Adult Medulloblastoma Demographic, Tumor and Treatment Impact since 2006: A Canadian University Experience


 ,
,
Abstract
1. Introduction
2. Materials and Methods
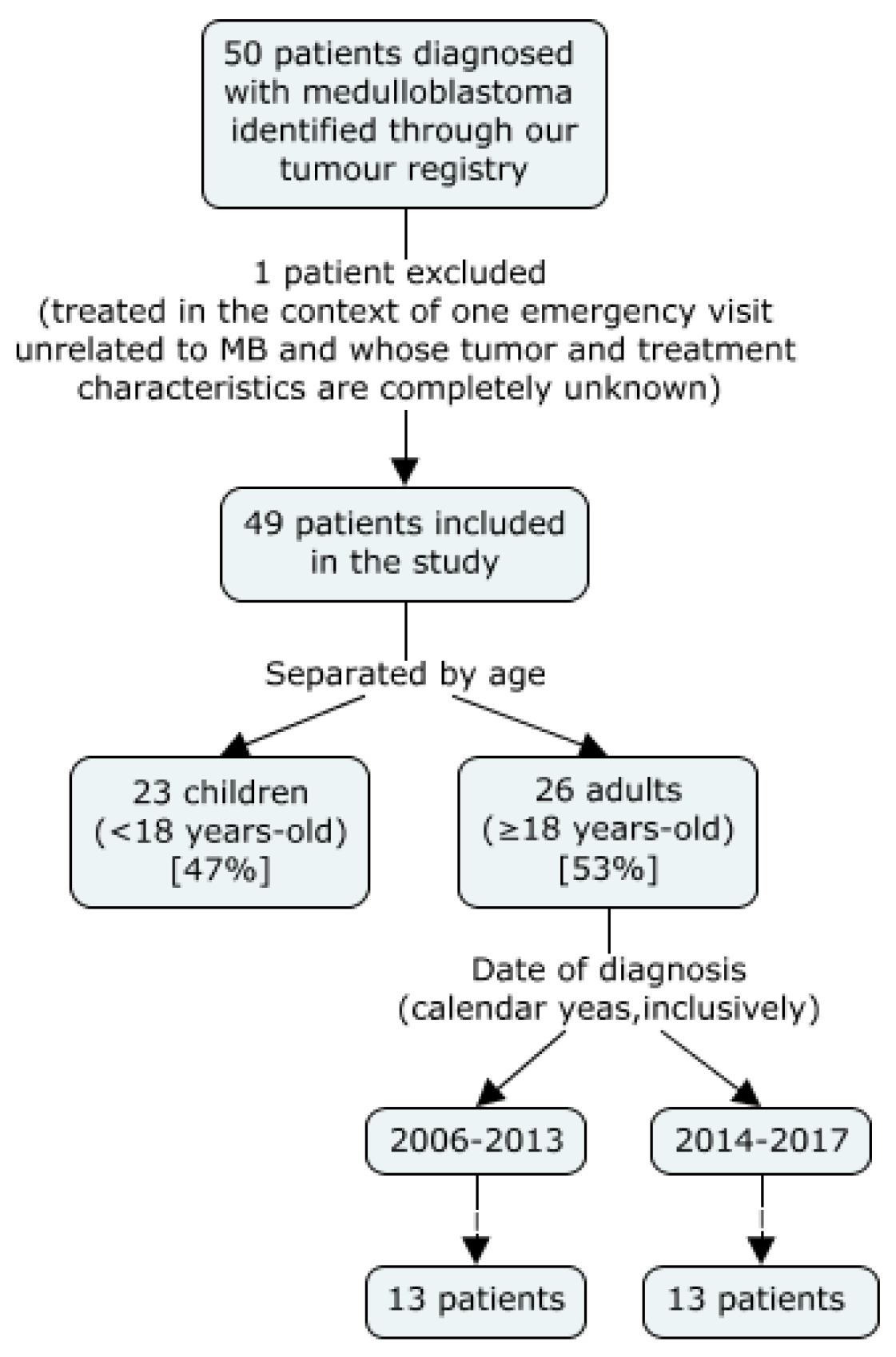
2.1. Data Source and Patient Selection
2.2. Patient Distribution
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Patient and Tumour Characteristics
3.2. Treatment Modalities
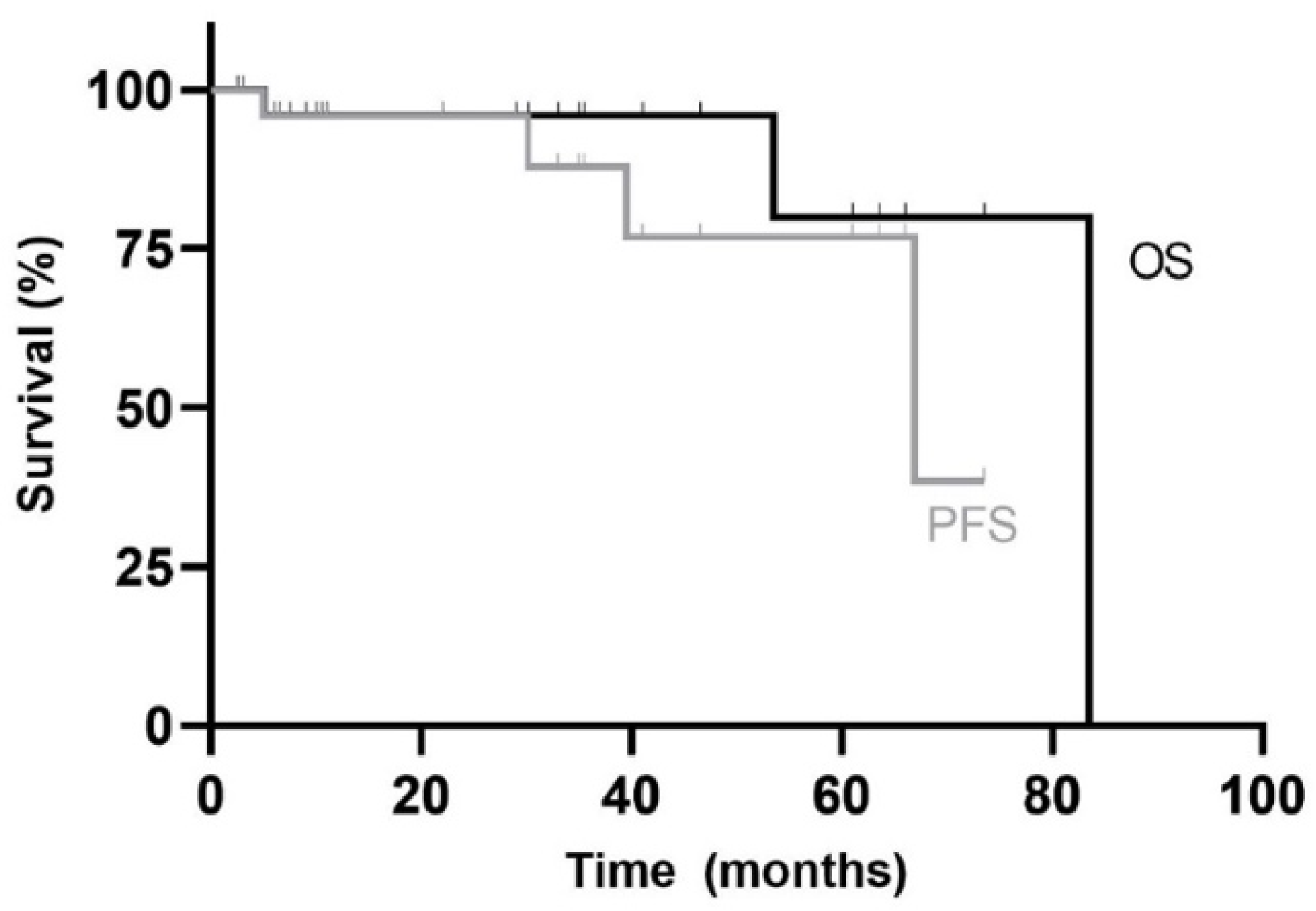
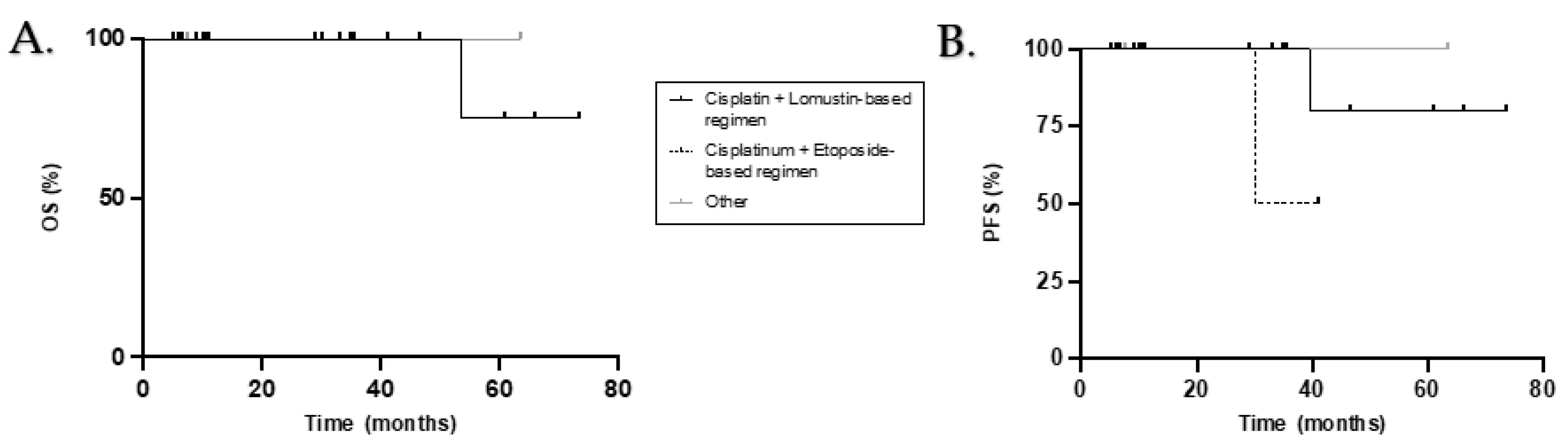
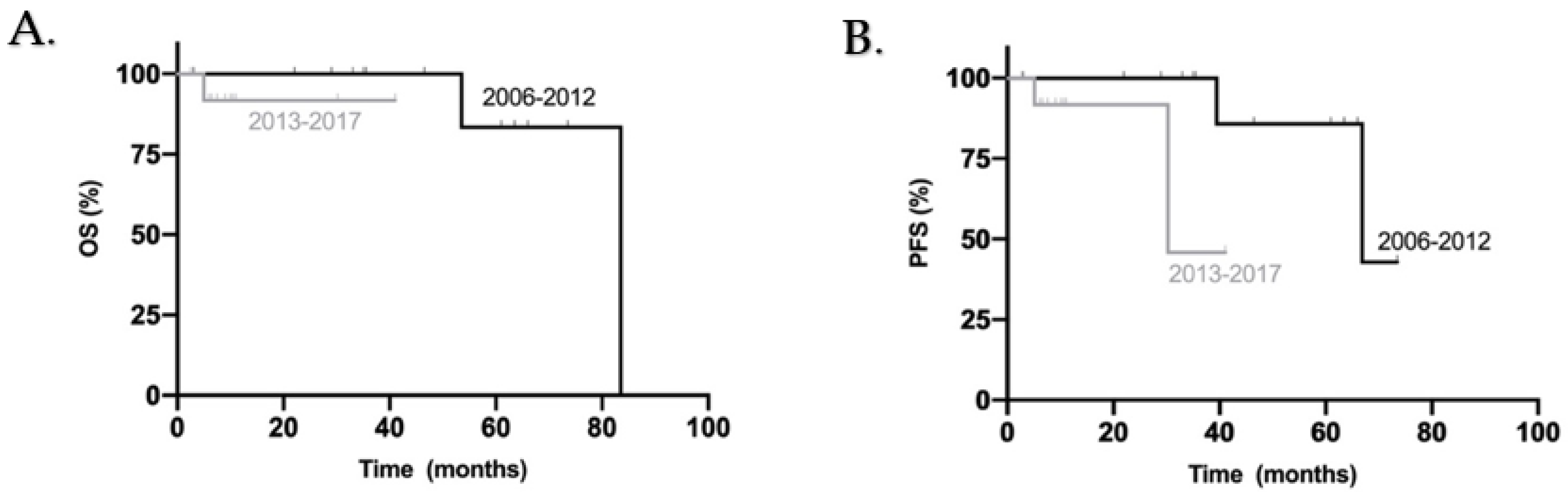
3.3. Survival
4. Discussion
4.1. Survival
4.2. Impact of Demographic and Tumour Factors
4.3. Role of the Different Treatment Variables
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abacioglu, U.; Uzel, O.; Sengoz, M.; Turkan, S.; Ober, A. Medulloblastoma in Adults: Treatment Results and Prognostic Factors. Int. J. Radiat. Oncol. 2002, 54, 855–860. [Google Scholar] [CrossRef]
- Brandes, A.A.; Paris, M.K. Review of the Prognostic Factors in Medulloblastoma of Children and Adults. Crit. Rev. Oncol. Hematol. 2004, 50, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Silvani, A.; Gaviani, P.; Lamperti, E.; Botturi, A.; Dimeco, F.; Franzini, A.; Ferroli, P.; Fariselli, L.; Milanesi, I.; Erbetta, A.; et al. Adult Medulloblastoma: Multiagent Chemotherapy with Cisplatinum and Etoposide: A Single Institutional Experience. J. Neuro-Oncol. 2012, 106, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Giordana, M.T.; Cavalla, P.; Dutto, A.; Borsotti, L.; Chiò, A.; Schiffer, D. Is Medulloblastoma the Same Tumor in Children and Adults? J. Neuro-Oncol. 1997, 35, 169–176. [Google Scholar] [CrossRef]
- Li, Q.; Dai, Z.; Cao, Y.; Wang, L. Comparing Children and Adults with Medulloblastoma: A SEER Based Analysis. Oncotarget 2018, 9, 30189–30198. [Google Scholar] [CrossRef]
