Evaluation of Adjuvant Chemotherapy-Associated Steatosis (CAS) in Colorectal Cancer

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
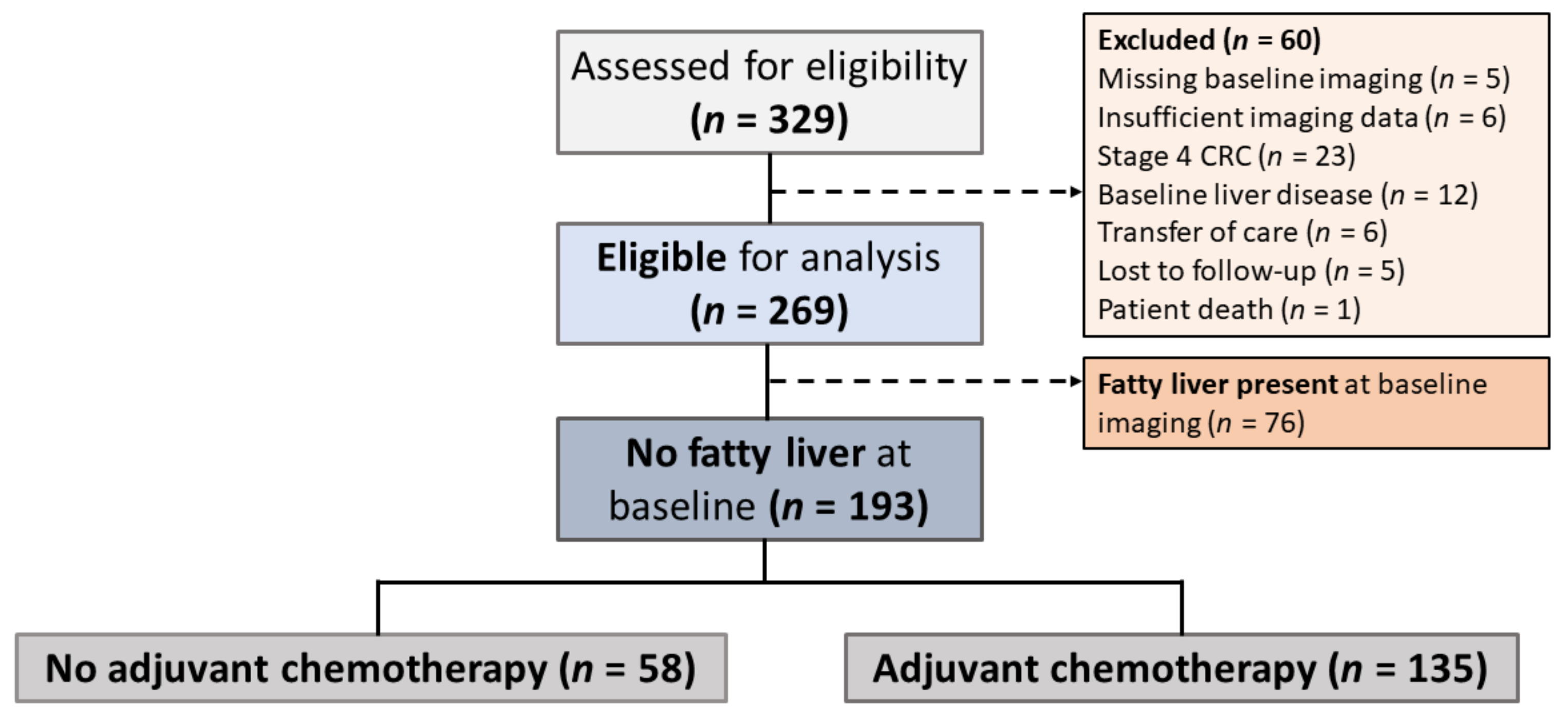
2.1. Patients and Data Collection
2.2. Determination of CAS Status
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haas, J.T.; Francque, S.; Staels, B. Pathophysiology and mechanisms of nonalcoholic fatty liver disease. Annu. Rev. Physiol. 2016, 78, 181–205. [Google Scholar] [CrossRef]
- Canadian Liver Foundation 2017 [cited 2020 May 24]. Fatty Liver Disease. Available online: https://www.liver.ca/patients-caregivers/liver-diseases/fatty-liver-disease/ (accessed on 24 May 2020).
