Trajectory of End-of-Life Pain and Other Physical Symptoms among Cancer Patients Receiving Home Care

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Population
2.2. Data Sources
2.3. Outcomes
2.4. Covariates
2.5. Analysis
3. Results
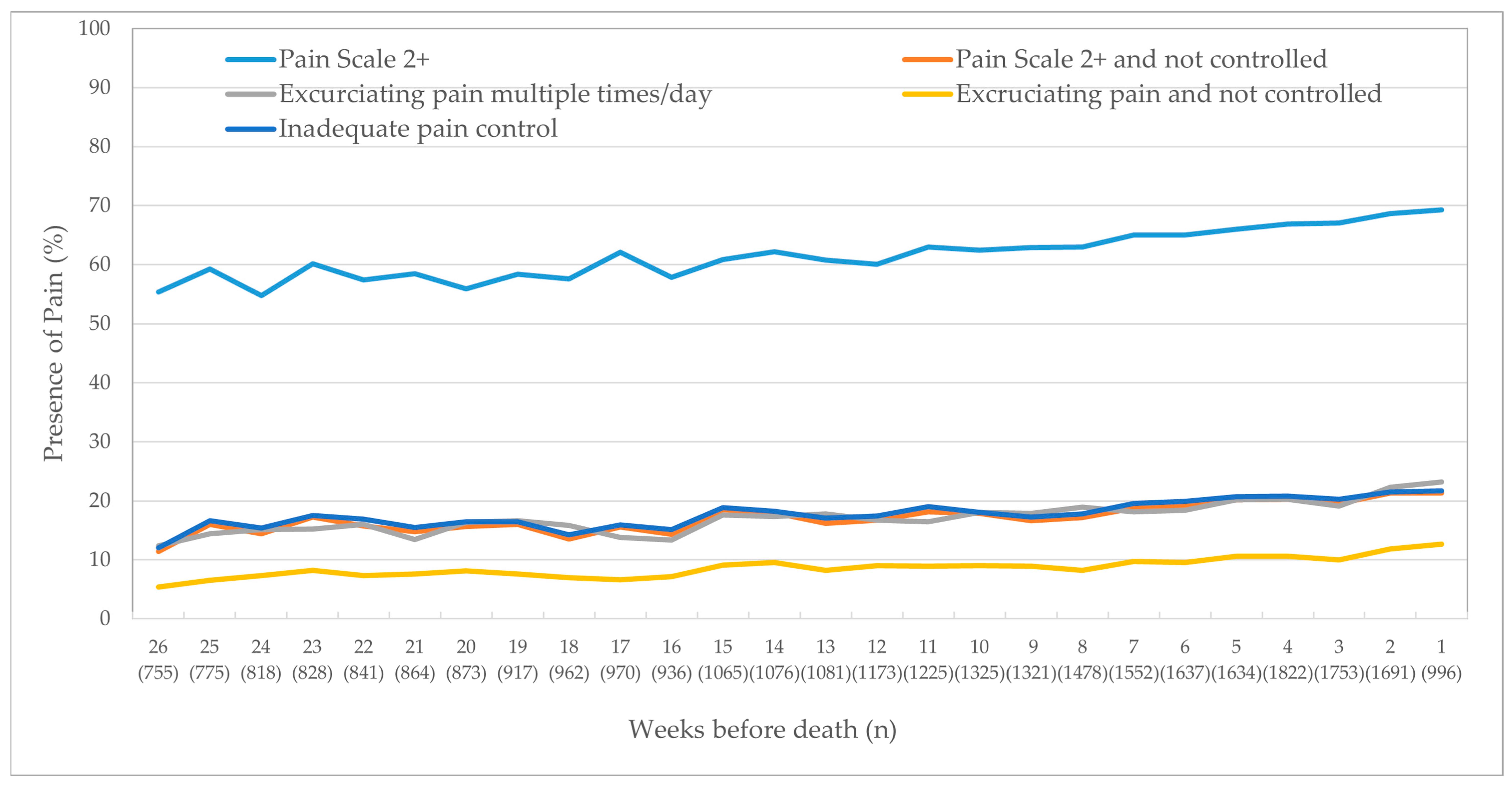
3.1. Pain
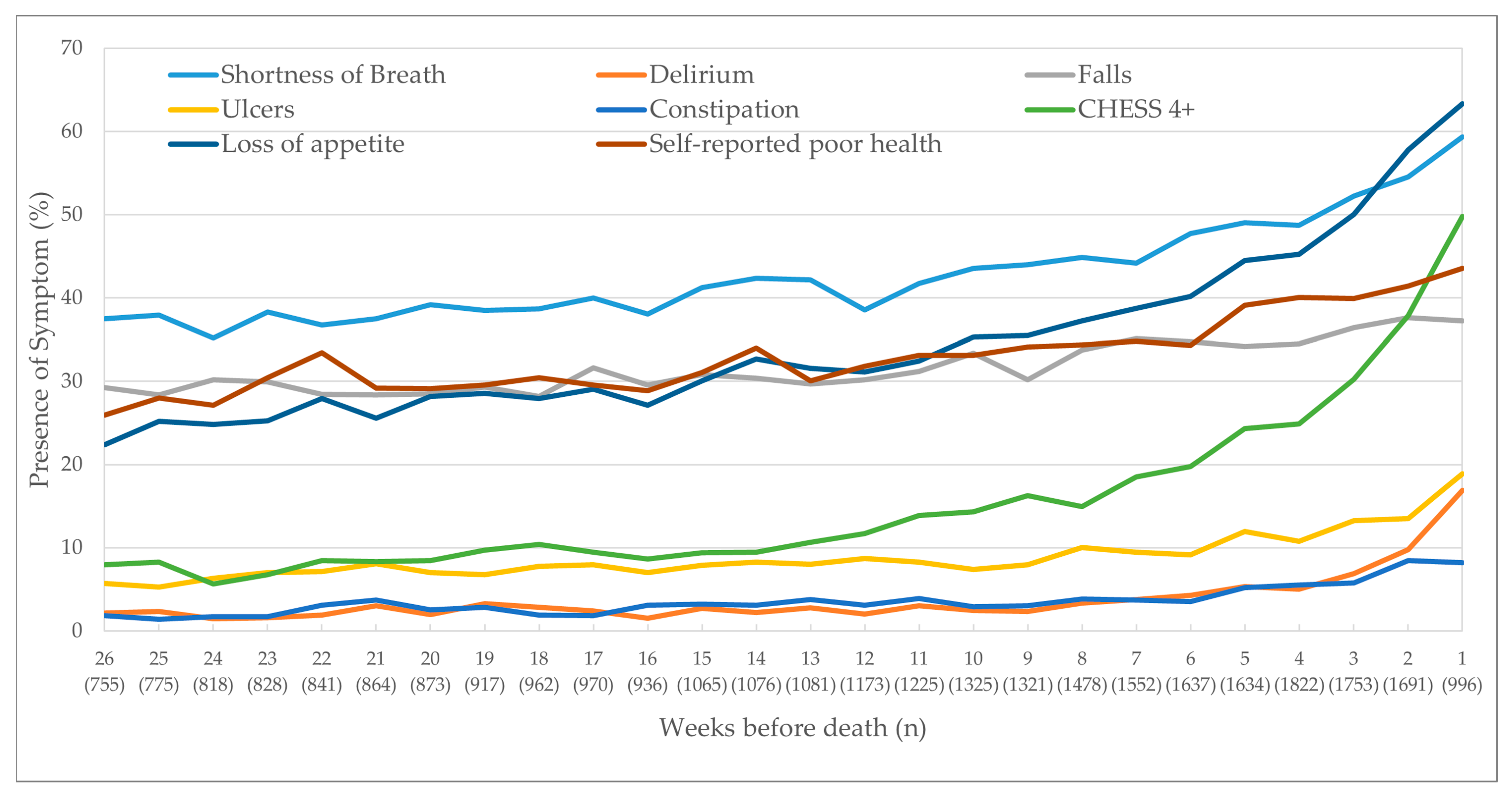
3.2. Other Non-Pain-Related Physical Outcomes
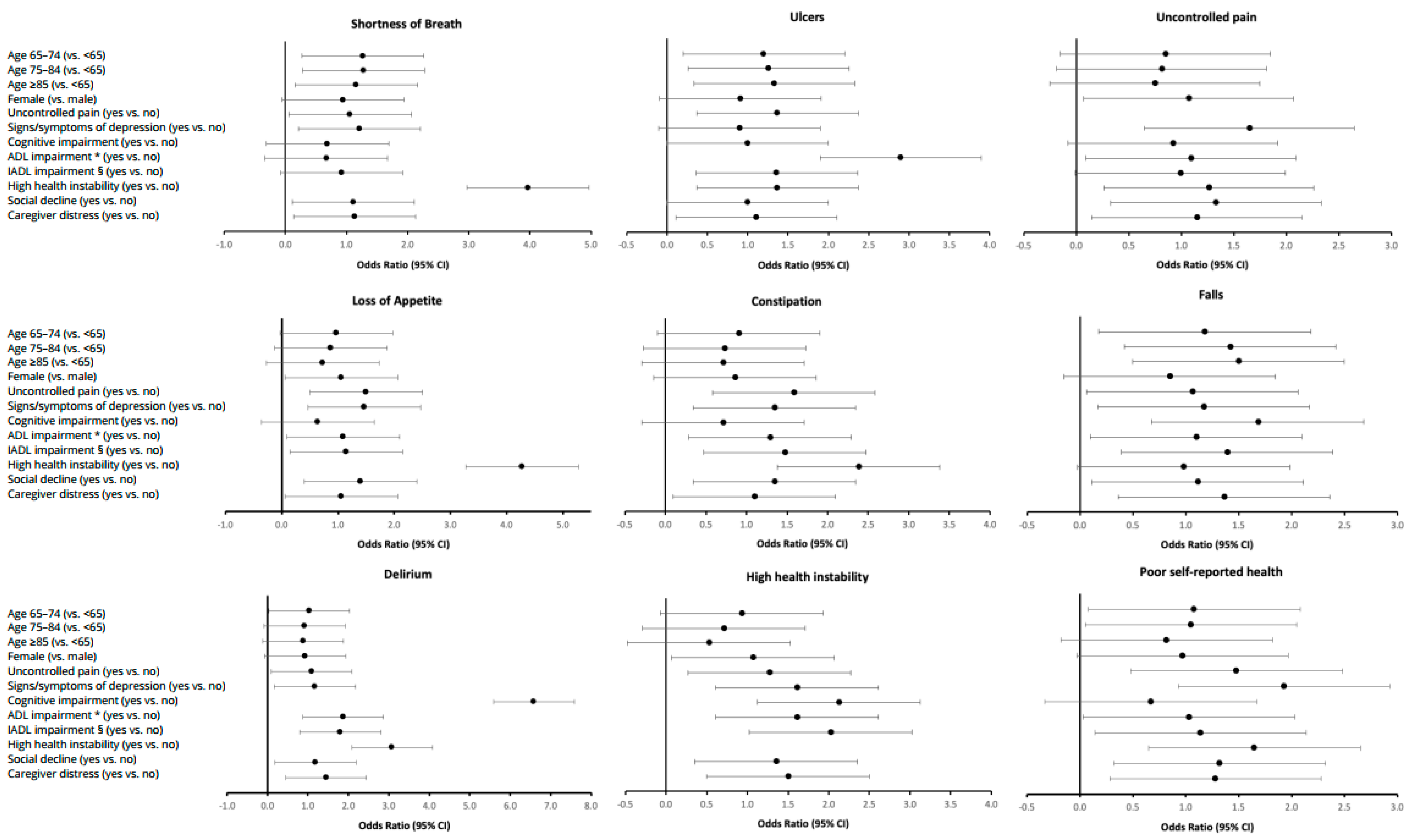
3.3. Regression
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lorenz, K.; Lynn, J.; Dy, S.; Hughes, R.; Mularski, R.; Shugarman, L.R.; Wilkinson, A.M. Cancer care quality measures: Symptoms and end-of-life care. Évid. Rep. Assess. 2006, 2006, 1–77. [Google Scholar]
- Lorenz, K.A.; Lynn, J.; Dy, S.M.; Shugarman, L.R.; Wilkinson, A.; Mularski, R.A.; Morton, S.C.; Hughes, R.G.; Hilton, L.K.; Maglione, M.; et al. Evidence for Improving Palliative Care at the End of Life: A Systematic Review. Ann. Intern. Med. 2008, 148, 147–159. [Google Scholar] [CrossRef]
- Carr, D.; Goudas, L.; Lawrence, D.; Pirl, W.; Lau, J.; Devine, D.; Kupelnick, B.; Miller, K. Management of Cancer Symptoms: Pain, Depression, and Fatigue: Evidence Report /Technology Assessment, Number. PsycEXTRA Dataset 2002, 2002, 1–5. [Google Scholar] [CrossRef][Green Version]
- Barbera, L.; Seow, H.; Howell, D.; Sutradhar, R.; Earle, C.; Liu, Y.; Stitt, A.; Husain, A.; Sussman, J.; Dudgeon, D. Symptom burden and performance status in a population-based cohort of ambulatory cancer patients. Cancer 2010, 116, 5767–5776. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.E.; Snyder, C.F.; Abernethy, A.P.; Basch, E.; Potosky, A.L.; Roberts, A.C.; Loeffler, D.R.; Reeve, B.B. Review of Electronic Patient-Reported Outcomes Systems Used in Cancer Clinical Care. J. Oncol. Pr. 2014, 10, e215–e222. [Google Scholar] [CrossRef]