- Zhao, F.; Ohgaki, H.; Xu, L.; Giangaspero, F.; Li, C.; Li, P.; Yang, Z.; Wang, B.; Wang, X.; Wang, Z.; et al. Molecular Subgroups of Adults Medulloblastoma: A Long-Term Single-Institution Study. Neuro-Oncology 2016, 18, 982–990. [Google Scholar] [CrossRef]
- Ang, C.; Hauerstock, D.; Guiot, M.C.; Kasumjanova, G.; Roberge, D.; Kavan, P.; Muanza, T. Characteristics and outcomes of medulloblastoma in adults. Pediatr. Blood Cancer 2008, 51, 603–607. [Google Scholar] [CrossRef]
- Carrie, C.; Lasset, C.; Alapetite, C.; Haie-Meder, C.; Hoffstetter, S.; Demaille, M.C.; Kerr, C.; Wagner, J.P.; Lagrange, J.L.; Maire, J.P. Multivariate Analysis of Prognostic Factors in Adult Patients with Medulloblastoma. Retrospective Study of 156 Patients. Cancer 1994, 74, 2352–2360. [Google Scholar] [CrossRef]
- Kool, M.; Korshunov, A.; Remke, M.; Jones, D.T.; Schlanstein, M.; Northcott, P.A.; Cho, Y.J.; Koster, J.; Schouten-van Meeteren, A.; van Vuurden, D.; et al. Molecular Subgroups of Medulloblastoma: An International Meta-Analysis of Transcriptome, Genetic Aberrations, and Clinical Data of WNT, SHH, Group 3, and Group 4 Medulloblastomas. Acta Neuropathol. 2012, 123, 473–484. [Google Scholar] [CrossRef]
- Atalar, B.; Ozsahin, M.; Call, J.; Napieralska, A.; Kamer, S.; Villa, S.; Erpolat, P.; Negretti, L.; Lassen-Ramshad, Y.; Onal, C.; et al. Treatment Outcome and Prognostic Factors for Adult Patients with Medulloblastoma: The Rare Cancer Network (RCN) Experience. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2018, 127, 96–102. [Google Scholar] [CrossRef]
- BKann, H.; Lester-Coll, N.H.; Park, H.S.; Yeboa, D.N.; Kelly, J.R.; Baehring, J.M.; Becker, K.P.; Yu, J.B.; Bindra, R.S.; Roberts, K.B. Adjuvant Chemotherapy and Overall Survival in Adult Medulloblastoma. Neuro-Oncology 2017, 19, 259–269. [Google Scholar]
- Chan, A.W.; Tarbell, N.J.; Black, P.M.; Louis, D.N.; Frosch, M.P.; Ancukiewicz, M.; Chapman, P.; Loeffler, J.S. Adult Medulloblastoma: Prognostic Factors and Patterns of Relapse. Neurosurgery 2000, 47, 623–632. [Google Scholar]
