Clinicopathological Significances of Tumor–Stroma Ratio (TSR) in Colorectal Cancers: Prognostic Implication of TSR Compared to Hypoxia-Inducible Factor-1α Expression and Microvessel Density



Abstract
1. Introduction
2. Materials and Methods
2.1. Cases Selection and Specimens
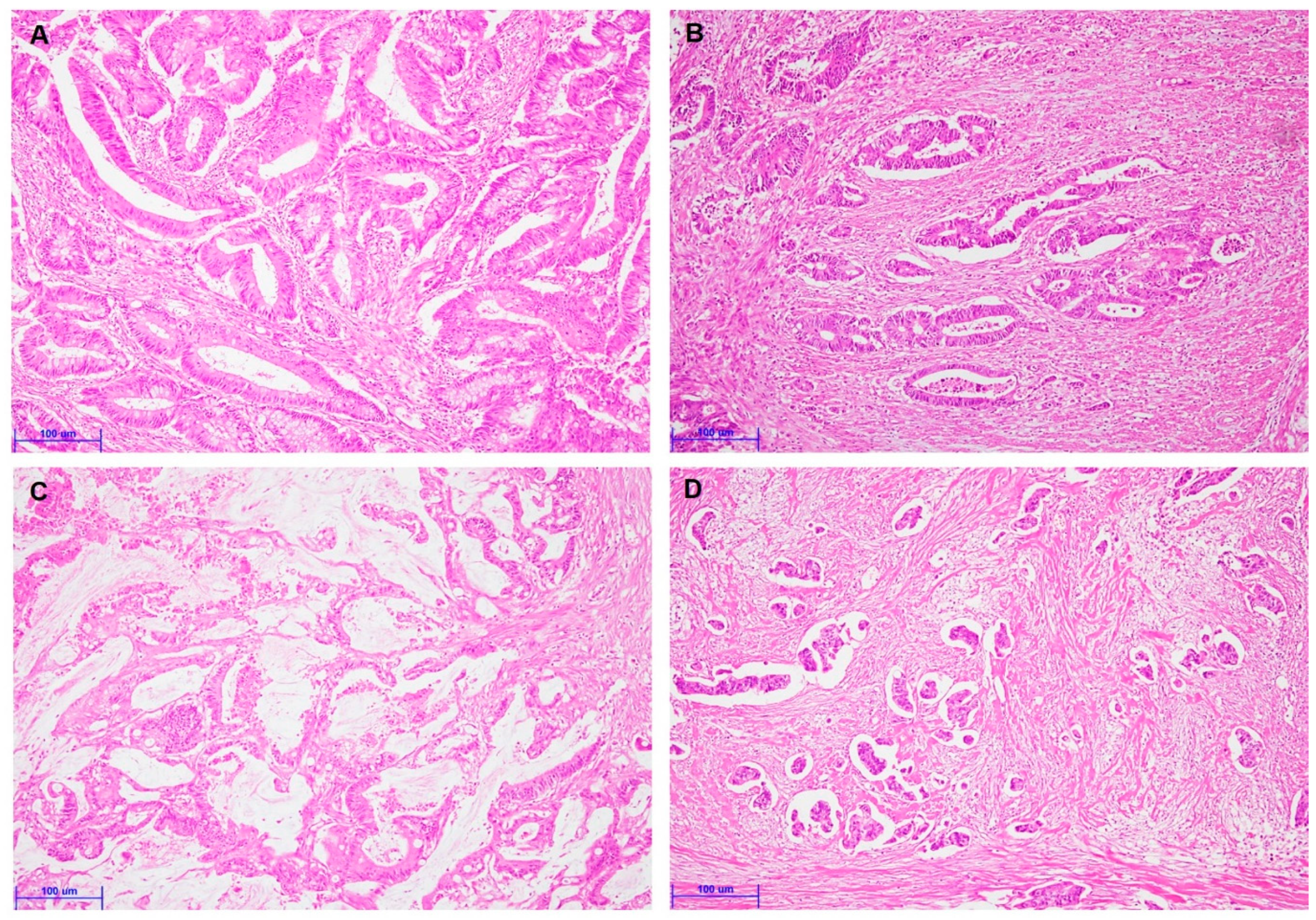
2.2. Evaluation of Tumor–Stroma Ratio
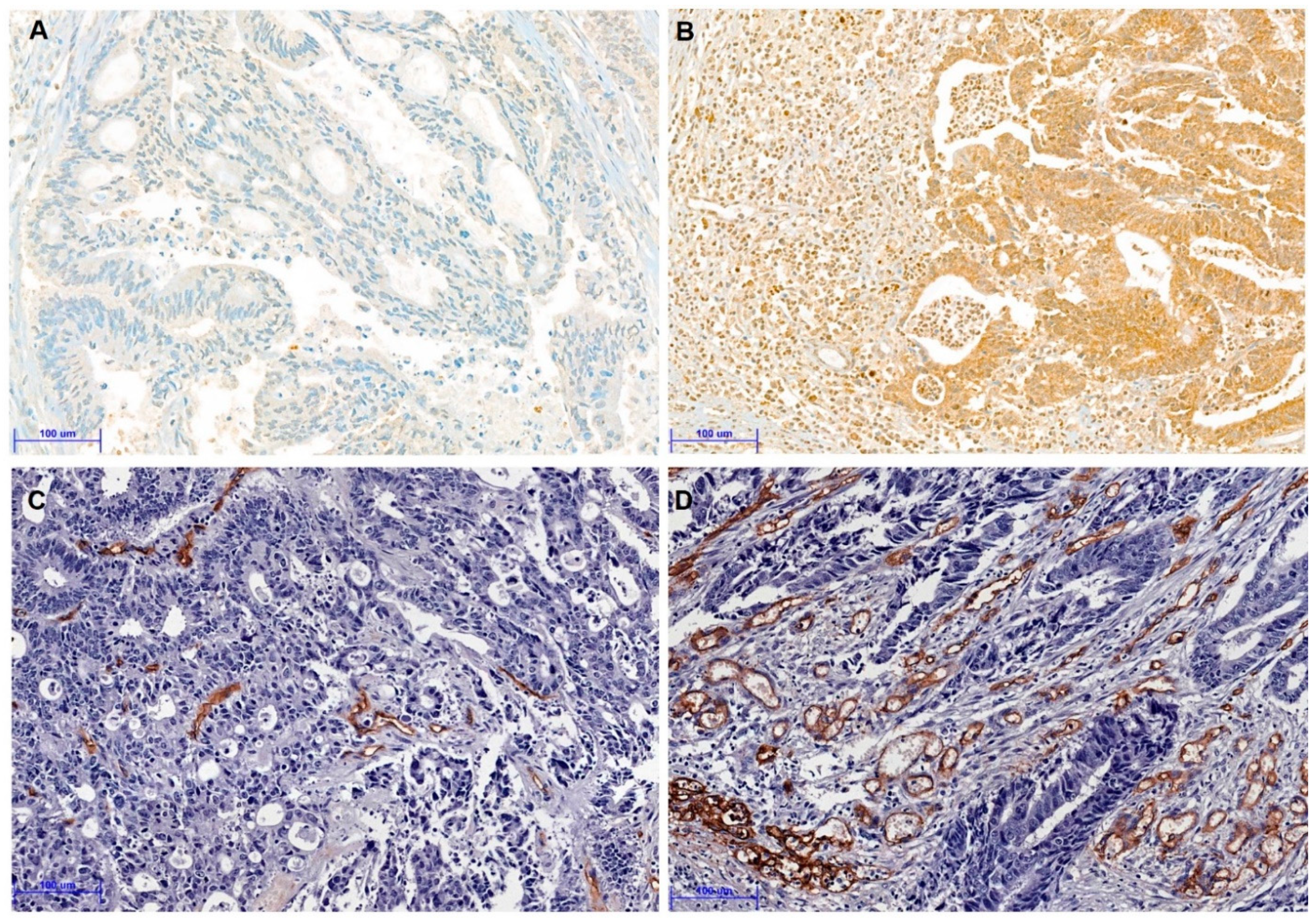
2.3. Tissue Microarrays and Immunohistochemistry
2.4. Evaluation of Microvessel Density
2.5. Statistical Analyses
3. Results
3.1. Correlation between Tumor–Stroma Ratio and Clinicopathological Characteristics
3.2. Correlation between Tumor–Stroma Ratio and Clinicopathological Characteristics
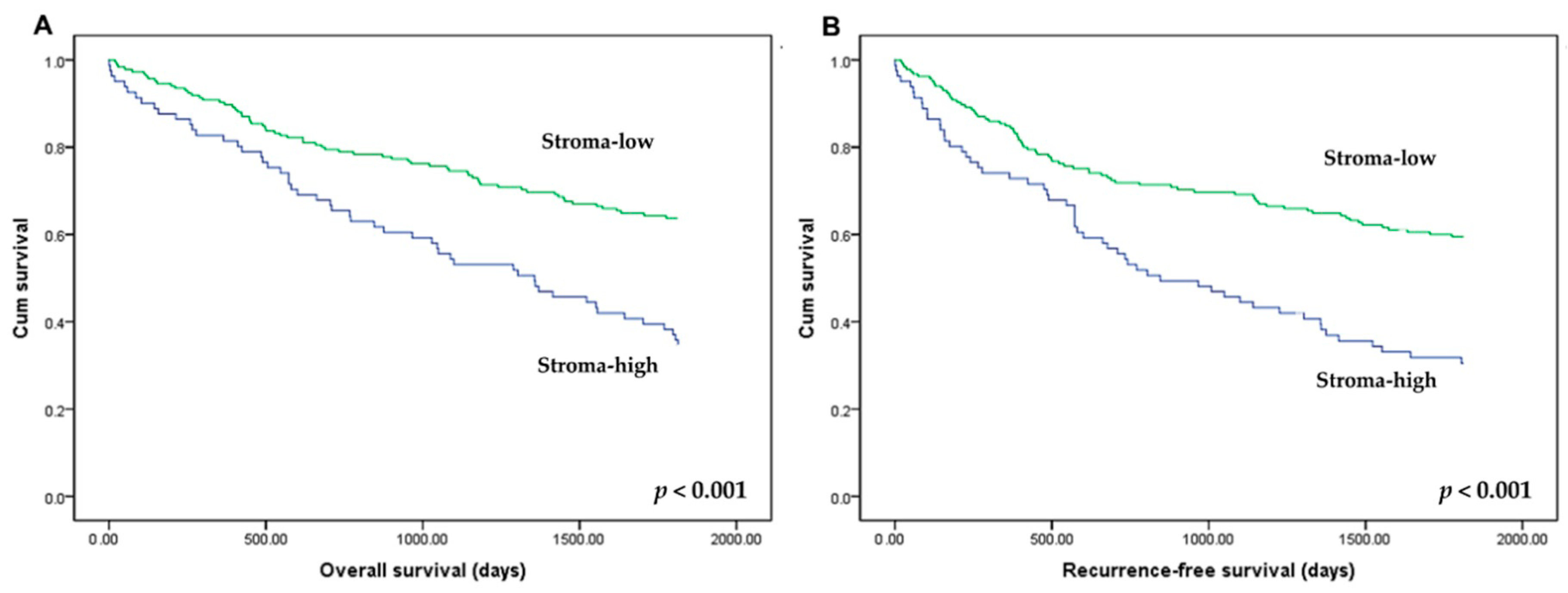
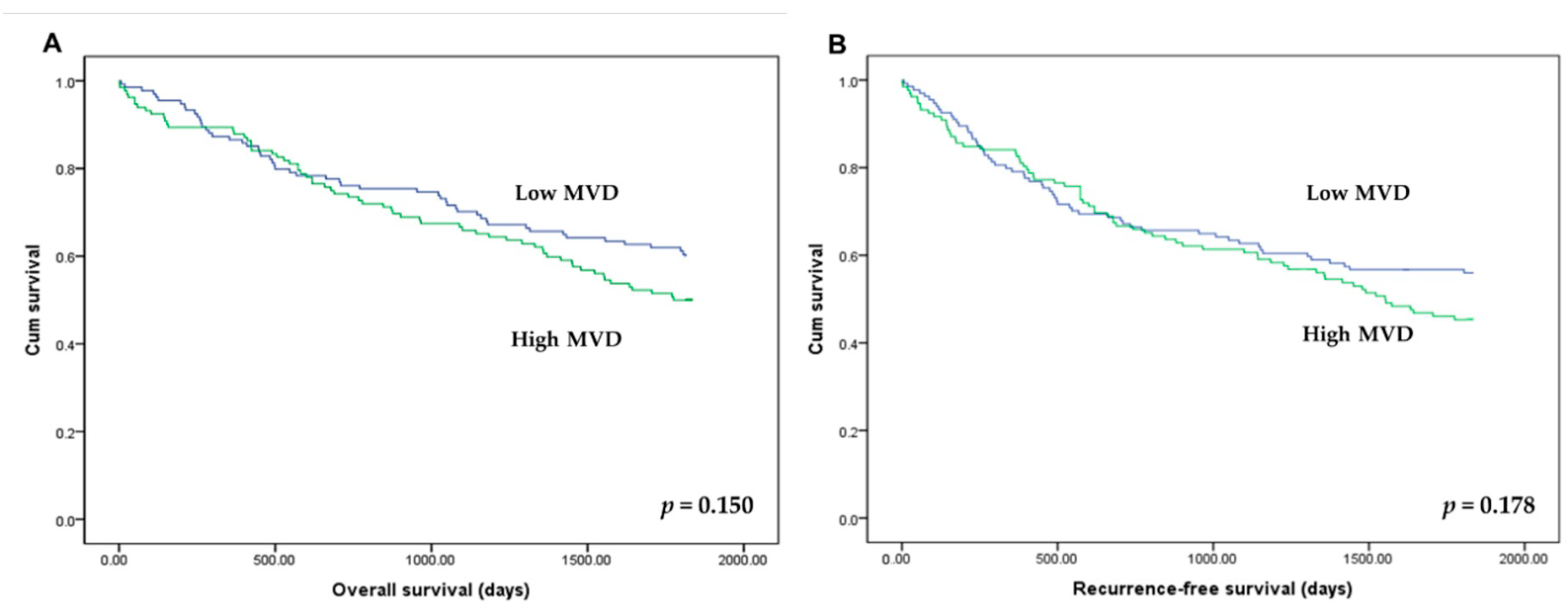
3.3. Correlation between Tumor–Stroma Ratio and Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xu, R.; Won, J.Y.; Kim, C.H.; Kim, D.E.; Yim, H. Roles of the Phosphorylation of Transcriptional Factors in Epithelial-Mesenchymal Transition. J. Oncol. 2019, 2019, 5810465. [Google Scholar] [CrossRef]
- Vogelaar, F.J.; van Pelt, G.W.; van Leeuwen, A.M.; Willems, J.M.; Tollenaar, R.A.; Liefers, G.J.; Mesker, W.E. Are disseminated tumor cells in bone marrow and tumor-stroma ratio clinically applicable for patients undergoing surgical resection of primary colorectal cancer? The Leiden MRD study. Cell. Oncol. 2016, 39, 537–544. [Google Scholar] [CrossRef]
- Le, C.C.; Bennasroune, A.; Langlois, B.; Salesse, S.; Boulagnon-Rombi, C.; Morjani, H.; Dedieu, S.; Appert-Collin, A. Functional Interplay Between Collagen Network and Cell Behavior Within Tumor Microenvironment in Colorectal Cancer. Front. Oncol. 2020, 10, 527. [Google Scholar] [CrossRef] [PubMed]
