Association between Ureteral Clamping Time and Acute Kidney Injury during Robot-Assisted Radical Cystectomy

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Study Design
2.3. Surgery and Perioperative Care
2.4. Neoadjuvant and Adjuvant Chemotherapy
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
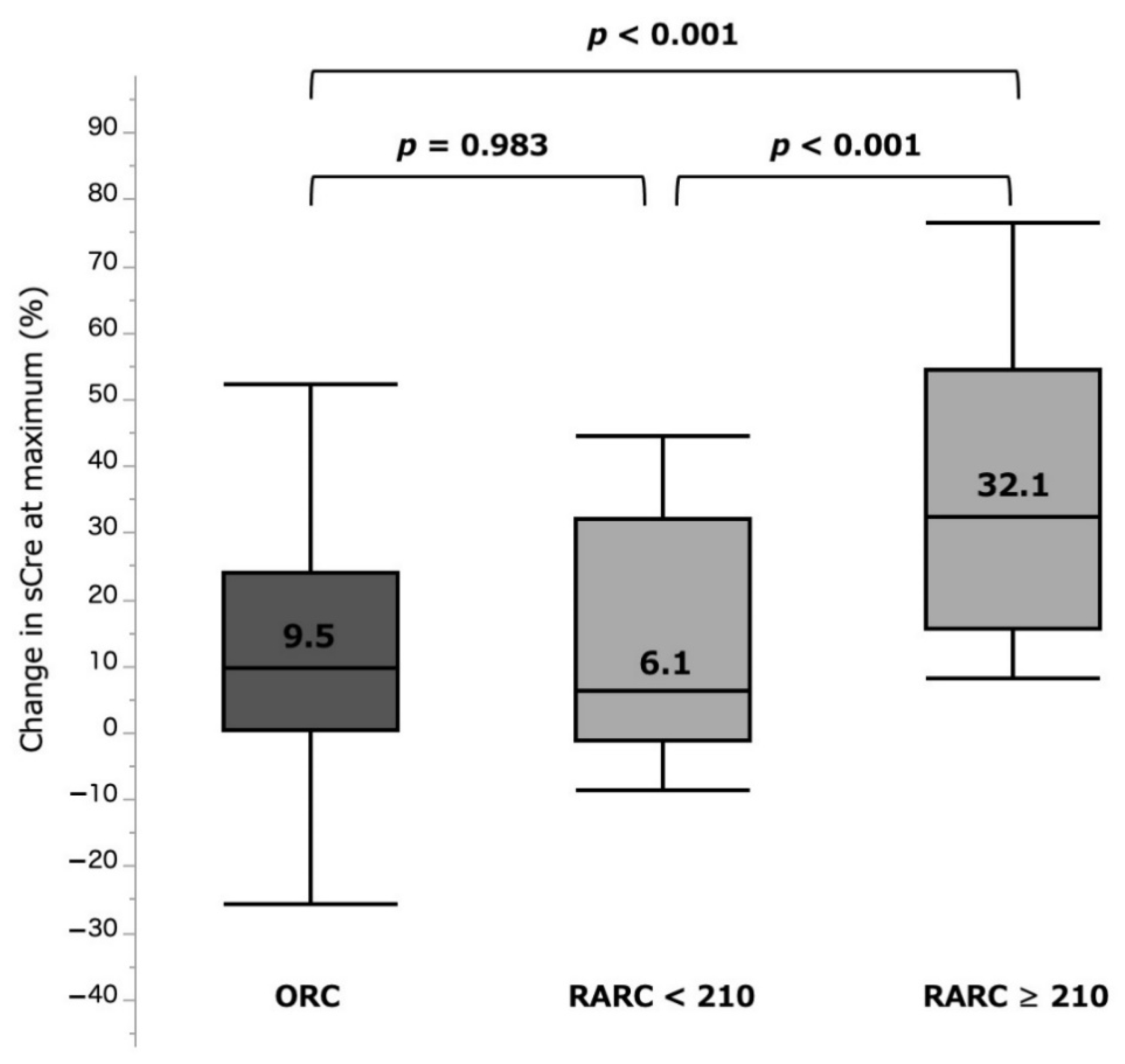
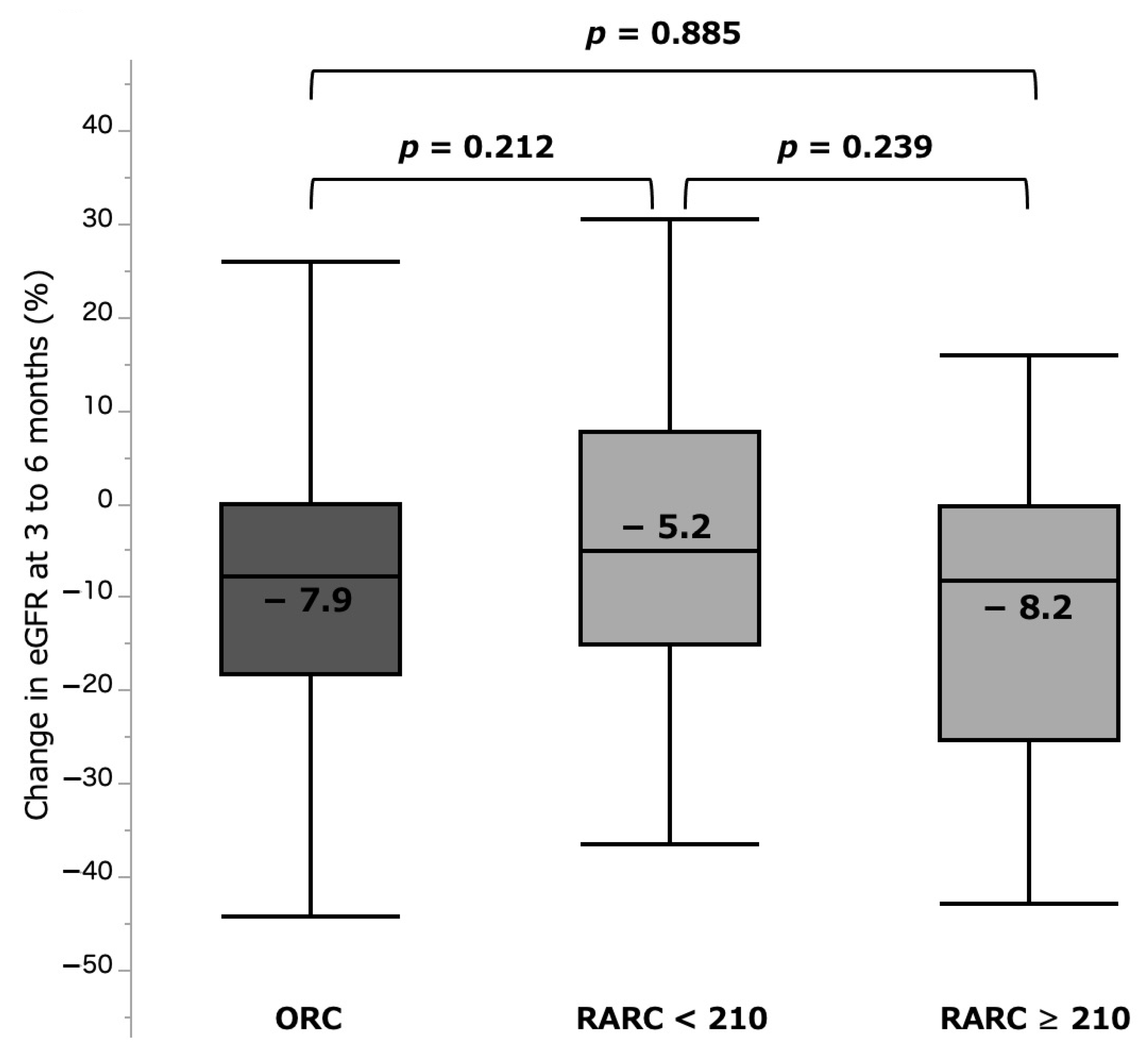
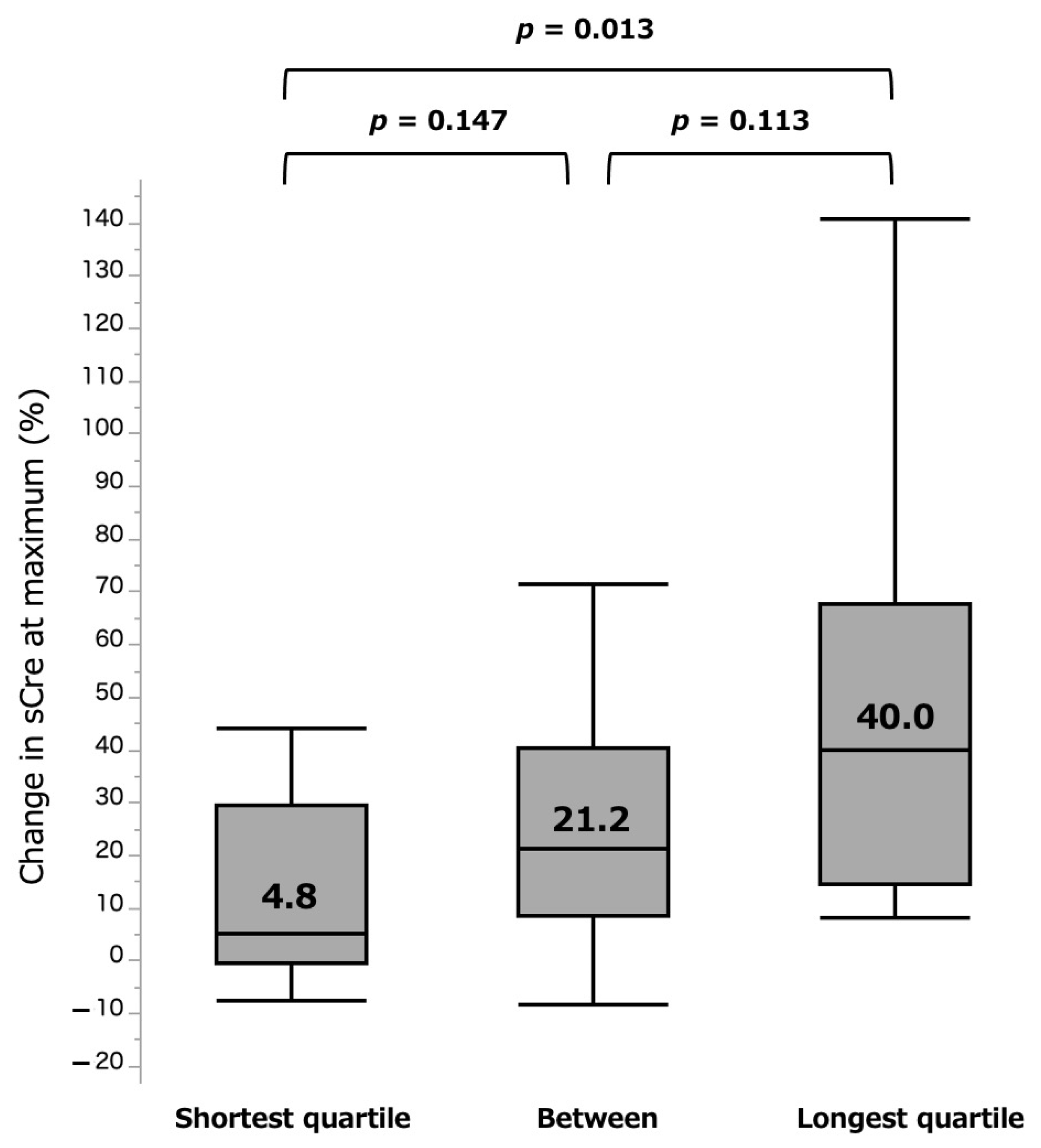
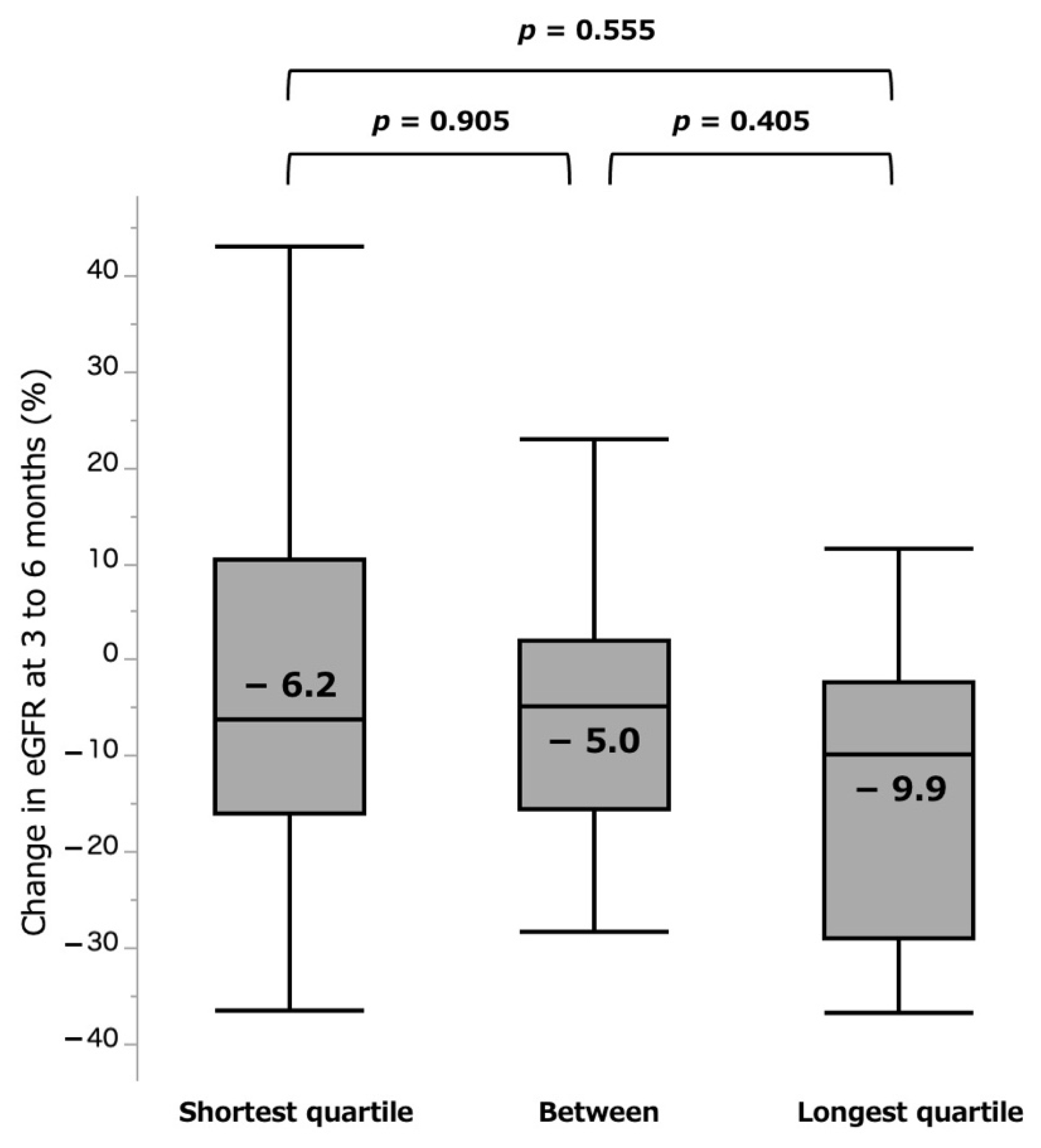
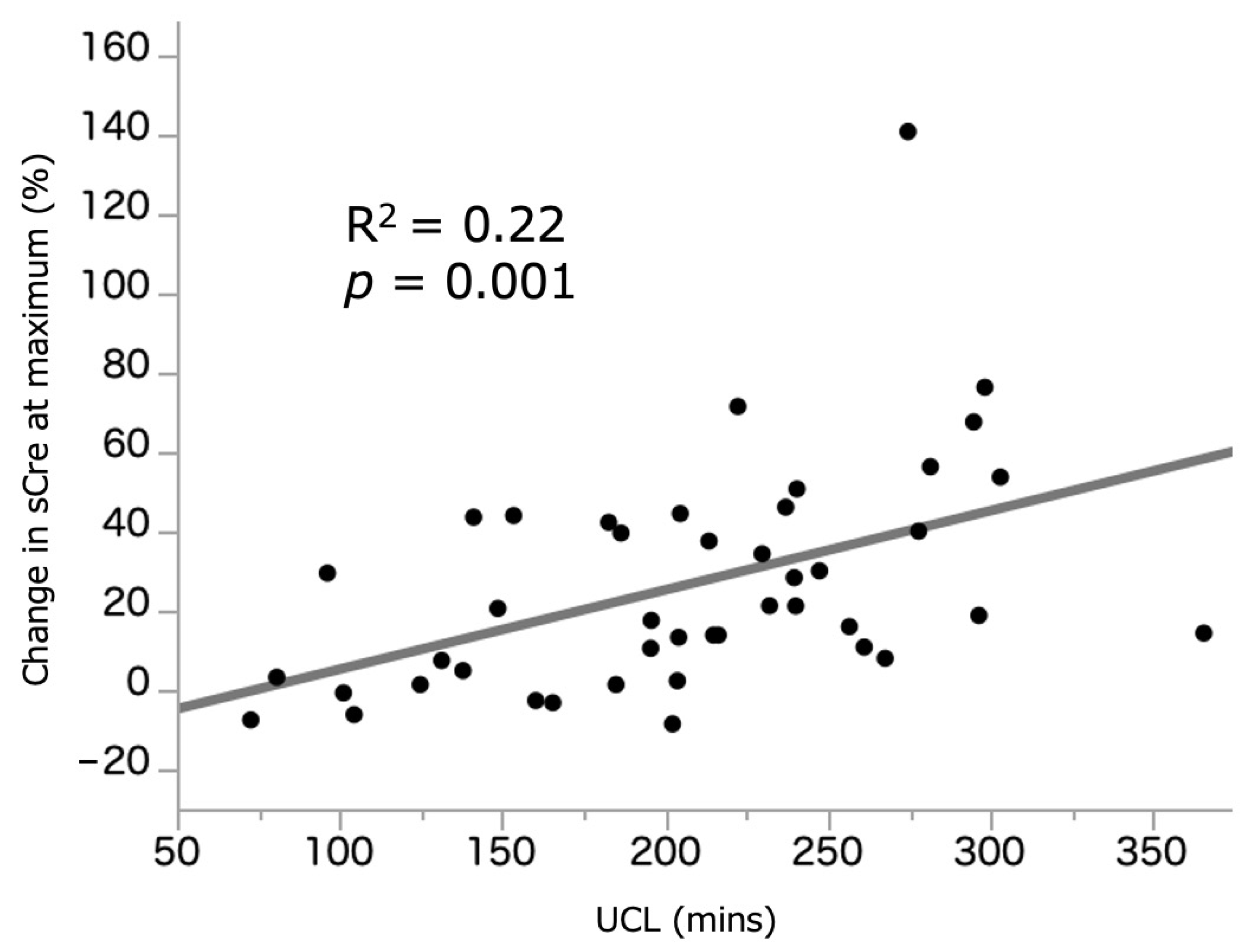
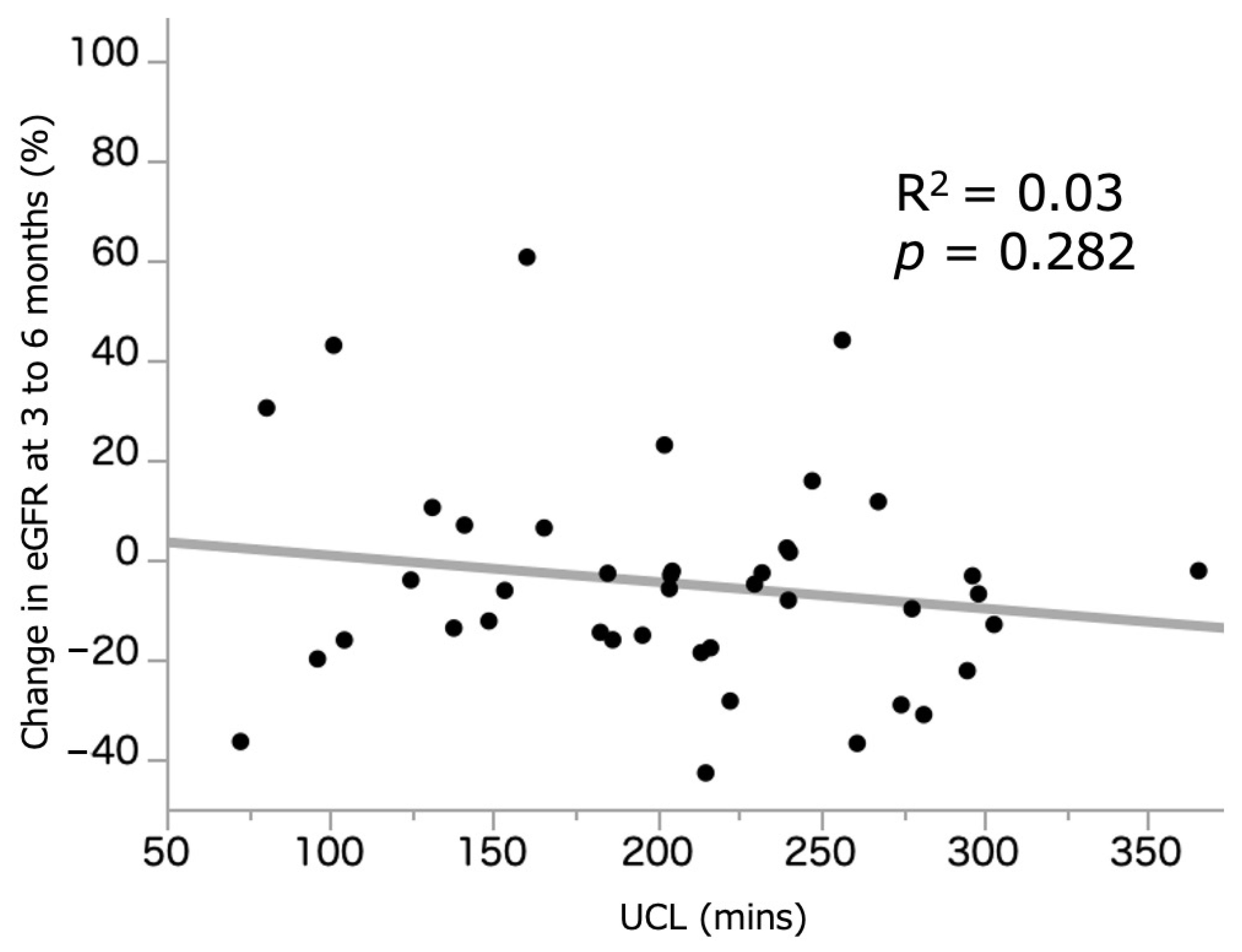
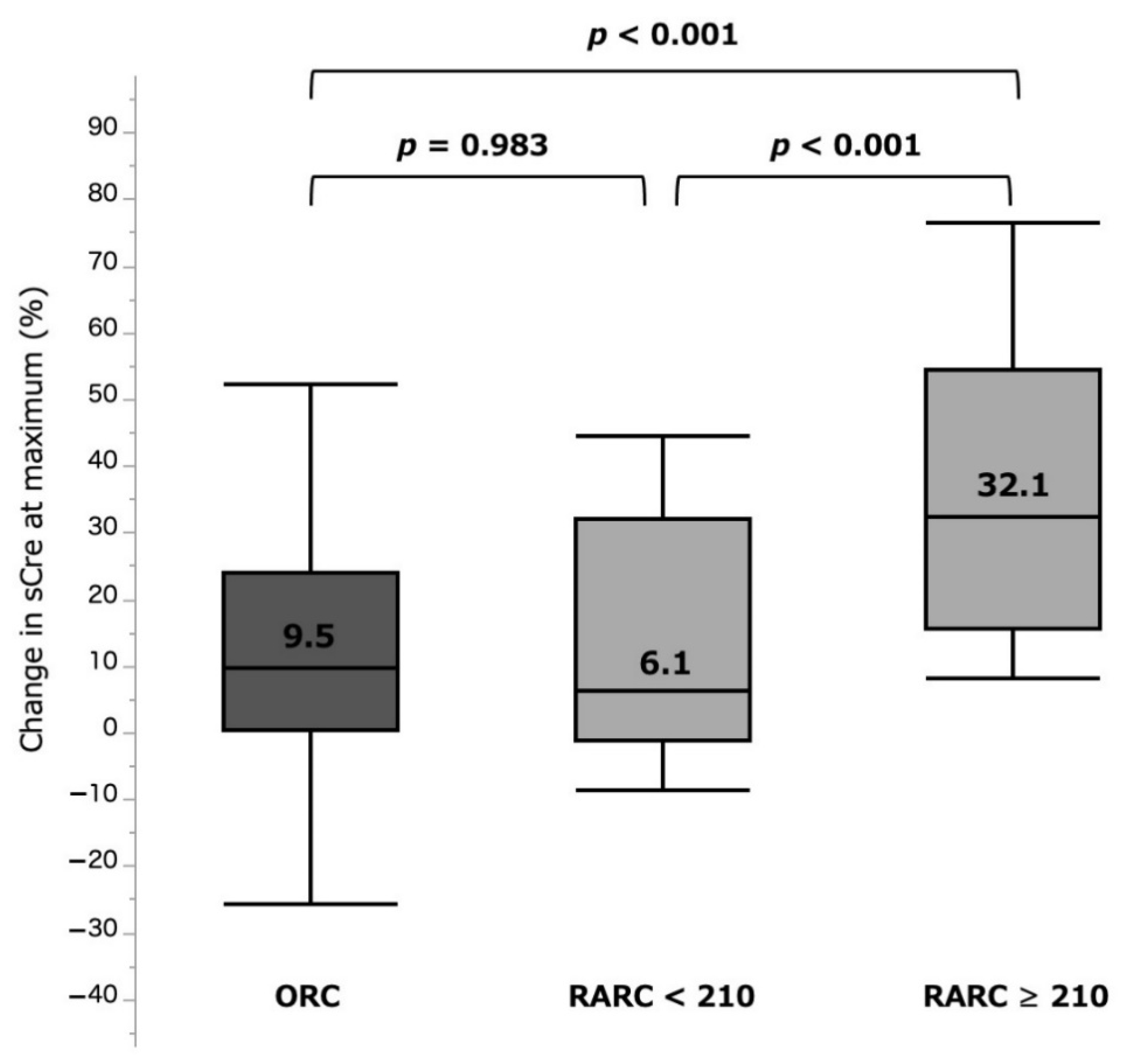
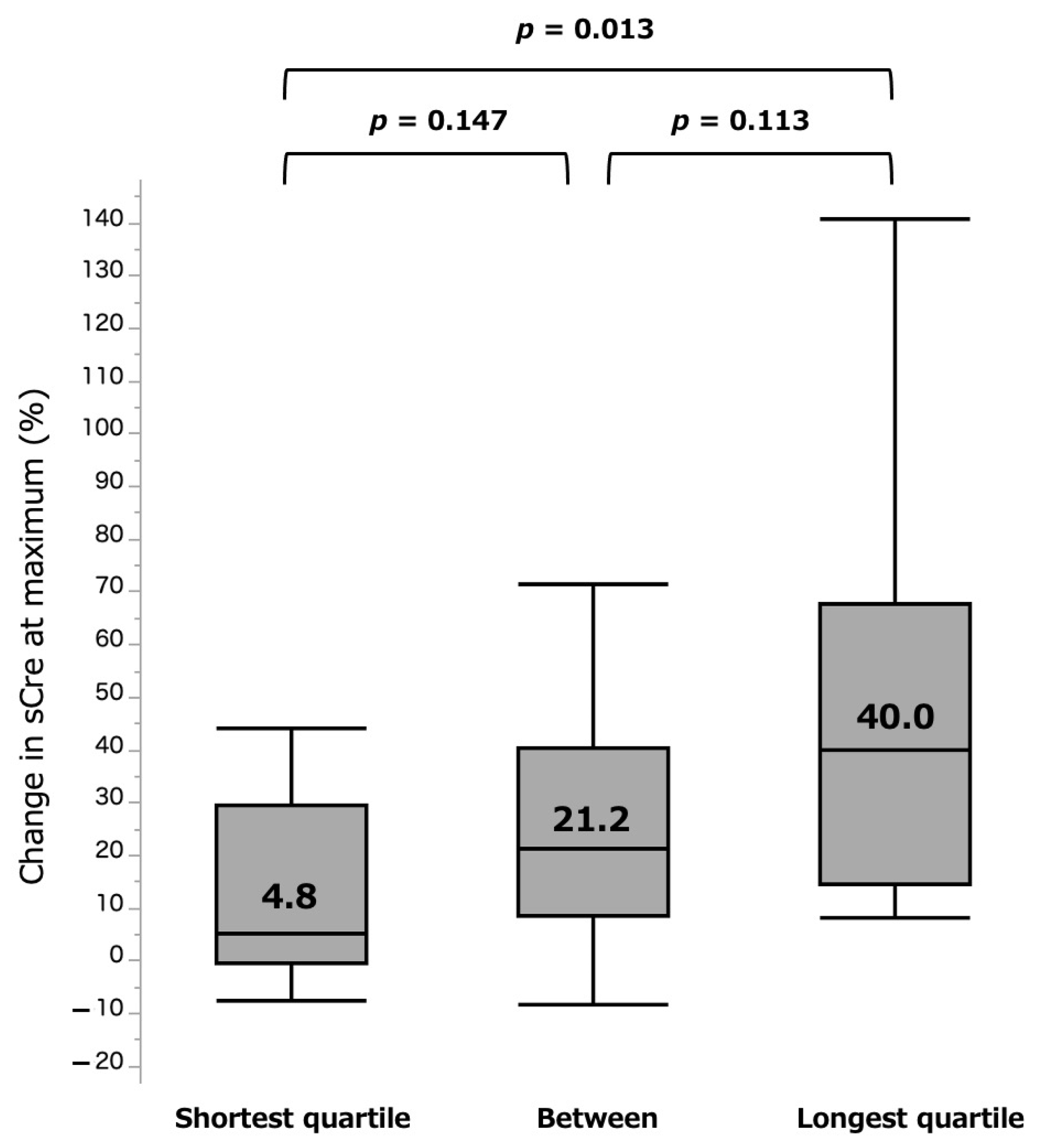
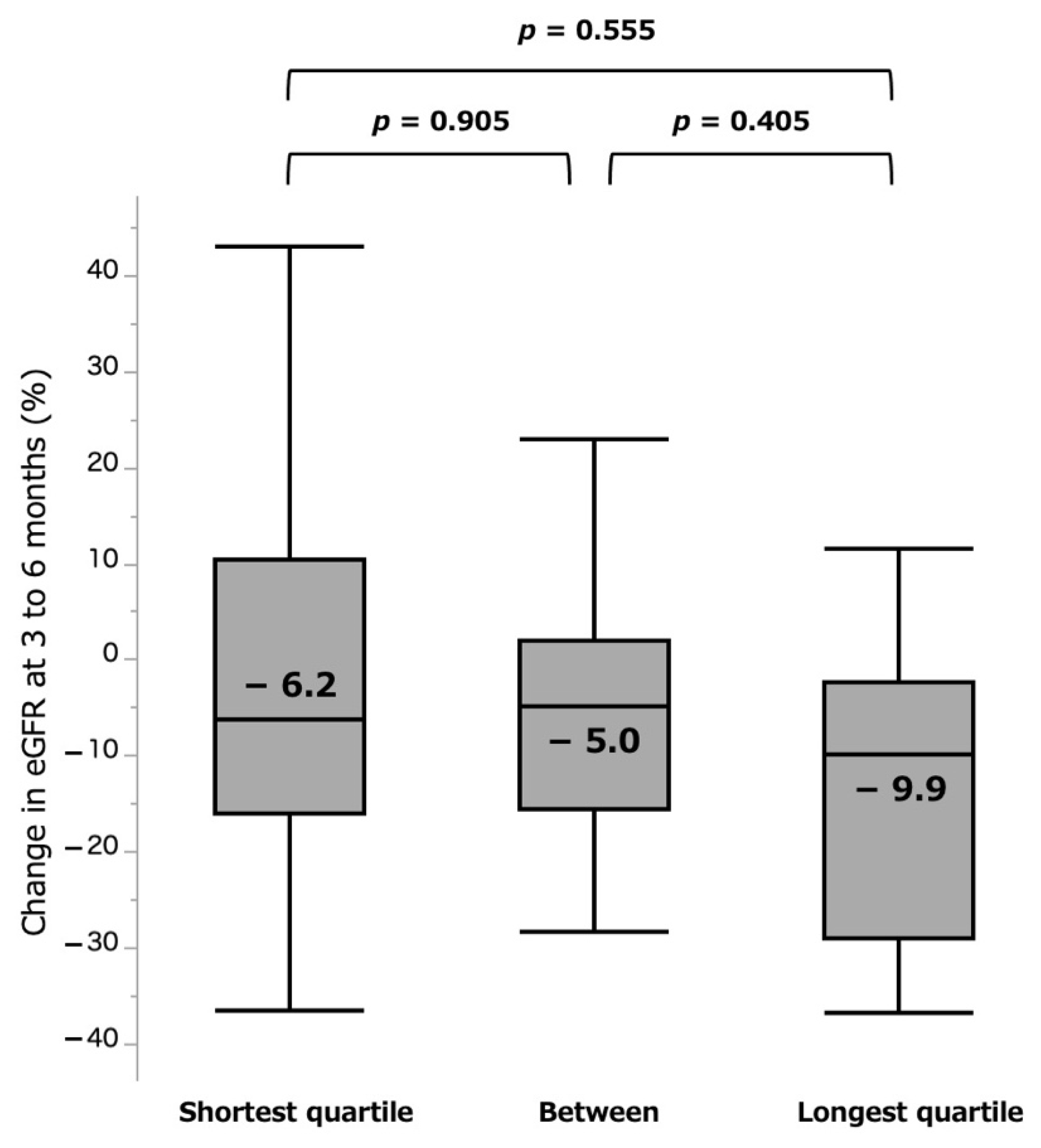
3.2. Association between UCL and Acute/Chronic Phase Renal Function Change in RARC
3.3. Relationship between UCL and Other Outcomes
3.4. Factors Affecting the Acute/Chronic Phase Renal Function Change in RARC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chang, S.S.; Bochner, B.H.; Chou, R.; Dreicer, R.; Kamat, A.M.; Lerner, S.P.; Lotan, Y.; Meeks, J.J.; Michalski, J.M.; Morgan, T.M.; et al. Treatment of non-metastatic muscle-invasive bladder cancer: Aua/asco/astro/suo guideline. J. Urol. 2017, 198, 552–559. [Google Scholar] [CrossRef]
- Witjes, J.A.; Bruins, H.M.; Cathomas, R.; Comperat, E.M.; Cowan, N.C.; Gakis, G.; Hernandez, V.; Linares Espinos, E.; Lorch, A.; Neuzillet, Y.; et al. European association of urology guidelines on muscle-invasive and metastatic bladder cancer: Summary of the 2020 guidelines. Eur. Urol. 2021, 79, 82–104. [Google Scholar] [CrossRef]