- Tait, D.M.; Thornton-Jones, H.; Bloom, H.J.; Lemerle, J.; Morris-Jones, P. Adjuvant Chemotherapy for Medulloblastoma: The First Multi-Centre Control Trial of the International Society of Paediatric Oncology (SIOP I). Eur. J. Cancer 1990, 26, 464–469. [Google Scholar] [CrossRef]
- Weil, M.D.; Lamborn, K.; Edwards, M.S.; Wara, W.M. Influence of a Child’s Sex on Medulloblastoma Outcome. JAMA 1998, 279, 1474–1476. [Google Scholar] [CrossRef][Green Version]
- Duffner, P.K.; Horowitz, M.E.; Krischer, J.P.; Friedman, H.S.; Burger, P.C.; Cohen, M.E.; Sanford, R.A.; Mulhern, R.K.; James, H.E.; Freeman, C.R. Postoperative Chemotherapy and Delayed Radiation in Children Less than Three Years of Age with Malignant Brain Tumors. N. Engl. J. Med. 1993, 328, 1725–1731. [Google Scholar] [CrossRef] [PubMed]
- Curran, E.K.; Le, G.M.; Sainani, K.L.; Propp, J.M.; Fisher, P.G. Do Children and Adults Differ in Survival from Medulloblastoma? A Study from the SEER Registry. J. Neuro-Oncol. 2009, 95, 81–85. [Google Scholar] [CrossRef] [PubMed]
- De, B.; Beal, K.; de Braganca, K.C.; Souweidane, M.M.; Dunkel, I.J.; Khakoo, Y.; Gilheeney, S.W.; DeAngelis, L.M.; Menzel, P.; Patel, S.H.; et al. Long-Term Outcomes of Adult Medulloblastoma Patients Treated with Radiotherapy. J. Neuro-Oncol. 2018, 136, 95–104. [Google Scholar] [CrossRef]
- Rutkowski, S.; von Hoff, K.; Emser, A.; Zwiener, I.; Pietsch, T.; Figarella-Branger, D.; Giangaspero, F.; Ellison, D.W.; Garre, M.L.; Biassoni, V.; et al. Survival and Prognostic Factors of Early Childhood Medulloblastoma: An International Meta-Analysis. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 4961–4968. [Google Scholar] [CrossRef]
- Kocakaya, S.; Beier, C.P.; Beier, D. Chemotherapy Increases Long-Term Survival in Patients with Adult Medulloblastoma—A Literature-Based Meta-Analysis. Neuro-Oncology 2016, 18, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Lai, R. Survival of Patients with Adult Medulloblastoma: A Population-Based Study. Cancer 2008, 18, 1568–1574. [Google Scholar] [CrossRef] [PubMed]