- Seow, H.; Barbera, L.; Sutradhar, R.; Howell, D.; Dudgeon, D.; Atzema, C.; Liu, Y.; Husain, A.; Sussman, J.; Earle, C. Trajectory of Performance Status and Symptom Scores for Patients with Cancer During the Last Six Months of Life. J. Clin. Oncol. 2011, 29, 1151–1158. [Google Scholar] [CrossRef]
- Barbera, L.; Seow, H.; Sutradhar, R.; Chu, A.; Burge, F.; Fassbender, K.; McGrail, K.; Lawson, B.; Liu, Y.; Pataky, R.; et al. Quality of End-of-Life Cancer Care in Canada: A Retrospective Four-Province Study Using Administrative Health Care Data. Curr. Oncol. 2015, 22, 341–355. [Google Scholar] [CrossRef]
- Armstrong, J.J.; Stolee, P.; Hirdes, J.P.; Poss, J.W. Examining three frailty conceptualizations in their ability to predict negative outcomes for home-care clients. Age Ageing 2010, 39, 755–758. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.N.; Fries, B.E.; Steel, K.; Ikegami, N.; Bernabei, R.; Carpenter, G.I.; Gilgen, R.; Hirdes, J.P.; Topinková, E. Comprehensive Clinical Assessment in Community Setting: Applicability of the MDS-HC. J. Am. Geriatr. Soc. 1997, 45, 1017–1024. [Google Scholar] [CrossRef] [PubMed]
- Hawes, C.; Fries, B.E.; James, M.L.; Guihan, M. Prospects and pitfalls: Use of the RAI-HC assessment by the Department of Veterans Affairs for home care clients. Gerontologist 2007, 47, 378–387. [Google Scholar] [CrossRef]
- Barbera, L.; Seow, H.; Husain, A.; Howell, D.; Atzema, C.; Sutradhar, R.; Earle, C.; Sussman, J.; Liu, Y.; Dudgeon, D. Opioid Prescription After Pain Assessment: A Population-Based Cohort of Elderly Patients with Cancer. J. Clin. Oncol. 2012, 30, 1095–1099. [Google Scholar] [CrossRef] [PubMed]
- de Arriba, J.J.; Nerin, C.; Ortiz, M.C.; del Soto Sesma, M.; Beltran, S.; Vila, B. Symptom scores and delirium in advanced cancer. J. Clin. Oncol. 2011, 29, 2833–2834. [Google Scholar] [CrossRef]
- Cook, R.J.; Berg, K.; Lee, K.-A.; Poss, J.W.; Hirdes, J.P.; Stolee, P. Rehabilitation in Home Care Is Associated With Functional Improvement and Preferred Discharge. Arch. Phys. Med. Rehabil. 2013, 94, 1038–1047. [Google Scholar] [CrossRef]
