Feasibility of Stereotactic Body Radiation Therapy on Unresectable Stage III NSCLC with Peripheral Primary Tumor: A Prospective Study (GFPC 01-14)

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
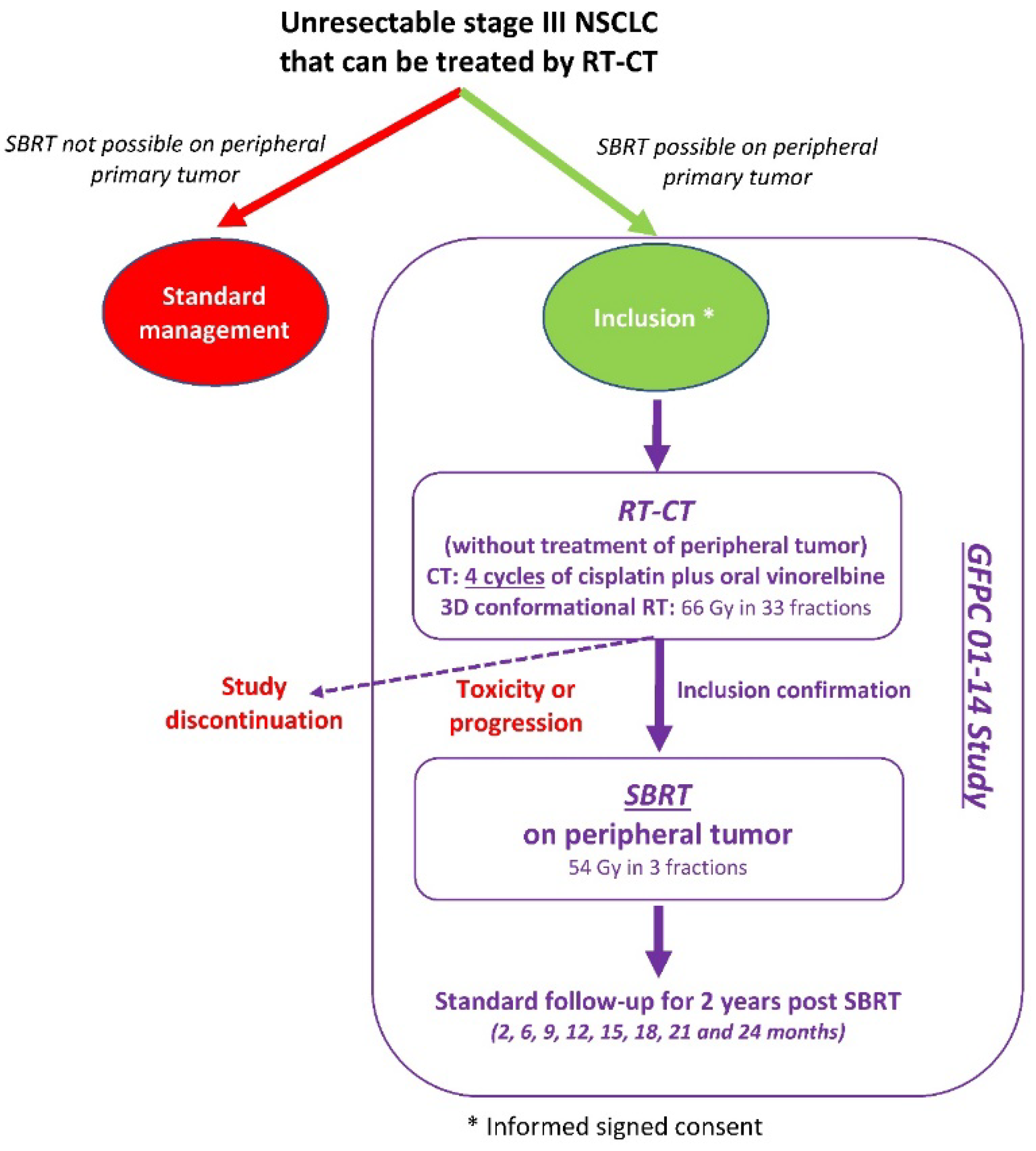
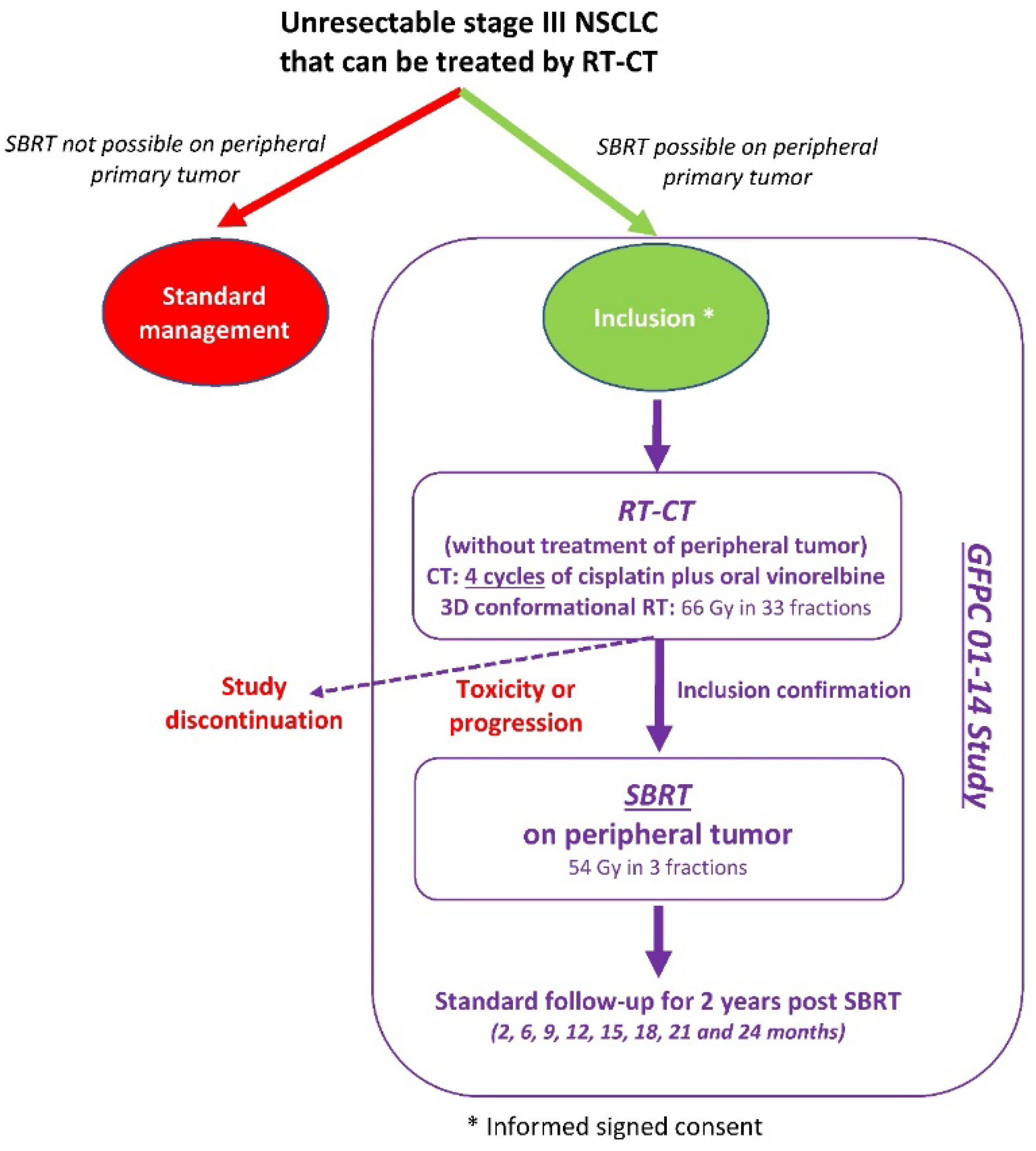
2.1. Type of Study and Design
2.2. Patients
2.3. Treatments
2.4. Data Collection and Evaluations
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Cancer Fact Sheet No. 297. 2017. Available online: http://www.who.int/mediacentre/factsheets/fs297/en/ (accessed on 28 September 2021).