- Padovani, L.; Sunyach, M.P.; Perol, D.; Mercier, C.; Alapetite, C.; Haie-Meder, C.; Hoffstetter, S.; Muracciole, X.; Kerr, C.; Wagner, J.P.; et al. Common Strategy for Adult and Pediatric Medulloblastoma: A Multicenter Series of 253 Adults. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 433–440. [Google Scholar] [CrossRef]
- Northcott, P.A.; Jones, D.T.; Kool, M.; Robinson, G.W.; Gilbertson, R.J.; Cho, Y.J.; Pomeroy, S.L.; Korshunov, A.; Lichter, P.; Taylor, M.D.; et al. Medulloblastomics: The End of the Beginning. Nat. Rev. Cancer 2012, 12, 818–834. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, E.; Hofer, S.; Brandes, A.A.; Frappaz, D.; Kortmann, R.D.; Bromberg, J.; Dangouloff-Ros, V.; Boddaert, N.; Hattingen, E.; Wiestler, B.; et al. EANO-EURACAN Clinical Practice Guideline for Diagnosis, Treatment, and Follow-Up of Post-Pubertal and Adult Patients with Medulloblastoma. Lancet Oncol. 2019, 20, e715–e728. [Google Scholar] [CrossRef]
- Khalil, E.M. Treatment Results of Adults and Children with Medulloblastoma NCI, Cairo University Experience. J. Egypt. Natl. Cancer Inst. 2008, 20, 175–186. [Google Scholar]
- Packer, R.J.; Gajjar, A.; Vezina, G.; Rorke-Adams, L.; Burger, P.C.; Robertson, P.L.; Bayer, L.; LaFond, D.; Donahue, B.R.; Marymont, M.H.; et al. Phase III Study of Craniospinal Radiation Therapy Followed by Adjuvant Chemotherapy for Newly Diagnosed Average-Risk Medulloblastoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2006, 24, 4202–4208. [Google Scholar] [CrossRef]
- Packer, R.J.; Pfister, S.M. Medulloblastoma. In Encyclopedia of Neuroscience; Squire, L.R., Ed.; Academic Press: Cambridge, MA, USA, 2009; pp. 703–711. [Google Scholar]