- Anitei, M.G.; Zeitoun, G.; Mlecnik, B.; Marliot, F.; Haicheur, N.; Todosi, A.M.; Kirilovsky, A.; Lagorce, C.; Bindea, G.; Ferariu, D.; et al. Prognostic and predictive values of the immunoscore in patients with rectal cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2014, 20, 1891–1899. [Google Scholar] [CrossRef]
- Galon, J.; Mlecnik, B.; Bindea, G.; Angell, H.K.; Berger, A.; Lagorce, C.; Lugli, A.; Zlobec, I.; Hartmann, A.; Bifulco, C.; et al. Towards the introduction of the ‘Immunoscore’ in the classification of malignant tumours. J. Pathol. 2014, 232, 199–209. [Google Scholar] [CrossRef]
- Galon, J.; Pagès, F.; Marincola, F.M.; Angell, H.K.; Thurin, M.; Lugli, A.; Zlobec, I.; Berger, A.; Bifulco, C.; Botti, G.; et al. Cancer classification using the Immunoscore: A worldwide task force. J. Transl. Med. 2012, 10, 205. [Google Scholar] [CrossRef]
- Pyo, J.S.; Son, B.K.; Chung, K.H.; Oh, I.H. Clinicopathological significance and prognostic implication of programmed death-1 ligand 2 expression in colorectal cancer. Int. J. Biol. Markers 2019, 34, 276–283. [Google Scholar] [CrossRef]
- Ko, Y.S.; Pyo, J.S. Clinicopathological significance and prognostic role of tumor-infiltrating lymphocytes in colorectal cancer. Int. J. Biol. Markers 2019, 34, 132–138. [Google Scholar] [CrossRef]
- Huijbers, A.; Tollenaar, R.A.; v Pelt, G.W.; Zeestraten, E.C.; Dutton, S.; McConkey, C.C.; Domingo, E.; Smit, V.T.; Midgley, R.; Warren, B.F.; et al. The proportion of tumor-stroma as a strong prognosticator for stage II and III colon cancer patients: Validation in the VICTOR trial. Ann. Oncol. 2013, 24, 179–185. [Google Scholar] [CrossRef]
