A Randomized Trial Comparing 3- versus 4-Monthly Cardiac Monitoring in Patients Receiving Trastuzumab-Based Chemotherapy for Early Breast Cancer


 on behalf of the REaCT Investigators
on behalf of the REaCT Investigators
Abstract
:1. Introduction
2. Patients and Methods
2.1. Randomization
2.2. Procedures
2.3. Outcomes
2.4. Sample Size Calculation
2.5. Statistical Considerations
2.5.1. Per Protocol Analysis
2.5.2. Intention-to-Treat Analysis
2.5.3. General Statistical Considerations
2.5.4. Analysis of the Primary Outcome (LVEF)
2.5.5. Subgroup Analyses
3. Results
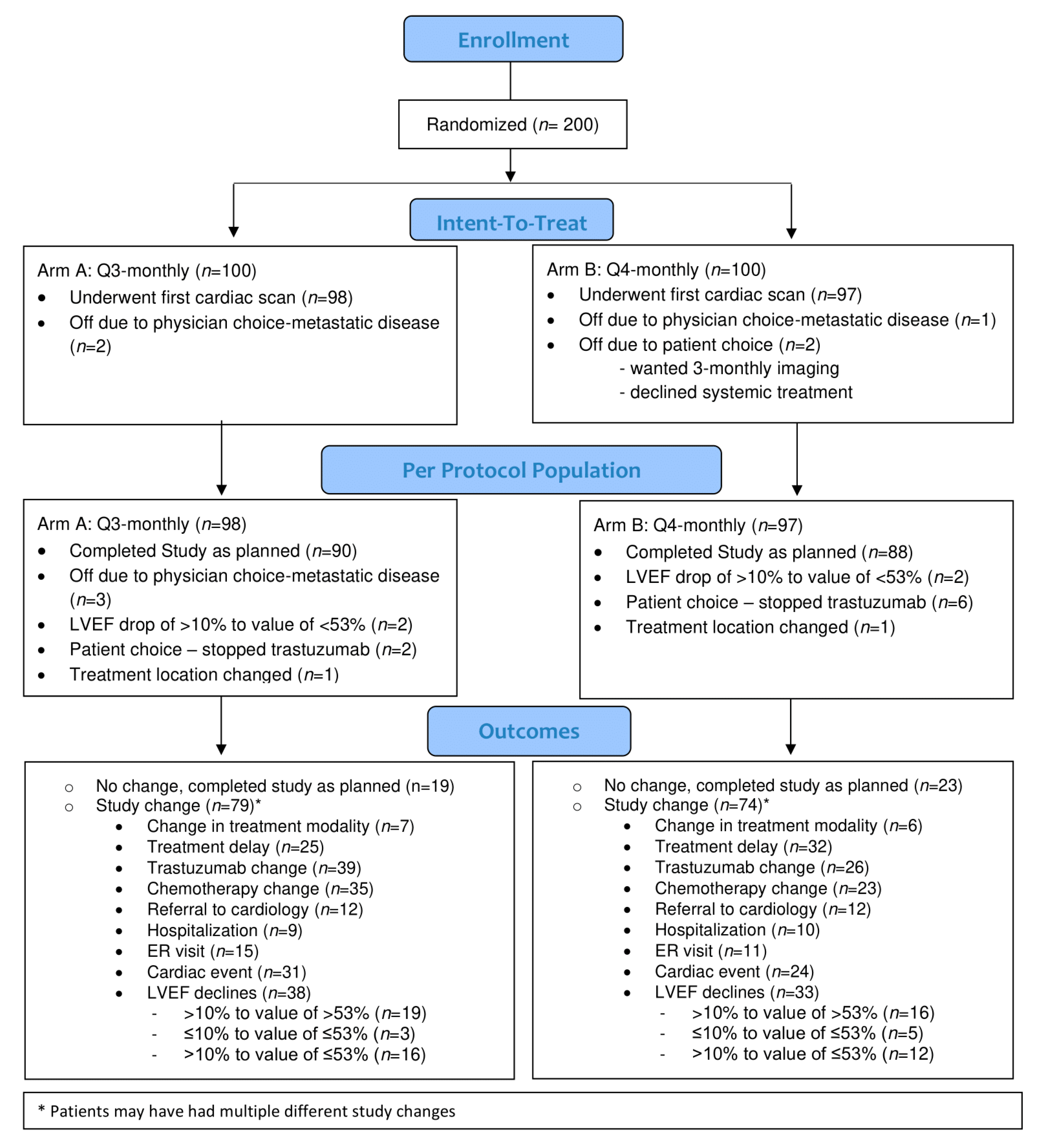
3.1. Patients
3.2. Primary Outcome
3.3. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dang, C.T.; Anthony, F.Y.; Jones, L.W.; Liu, J.; Steingart, R.M.; Argolo, D.F.; Norton, L.; Hudis, C.A. Cardiac surveillance guidelines for trastuzumab-containing therapy in early-stage breast cancer: Getting to the heart of the matter. J. Clin. Oncol. 2016, 34, 1030–1033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, A.; Yin, A.; Liu, J.; Steingart, R. Cost-effectiveness of cardiotoxicity monitoring. Am. Coll. Cardiol. Expert Anal. 2017, 19, 330. [Google Scholar]
- Mehta, L.S.; Watson, K.E.; Barac, A.; Beckie, T.M.; Bittner, V.; Cruz-Flores, S.; Dent, S.; Kondapalli, L.; Ky, B.; Okwuosa, T. Cardiovascular disease and breast cancer: Where these entities intersect: A scientific statement from the American Heart Association. Circulation 2018, 137, e30–e66. [Google Scholar] [CrossRef] [PubMed]
- Rushton, M.; Lima, I.; Tuna, M.; Johnson, C.; Ivars, J.; Pritchard, K.; Hawken, S.; Dent, S. Impact of Stopping Trastuzumab in Early Breast Cancer: A Population-Based Study in Ontario, Canada. J. Natl. Cancer Inst. 2020, 112, 1222–1230. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.A.; Dent, S.; Brezden-Masley, C.; Clarke, B.; Davis, M.K.; Jassal, D.S.; Johnson, C.; Lemieux, J.; Paterson, I.; Sebag, I.A. Canadian Cardiovascular Society guidelines for evaluation and management of cardiovascular complications of cancer therapy. Can. J. Cardiol. 2016, 32, 831–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curigliano, G.; Cardinale, D.; Suter, T.; Plataniotis, G.; De Azambuja, E.; Sandri, M.T.; Criscitiello, C.; Goldhirsch, A.; Cipolla, C.; Roila, F. Cardiovascular toxicity induced by chemotherapy, targeted agents and radiotherapy: ESMO Clinical Practice Guidelines. Ann. Oncol. 2012, 23, vii155–vii166. [Google Scholar] [CrossRef] [PubMed]