- Selek, U.; Zorlu, F.; Hurmuz, P.; Cengiz, M.; Turker, A.; Soylemezoglu, F.; Gurkaynak, M. Craniospinal Radiotherapy in Adult Medulloblastoma. Strahlenther. Onkol. Organ. Dtsch. Rontgenges. 2007, 183, 236–240. [Google Scholar] [CrossRef]
- Greenberg, H.S.; Chamberlain, M.C.; Glantz, M.J.; Wang, S. Adult Medulloblastoma: Multiagent Chemotherapy. Neuro-Oncology 2001, 31, 29–34. [Google Scholar] [CrossRef]
- Call, J.A.; Naik, M.; Rodriguez, F.J.; Giannini, C.; Wu, W.; Buckner, J.C.; IParney, F.; Laack, N.N. Long-Term Outcomes and Role of Chemotherapy in Adults with Newly Diagnosed Medulloblastoma. Am. J. Clin. Oncol. 2014, 37, 1–7. [Google Scholar] [CrossRef]
- Franceschi, E.; Bartolotti, M.; Paccapelo, A.; Marucci, G.; Agati, R.; Volpin, L.; Danieli, D.; Ghimenton, C.; Gardiman, M.P.; Sturiale, C.; et al. Adjuvant Chemotherapy in Adult Medulloblastoma: Is it an Option for Average-Risk Patients? J. Neuro-Oncol. 2016, 128, 235–240. [Google Scholar] [CrossRef]
- Herlinger, U.; Steinbrecher, A.; Rieger, J.; Hau, P.; Kortmann, R.D.; Meyermann, R.; Schabet, M.; Bamberg, M.; Dichgans, J.; Bogdahn, U.; et al. Adult Medulloblastoma: Prognostic Factors and Response to Therapy at Diagnosis and at Relapse. J. Neurol. 2005, 252, 291–299. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Participants N = 49 (%) | Adults N = 26 (%) | Children N = 23 (%) | ||
|---|---|---|---|---|
| Demographic Characteristics | ||||
| Median Age in Years (range) | 19 (0–53) | 29 (18–53) | 7 (0–16) | |
| Sex | Male | 36 (73) | 19 (73) | 17 (74) |
| Female | 13 (27) | 7 (27) | 6 (26) | |
| Family history of CNS cancer | Yes | - | - | - |
| No | 15 (31) | 15 (58) | - | |
| Unknown | 34 (69) | 11 (42) | 23 (100) | |
| Comorbidities | Yes | 4 (8) | 4 (15) | - |
| No | 45 (92) | 22 (85) | 23 (100) | |
| Tumor Characteristics | ||||
| Histopathology | Classic (CMB) | 26 (53) | 11 (42) | 15 (65) |
| Desmoplastic/nodular (DNMB) | 16 (33) | 12 (46) | 4 (17) | |