- Hirdes, J.P.; Ljunggren, G.; Morris, J.N.; Frijters, D.H.M.; Soveri, H.F.; Gray, L.; Björkgren, M.; Gilgen, R. Reliability of the interRAI suite of assessment instruments: A 12-country study of an integrated health information system. BMC Heal. Serv. Res. 2008, 8, 277. [Google Scholar] [CrossRef]
- Kim, H.; Jung, Y.; Sung, M.; Lee, J.; Yoon, J.; Yoon, J. Reliability of the interRAI Long Term Care Facilities (LTCF) and interRAI Home Care (HC). Geriatr. Gerontol. Int. 2015, 15, 220–228. [Google Scholar] [CrossRef]
- Morris, J.N.; Bernabei, R.; Ikegami, N.; Gilgen, R.; Frijters, D.; Hirdes, J.P.; Fries, B.E.; Steel, K.; Carpenter, I.; Du Pasquier, J.; et al. RAI-Home Care (RAI-HC) Assessment Manual for Version 2; interRAI Corporation: Washington, DC, USA, 1999. [Google Scholar]
- Fries, B.E.; Simon, S.E.; Morris, J.N.; Flodstrom, C.; Bookstein, F.L. Pain in U.S. nursing homes: Validating a pain scale for the minimum data set. Gerontologist 2001, 41, 173–179. [Google Scholar] [CrossRef]
- Hirdes, J.P.; Frijters, D.H.; Teare, G.F. The MDS-CHESS Scale: A New Measure to Predict Mortality in Institutionalized Older People. J. Am. Geriatr. Soc. 2003, 51, 96–100. [Google Scholar] [CrossRef]
- Burrows, A.B.; Morris, J.N.; Simon, S.; Hirdes, J.P.; Phillips, C. Development of a minimum data set-based depression rating scale for use in nursing homes. Age Ageing 2000, 29, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.N.; Fries, B.E.; Mehr, D.R.; Hawes, C.; Phillips, C.; Mor, V.; Lipsitz, L.A. MDS Cognitive Performance Scale(C). J. Gerontol. 1994, 49, M174–M182. [Google Scholar] [CrossRef]
- Morris, J.N.; Fries, B.E.; Morris, S.A. Scaling ADLs Within the MDS. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 1999, 54, M546–M553. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.N.; Berg, K.; Fries, B.; Steel, K.; Howard, E.P. Scaling functional status within the interRAI suite of assessment instruments. BMC Geriatr. 2013, 13, 128. [Google Scholar] [CrossRef]