- Armenian, S.H.; Lacchetti, C.; Barac, A.; Carver, J.; Constine, L.S.; Denduluri, N.; Dent, S.; Douglas, P.S.; Durand, J.-B.; Ewer, M. Prevention and monitoring of cardiac dysfunction in survivors of adult cancers: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2017, 35, 893–911. [Google Scholar] [CrossRef]
- Jones, A.; Barlow, M.; Barrett-Lee, P.; Canney, P.A.; Gilmour, I.; Robb, S.; Plummer, C.; Wardley, A.M.; Verrill, M.W. Management of cardiac health in trastuzumab-treated patients with breast cancer: Updated United Kingdom National Cancer Research Institute recommendations for monitoring. Br. J. Cancer 2009, 100, 684–692. [Google Scholar] [CrossRef] [Green Version]
- Bouwer, N.I.; Jager, A.; Liesting, C.; Kofflard, M.J.; Brugts, J.J.; Kitzen, J.J.; Boersma, E.; Levin, M.-D. Cardiac monitoring in HER2-positive patients on trastuzumab treatment: A review and implications for clinical practice. Breast 2020, 52, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Surujballi, J.; Shah, H.; Hutton, B.; Alzahrani, M.; Beltran-Bless, A.-A.; Shorr, R.; Larocque, G.; McGee, S.; Cole, K.; Ibrahim, M.F.; et al. The COVID-19 pandemic: An opportunity to rethink and harmonise the frequency of follow-up visits for patients with early stage breast cancer. Cancer Treat. Rev. 2021, 97, 102188. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Miller, F.G. Informed consent for pragmatic trials--the integrated consent model. N. Engl. J. Med. 2014, 370, 769–772. [Google Scholar] [CrossRef]
- Plana, J.C.; Galderisi, M.; Barac, A.; Ewer, M.S.; Ky, B.; Scherrer-Crosbie, M.; Ganame, J.; Sebag, I.A.; Agler, D.A.; Badano, L.P. Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: A report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J.–Cardiovasc. Imaging 2014, 15, 1063–1093. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [PubMed]
- Van Reenen, M.; Janssen, B. EQ-5D-5L User Guide: Basic Information on How to Use the EQ-5D-5L Instrument; EuroQol Research Foundation: Rotterdam, The Netherlands, 2015. [Google Scholar]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®); Antiemesis, Version 2; National Comprehensive Cancer Network: Pennsylvania, PA, USA, 2016. [Google Scholar]
- Chavez-MacGregor, M.; Niu, J.; Zhang, N.; Elting, L.S.; Smith, B.D.; Banchs, J.; Hortobagyi, G.N.; Giordano, S.H. Cardiac monitoring during adjuvant trastuzumab-based chemotherapy among older patients with breast cancer. J. Clin. Oncol. 2015, 33, 2176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Florido, R.; Smith, K.L.; Cuomo, K.K.; Russell, S.D. Cardiotoxicity from Human Epidermal Growth Factor Receptor-2 (HER 2) Targeted Therapies. J. Am. Heart Assoc. 2017, 6, e006915. [Google Scholar] [CrossRef] [PubMed]