- Mesker, W.E.; Junggeburt, J.M.; Szuhai, K.; de Heer, P.; Morreau, H.; Tanke, H.J.; Tollenaar, R.A. The carcinoma-stromal ratio of colon carcinoma is an independent factor for survival compared to lymph node status and tumor stage. Cell. Oncol. Off. J. Int. Soc. Cell. Oncol. 2007, 29, 387–398. [Google Scholar] [CrossRef]
- Mesker, W.E.; Liefers, G.J.; Junggeburt, J.M.; van Pelt, G.W.; Alberici, P.; Kuppen, P.J.; Miranda, N.F.; van Leeuwen, K.A.; Morreau, H.; Szuhai, K.; et al. Presence of a high amount of stroma and downregulation of SMAD4 predict for worse survival for stage I-II colon cancer patients. Cell. Oncol. 2009, 31, 169–178. [Google Scholar] [CrossRef]
- Park, J.H.; Richards, C.H.; McMillan, D.C.; Horgan, P.G.; Roxburgh, C.S.D. The relationship between tumour stroma percentage, the tumour microenvironment and survival in patients with primary operable colorectal cancer. Ann. Oncol. 2014, 25, 644–651. [Google Scholar] [CrossRef]
- Scheer, R.; Baidoshvili, A.; Zoidze, S.; Elferink, M.A.G.; Berkel, A.E.M.; Klaase, J.M.; van Diest, P.J. Tumor-stroma ratio as prognostic factor for survival in rectal adenocarcinoma: A retrospective cohort study. World J. Gastrointest. Oncol. 2017, 9, 466–474. [Google Scholar] [CrossRef]
- Zengin, M. Tumour Budding and Tumour Stroma Ratio are Reliable Predictors for Death and Recurrence in Elderly Stage I Colon Cancer Patients. Pathol. Res. Pract. 2019, 215, 152635. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Kemi, N.; Eskuri, M.; Herva, A.; Leppänen, J.; Huhta, H.; Helminen, O.; Saarnio, J.; Karttunen, T.J.; Kauppila, J.H. Tumour-stroma ratio and prognosis in gastric adenocarcinoma. Br. J. Cancer 2018, 119, 435–439. [Google Scholar] [CrossRef]