- Freeman, S.; Hirdes, J.P.; Stolee, P.; Garcia, J.; Smith, T.F. Correlates and Predictors of Changes in Dyspnea Symptoms Over Time Among Community-Dwelling Palliative Home Care Clients. J. Pain Symptom Manag. 2015, 50, 793–805. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Non-Pain Physical Items | Description of Questions in the RAI-HC |
|---|---|
| Shortness of breath | Client experiences shortness of breath at any point in the last three days |
| Delirium | Client experiences a sudden change in mental function within the last seven days |
| Falls | Client has experienced one or more falls within the last 90 days |
| Ulcers | Presence of any ulcer (pressure or stasis) at the time of the assessment |
| Loss of appetite | Client experiences a loss of appetite on at least two of the last three days |
| Constipation | Client has not had a bowel movement within the last three days |
| High health instability using the CHESS Scale score of 4 or more | Client shows high or very high health instability. Client receives a score of 1 for having the presence of a symptom variable, up to a maximum of 2 (e.g., dyspnea, weight loss, dehydration, fluid loss), then another 1 point for having the presence of each of these three variables: change in decision making, change in ADL status, and evidence of end-stage disease, i.e., prognosis of less than six months (scale scored from 0 (no health instability) to 5 (very high health instability)) [18] |
| Self-reported poor heath | Client feels they have poor health |
| Pain Items | |
| Pain Scale score of 2 or more | The Pain Scale is scored from 0 to 3. A score of 0 means a patient experiences no pain; 1 means less than daily pain; 2 means daily pain that is not severe; 3 means daily pain that is severe [17] |
| Pain Scale 2 or more and not controlled | Pain Scale score of 2 or more, and the pain is not adequately controlled by medications |