- Romond, E.H.; Jeong, J.-H.; Rastogi, P.; Swain, S.M.; Geyer, C.E., Jr.; Ewer, M.S.; Rathi, V.; Fehrenbacher, L.; Brufsky, A.; Azar, C.A. Seven-year follow-up assessment of cardiac function in NSABP B-31, a randomized trial comparing doxorubicin and cyclophosphamide followed by paclitaxel (ACP) with ACP plus trastuzumab as adjuvant therapy for patients with node-positive, human epidermal growth factor receptor 2–positive breast cancer. J. Clin. Oncol. 2012, 30, 3792–3799. [Google Scholar] [PubMed]
- Ezaz, G.; Long, J.B.; Gross, C.P.; Chen, J. Risk prediction model for heart failure and cardiomyopathy after adjuvant trastuzumab therapy for breast cancer. J. Am. Heart Assoc. 2014, 3, e000472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rushton, M.; Johnson, C.; Dent, S. Trastuzumab-induced cardiotoxicity: Testing a clinical risk score in a real-world cardio-oncology population. Curr. Oncol. 2017, 24, 176–180. [Google Scholar] [CrossRef] [Green Version]
- Negishi, K.; Negishi, T.; Hare, J.L.; Haluska, B.A.; Plana, J.C.; Marwick, T.H. Independent and incremental value of deformation indices for prediction of trastuzumab-induced cardiotoxicity. J. Am. Soc. Echocardiogr. 2013, 26, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Sawaya, H.; Sebag, I.A.; Plana, J.C.; Januzzi, J.L.; Ky, B.; Cohen, V.; Gosavi, S.; Carver, J.R.; Wiegers, S.E.; Martin, R.P. Early detection and prediction of cardiotoxicity in chemotherapy-treated patients. Am. J. Cardiol. 2011, 107, 1375–1380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seferina, S.C.; Maaike de Boer, M.; van den Berkmortel, F.; van Kampen, R.J.; van de Wouw, A.J.; Joore, M.; Peer, P.G.; Voogd, A.C.; Tjan-Heijnen, V.C. Cardiotoxicity and cardiac monitoring during adjuvant trastuzumab in daily Dutch practice: A study of the Southeast Netherlands Breast Cancer Consortium. Oncologist 2016, 21, 555. [Google Scholar] [CrossRef] [Green Version]
- Thavendiranathan, P.; Abdel-Qadir, H.; Fischer, H.D.; Liu, Y.; Camacho, X.; Amir, E.; Austin, P.C.; Lee, D.S. Risk-imaging mismatch in cardiac imaging practices for women receiving systemic therapy for early-stage breast cancer: A population-based cohort study. J. Clin. Oncol. 2018, 36, 2980–2987. [Google Scholar] [CrossRef]
- Von Minckwitz, G.; Procter, M.; de Azambuja, E.; Zardavas, D.; Benyunes, M.; Viale, G.; Suter, T.; Arahmani, A.; Rouchet, N.; Clark, E. Adjuvant pertuzumab and trastuzumab in early HER2-positive breast cancer. N. Engl. J. Med. 2017, 377, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Arnaout, A.; Zhang, J.; Frank, S.; Momtazi, M.; Cordeiro, E.; Roberts, A.; Ghumman, A.; Fergusson, D.; Stober, C.; Pond, G. A Randomized Controlled Trial Comparing Alloderm-RTU with DermACELL in Immediate Subpectoral Implant-Based Breast Reconstruction. Curr. Oncol. 2021, 28, 184–195. [Google Scholar] [CrossRef] [PubMed]