- Pyo, J.S.; Son, B.K.; Oh, D.; Kim, E.K. BRG1 is correlated with poor prognosis in colorectal cancer. Hum. Pathol. 2018, 73, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Remmele, W.; Stegner, H.E. Recommendation for uniform definition of an immunoreactive score (IRS) for immunohistochemical estrogen receptor detection (ER-ICA) in breast cancer tissue. Pathologe 1987, 8, 138–140. [Google Scholar]
- Kim, S.Y.; Ko, Y.S.; Park, J.; Choi, Y.; Park, J.W.; Kim, Y.; Pyo, J.S.; Yoo, Y.B.; Lee, J.S.; Lee, B.L. Forkhead Transcription Factor FOXO1 Inhibits Angiogenesis in Gastric Cancer in Relation to SIRT1. Cancer Res. Treat. 2016, 48, 345–354. [Google Scholar] [CrossRef] [PubMed]
- Hansen, T.F.; Kjær-Frifeldt, S.; Lindebjerg, J.; Rafaelsen, S.R.; Jensen, L.H.; Jakobsen, A.; Sørensen, F.B. Tumor-stroma ratio predicts recurrence in patients with colon cancer treated with neoadjuvant chemotherapy. Acta Oncol. 2018, 57, 528–533. [Google Scholar] [CrossRef] [PubMed]
- Sandberg, T.P.; Oosting, J.; van Pelt, G.W.; Mesker, W.E.; Tollenaar, R.; Morreau, H. Molecular profiling of colorectal tumors stratified by the histological tumor-stroma ratio—Increased expression of galectin-1 in tumors with high stromal content. Oncotarget 2018, 9, 31502–31515. [Google Scholar] [CrossRef]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef]
- van Pelt, G.W.; Kjær-Frifeldt, S.; van Krieken, J.; Al Dieri, R.; Morreau, H.; Tollenaar, R.; Sørensen, F.B.; Mesker, W.E. Scoring the tumor-stroma ratio in colon cancer: Procedure and recommendations. Virchows Arch. Int. J. Pathol. 2018, 473, 405–412. [Google Scholar] [CrossRef]