- Parekh, D.J.; Reis, I.M.; Castle, E.P.; Gonzalgo, M.L.; Woods, M.E.; Svatek, R.S.; Weizer, A.Z.; Konety, B.R.; Tollefson, M.; Krupski, T.L.; et al. Robot-assisted radical cystectomy versus open radical cystectomy in patients with bladder cancer (razor): An open-label, randomised, phase 3, non-inferiority trial. Lancet 2018, 391, 2525–2536. [Google Scholar] [CrossRef]
- Basile, D.P.; Anderson, M.D.; Sutton, T.A. Pathophysiology of acute kidney injury. Compr. Physiol. 2012, 2, 1303–1353. [Google Scholar] [PubMed] [Green Version]
- Lone, Z.; Murthy, P.B.; Zhang, J.H.; Ericson, K.J.; Thomas, L.; Khanna, A.; Haber, G.P.; Lee, B.H. Comparison of renal function after open radical cystectomy, extracorporeal robot assisted radical cystectomy, and intracorporeal robot assisted radical cystectomy. Urol. Oncol. 2021, 39, 301.e301–301.e309. [Google Scholar] [CrossRef]
- KDIGO. Kdigo clinical practice guideline for acute kidney injury. Kidney Int. Suppl. 2012, 2, 1–38. [Google Scholar]
- KDIGO. Kdigo 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1. [Google Scholar]
- Wein, A.J.; Kavoussi, L.R.; Partin, A.W.; Peters, C. Transurethral and open surgery for bladder cancer. In Campbell-Walsh Urology, 11th ed.; Elsevier: Philadelphia, PA, USA, 2016. [Google Scholar]
- Wein, A.J.; Kavoussi, L.R.; Partin, A.W.; Peters, C. Robotic and laparoscopic bladder surgery. In Campbell-Walsh Urology, 11th ed.; Elsevier: Philadelphia, PA, USA, 2016. [Google Scholar]
- Wein, A.J.; Kavoussi, L.R.; Partin, A.W.; Peters, C. Use of intestinal segments in urinary diversion. In Campbell-Walsh Urology; Elsevier: Philadelphia, PA, USA, 2016. [Google Scholar]
- Wein, A.J.; Kavoussi, L.R.; Partin, A.W.; Peters, C. Orthotopic urinary diversion. In Campbell-Walsh Urology; Elsevier: Philadelphia, PA, USA, 2016. [Google Scholar]