- Goldberg, D.; Ditah, I.C.; Saeian, K.; Lalehzari, M.; Aronsohn, A.; Gorospe, E.C.; Charlton, M. Changes in the Prevalence of hepatitis C virus infection, nonalcoholic steatohepatitis, and alcoholic liver disease among patients with cirrhosis or liver failure on the waitlist for liver transplantation. Gastroenterology 2017, 152, 1090–1099. [Google Scholar] [CrossRef] [PubMed]
- Mittal, S.; El-Serag, H.B.; Sada, Y.H.; Kanwal, F.; Duan, Z.; Temple, S.; May, S.B.; Kramer, J.R.; Richardson, P.A.; Davila, J.A. Hepatocellular carcinoma in the absence of cirrhosis in united states veterans is associated with nonalcoholic fatty liver disease. Clin. Gastroenterol. Hepatol. 2016, 14, 124–131.e1. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.L.; Neuschwander-Tetri, B.A.; Rinella, M.; Sanyal, A.J. Mechanisms of NAFLD development and therapeutic strategies. Nat. Med. 2018, 24, 908–922. [Google Scholar] [CrossRef]
- Grieco, A.; Forgione, A.; Miele, L.; Greco, A.V.; Gasbarrini, A.; Gasbarrini, G. Fatty liver and drugs. Eur. Rev. Med. Pharmacol. Sci. 2005, 9, 261–263. [Google Scholar]
- Meunier, L.; Larrey, D. Chemotherapy-associated steatohepatitis. Ann. Hepatol. 2020, 19, 597–601. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.I.; Lee, H.W.; Lee, K.S.; Lee, H.S.; Park, J.Y. Effects of Statin Use on the Development and Progression of Nonalcoholic Fatty Liver Disease: A Nationwide Nested Case-Control Study. Am. J. Gastroenterol. 2021, 116, 116–124. [Google Scholar] [CrossRef]
- Canadian Cancer Society’s Advisory Committee on Cancer Statistics. Canadian Cancer Statistics 2017; Canadian Cancer Society: Toronto, ON, Canada, 2017; Available online: https://www.cancer.ca/~/media/cancer.ca/CW/cancer%20information/cancer%20101/Canadian%20cancer%20statistics/Canadian-Cancer-Statistics-2017-EN.pdf (accessed on 24 May 2020).
- André, T.; Boni, C.; Mounedji-Boudiaf, L.; Navarro, M.; Tabernero, J.; Hickish, T.; Topham, C.; Zaninelli, M.; Clingan, P.; Bridgewater, J.; et al. Oxaliplatin, Fluorouracil, and Leucovorin as Adjuvant Treatment for Colon Cancer. N. Engl. J. Med. 2004, 350, 2343–2351. [Google Scholar] [CrossRef]
- André, T.; Boni, C.; Navarro, M.; Tabernero, J.; Hickish, T.; Topham, C.; Bonetti, A.; Clingan, P.; Bridgewater, J.; Rivera, F.; et al. Improved overall survival with oxaliplatin, fluorouracil, and leucovorin and adjuvant treatment in stage II and III colon cancer in the MOSAIC trial. J. Clin. Oncol. 2009, 27, 3109–3116. [Google Scholar] [CrossRef]
- Twelves, C.; Scheithauer, W.; McKendrick, J.; Seitz, J.F.; Van Hazel, G.; Wong, A.; Diaz-Rubio, E.; Gilberg, F.; Cassidy, J. Capecitabine versus 5-fluorouracil/folinic acid as adjuvant therapy for stage III colon cancer: Final results from the X-ACT trial with analysis by age and preliminary evidence of a pharmacodynamic marker of efficacy. Ann. Oncol. 2012, 23, 1190–1197. [Google Scholar] [CrossRef]