- Huijbers, A.; van Pelt, G.W.; Kerr, R.S.; Johnstone, E.C.; Tollenaar, R.; Kerr, D.J.; Mesker, W.E. The value of additional bevacizumab in patients with high-risk stroma-high colon cancer. A study within the QUASAR2 trial, an open-label randomized phase 3 trial. J. Surg. Oncol. 2018, 117, 1043–1048. [Google Scholar] [CrossRef]
- Geessink, O.G.F.; Baidoshvili, A.; Klaase, J.M.; Ehteshami Bejnordi, B.; Litjens, G.J.S.; van Pelt, G.W.; Mesker, W.E.; Nagtegaal, I.D.; Ciompi, F.; van der Laak, J. Computer aided quantification of intratumoral stroma yields an independent prognosticator in rectal cancer. Cell. Oncol. 2019, 42, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Pyo, J.S.; Park, M.J.; Kang, D.W. The clinicopathological significance of micropapillary pattern in colorectal cancers. Hum. Pathol. 2018, 77, 159–165. [Google Scholar] [CrossRef]
- Klaassen, R.; Steins, A.; Gurney-Champion, O.J.; Bijlsma, M.F.; van Tienhoven, G.; Engelbrecht, M.R.W.; van Eijck, C.H.J.; Suker, M.; Wilmink, J.W.; Besselink, M.G.; et al. Pathological validation and prognostic potential of quantitative MRI in the characterization of pancreas cancer: Preliminary experience. Mol. Oncol. 2020, 14, 2176–2189. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stroma | p-Value | ||
|---|---|---|---|
| Low | High | ||
| Total (n = 266) | 185 (69.5) | 81 (30.5) | |
| Age (years ± SD) | 63.88 ± 12.97 | 62.91 ± 12.84 | 0.575 |
| Sex | 0.614 | ||
| Male | 92 (49.7) | 43 (53.1) | |
| Female | 93 (50.3) | 38 (46.9) | |
| Tumor size | 0.639 | ||