- Wein, A.J.; Kavoussi, L.R.; Partin, A.W.; Peters, C. Minimally invasive urinary diversion. In Campbell-Walsh Urology; Elsevier: Philadelphia, PA, USA, 2016. [Google Scholar]
- Dhar, N.B.; Klein, E.A.; Reuther, A.M.; Thalmann, G.N.; Madersbacher, S.; Studer, U.E. Outcome after radical cystectomy with limited or extended pelvic lymph node dissection. J. Urol. 2008, 179, 873–878. [Google Scholar] [CrossRef] [PubMed]
- Cerantola, Y.; Valerio, M.; Persson, B.; Jichlinski, P.; Ljungqvist, O.; Hubner, M.; Kassouf, W.; Muller, S.; Baldini, G.; Carli, F.; et al. Guidelines for perioperative care after radical cystectomy for bladder cancer: Enhanced recovery after surgery (eras((r))) society recommendations. Clin. Nutr. 2013, 32, 879–887. [Google Scholar] [CrossRef] [PubMed]
- Hegarty, N.J.; Young, L.S.; Kirwan, C.N.; O’Neill, A.J.; Bouchier-Hayes, D.M.; Sweeney, P.; Watson, R.W.; Fitzpatrick, J.M. Nitric oxide in unilateral ureteral obstruction: Effect on regional renal blood flow. Kidney Int. 2001, 59, 1059–1065. [Google Scholar] [CrossRef] [Green Version]
- ahlberg, J.; Karlberg, L.; Persson, A.E. Total and regional renal blood flow during complete unilateral ureteral obstruction. Acta Physiol. Scand. 1984, 121, 111–118. [Google Scholar] [CrossRef]
- Washino, S.; Hosohata, K.; Miyagawa, T. Roles played by biomarkers of kidney injury in patients with upper urinary tract obstruction. Int. J. Mol. Sci. 2020, 21, 5490. [Google Scholar] [CrossRef]
- Schelfhout, W.; Simons, M.; Oosterlinck, W.; De Sy, W.A. Evaluation of 99mtc-dimercaptosuccinic acid renal uptake as an index of individual kidney function after acute ureteral obstruction and desobstruction. An experimental study in rats. Eur. Urol. 1983, 9, 221–226. [Google Scholar] [CrossRef]