- Miyake, K.; Hayakawa, K.; Nishino, M.; Morimoto, T.; Mukaihara, S. Effects of oral 5-fluorouracil drugs on hepatic fat content in patients with colon cancer. Acad. Radiol. 2005, 12, 722–727. [Google Scholar] [CrossRef]
- Peppercorn, P.; Reznek, R.; Wilzon, P.; Slevin, M.L.; Gupta, R.K. Demonstration of hepatic steatosis by computerized tomography in patients receiving 5-fluorouracil-based therapy for advanced colorectal cancer. Br. J. Cancer 1998, 77, 2008–2011. [Google Scholar] [CrossRef]
- Alpern, M.B.; Lawson, T.L.; Foley, W.D.; Perlman, S.J.; Reif, L.J.; Arevalos, E.; Rimm, A.A. Focal hepatic masses and fatty infiltration detected by enhanced dynamic CT. Radiology 1986, 158, 45–49. [Google Scholar] [CrossRef]
- Rofsky, N.M.; Fleishaker, H. CT and MRI of diffuse liver disease. Semin. Ultrasound CT MR 1995, 16, 16–33. [Google Scholar] [CrossRef]
- Joy, D.; Thava, V.R.; Scott, B.B. Diagnosis of fatty liver disease: Is biopsy necessary? Eur. J. Gastroenterol. Hepatol. 2003, 15, 539–543. [Google Scholar]
- Kreft, B.P.; Tanimoto, A.; Baba, Y.; Zhao, L.; Chen, J.; Middleton, M.S.; Compton, C.C.; Finn, J.P.; Stark, D.D. Diagnosis of fatty liver with MR imaging. J. Magn. Reson. Imaging 1992, 2, 463–471. [Google Scholar] [CrossRef]
- Ballestri, S.; Nascimbeni, F.; Baldelli, E.; Marrazzo, A.; Romagnoli, D.; Lonardo, A. NAFLD as a Sexual Dimorphic Disease: Role of Gender and Reproductive Status in the Development and Progression of Nonalcoholic Fatty Liver Disease and Inherent Cardiovascular Risk. Adv. Ther. 2017, 34, 1291–1326. [Google Scholar] [CrossRef]
- Fan, R.; Wang, J.; Du, J. Association between body mass index and fatty liver risk: A dose-response analysis. Sci. Rep. 2018, 8, 15273. [Google Scholar] [CrossRef]
- Woods, C.P.; Hazlehurst, J.M.; Tomlinson, J.W. Glucocorticoids and non-alcoholic fatty liver disease. J. Steroid Biochem. Mol. Biol. 2015, 154, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Garvey, W.T.; Mechanick, J.I.; Brett, E.M.; Garber, A.J.; Hurley, D.L.; Jastreboff, A.M.; Nadolsky, K.; Pessah-Pollack, R.; Plodkowski, R. Reviewers of the AACE/ACE Obesity Clinical Practice Guidelines. American Association of Clinical Endocrinologists and American College of Endocrinology Comprehensive Clinical Practice Guidelines for Medical Care of Patients with Obesity. Endocr. Pract. 2016, 22 (Suppl. 3), 1–203. [Google Scholar] [CrossRef] [PubMed]
- Moertel, C.; Fleming, T.; Macdonald, J.; Haller, D.G.; Laurie, J.A. Hepatic toxicity associated with fluorouracil plus levamisole adjuvant therapy. J. Clin. Oncol. 1993, 11, 2386–2390. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, P.; Edal, A.; Madsen, E.; Fenger, C.; Poulsen, M.R.; Petersen, O.F. Reversible hepatic steatosis in patients treated with interferon alfa-2A and 5-fluorouracil. Cancer 1995, 75, 2592–2596. [Google Scholar] [CrossRef]
- Vigano, L.; De Rosa, G.; Toso, C.; Andres, A.; Ferrero, A.; Roth, A.; Sperti, E.; Majno, P.; Rubbia-Brandt, L. Reversibility of chemotherapy-related liver injury. J. Hepatol. 2017, 67, 10–11. [Google Scholar] [CrossRef]