| ≤5 cm | 72 (38.9) | 34 (42.0) | |
| >5 cm | 113 (61.1) | 47 (58.0) | |
| Tumor size (cm ± SD) | 5.58 ± 2.17 | 5.18 ± 1.83 | 0.142 |
| Location of tumor | 0.280 | ||
| Right colon | 95 (51.4) | 33 (40.7) | |
| Left colon | 54 (29.2) | 29 (35.8) | |
| Rectum | 36 (19.5) | 19 (23.5) | |
| Tumor differentiation | 0.161 | ||
| Well | 15 (8.1) | 2 (2.5) | |
| Moderate | 130 (70.3) | 64 (79.0) | |
| Poorly | 40 (21.6) | 15 (18.5) | |
| Vascular invasion | 0.002 | ||
| Present | 10 (5.4) | 14 (17.3) | |
| Absent | 175 (94.6) | 67 (82.7) | |
| Lymphatic invasion | 0.085 | ||
| Present | 43 (23.2) | 27 (33.3) | |
| Absent | 142 (76.8) | 54 (66.7) | |
| Perineural invasion | <0.001 | ||
| Present | 19 (10.3) | 25 (30.9) | |
| Absent | 166 (89.7) | 56 (69.1) | |
| pT stage | 0.098 | ||
| pT1-2 | 33 (17.8) | 8 (9.9) | |
| pT3-4 | 152 (82.2) | 73 (90.1) | |
| Lymph node metastasis | 0.343 | ||
| Present | 98 (53.0) | 48 (59.3) | |
| Absent | 87 (47.0) | 33 (40.7) | |
| Distant metastasis | 0.027 | ||
| Present | 15 (8.1) | 14 (17.3) | |
| Absent | 170 (91.9) | 67 (82.7) | |
| pTNM stage | 0.280 | ||
| I | 25 (13.5) | 7 (8.6) | |
| II | 59 (31.9) | 24 (29.6) | |
| III | 86 (46.5) | 36 (44.4) | |
| IV | 15 (8.1) | 14 (17.3) | |
| Stroma | p-Value | ||
|---|---|---|---|
| Low | High | ||
| Mucinous component | 0.034 | ||
| Present | 38 (20.5) | 8 (9.9) | |
| Absent | 147 (79.5) | 73 (90.1) | |
| Pure micropapillary component | 0.002 | ||
| Present | 25 (13.5) | 24 (29.6) | |
| Absent | 160 (86.5) | 57 (70.4) | |
| Distribution of micropapillary component | 0.048 | ||
| ≥5% | 12 (25.5) | 13 (48.1) | |
| <5% or negative | 35 (74.5) | 14 (51.9) | |