- Yang, P.; Allen, M.S.; Aubry, M.C.; Wampfler, J.A.; Marks, R.S.; Edell, E.S.; Thibodeau, S.; Adjei, A.A.; Jett, J.; Deschamps, C. Clinical features of 5,628 primary lung cancer patients: Experience at Mayo Clinic from 1997 to 2003. Chest 2005, 128, 452–462. [Google Scholar] [CrossRef]
- Goya, T.; Asamura, H.; Yoshimura, H.; Kato, H.; Shimokata, K.; Tsuchiya, R.; Sohara, Y.; Miya, T.; Miyaoka, E.; The Japanese Joint Committee of Lung Cancer Registry. Prognosis of 6644 resected non-small cell lung cancers in Japan: A Japanese lung cancer registry study. Lung Cancer 2005, 50, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Eberhardt, W.E.; De Ruysscher, D.; Weder, W.; Le Pechoux, C.; De Leyn, P.; Hoffmann, H.; Westeel, V.; Stahel, R.; Felip, E.; Peters, S.; et al. 2nd ESMO Consensus Conference in Lung Cancer: Locally advanced stage III non-small-cell lung cancer. Ann. Oncol. 2015, 26, 1573–1588. [Google Scholar] [CrossRef] [PubMed]
- Vokes, E.E.; Herndon, J.E., 2nd; Crawford, J.; Leopold, K.A.; Perry, M.C.; Miller, A.A.; Green, M.R. Randomized phase II study of cisplatin with gemcitabine or paclitaxel or vinorelbine as induction chemotherapy followed by concomitant chemoradiotherapy for stage IIIB non-small-cell lung cancer: Cancer and leukemia group B study 9431. J. Clin. Oncol. 2002, 20, 4191–4198. [Google Scholar] [CrossRef] [PubMed]
- Descourt, R.; Vergnenegre, A.; Barlesi, F.; Lena, H.; Fournel, P.; Falchero, L.; Berard, H.; Hureaux, J.; Le Caer, H.; Chavaillon, J.M.; et al. Oral vinorelbine and cisplatin with concurrent radiotherapy after induction chemotherapy with cisplatin and docetaxel for patients with locally advanced non-small cell lung cancer: The GFPC 05-03 study. J. Thorac. Oncol. 2011, 6, 351–357. [Google Scholar] [CrossRef] [Green Version]
- Graham, M.V.; Purdy, J.A.; Emami, B.; Harms, W.; Bosch, W.; Lockett, M.A.; Perez, C.A. Clinical dose-volume histogram analysis for pneumonitis after 3D treatment for non-small cell lung cancer (NSCLC). Int. J. Radiat. Oncol. Biol. Phys. 1999, 45, 323–329. [Google Scholar] [CrossRef]
- Baumann, P.; Nyman, J.; Lax, I.; Friesland, S.; Hoyer, M.; Rehn Ericsson, S.; Johansson, K.A.; Ekberg, L.; Morhed, E.; Paludan, M.; et al. Factors important for efficacy of stereotactic body radiotherapy of medically inoperable stage I lung cancer. A retrospective analysis of patients treated in the Nordic countries. Acta Oncol. 2006, 45, 787–795. [Google Scholar] [CrossRef]
- Martel-Lafay, I. Stereotactic body radiotherapy for stage I non-small cell lung cancer. Clevel. Clin. J. Med. 2012, 14, 282–288. [Google Scholar]
- Timmerman, R.; McGarry, R.; Yiannoutsos, C.; Papiez, L.; Tudor, K.; DeLuca, J.; Ewing, M.; Abdulrahman, R.; DesRosiers, C.; Williams, M.; et al. Excessive toxicity when treating central tumors in a phase II study of stereotactic body radiation therapy for medically inoperable early-stage lung cancer. J. Clin. Oncol. 2006, 24, 4833–4839. [Google Scholar] [CrossRef]
- Fleming, T.R. One-sample multiple testing procedure for phase II clinical trials. Biometrics 1982, 38, 143–151. [Google Scholar]