- Schumacher, J.D.; Guo, G.L. Mechanistic review of drug-induced steatohepatitis. Toxicol. Appl. Pharmacol. 2015, 289, 40–47. [Google Scholar] [CrossRef]
- Lu, Y.; Lin, Y.; Huang, X.; Wu, S.; Wei, J.; Yang, C. Oxaliplatin aggravates hepatic oxidative stress, inflammation and fibrosis in a non-alcoholic fatty liver disease mouse model. Int. J. Mol. Med. 2019, 43, 2398–2408. [Google Scholar] [CrossRef]
- Gangi, A.; Lu, S.C. Chemotherapy-associated liver injury in colorectal cancer. Therap. Adv. Gastroenterol. 2020, 13, 1756284820924194. [Google Scholar] [CrossRef]
- Miwa, M.; Ura, M.; Nishida, M.; Sawada, N.; Ishikawa, T.; Mori, K.; Shimma, N.; Umeda, I.; Ishitsuka, H. Design of a novel oral fluoropyrimidine carbamate, capecitabine, which generates 5-fluorouracil selectively in tumours by enzymes concentrated in human liver and cancer tissue. Eur. J. Cancer 1998, 34, 1274–1281. [Google Scholar] [CrossRef]
- Saif, M.W.; Katirtzoglou, N.A.; Syrigos, K.N. Capecitabine: An overview of the side effects and their management. Anticancer Drugs 2008, 19, 447–464. [Google Scholar] [CrossRef]
- Habib, M.B.; Hanafi, I.; Al Zoubi, M.; Bdeir, Z.; Yassin, M.A. Severe and Late Acute Liver Injury Induced by Capecitabine. Cureus 2021, 13, e12477. [Google Scholar] [PubMed]
- Chin, S.N.; Kim, T.K.; Siu, L.L. Hepatic steatosis secondary to capecitabine: A case report. J. Med. Case Rep. 2010, 4, 227. [Google Scholar] [CrossRef][Green Version]
- Piscaglia, F.; Svegliati-Baroni, G.; Barchetti, A.; Pecorelli, A.; Marinelli, S.; Tiribelli, C.; Bellentani, S. HCC-NADFL Italian Study Group. Clinical patterns of hepatocellular carcinoma in nonalcoholic fatty liver disease: A multicenter prospective study. Hepatology 2016, 63, 827–838. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012, 55, 2005–2023. [Google Scholar] [CrossRef] [PubMed]
- Alkhouri, N. NASH and NAFLD: Emerging drugs, therapeutic targets and translational and clinical challenges. Expert Opin. Investig. Drugs 2020, 29, 87. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- Katsiki, N.; Mikhailidis, D.; Mantzoros, C. Non-alcoholic fatty liver disease and dyslipidemia: An update. Metabolism 2016, 65, 1109–1123. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, J.; Cobbe, S.; Ford, I.; Isles, C.G.; Lorimer, A.R.; MacFarlane, P.W.; McKillop, J.H.; Packard, C.J. Prevention of coronary heart diseases with pravastatin in men with hypercholesterolemia: West of Scotland coronary prevention study group. N. Engl. J. Med. 1995, 333, 1301–1307. [Google Scholar] [CrossRef]
- Doumas, M.; Imprialos, K.; Dimakopoulou, A.; Stavropoulos, K.; Binas, A.; Athyros, V.G. The role of statins in the management of nonalcoholic fatty liver disease. Curr. Pharm. Des. 2018, 24, 4587–4592. [Google Scholar] [CrossRef] [PubMed]
- Sigler, M.A.; Congdon, L.; Edwards, K.L. An evidence-based review of statin use in patients with nonalcoholic fatty liver disease. Clin. Med. Insights Gastroenterol. 2018, 11, 1179552218787502. [Google Scholar] [CrossRef]
