risk factors and the likelihood of visiting a physician. | |
| Sanchez-Ramirez, et al., 2016 [32] | Alberta | Métis Nation Alberta Information Registry | X | Cancer incidence & mortality | Cancer incidence among Métis populations and non-Indigenous adults is similar for many cancers. Incidence of bronchus/lung cancer was higher among Métis men than non-Métis men. No differences in cancer mortality between Métis and non-Métis people. | |
| Sheppard et al., 2019 [35] | Ontario | NA | X | Patient navigation | Ontario Indigenous Navigator role includes symptom assessment and management, facilitating traditional healing, providing health literacy, alleviating anxiety, ensuring access to supports at the right time, and engaging with other relevant programs. | |
| Tjepkema et al., 2011 [41] | Canada | Canadian Census (1991–2011); Canadian Mortality Database | X | Cancer mortality & sociodemographic variables | Potential years of life lost among Métis were twice those of non-Indigenous people. Cancer was a significant contributor to potential years of life lost for Métis. Sociodemographic factors are an important contributor to premature mortality rates of Métis. | |
| Withrow et al., 2014 [42] | Ontario | Canadian Community Health Survey 2007–2011 | X | Behavioral risk factors, screening rates & sociodemographic variables | Métis women are 2.5 times more likely to smoke than non-Indigenous women. Prevalence of smoking is higher in Métis adults and adolescents than non-Indigenous adults and adolescents. Métis people are twice as likely to be obese than non-Indigenous people. No significant differences in screening rates between Métis and non-Métis in Canada. (Screening rates among women are below national goals, regardless of ethnic identity (Withrow et al., 2014), so similar screening rates between Métis and non-Métis women does not necessarily indicate high or effective screening participation [42].) Ethnicity is a determinant of health-related lifestyle factors for Métis peoples. | |
| Withrow, 2016 [43] | Canada | 1991 Canadian Census Mortality Study; Canadian Cancer Registry | X | Cancer survival & sociodemographic variables | Métis have poorer survival rates for almost all of the most common cancers compared to the non-Indigenous population. Disparity remains when income and rurality are considered. |
| Author(s) | Record Type | Jurisdiction | Qualitative | Quantitative | Focus Area |
|---|---|---|---|---|---|
| Baidoobonso, 2017 [44] | Report to inform strategy/policy | Ontario | X | Screening for FNIM in Ontario | |
| Bartlett et al., 2011 [45] | Report | Manitoba | X | Cancer incidence among Métis | |
| Canadian Partnership Against Cancer, 2009 [46] | Report | Canada | X | FNIM cancer control | |
| Canadian Partnership Against Cancer, 2014 [25] | Report/Document review | Canada | X | Cancer control for Métis, including behavioural risk factors and mortality | |
| Cancer Care Ontario, 2016 [47] | Report to inform policy/strategy | Ontario | X | FNIM cancer control | |
| Cancer Control Alberta, 2016 [58] | Report | Alberta | X | FNIM cancer care | |
| Carter et al., 2013 [50] | Discussion paper | Manitoba | X | Métis cancer experience | |
| Cats et al., 2012 [52] | Environmental scan | Canada | X | FNIM patient identification for cancer control; data gaps | |
| Haver, 2014 [51] | Literature review | North America | X | FNIM patient navigator | |
| Institute for Clinical Evaluative Sciences and Métis Nation Ontario, 2012 [55] | Lay report | Ontario | X | Lung cancer rates for Métis | |
| Klein-Geltink et al., 2012 [56] | Lay Report | Ontario | X | Cancer incidence among Métis | |
| Kliewer, Mayer & Wajda, 2002 [54] | Report | Manitoba | X | Cancer incidence among Métis | |
| Martens et al., 2010 [8] | Report | Manitoba | X | Cancer incidence, screening rates and mortality among Métis | |
| Métis Centre of the National Aboriginal Health Organization, 2012 [57] | Report | Canada | X | Cancer incidence & mortality among Métis women | |
| Métis Centre of the National Aboriginal Health Organization, 2011 [23] | Report | Canada | X | Métis cancer data/governance | |