| Large cell/anaplastic (LCAMB) | 7 (14) | 3 (12) | 4 (17) | |
| Molecular Subgroup * | SHH-activated (SHH-MB) | 13 (27) | 10 (39) | 3 (13) |
| SHH- activated: TP53-mutant | 1 (2) | - | 1 (4) | |
| SHH activated: TP53-wildtype | 12 (25) | 10 (39) | 2 (9) | |
| Non-WNT/non-SHH ** | 25 (51) | 11 (42) | 14 (61) | |
| Unknown | 11 (22) | 5 (19) | 6 (26) | |
| Stage at Diagnosis *** | M0 | 30 (61) | 14 (54) | 16 (70) |
| M2 | 3 (6) | 1 (4) | 2 (9) | |
| M3 | 3 (6) | - | 3 (13) | |
| Unknown | 13 (27) | 11 (42) | 2 (9) | |
| Cerebral Spinal Fluid (CSF) at Diagnosis | Positive | 1 (2) | 1 (4) | - |
| Negative | 11 (22) | 6 (23) | 5 (22) | |
| Unknown | 37 (76) | 19 (73) | 18 (78) | |
| Tumor Location | Cerebellum | 40 (82) | 23 (88) | 17 (74) |
| Brainstem | 9 (18) | 3 (12) | 6 (26) | |
| Treatment Characteristics | ||||
| Surgical macroscopic resection | Complete | 43 (88) | 22 (85) | 21 (91) |
| Partial | 6 (12) | 4 (15) | 2 (9) | |
| Radiotherapy | None | 1 (2) | 1 (4) | - |
| Alone | 25 (51) | 13 (50) | 12 (52) | |
| With concomitant chemotherapy | 23 (47) | 12 (46) | 11 (48) | |
| Adjuvant Chemotherapy | Yes | 22 (45) | 21 (81) | 1 (4) |
| No | 5 (10) | 5 (19) | - | |
| Unknown **** | 22 (45) | - | 22 (96) | |
| All Adults N = 26 (%) | 2006–2012 N = 13 (%) | 2013–2017 N = 13 (%) | ||
|---|---|---|---|---|
| Demographic and Tumour Characteristics | ||||
| Median Age in Years (range) | 29 (18–53) | 28 (20–53) | 31 (18–51) | |
| Sex | Male | 19 (73) | 10 (77) | 9 (69) |
| Female | 7 (27) | 3 (23) | 4 (31) | |
| Histopathology | Classic (CMB) | 11 (42) | 8 (61.5) | 3 (23.5) |
| Desmoplastic/nodular (DNMB) | 12 (46) | 4 (31) | 8 (61.5) | |
| Large cell/anaplastic (LCAMB) | 3 (12) | 1 (7.5) | 2 (15) | |
| Molecular Subgroup | SHH-activated * | 10 (39) | - | 10 (77) |
| Non-WNT/non-SHH | 11 (42) | 9 (69) | 2 (15) | |
| Unknown | 5 (19) | 4 (31) | 1 (7.5) | |