- Awan, A.; Ng, T.; Conter, H.; Raskin, W.; Stober, C.; Simos, D.; Pond, G.; Dhesy-Thind, S.; Mates, M.; Kumar, V.; et al. Feasibility outcomes of a randomised, multicentre, pilot trial comparing standard 6-monthly dosing of adjuvant zoledronate with a single one-time dose in patients with early stage breast cancer. J. Bone Oncol. 2020, 26, 100343. [Google Scholar] [CrossRef] [PubMed]
- Clemons, M.; Stober, C.; Kehoe, A.; Bedard, D.; MacDonald, F.; Brunet, M.-C.; Saunders, D.; Vandermeer, L.; Mazzarello, S.; Awan, A. A randomized trial comparing vascular access strategies for patients receiving chemotherapy with trastuzumab for early-stage breast cancer. Supportive Care Cancer 2020, 28, 4891–4899. [Google Scholar] [CrossRef]
- Clemons, M.; Fergusson, D.; Simos, D.; Mates, M.; Robinson, A.; Califaretti, N.; Zibdawi, L.; Bahl, M.; Raphael, J.; Ibrahim, M. A multicentre, randomised trial comparing schedules of G-CSF (filgrastim) administration for primary prophylaxis of chemotherapy-induced febrile neutropenia in early stage breast cancer. Ann. Oncol. 2020, 31, 951–957. [Google Scholar] [CrossRef]
- Clemons, M.; Ong, M.; Stober, C.; Ernst, S.; Booth, C.; Canil, C.; Mates, M.; Robinson, A.; Blanchette, P.; Joy, A.A. A randomised trial of 4-versus 12-weekly administration of bone-targeted agents in patients with bone metastases from breast or castration-resistant prostate cancer. Eur. J. Cancer 2021, 142, 132–140. [Google Scholar] [CrossRef]


{kind=link}
| Q3-Monthly | Q4-Monthly | |
|---|---|---|
| N | 98 | 97 |
| Patient Characteristics | ||
| Age | ||
| Median [IQR] range | 55.7 [47.0–62.0] 32–83 | 56.0 [47.3–62.1] 28–77 |
| Mean (SD) | 55.4 (11.4) | 54.8 (11.3) |
| Baseline LVEF | ||
| Median (IQR) range | 65 [60–68] 54–82 | 64 [61–67] 54–76 |
| Mean (SD) | 64.5 (5.4) | 64.0 (5.0) |
| Baseline modality, N (%) echocardiogram | 71 (72.5) | 69 (71.1) |
| CV risk factors, N (%) Yes | 49 (50.0) | 51 (52.6) |
| CAD stroke PVD, N (%) Yes | 1 (1.0) | 0 (0.0) |
| Atrial fibrillation, N (%) Yes | 1 (1.0) | 2 (2.1) |
| Obesity, N (%) Yes | 10 (10.2) | 15 (15.5) |
| Smoking status | ||
| Non-smoker, N (%) | 81 (82.7) | 79 (81.4) |
| Current smoker | 5 (5.1) | 5 (5.2) |
| Past smoker | 12 (12.2) | 13 (13.4) |
| Hypertension, N (%) Yes | 21 (21.4) | 19 (19.6) |
| Diabetes, N (%) Yes | 9 (9.2) | 3 (3.1) |