- Vaughan, E.D., Jr.; Gillenwater, J.Y. Recovery following complete chronic unilateral ureteral occlusion: Functional, radiographic and pathologic alterations. J. Urol. 1971, 106, 27–35. [Google Scholar] [CrossRef]
- Fink, R.L.; Caridis, D.T.; Chmiel, R.; Ryan, G. Renal impairment and its reversibility following variable periods of complete ureteric obstruction. Aust. N. Z. J. Surg. 1980, 50, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Makris, K.; Spanou, L. Acute kidney injury: Definition, pathophysiology and clinical phenotypes. Clin. Biochemist. Rev. 2016, 37, 85–98. [Google Scholar]
- Chawla, L.S.; Eggers, P.W.; Star, R.A.; Kimmel, P.L. Acute kidney injury and chronic kidney disease as interconnected syndromes. N. Engl. J. Med. 2014, 371, 58–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gameiro, J.; Fonseca, J.A.; Neves, M.; Jorge, S.; Lopes, J.A. Acute kidney injury in major abdominal surgery: Incidence, risk factors, pathogenesis and outcomes. Ann. Intensive Care 2018, 8, 22. [Google Scholar] [CrossRef] [Green Version]
- Bravi, C.A.; Vertosick, E.; Benfante, N.; Tin, A.; Sjoberg, D.; Hakimi, A.A.; Touijer, K.; Montorsi, F.; Eastham, J.; Russo, P.; et al. Impact of acute kidney injury and its duration on long-term renal function after partial nephrectomy. Eur. Urol. 2019, 76, 398–403. [Google Scholar] [CrossRef]
- Furrer, M.A.; Schneider, M.P.; Burkhard, F.C.; Wuethrich, P.Y. Incidence and perioperative risk factors for early acute kidney injury after radical cystectomy and urinary diversion. Urol. Oncol. 2018, 36, 306.e317–306.e323. [Google Scholar] [CrossRef] [PubMed]