| Stage at Diagnosis | M0 | 14 (54) | 5 (38.5) | 9 (69) |
| M2 | 1 (4) | - | 1 (7.5) | |
| Unknown | 11 (42) | 8 (61.5) | 3 (23) | |
| Treatment Variables | ||||
| Surgical Macroscopic resection | Complete | 22 (85) | 11 (85) | 11 (85) |
| Partial | 4 (15) | 2 (15) | 2 (15) | |
| Radiotherapy | None | 1 (4) | - | 1 (7.5) |
| Alone | 13 (50) | 2 (15) | 11 (85) | |
| With induction/concomitant chemotherapy | 12 (46) | 11 (85) | 1 (7.5) | |
| First Intention Maintenance Chemotherapy | None | 5 (19) | 3 (23.5) | 2 (15) |
| Cisplatinum + Lomustine-based regimen | 9 (43) | 9 (69) | - | |
| Cisplatinum + Lomustine ** | 1 (5) | 1 (7.5) | - | |
| Cisplatinum + Lomustine + Vincristine | 8 (38) | 8 (61.5) | - | |
| Cisplatinum + Etoposide-based regimen | 10 (48) | - | 10 (76.5) | |
| Cisplatinum + Etoposide | 1 (5) | - | 1 (7.5) | |
| Cisplatinum + Etoposide + Cyclophosphamide | 9 (43) | - | 9 (69) | |
| Other | 2 (10) | 1 (7.5) | 1 (7.5) | |
| Temozolomide | 1 (5) | 1 (7.5) | - | |
| Vincristine + Cisplatinum + Cyclophosphamide alternating with Premetrexed and Gemcitabine | 1 (5) | - | 1 (7.5) | |
| No. of Pts n = 26 | 5yOS (%) | p-Value | 5yPFS (%) | p-Value | ||
|---|---|---|---|---|---|---|
| Demographic and Tumour Characteristics | ||||||
| Sex | Male | 19 | 75 | 0.515 | 75 | 0.642 |
| Female | 7 | 83.3 | 83.3 | |||
| Histopathology | Classic (CMB) | 11 | 100 | 0.368 | 100 | 0.162 |
| Desmoplastic/nodular (DNMB) | 12 | 61.1 | 68.8 | |||
| Large cell/anaplastic (LCAMB) | 3 | 100 | 100 | |||
| Molecular Subgroup | SHH-activated | 10 | NR | 0.412 | NR | 0.148 |
| Non-WNT/non-SHH | 11 | 80 | 80 | |||
| Unknown | 5 | NR | NR | |||
| Stage at Diagnosis | M0 | 14 | 92.3 | 0.889 | 73.8 | 0.496 |
| M2 | 1 | NR | NR | |||
| Unknown | 11 | 80 | 80 | |||
| Treatment Variables | ||||||
| Surgical Macroscopic Resection | Complete | 22 | 79.2 | 0.655 | 74.8 | 0.527 |
| Partial | 4 | NR | NR | |||