| Angina, N (%) Yes | 1 (1.0) | 0 (0.0) |
| Dyslipidemia, N (%) Yes | 12 (12.2) | 7 (7.2) |
| Other risk factors *, N (%) Yes | 5 (5.1) | 6 (6.2) |
| Treatments | ||
| Chemotherapy type | ||
| N (%) Anthracycline-based | 53 (54.1) | 50 (51.6) |
| Radiation On-Study | ||
| N (%) Yes | 79 (80.6) | 68 (70.1) |
| Median (range) dose | 50 (40–92.6) | 50 (40–87.1) |
| N (%) Location: Left | 45 (57.0) | 35 (51.5) |
| left | 34 (43.0) | 32 (47.1) |
| Both | 0 (0.0) | 1 (1.5) |
| Medication information (available in only n = 83 patients) | 39 | 43 |
| Medication, N (%) Yes | 6 (15.4) | 10 (23.3) |
| Aspirin, N (%) Yes | 0 (0.0) | 1 (2.3) |
| ACE-inhibitor, N (%) Yes | 3 (7.7) | 7 (16.3) |
| Beta blocker, N (%) Yes | 3 (7.7) | 0 (0.0) |
| Angiotensin blocker, N (%) Yes | 1 (2.6) | 3 (7.0) |
| CA channel antagonist, N (%) Yes | 3 (7.7) | 0 (0.0) |
| Diuretic, N (%) Yes | 2 (5.1) | 3 (7.0) |
| Statin, N (%) Yes | 1 (2.6) | 1 (2.3) |
| Other medications, N (%) Yes | 0 (0.0) | 1 (2.3) |
| Outcomes | ||
| Completed study as planned | ||
| N (%) Yes | 90 (91.8) | 88 (90.7) |
| Reason = LVEF | 2 | 2 |
| Stopped trastuzumab | 2 | 6 |
| Metastatic disease | 3 | 0 |
| Location changed | 1 | 1 |
| Q3-Monthly | Q4-Monthly | Diff (95% CI) | ||
|---|---|---|---|---|
| N | 98 | 97 | ||
| Primary Outcome | ||||
| Any change in LVEF from baseline | N (%) Yes | 79 (80.6) | 74 (76.3) | 4.3 (−7.2, 15.9) |
| Absolute change in LVEF | Median [IQR] range | −8 [−1, −4] −26 to 17 | −6 [−10, −2] −33 to 10 | −0.6 [−2.5, 1.2] |
| Mean (SD) | −7.4 (6.5) | −6.8 (6.8) | ||
| Secondary Outcomes | ||||
| Change in LVEF | No decline | 60 (61.2) | 64 (66.0) | |
| Decline >10% to value of >53% | 19 (19.4) | 16 (16.5) | ||
| Decline ≤10% to value of ≤53% | 3 (3.1) | 5 (5.2) | ||
| Decline >10% to value of ≤53% | 16 (16.3) | 12 (12.4) | ||
| Cardiac dysfunction | N (%) Yes | 16 (16.3) | 12 (12.4) | 4.0 (−5.9, 13.8) |
| Cardiac event | N (%) Yes | 31 (31.6) | 24 (24.7) | 6.9 (−5.7, 19.5) |
| Decrease in EF | 6 (66.7) | 10 (90.9) | ||
| Congestive heart failure | 1 (11.1) | 0 () | ||
| Other * | 2 (22.2) | 1 (9.1) | ||
| Change in type of imaging modality | N (%) Yes | 7 (7.1) | 6 (6.2) | 1.0 (−6.0, 8.0) |
| Trastuzumab | N (%) Yes | 14 (14.3) | 10 (10.3) | 4.0 (−5.2, 13.2) |
| Delays | 9 (9.2) | 2 (2.1) | 7.1 (0.7, 13.5) | |
| Reduction | 3 (3.1) | 1 (1.0) | 2.0 (−1.9, 6.0) | |
| Discontinuation ** | 2 (2.0) | 7 (7.2) | −5.2 (−11.0, 0.7) | |
| Chemotherapy | N (%) Yes | 35 (35.7) | 23 (23.7) | 12. 0 (−0.7, 24.7) |
| Delay | 7 (7.1) | 9 (9.3) | −2.1 (−9.8, 5.6) | |
| Reduction | 12 (12.2) | 6 (6.2) | 6.1 (−2.0, 14.1) | |