- Mancini, M.; Righetto, M.; Baggio, G. Spotlight on gender-specific disparities in bladder cancer. Urologia 2020, 87, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Legrand, M.; Rossignol, P. Cardiovascular consequences of acute kidney injury. N. Engl. J. Med. 2020, 382, 2238–2247. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Noone, A.; Krapcho, M.; Miller, D.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D. Seer Cancer Statistics Review, 1975–2017. Available online: https://seer.cancer.gov/csr/1975_2017/ (accessed on 23 March 2021).
- Schmitt, R.; Coca, S.; Kanbay, M.; Tinetti, M.E.; Cantley, L.G.; Parikh, C.R. Recovery of kidney function after acute kidney injury in the elderly: A systematic review and meta-analysis. Am. J. Kidney Dis. 2008, 52, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Ishani, A.; Xue, J.L.; Himmelfarb, J.; Eggers, P.W.; Kimmel, P.L.; Molitoris, B.A.; Collins, A.J. Acute kidney injury increases risk of esrd among elderly. J. Am. Soc. Nephrol. 2009, 20, 223–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, J.W.; Tyritzis, S.; Nyberg, T.; Schumacher, M.C.; Laurin, O.; Adding, C.; Jonsson, M.; Khazaeli, D.; Steineck, G.; Wiklund, P.; et al. Robot-assisted radical cystectomy (rarc) with intracorporeal neobladder—What is the effect of the learning curve on outcomes? BJU Int. 2014, 113, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Tuderti, G.; Mastroianni, R.; Brassetti, A.; Bove, A.M.; Misuraca, L.; Anceschi, U.; Ferriero, M.; Gallucci, M.; Simone, G. Robot-assisted radical cystectomy with intracorporeal neobladder: Impact of learning curve and long-term assessment of functional outcomes. Minerva Urol. Nefrol. 2020. Online ahead of print. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 120) | RARC (n = 44) | ORC (n = 76) | p-Value | |