| Excruciating pain multiple times per day | Client experiences pain that is excruciating or horrible multiple times per day |
| Excruciating pain and not controlled | Excruciating pain multiple times per day, and the pain is not adequately controlled by medications |
| Inadequate pain control by medications | From a client’s point of view, medications do not adequately control pain |
| Cohort Characteristics | Overall | Died in Hospital | Died at Home | Absolute Standardized Difference | |
|---|---|---|---|---|---|
| % (N) | |||||
| Total | 100.0 (27,295) | 58.2 (15,888) | 41.8 (11,407) | ||
| Age | Under 65 | 22.1 (6021) | 22.4 (3562) | 21.6 (2459) | 0.02 |
| 65–74 | 22.0 (6009) | 22.0 (3496) | 22.0 (2513) | 0.00 | |
| 75–84 | 32.9 (8988) | 33.6 (5340) | 32.0 (3648) | 0.03 | |
| 85+ | 23.0 (6275) | 22.0 (3488) | 24.4 (2787) | 0.06 | |
| Most recent assessment’s date before death | 0–4 weeks | 22.8 (6219) | 22.1 (3504) | 23.8 (2714) | 0.04 |
| 5–12 weeks | 39.3 (10,717) | 39.4 (6251) | 39.1 (4465) | 0.01 | |
| 13–26 weeks | 38.0 (10,359) | 38.6 (6131) | 37.1 (4228) | 0.03 | |
| Sex | Female | 46.8 (12,777) | 46.7 (7411) | 47.0 (5365) | 0.01 |
| Pain Scale | Moderate to Severe Pain (score of 2–4) | 62.8 (17,154) | 61.4 (9751) | 64.9 (7403) | 0.07 |
| Depression Rating Scale | Signs/symptoms of depression (score of 3–14) | 22.3 (6076) | 21.6 (3434) | 23.2 (2642) | 0.04 |
| Cognitive Performance Scale | Moderate–severe impairment (score of 2–6) | 31.8 (8683) | 29.5 (4681) | 35.1 (4002) | 0.12 |
| ADL* Self-Performance Hierarchy Scale | Moderate–severe impairment (score of 3–6) | 20.3 (5543) | 15.9 (2530) | 26.4 (3013) | 0.26 |
| IADL § Involvement Scale | Moderate–severe impairment (score of 14–48) | 48.9 (13,361) | 44.1 (7006) | 55.7 (6355) | 0.23 |
| Social decline | Decline in social activities as compared to 90 days ago | 62.0 (19,622) | 59.0 (9374) | 66.2 (7548) | 0.15 |
| Caregiver items | Primary caregiver lives with client | 67.9 (18,532) | 67.1 (10,659) | 69.0 (7873) | 0.04 |
