1. INTRODUCTION
Since the 1990s, a 6-month course of adjuvant chemotherapy has been the standard of care for patients with resected high-risk stage II or III colon cancer [
1]. Despite recent advances in adjuvant therapy, a substantial proportion of such patients still experience disease relapse and premature death [
2]. Recently published observational data suggest that physical activity (
pa) is associated with a reduced risk of disease relapse and premature death in these colon cancer survivors.
In 2006, Meyerhardt
et al. [
3] reported results of a prospective observational study of 832 patients with stage III colon cancer enrolled in a randomized adjuvant chemotherapy trial and followed for a median of 3.8 years from trial entry. In that trial,
pa was self-reported approximately 6 months after completion of chemotherapy and was quantified as weekly metabolic equivalent task (
met)–hours (for example, walking briskly is approximately 4.0
mets). Categories of
pa were predefined in terms of these
met– hours: fewer than 3 (referent), 3–8.9, 9–17.9, 18–26.9, and more than 27. Analyses adjusted for known prognostic factors, including body mass index (BMI), indicated that higher levels of
pa were associated with superior disease-free (
dfs), recurrence-free, and overall survival. The 3-year
dfs was 75.1% in patients who exercised for fewer than 18
met–hours weekly as compared with 84.5% in patients who exercisedfor more than 18
met–hours weekly [hazard ratio (HR): 0.57; 95% confidence interval (
ci): 0.39 to 0.85].
In a second article, Meyerhardt
et al. [
4] reported results of a prospective observational study of 573 women from the Nurses’ Health Study diagnosed with stages I–III colorectal cancer. Self-reported leisure-time
pa before diagnosis and 1–4 years post-diagnosis was assessed, and analyses were again adjusted for known prognostic factors, including BMI. An inverse relationship was observed between the amount of
pa post-diagnosis and the risk of both colorectal cancer–specific and overall mortality. Specifically, as compared with women exercising for fewer than 3
met–hours weekly, the risk of colorectal cancer–specific mortality declined in successive groups performing more exercise: the HR was 0.92 (95%
ci: 0.50 to 1.69) in the 3–8.9
met–hours weekly group, 0.57 (95%
ci: 0.27 to 1.20) in the 9–17.9
met–hours weekly group, and 0.39 (95%
ci: 0.18 to 0.82) in the more than 18
met–hours weekly group. Risk of overall mortality was similarly reduced. Furthermore, change in
pa from preto post-diagnosis was also predictive of outcome. Compared with women who did not change their
pa, women who increased their
pa by at least 1 predefined
met category—for example, from fewer than 3
met–hours to 3–8.9
met–hours—between their pre-diagnostic and post-treatment assessments experienced improved outcomes; women whose exercise levels decreased by at least 1 predefined
met category had poorer outcomes. Further analysis of these data suggested that no additional benefit accrued with an increase in
pa post-diagnosis in women who were already achieving at least 9
met–hours weekly before diagnosis (that is, those who were roughly already meeting current public health guidelines).
Several plausible biologic mechanisms could account for an association between
pa and colon cancer outcomes, including metabolic consequences of obesity; decreased gastrointestinal transit time; decreased levels of insulin, insulin-like growth factors, and prostaglandin ratios; lowered bile acid secretion; and altered gut flora [
5]. Moreover, there is evidence that colon cancer survivors experience significant declines in
pa during adjuvant therapy [
6] and that they report among the lowest
pa participation rates of any cancer survivor group [
7], suggesting that, in the current
pa levels of colon cancer survivors, there is considerable room for improvement from a public health perspective. Finally, progress has been made in the science of health behaviour change over the past decade demonstrating that
pa can, indeed, be increased substantially and maintained over extended periods of time with an appropriate behavioural support program [
8,
9,
10]. Together, these observations suggest that interventions to increase
pa in colon cancer survivors may improve disease outcomes, that associated correlative biologic studies may provide insights into the mechanisms of colon cancer pathogenesis, and that sufficient understanding exists to implement an effective intervention.