- Pastori, D.; Polimeni, L.; Baratta, F.; Pani, A.; Del Ben, M.; Angelico, F. The efficacy and safety of statins for the treatment of non-alcoholic fatty liver disease. Dig. Liver Dis. 2015, 47, 4–11. [Google Scholar] [CrossRef]
- Li, Q.; Dhyani, M.; Grajo, J.R.; Sirlin, C.; Samir, A.E. Current status of imaging in nonalcoholic fatty liver disease. World J. Hepatol. 2018, 10, 530–542. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, D.A.; Oliva, I.B.; Israel, G.M. Detection of hepatic steatosis on contrast-enhanced CT images: Diagnostic accuracy of identification of areas of presumed focal fatty sparing. AJR Am. J. Roentgenol. 2012, 199, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Obika, M.; Noguchi, H. Diagnosis and evaluation of nonalcoholic fatty liver disease. Exp. Diabetes Res. 2012, 2012, 145754. [Google Scholar] [CrossRef] [PubMed]
- Browning, J.D.; Szczepaniak, L.S.; Dobbins, R.; Nuremberg, P.; Horton, J.D.; Cohen, J.C.; Grundy, S.M.; Hobbs, H.H. Prevalence of hepatic steatosis in an urban population in the United States: Impact of ethnicity. Hepatology 2004, 40, 1387–1395. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| No Adjuvant Chemotherapy | Adjuvant Chemotherapy | |
|---|---|---|
| n = 58 | n = 135 | |
| Sex, Male | 24 (41.4%) | 81 (60.0%) |
| Age at diagnosis, years (mean ± SD) | 68.0 ± 14.1 | 59.9 ± 11.4 |
| ≤55 | 11 (19.0%) | 50 (37.0%) |
| 56–69 | 20 (34.5%) | 57 (42.2%) |
| ≥70 | 27 (46.6%) | 28 (20.7%) |
| BMI (kg/m2) | ||
| Underweight (<18.5) | 0 (0.0%) | 4 (3.0%) |
| Normal Weight (18.5–24.9) | 18 (31.0%) | 65 (48.2%) |
| Overweight (25–29.9) | 19 (32.8%) | 48 (35.6%) |
| Obese (≥30) | 7 (12.1%) | 15 (11.1%) |
| Missing | 14 (24.1%) | 3 (2.2%) |
| Type 2 Diabetes | 11 (19.0%) | 18 (13.3%) |
| Hyperlipidemia | 25 (43.1%) | 39 (28.9%) |
| Hypertension | 30 (51.7%) | 52 (38.5%) |
| Tumour location | ||
| Right colon (ascending, transverse) | 36 (62.1%) | 32 (23.7%) |
| Left colon (descending, sigmoid) | 16 (27.6%) | 32 (23.7%) |
| Rectum | 6 (10.3%) | 61 (45.2%) |
| Multiple locations | 0 (0.0%) | 10 (7.4%) |
| Primary surgical resection | 55 (94.8%) | 134 (99.3%) |
| Pelvic radiation | 6 (10.3%) | 52 (38.5%) |
| Steroid use | 8 (13.8%) | 9 (6.7%) |
| Statin use | 21 (36.2%) | 37 (27.4%) |
| Atorvastatin | 13 (61.9%) | 19 (55.9%) |
| Pravastatin | 2 (9.5%) | 1 (2.9%) |
| Rosuvastatin | 2 (9.5%) | 7 (20.6%) |
| Simvastatin | 4 (19.1%) | 7 (20.6%) |
| Alcohol consumption a | ||
| None | 27 (46.6%) | 73 (54.1%) |
| Moderate | 27 (46.6%) | 55 (40.7%) |
| Frequent | 4 (6.9%) | 7 (5.2%) |
| Developed Steatosis | No Steatosis | Crude Relative Risk | Adjusted a Relative Risk (95% CI) | p-Value | |
|---|---|---|---|---|---|
| Adjuvant Chemotherapy | 52 (38.5%) | 83 (61.5%) | 1.60 | 1.57 (0.89–2.79) | 0.12 |
| No Adjuvant Chemotherapy (Ref) | 14 (24.1%) | 44 (75.9%) | 1.00 | 1.00 |