|---|---|---|---|---|
| Age at surgery, median (IQR) | 71.6 (62.4–77.5) | 74.3 (69.0–80.0) | 69.2 (58.5–75.6) | 0.001 |
| Sex, male (%) | 88 (73.3) | 34 (77.3) | 54 (71.1) | 0.454 |
| ASA score | 0.043 | |||
| 1 | 12 (10.0) | 1 (2.3) | 11 (14.5) | |
| 2 | 86 (71.7) | 37 (84.1) | 49 (64.5) | |
| 3 | 21 (17.5) | 6 (13.6) | 15 (19.7) | |
| 4 | 1 (0.8) | 0 (0.0) | 1 (1.3) | |
| Diabetes mellitus | 27 (22.5) | 13 (29.5) | 14 (18.4) | 0.164 |
| Hypertension | 34 (28.3) | 12 (27.3) | 22 (28.9) | 0.844 |
| BMI, median (IQR) | 22.2 (19.8–24.6) | 22.4 (19.8–24.8) | 21.9 (19.8–24.6) | 0.226 |
| Preoperative sCre, median (IQR) | 0.9 (0.8–1.2) | 0.9 (0.8–1.2) | 0.9 (0.7–1.2) | 0.174 |
| Preoperative eGFR, median (IQR) | 59.5 (45.6–76.7) | 52.0 (45.1–70.1) | 62.5 (47.6–81.2) | 0.065 |
| Neoadjuvant chemotherapy | 60 (50.0) | 21 (47.7) | 39 (51.3) | 0.705 |
| Preoperative T stage | 0.278 | |||
| <T1 | 32 (26.7) | 9 (20.5) | 23 (30.3) | |
| T2 | 49 (40.8) | 20 (45.5) | 19 (25.0) | |
| T3 | 25 (20.8) | 12 (27.3) | 13 (17.1) | |
| Preoperative hydronephrosis | 38 (31.7) | 16 (36.4) | 22 (28.9) | 0.402 |
| Type of urinary diversion | <0.001 | |||
| Ileal conduit | 74 (61.7) | 35 (79.5) | 39 (51.3) | |
| Neobladder | 29 (24.2) | 2 (4.5) | 27 (35.5) | |
| Ureterocutaneostomy | 17 (14.2) | 7 (15.9) | 10 (13.2) | |
| ICUD or ECUD | ||||
| ICUD | - | 28 (63.6) | - | - |
| ECUD | - | 18 (40.9) | - | - |
| ALL (n = 120) | RARC < 210 (n = 22) | RARC ≥ 210 (n = 22) | ORC (n = 76) | p-Value RARC < 210 vs. RARC ≥ 210 | p-Value RARC < 210 vs. ORC | p-Value RARC ≥ 210 vs. ORC | |