Despite the highly suggestive observational findings, a randomized controlled trial (RCT) is needed to establish unequivocally the causal nature of this association and to inform policies for health care delivery. The primary objective of the Colon Health and LifeLong Exercise Change (challenge) trial CO.21 being undertaken by the National Cancer Institute of Canada Clinical Trials Group (ncic ctg) is to determine the effects of a 3-year structured pa intervention on dfs in survivors of high-risk stage II or III colon cancer who have completed adjuvant chemotherapy in the preceding 2–6 months and who are insufficiently active. Secondary objectives are to
determine the effects of the pa intervention on important secondary endpoints including overall survival, multiple patient-reported outcomes (pros), and objective physical functioning.
identify the determinants of long-term pa adherence in the intervention arm.
explore the associations between selected molecular markers and study endpoint measures.
provide an economic evaluation of the pa intervention.
We hypothesize that colon cancer survivors randomized to the pa intervention arm will experience improvements in dfs, pros, and objective physical functioning as compared with survivors allocated to general health education.
2. METHODS
2.1. Study Design and Participants
We will be conducting a multinational, multicentre, phase III trial with randomization to a
pa intervention versus general health education materials. This study will be led by the
ncic ctg and will include collaboration with the Australasian Gastro-Intestinal Trials Group.
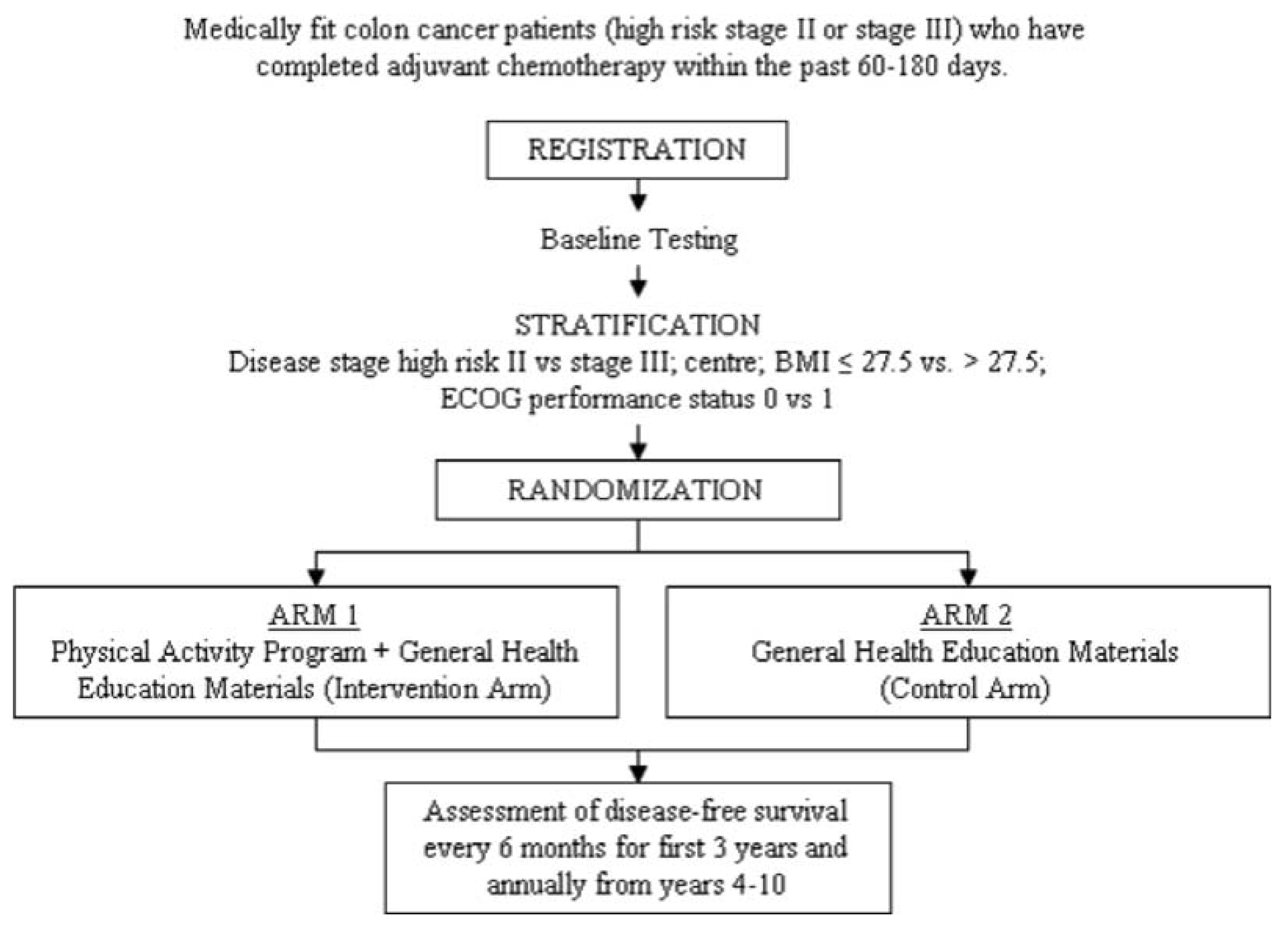