- Ball, D.; Mai, G.T.; Vinod, S.; Babington, S.; Ruben, J.; Kron, T.; Chesson, B.; Herschtal, A.; Vanevski, M.; Rezo, A.; et al. Stereotactic ablative radiotherapy versus standard radiotherapy in stage 1 non-small-cell lung cancer (TROG 09.02 CHISEL): A phase 3, open-label, randomised controlled trial. Lancet Oncol. 2019, 20, 494–503. [Google Scholar] [CrossRef]
- Li, C.; Wang, L.; Wu, Q.; Zhao, J.; Yi, F.; Xu, J.; Wei, Y.; Zhang, W. A meta-analysis comparing stereotactic body radiotherapy vs conventional radiotherapy in inoperable stage I non-small cell lung cancer. Medicine 2020, 99, e21715. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.; Loo, B.W., Jr.; Biswas, T.; Ding, G.X.; El Naqa, I.M.; Jackson, A.; Kong, F.M.; LaCouture, T.; Miften, M.; Solberg, T.; et al. Local Control After Stereotactic Body Radiation Therapy for Stage I Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 160–171. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.K.; Hennon, M.; Ma, S.J.; Demmy, T.L.; Picone, A.; Dexter, E.U.; Nwogu, C.; Attwood, K.; Tan, W.; Hermann, G.M.; et al. A pilot study of stereotactic body radiation therapy (SBRT) after surgery for stage III non-small cell lung cancer. BMC Cancer 2018, 18, 1183. [Google Scholar] [CrossRef] [PubMed]
- Higgins, K.A.; Pillai, R.N.; Chen, Z.; Tian, S.; Zhang, C.; Patel, P.; Pakkala, S.; Shelton, J.; Force, S.D.; Fernandez, F.G.; et al. Concomitant Chemotherapy and Radiotherapy with SBRT Boost for Unresectable Stage III Non-Small Cell Lung Cancer: A Phase I Study. J. Thorac. Oncol. 2017, 12, 1687–1695. [Google Scholar] [CrossRef] [Green Version]
- Kaster, T.S.; Yaremko, B.; Palma, D.A.; Rodrigues, G.B. Radical-intent hypofractionated radiotherapy for locally advanced non-small-cell lung cancer: A systematic review of the literature. Clin. Lung Cancer 2015, 16, 71–79. [Google Scholar] [CrossRef]
- Zehentmayr, F.; Grambozov, B.; Kaiser, J.; Fastner, G.; Sedlmayer, F. Radiation dose escalation with modified fractionation schedules for locally advanced NSCLC: A systematic review. Thorac. Cancer 2020, 11, 1375–1385. [Google Scholar] [CrossRef] [Green Version]
- Faivre-Finn, C.; Vicente, D.; Kurata, T.; Planchard, D.; Paz-Ares, L.; Vansteenkiste, J.F.; Spigel, D.R.; Garassino, M.C.; Reck, M.; Senan, S.; et al. Four-Year Survival With Durvalumab After Chemoradiotherapy in Stage III NSCLC-An Update From the PACIFIC Trial. J. Thorac. Oncol. 2021, 16, 860–867. [Google Scholar] [CrossRef]
- Vanneste, B.G.L.; Van Limbergen, E.J.; Reynders, K.; De Ruysscher, D. An overview of the published and running randomized phase 3 clinical results of radiotherapy in combination with immunotherapy. Transl. Lung Cancer Res. 2021, 10, 2048–2058. [Google Scholar] [CrossRef]
- Kwon, E.D.; Drake, C.G.; Scher, H.I.; Fizazi, K.; Bossi, A.; van den Eertwegh, A.J.; Krainer, M.; Houede, N.; Santos, R.; Mahammedi, H.; et al. Ipilimumab versus placebo after radiotherapy in patients with metastatic castration-resistant prostate cancer that had progressed after docetaxel chemotherapy (CA184-043): A multicentre, randomised, double-blind, phase 3 trial. Lancet Oncol. 2014, 15, 700–712. [Google Scholar] [CrossRef] [Green Version]