| Stroma | p-Value | ||
|---|---|---|---|
| Low | High | ||
| HIF-1α * | 0.035 | ||
| Positive | 54 (29.2) | 34 (42.5) | |
| Negative | 131 (70.8) | 46 (57.5) | |
| Microvessel density ** | 0.008 | ||
| High | 82 (44.8) | 50 (62.5) | |
| Low | 101 (55.2) | 30 (37.5) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, G.; Pyo, J.-S.; Kim, N.-Y.; Kang, D.-W. Clinicopathological Significances of Tumor–Stroma Ratio (TSR) in Colorectal Cancers: Prognostic Implication of TSR Compared to Hypoxia-Inducible Factor-1α Expression and Microvessel Density. Curr. Oncol. 2021, 28, 1314-1324. https://doi.org/10.3390/curroncol28020125
Kang G, Pyo J-S, Kim N-Y, Kang D-W. Clinicopathological Significances of Tumor–Stroma Ratio (TSR) in Colorectal Cancers: Prognostic Implication of TSR Compared to Hypoxia-Inducible Factor-1α Expression and Microvessel Density. Current Oncology. 2021; 28(2):1314-1324. https://doi.org/10.3390/curroncol28020125
Chicago/Turabian StyleKang, Guhyun, Jung-Soo Pyo, Nae-Yu Kim, and Dong-Wook Kang. 2021. "Clinicopathological Significances of Tumor–Stroma Ratio (TSR) in Colorectal Cancers: Prognostic Implication of TSR Compared to Hypoxia-Inducible Factor-1α Expression and Microvessel Density" Current Oncology 28, no. 2: 1314-1324. https://doi.org/10.3390/curroncol28020125
APA StyleKang, G., Pyo, J.-S., Kim, N.-Y., & Kang, D.-W. (2021). Clinicopathological Significances of Tumor–Stroma Ratio (TSR) in Colorectal Cancers: Prognostic Implication of TSR Compared to Hypoxia-Inducible Factor-1α Expression and Microvessel Density. Current Oncology, 28(2), 1314-1324. https://doi.org/10.3390/curroncol28020125