| Radiotherapy | Alone | 13 | 50 | 0.157 | 50 | 0.033 |
| With induction/concomitant chemotherapy | 12 | 100 | 100 | |||
| Adjuvant Chemotherapy | Yes | 21 | 80 | 0.155 | 77.9 | 0.114 |
| No | 5 | 66.7 | 66.7 | |||
| Type of Adjuvant Chemotherapy (First Intention) | Cisplatinum + Lomustine-based regimen | 9 | 75 | - | 80 | 0.410 |
| Cisplatinum + Etoposide-based regimen | 10 | NR | NR | |||
| Other | 2 | NR | NR | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quinones, M.C.; Bélanger, K.; Lemieux Blanchard, É.; Lemieux, B.; Bahary, J.-P.; Masucci, L.G.; Roberge, D.; Menard, C.; Lambert, C.; Berthelet, F.; et al. Adult Medulloblastoma Demographic, Tumor and Treatment Impact since 2006: A Canadian University Experience. Curr. Oncol. 2021, 28, 3104-3114. https://doi.org/10.3390/curroncol28040271
Quinones MC, Bélanger K, Lemieux Blanchard É, Lemieux B, Bahary J-P, Masucci LG, Roberge D, Menard C, Lambert C, Berthelet F, et al. Adult Medulloblastoma Demographic, Tumor and Treatment Impact since 2006: A Canadian University Experience. Current Oncology. 2021; 28(4):3104-3114. https://doi.org/10.3390/curroncol28040271
Chicago/Turabian StyleQuinones, Maria Camila, Karl Bélanger, Émilie Lemieux Blanchard, Bernard Lemieux, Jean-Paul Bahary, Laura G. Masucci, David Roberge, Cynthia Menard, Carole Lambert, France Berthelet, and et al. 2021. "Adult Medulloblastoma Demographic, Tumor and Treatment Impact since 2006: A Canadian University Experience" Current Oncology 28, no. 4: 3104-3114. https://doi.org/10.3390/curroncol28040271
APA StyleQuinones, M. C., Bélanger, K., Lemieux Blanchard, É., Lemieux, B., Bahary, J.-P., Masucci, L. G., Roberge, D., Menard, C., Lambert, C., Berthelet, F., Moumdjian, R., & Florescu, M. (2021). Adult Medulloblastoma Demographic, Tumor and Treatment Impact since 2006: A Canadian University Experience. Current Oncology, 28(4), 3104-3114. https://doi.org/10.3390/curroncol28040271