- Butts, C.; Socinski, M.A.; Mitchell, P.L.; Thatcher, N.; Havel, L.; Krzakowski, M.; Nawrocki, S.; Ciuleanu, T.E.; Bosquee, L.; Trigo, J.M.; et al. Tecemotide (L-BLP25) versus placebo after chemoradiotherapy for stage III non-small-cell lung cancer (START): A randomised, double-blind, phase 3 trial. Lancet Oncol. 2014, 15, 59–68. [Google Scholar] [CrossRef] [Green Version]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Kurata, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Overall Survival with Durvalumab after Chemoradiotherapy in Stage III NSCLC. N. Engl. J. Med. 2018, 379, 2342–2350. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Patients and Treatment Characteristics | n = 19 |
|---|---|
| Age, years, median (range) | 60.9 (38–76) |
| Male gender, n (%) | 15 (78) |
| Stage, n (%) | |
| IIIA | 10 (53) |
| IIIB | 9 (47) |
| Histology, n (%) | |
| Adenocarcinoma | 14 (74) |
| Squamous-cell carcinoma | 2 (10.5) |
| Undifferentiated carcinoma | 2 (10.5) |
| Other | 1 (5) |
| ECOG performance status, n (%) | |
| 0 | 13 (68) |
| 1 | 6 (32) |
| Tobacco status, n (%) | |
| Current smoker | 8 (42) |
| Former smoker | 11 (58) |
| Peripheral primary tumor size, mm, median (range) | 19.0 (10–36) |
| Radiotherapy | |
| Number of fractions performed, median (range) | 33 (30–33) |
| Total dose, Gy, median (range) | 66 (0–66) |
| Chemotherapy | |
| Number of cycles, median (range) | 4 (3–4) |
| SBRT | |
| Total volume GTV, mm, median (range) | 3.0 (1–24) |
| Number of fractions performed, median (range) | 3 (3–5) |
| Radiotherapy duration, days, median (range) | 5 (3–16) |
| Total dose administered at prescription isodose, Gy, median (range) | 54 (10–62) |
| Prescription isodose, %, median (range) | 80 (70–99) |
| Type of radiotherapy, n (%) | |
| CyberKnife | 9 (47) |
| Accelerator | 2 (11) |
| Novalis | 1 (5) |
| TrueBeam | 1 (5) |
| Vero | 2 (11) |
| Other | 4 (21) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martel-Lafay, I.; Monnet, I.; Lardy-Cleaud, A.; Danhier, S.; Salem, N.; Gallocher, O.; Fournel, P.; Chouaid, C.; Bylicki, O.; the GFPC 01-14 Investigators. Feasibility of Stereotactic Body Radiation Therapy on Unresectable Stage III NSCLC with Peripheral Primary Tumor: A Prospective Study (GFPC 01-14). Curr. Oncol. 2021, 28, 3804-3811. https://doi.org/10.3390/curroncol28050324
Martel-Lafay I, Monnet I, Lardy-Cleaud A, Danhier S, Salem N, Gallocher O, Fournel P, Chouaid C, Bylicki O, the GFPC 01-14 Investigators. Feasibility of Stereotactic Body Radiation Therapy on Unresectable Stage III NSCLC with Peripheral Primary Tumor: A Prospective Study (GFPC 01-14). Current Oncology. 2021; 28(5):3804-3811. https://doi.org/10.3390/curroncol28050324
Chicago/Turabian StyleMartel-Lafay, Isabelle, Isabelle Monnet, Audrey Lardy-Cleaud, Serge Danhier, Naji Salem, Olivier Gallocher, Pierre Fournel, Christos Chouaid, Olivier Bylicki, and the GFPC 01-14 Investigators. 2021. "Feasibility of Stereotactic Body Radiation Therapy on Unresectable Stage III NSCLC with Peripheral Primary Tumor: A Prospective Study (GFPC 01-14)" Current Oncology 28, no. 5: 3804-3811. https://doi.org/10.3390/curroncol28050324
APA StyleMartel-Lafay, I., Monnet, I., Lardy-Cleaud, A., Danhier, S., Salem, N., Gallocher, O., Fournel, P., Chouaid, C., Bylicki, O., & the GFPC 01-14 Investigators. (2021). Feasibility of Stereotactic Body Radiation Therapy on Unresectable Stage III NSCLC with Peripheral Primary Tumor: A Prospective Study (GFPC 01-14). Current Oncology, 28(5), 3804-3811. https://doi.org/10.3390/curroncol28050324