Figure 1 presents the anticipated flow of participants through the trial. Medically-fit survivors of high-risk stage II or III colon cancer who have received their last dose of adjuvant chemotherapy within the preceding 60–180 days will be recruited. This group has been identified as being at high risk for disease recurrence or death, being most likely to adhere to the intervention, and being individuals for whom the
pa intervention is safe.
Table 1 details the eligibility criteria. Pre-registration evaluations will focus on current
pa involvement and medical eligibility for study participation. Patients who are already meeting current public health guidelines for
pa (150 minutes or more of moderate-to-vigorous or 75 minutes or more of vigorous
pa weekly), as estimated for the month before registration using the Leisure Time Exercise Questionnaire, will be ineligible. Consenting patients will be registered and will then undergo submaximal exercise testing to ensure that they are able to exercise safely at a moderate-to-vigorous intensity. Provided that 2 stages of the treadmill test are completed with acceptable heart rate and blood pressure responses, patients will then complete the remaining baseline investigations, including a physical functioning test, anthropometric testing, blood collection for correlative studies,
pros,
pa behaviour and determinants, health utility, and a health economics work productivity and activity impairment questionnaire (
wpai). Patients will then be stratified by centre, disease stage (high-risk II vs. III), BMI (≤27.5 vs. >27.5), and Eastern Cooperative Oncology Group performance status (0 vs. 1), and will be randomized to receive the
pa intervention program (intervention arm) or general health education materials (comparison arm).
Figure 1.
Flow of participants through the Colon Health and Life-Long Exercise Change (challenge) trial.
Figure 1.
Flow of participants through the Colon Health and Life-Long Exercise Change (challenge) trial.