| Métis Nation of Ontario and Cancer Care Ontario, 2015 [49] | Report | Ontario | X | Behavioural risk factors & screening behaviour among Métis | |
| O’Connor, 2019 [48] | Document review | Canada | X | Cancer control for FNIM | |
| Randall et al., 2012 [21] | Report | Alberta | X | Cancer mortality among Métis | |
| Sanchez-Ramirez et al., 2016 [32] | Report | Alberta | X | Cancer incidence among Métis | |
| Snelling, 2017 [53] | Report | Canada | X | FNIM cancer prevention initiatives | |
| Groot, 2020 [30] | Environmental scan | Canada | X | FNIM cancer supports |
| Jurisdiction | Title | Resource Type | Creator(s) | Subject |
|---|---|---|---|---|
| Alberta | Guide to Cancer Care in Alberta for Newly Diagnosed Indigenous People | Patient information guide | Alberta Health Services Cancer Control Alberta | Cancer journey/experience |
| Alberta | Indigenous Cancer Care Experiences: Video Series | Video series | Cancer Control Alberta Alberta Health Services Saint Elizabeth Research Centre | Survivor story Grief Traditional healing Ceremony |
| British Colombia | Living with Cancer—everyone deserves support (Metis version) | Patient information guide | Metis Nation BC First Nation Health Authority BC Cancer Agency BC Association of Friendship Centres | Cancer journey/experience |
| Ontario & British Colombia | Silent Enemy | Comic book | Cancer Care Ontario First Nations Health Authority | Story: Indigenous family dealing with cancer |
| National | LivingMyCulture.ca | Video series | Canadian Partnership Against Cancer Virtual Hospice | Cancer journey/experience |
| Ontario | Be Tobacco-Wise—Métis | Brochure | Cancer Care Ontario | Prevention Tobacco cessation |
| Ontario | Environment, Heredity and Cancer | Factsheet | Cancer Care Ontario | Cancer risk factors |
| Ontario | Honouring the Métis path of well-being—breast screening | Factsheet | Cancer Care Ontario | Screening for breast cancer |
| Ontario | Honouring the Métis path of well-being—colorectal screening | Factsheet | Cancer Care Ontario | Screening for colorectal cancer |
| Ontario | Honouring the Métis path of well-being—cervical screening | Factsheet | Cancer Care Ontario | Screening for cervical cancer |
| Ontario | ON Cancer Treatment—Feel Good, Quit Smoking | Factsheet | Cancer Care Ontario | Quitting smoking during cancer treatment |
| Ontario | ON Métis Reduce Your Cancer Risks | Factsheet | Cancer Care Ontario | Prevention Behaviour risk factors |
| Ontario | Quit Smoking | Factsheet | Cancer Care Ontario | |
| Ontario | What is Cancer? | Factsheet | Cancer Care Ontario | General cancer information Behavioural risk factors |
| Ontario | Check-up for Prevention | Flashcard | Cancer Care Ontario | Prevention General cancer information |
| Ontario | Healthy Weight—Eat Right | Flashcard | Cancer Care Ontario | Prevention |
| Ontario | Stages of Cancer | Flashcard | Cancer Care Ontario | General cancer information |
| Ontario | Screening Q&A | Flashcard | Cancer Care Ontario | Screening general information |
| Ontario | Activity and Exercise | Flashcard | Cancer Care Ontario | Prevention |
| Ontario | Drinking Alcohol | Flashcard | Cancer Care Ontario | Prevention |
| Ontario | Cancer 101 Toolkit for FNIM People | Toolkit | Cancer Care Ontario | General cancer information Prevention screening |
| Ontario | Tools for the Journey: Palliative Care in First Nations, Inuit and Métis Communities | Toolkit | Cancer Care Ontario | Palliative care Grief |
| Ontario | Let’s take a stand against colorectal cancer!: Community Learning Series Reference Manual | Reference manual | Cancer Care Ontario | General cancer information Colorectal cancer Prevention screening |
| Ontario | Métis Cancer Survivor Story | Video | Cancer Care Ontario & Métis Nation Ontario | Métis survivor story |
| Ontario | Healing and Wellness—Cancer Care | Website | Métis Nation Ontario | General cancer information Breast screening Cervical screening |
| Organization | Title | Service Purpose | Services Available |
|---|---|---|---|
| Alberta | |||
| Alberta Health Services | Alberta Health Indigenous Wellness Core | Provide culturally appropriate cancer care to Indigenous cancer patients and families. | Nurse navigators, Indigenous-specific cancer resources, traditional wellness and cultural support. |