| Developed Steatosis | No Steatosis | Crude Relative Risk | Adjusted a Relative Risk (95% CI) | p-Value | |
|---|---|---|---|---|---|
| Oxaliplatin | 36 (35.0%) | 67 (65.1%) | 0.70 | 0.64 (0.30–1.38) | 0.26 |
| Non-Oxaliplatin (Ref) | 16 (50.0%) | 16 (50.0%) | 1.00 | 1.00 |
| Developed Steatosis | No Steatosis | Crude Relative Risk | Adjusted a Relative Risk (95% CI) | p-Value | |
|---|---|---|---|---|---|
| Capecitabine | 14 (48.3%) | 15 (51.7%) | 1.35 | 1.56 (0.65–3.73) | 0.32 |
| Intravenous regimens b (Ref) | 38 (35.9%) | 68 (64.2%) | 1.00 | 1.00 |
| No Statin Administration | Statin Administration | |
|---|---|---|
| n = 98 | n = 37 | |
| Sex, Male | 55 (56.1%) | 26 (70.3%) |
| BMI (kg/m2) | ||
| Underweight (<18.5) | 3 (3.1%) | 1 (2.7%) |
| Normal Weight (18.5–24.9) | 49 (50.0%) | 16 (43.2%) |
| Overweight (25–29.9) | 32 (32.7%) | 16 (43.2%) |
| Obese (≥30) | 11 (11.2%) | 4 (10.8%) |
| Missing | 3 (3.1%) | 0 (0.0%) |
| Comorbitities | ||
| Type 2 Diabetes | 7 (7.1%) | 11 (29.7%) |
| Hyperlipidemia | 2 (2.0%) | 37 (100.0%) |
| Hypertension | 25 (25.5%) | 27 (73.0%) |
| Treatment | ||
| Pelvic radiation | 38 (38.8%) | 14 (37.8%) |
| Steroid use | 7 (7.1%) | 2 (5.4%) |
| Adjuvant chemotherapy characteristics | ||
| Duration of adjuvant chemotherapy, cycles a (mean ± SD) | 8.7 ± 2.7 | 8.0 ± 2.8 |
| Type of adjuvant chemotherapy received | ||
| FOLFOX | 84 (85.7%) | 19 (51.4%) |
| Capecitabine | 14 (14.3%) | 15 (40.5%) |
| FUFA | 0 (0.0%) | 3 (8.1%) |
| Developed Steatosis | No Steatosis | Crude Relative Risk | Adjusted a Relative Risk (95% CI) | p-Value | |
|---|---|---|---|---|---|
| Statin use | 11 (29.7%) | 26 (70.3%) | 0.71 | 0.53 (0.10–2.75) | 0.45 |
| No statin use (Ref) | 41 (41.8%) | 57 (58.2%) | 1.00 | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, M.C.M.; Kachura, J.J.; Vlachou, P.A.; Dzulynsky, R.; Di Tomaso, A.; Samawi, H.; Baxter, N.; Brezden-Masley, C. Evaluation of Adjuvant Chemotherapy-Associated Steatosis (CAS) in Colorectal Cancer. Curr. Oncol. 2021, 28, 3030-3040. https://doi.org/10.3390/curroncol28040265
Lee MCM, Kachura JJ, Vlachou PA, Dzulynsky R, Di Tomaso A, Samawi H, Baxter N, Brezden-Masley C. Evaluation of Adjuvant Chemotherapy-Associated Steatosis (CAS) in Colorectal Cancer. Current Oncology. 2021; 28(4):3030-3040. https://doi.org/10.3390/curroncol28040265
Chicago/Turabian StyleLee, Michelle C. M., Jacob J. Kachura, Paraskevi A. Vlachou, Raissa Dzulynsky, Amy Di Tomaso, Haider Samawi, Nancy Baxter, and Christine Brezden-Masley. 2021. "Evaluation of Adjuvant Chemotherapy-Associated Steatosis (CAS) in Colorectal Cancer" Current Oncology 28, no. 4: 3030-3040. https://doi.org/10.3390/curroncol28040265
APA StyleLee, M. C. M., Kachura, J. J., Vlachou, P. A., Dzulynsky, R., Di Tomaso, A., Samawi, H., Baxter, N., & Brezden-Masley, C. (2021). Evaluation of Adjuvant Chemotherapy-Associated Steatosis (CAS) in Colorectal Cancer. Current Oncology, 28(4), 3030-3040. https://doi.org/10.3390/curroncol28040265