| Caregiver expresses feelings of anger, distress or depression | 18.8 (5143) | 18.1 (2877) | 19.9 (2266) | 0.05 | |
| Marital status | Married, common-law | 58.2 (15,878) | 57.8 (9178) | 58.7 (6700) | 0.02 |
| Widowed, separated, divorced | 37.1 (10,116) | 36.9 (5858) | 37.3 (4258) | 0.01 | |
| Never married | 4.8 (1301) | 5.4 (852) | 3.9 (449) | 0.07 | |
| Education completed µ | Grade 11 or less | 38.7 (7233) | 40.6 (4481) | 36.0 (2752) | 0.09 |
| High school | 24.6 (4587) | 23.9 (2640) | 25.5 (1947) | 0.04 | |
| College, university, trade | 36.8 (6867) | 35.5 (3915) | 38.6 (2952) | 0.06 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seow, H.; Guthrie, D.M.; Stevens, T.; Barbera, L.C.; Burge, F.; McGrail, K.; Chan, K.K.W.; Peacock, S.J.; Sutradhar, R. Trajectory of End-of-Life Pain and Other Physical Symptoms among Cancer Patients Receiving Home Care. Curr. Oncol. 2021, 28, 1641-1651. https://doi.org/10.3390/curroncol28030153
Seow H, Guthrie DM, Stevens T, Barbera LC, Burge F, McGrail K, Chan KKW, Peacock SJ, Sutradhar R. Trajectory of End-of-Life Pain and Other Physical Symptoms among Cancer Patients Receiving Home Care. Current Oncology. 2021; 28(3):1641-1651. https://doi.org/10.3390/curroncol28030153
Chicago/Turabian StyleSeow, Hsien, Dawn M. Guthrie, Tara Stevens, Lisa C. Barbera, Fred Burge, Kimberlyn McGrail, Kelvin K. W. Chan, Stuart J. Peacock, and Rinku Sutradhar. 2021. "Trajectory of End-of-Life Pain and Other Physical Symptoms among Cancer Patients Receiving Home Care" Current Oncology 28, no. 3: 1641-1651. https://doi.org/10.3390/curroncol28030153
APA StyleSeow, H., Guthrie, D. M., Stevens, T., Barbera, L. C., Burge, F., McGrail, K., Chan, K. K. W., Peacock, S. J., & Sutradhar, R. (2021). Trajectory of End-of-Life Pain and Other Physical Symptoms among Cancer Patients Receiving Home Care. Current Oncology, 28(3), 1641-1651. https://doi.org/10.3390/curroncol28030153