|---|---|---|---|---|---|---|---|
| Postop maximum sCre | 1.1 (0.8–1.4) | 1.0 (0.8–1.3) | 1.3 (1.2–1.5) | 1.0 (0.8–1.3) | 0.005 | 0.414 | <0.001 |
| Change in sCre at maximum (%) | 13.8 (3.0–30.5) | 6.1 (−1.3 to 32.0) | 32.1 (15.5–54.3) | 9.5 (0.2–23.9) | <0.001 | 0.983 | <0.001 |
| AKI (stage) | <0.001 | 0.310 | <0.001 | ||||
| no AKI | 111 (92.5) | 22 (100.0) | 15 (68.2) | 74 (97.4) | |||
| stage 1 | 8.0 (6.7) | 0 (0.0) | 6 (27.3) | 2 (2.6) | |||
| stage 2 | 1.0 (0.8) | 0 (0.0) | 1 (4.5) | 0 (0.0) | |||
| Postoperative eGFR at 3 to 6 months | 52.4 (39.3–67.3) | 56.0 (41.3–64.0) | 44.5 (36.3–61.4) | 53.1 (39.8–71.7) | 0.148 | 0.997 | 0.147 |
| Change in eGFR at 3 to 6 months (%) | −7.8 (−17.9 to 0.0) | −5.0 (−15.2 to 7.7) | −8.2 (−25.4 to −0.4) | −7.9 (−18.3 to −0.2) | 0.239 | 0.212 | 0.885 |
| Surgical time, median | 454.0 (356.0–515.0) | 392.0 (278.8–452.8) | 466.0 (430.8–536.5) | 463.0 (356.0–548.0) | <0.001 | 0.003 | 0.395 |
| EBL, median | 545.0 (217.5–1578.5) | 103.5 (52.3–262.5) | 275.0 (160.3–470.0) | 1080.0 (527.5–2417.5) | <0.001 | <0.001 | <0.001 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| β-Coefficient | SE | p-Value | β-Coefficient | SE | p-Value | |
| Age (continuous) | −1.12 | 0.43 | 0.012 | −0.70 | 0.46 | 0.137 |
| Diabetes mellitus | −5.41 | 4.67 | 0.253 | |||
| Hypertension | 1.64 | 4.85 | 0.736 | |||
| Preoperative eGFR (continuous) | 0.17 | 0.24 | 0.494 | |||
| Surgical time | 0.09 | 0.04 | 0.025 | −0.07 | 0.07 | 0.292 |
| EBL | 0.01 | 0.01 | 0.614 | |||
| Hydronephrosis | 2.15 | 4.48 | 0.634 | |||
| UCL (continuous) | 0.20 | 0.06 | 0.001 | 0.25 | 0.11 | 0.023 |