| British Colombia | |||
| BC Cancer | Indigenous Cancer Control | Supporting Indigenous cancer patients, survivors and their families. | Liaison positions at BC cancer centers to navigate Indigenous patients and families; culturally appropriate screening information campaign. |
| Manitoba | |||
| Cancer Care Manitoba | Manitoba Underserved Populations Program (part of the Community Oncology Program) | Help people who, due to geography, language, culture, or other barriers, may have trouble getting screened for cancer or receiving cancer treatment and support | Education and Liaison Nurse works with FNIM patients and families |
| Ontario | |||
| Kingston Health Sciences Centre | Aboriginal Peoples with Cancer | Support Aboriginal people with cancer by someone of Indigenous ancestry | Patient navigator; All Nations Healing room. |
| Cancer Care Ontario, Southeast Regional Cancer Program | Aboriginal Navigator | Provide services to FNIM patients and family throughout the cancer journey from diagnosis, treatment, recovery to palliative in Southeast Ontario health region | Patient navigation during appointments, for healing options including traditional healing. |
| Mount Sinai Hospital, Toronto | Coping with Cancer/Indigenous Patient Navigator | Support Indigenous cancer patients throughout their cancer journey | Assistance with travel to treatment, connect Indigenous patient with spiritual and community support, assist with financial support, connect with care providers. |
| Ottawa Hospital | Indigenous Cancer Program | Improve the performance of the cancer system with and for First Nations, Inuit and Métis peoples in Ontario; Ensure delivery of culturally sensitive and safe care | Patient navigation for continuity of care, language translation, clinic visits, spiritual support, culturally safe care; Windocage Community Room. |
| Cancer Care Ontario and Toronto Central Regional Cancer Program | Indigenous Patient Navigation Specialist—Toronto Central Regional Cancer Program | Provide support and advocacy for FNIM and urban Indigenous patients and families | Coordinate access to cancer services; address cultural and spiritual needs; network with partners to ensure a culturally safe experience. |
| Ontario Health, Cancer Care Ontario | Indigenous Tobacco Program | Education and support to reduce tobacco use | Distinctions-based approach to tobacco cessation through partnership with FNIM communities and organizations. Focus on prevention, education and cessation. |
| Cancer Care Ontario | Indigenous Navigators | Provide support and advocacy for FNIM and urban Indigenous patients and families. | Available in ten health regions; coordinate access to cancer services; address cultural and spiritual needs; network with partners to ensure a culturally safe experience. |
| Recommendations for Researchers, Research Institutions, Data Custodians and Clinicians |
|---|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brock, T.; Chowdhury, M.A.; Carr, T.; Panahi, A.; Friesen, M.; Groot, G. Métis Peoples and Cancer: A Scoping Review of Literature, Programs, Policies and Educational Material in Canada. Curr. Oncol. 2021, 28, 5101-5123. https://doi.org/10.3390/curroncol28060429
Brock T, Chowdhury MA, Carr T, Panahi A, Friesen M, Groot G. Métis Peoples and Cancer: A Scoping Review of Literature, Programs, Policies and Educational Material in Canada. Current Oncology. 2021; 28(6):5101-5123. https://doi.org/10.3390/curroncol28060429
Chicago/Turabian StyleBrock, Tegan, Maniza Abedin Chowdhury, Tracey Carr, Adel Panahi, Marg Friesen, and Gary Groot. 2021. "Métis Peoples and Cancer: A Scoping Review of Literature, Programs, Policies and Educational Material in Canada" Current Oncology 28, no. 6: 5101-5123. https://doi.org/10.3390/curroncol28060429
APA StyleBrock, T., Chowdhury, M. A., Carr, T., Panahi, A., Friesen, M., & Groot, G. (2021). Métis Peoples and Cancer: A Scoping Review of Literature, Programs, Policies and Educational Material in Canada. Current Oncology, 28(6), 5101-5123. https://doi.org/10.3390/curroncol28060429