| Discontinuation | 16 (16.3) | 8 (8.3) | 8.1 (−1.1, 17.2) | |
| Referral to cardiology | N (%) Yes | 12 (12.2) | 12 (12.4) | −0.1 (−9.4, 9.1) |
| Treatment-related hospitalization *** | N (%) Yes | 9 (9.2) | 10 (10.3) | −1.1 (−9.5, 7.2) |
| Treatment-related ER visit **** | N (%) Yes | 15 (15.3) | 11 (11.3) | 4.0 (−5.6, 13.5) |
| Time Period | N | Q3-Monthly | Q4-Monthly |
|---|---|---|---|
| Week 12 | 97 | 61.2 (5.9) | |
| Week 16 | 95 | 61.0 (5.2) | |
| Week 24 | 97 | 59.7 (5.7) | |
| Week 32 | 94 | 61.2 (6.1) | |
| Week 36 | 95 | 60.6 (6.2) | |
| Week 48 | 93/93 | 60.7 (6.2) | 60.3 (7.0) |
| Mean (95% CI) difference at week 48 | 0.40 (−1.48, 2.34) | ||
| Change in LVEF from baseline | |||
| Week 12 | 97 | −3.3 (6.2) | |
| Week 16 | 95 | −2.9 (5.3) | |
| Week 24 | 97 | −6.0 (6.4) | |
| Week 32 | 94 | −5.0 (5.8) | |
| Week 36 | 95 | −6.9 (6.3) | |
| Week 48 | 93/93 | −7.5 (6.2) | −6.8 (6.9) |
| Mean (95% CI) difference at week 48 | −0.69 (−2.59, 1.21) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dent, S.; Fergusson, D.; Aseyev, O.; Stober, C.; Pond, G.; Awan, A.A.; McGee, S.F.; Ng, T.L.; Simos, D.; Vandermeer, L.; et al. A Randomized Trial Comparing 3- versus 4-Monthly Cardiac Monitoring in Patients Receiving Trastuzumab-Based Chemotherapy for Early Breast Cancer. Curr. Oncol. 2021, 28, 5073-5083. https://doi.org/10.3390/curroncol28060427
Dent S, Fergusson D, Aseyev O, Stober C, Pond G, Awan AA, McGee SF, Ng TL, Simos D, Vandermeer L, et al. A Randomized Trial Comparing 3- versus 4-Monthly Cardiac Monitoring in Patients Receiving Trastuzumab-Based Chemotherapy for Early Breast Cancer. Current Oncology. 2021; 28(6):5073-5083. https://doi.org/10.3390/curroncol28060427
Chicago/Turabian StyleDent, Susan, Dean Fergusson, Olexiy Aseyev, Carol Stober, Gregory Pond, Arif A. Awan, Sharon F. McGee, Terry L. Ng, Demetrios Simos, Lisa Vandermeer, and et al. 2021. "A Randomized Trial Comparing 3- versus 4-Monthly Cardiac Monitoring in Patients Receiving Trastuzumab-Based Chemotherapy for Early Breast Cancer" Current Oncology 28, no. 6: 5073-5083. https://doi.org/10.3390/curroncol28060427
APA StyleDent, S., Fergusson, D., Aseyev, O., Stober, C., Pond, G., Awan, A. A., McGee, S. F., Ng, T. L., Simos, D., Vandermeer, L., Saunders, D., Hilton, J. F., Hutton, B., & Clemons, M., on behalf of the REaCT Investigators. (2021). A Randomized Trial Comparing 3- versus 4-Monthly Cardiac Monitoring in Patients Receiving Trastuzumab-Based Chemotherapy for Early Breast Cancer. Current Oncology, 28(6), 5073-5083. https://doi.org/10.3390/curroncol28060427