| Univariate | |||
|---|---|---|---|
| β-Coefficient | SE | p-Value | |
| Age (continuous) | 0.59 | 0.34 | 0.061 |
| Diabetes mellitus | 5.87 | 3.48 | 0.100 |
| Hypertension | −4.84 | 3.61 | 0.187 |
| Preoperative eGFR (continuous) | −0.43 | 0.18 | 0.019 |
| Surgical time | −0.02 | 0.03 | 0.483 |
| EBL | 0.01 | 0.01 | 0.501 |
| Hydronephrosis | −3.52 | 3.38 | 0.303 |
| Perioperative UTI | −2.80 | 3.35 | 0.411 |
| UCL (continuous) | −0.05 | 0.05 | 0.282 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishiyama, Y.; Kondo, T.; Ishihara, H.; Yoshida, K.; Iizuka, J.; Tanabe, K.; Takagi, T. Association between Ureteral Clamping Time and Acute Kidney Injury during Robot-Assisted Radical Cystectomy. Curr. Oncol. 2021, 28, 4986-4997. https://doi.org/10.3390/curroncol28060418
Ishiyama Y, Kondo T, Ishihara H, Yoshida K, Iizuka J, Tanabe K, Takagi T. Association between Ureteral Clamping Time and Acute Kidney Injury during Robot-Assisted Radical Cystectomy. Current Oncology. 2021; 28(6):4986-4997. https://doi.org/10.3390/curroncol28060418
Chicago/Turabian StyleIshiyama, Yudai, Tsunenori Kondo, Hiroki Ishihara, Kazuhiko Yoshida, Junpei Iizuka, Kazunari Tanabe, and Toshio Takagi. 2021. "Association between Ureteral Clamping Time and Acute Kidney Injury during Robot-Assisted Radical Cystectomy" Current Oncology 28, no. 6: 4986-4997. https://doi.org/10.3390/curroncol28060418
APA StyleIshiyama, Y., Kondo, T., Ishihara, H., Yoshida, K., Iizuka, J., Tanabe, K., & Takagi, T. (2021). Association between Ureteral Clamping Time and Acute Kidney Injury during Robot-Assisted Radical Cystectomy. Current Oncology, 28(6), 4986-4997. https://doi.org/10.3390/curroncol28060418