2.2. Physical Activity Intervention
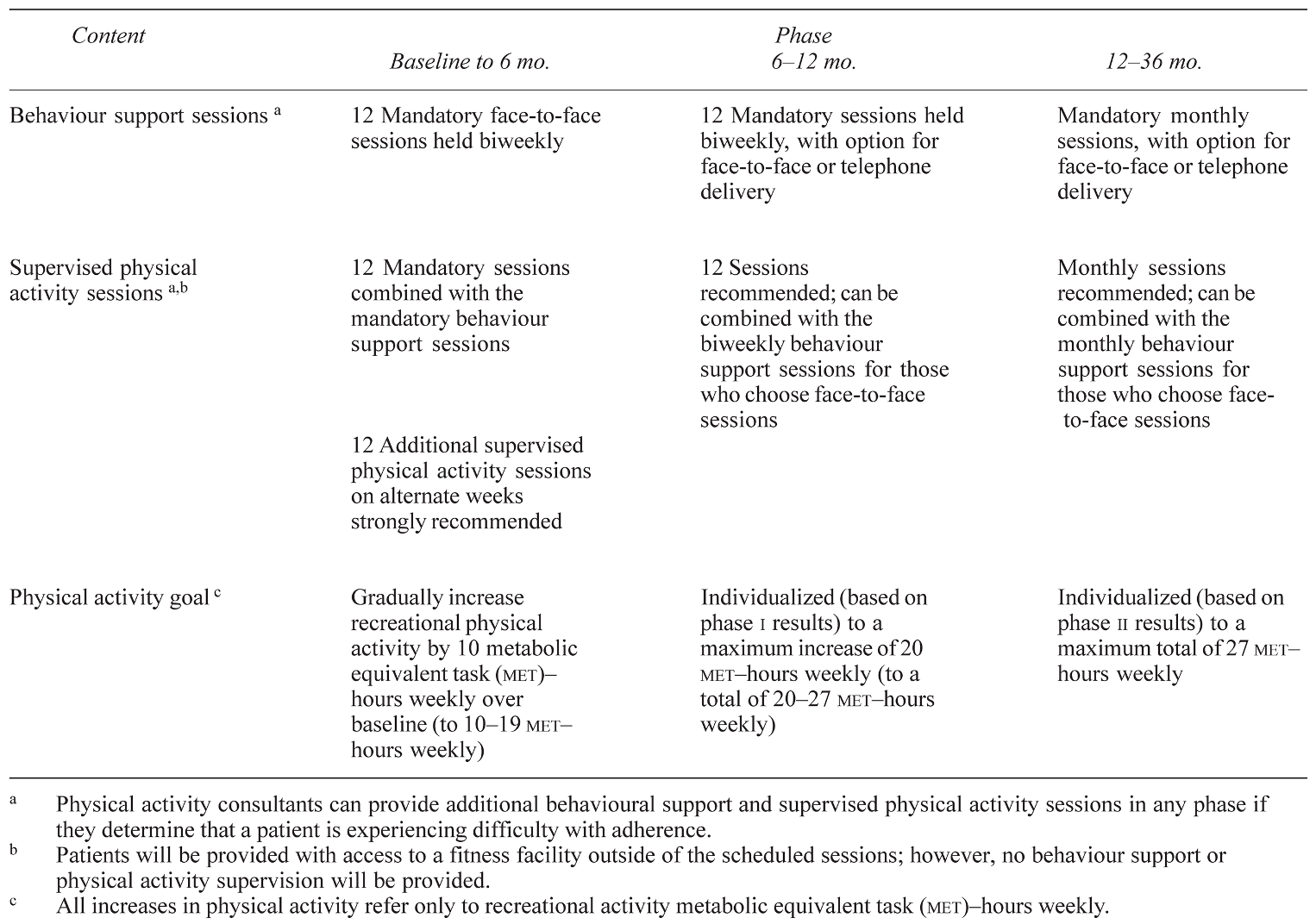
Participants in both arms will be provided with general health education materials including information about nutrition and pa. Participants in both groups will also receive follow-up care at the participating cancer centre, including regular physician visits, imaging, blood work, and colonoscopy. Participants assigned to the pa intervention will receive a structured 3-year pa program delivered by a local pa consultant (pac). The goal for the pa intervention group is to increase recreational pa from baseline by at least 10 met–hours weekly to a maximum of 27 met–hours weekly. The 10 met–hours weekly is roughly equivalent to the current public health guidelines of about 2.5 hours (for example, 5 days of 30 minutes daily) of moderate-intensity pa weekly, such as brisk walking (4 mets), or 1.25 hours (for example, 3 days of 25 minutes daily) of vigorous-intensity pa weekly such as jogging (8 mets). At the end of 6 months, a decision to encourage participants to increase pa by more than 10 met–hours weekly will be determined and will depend on their adaptation to the initial goal of an increase of 10 met– hours weekly. Patients will not be encouraged to increase their pa beyond 27 met–hours weekly, which is equivalent to about 1 hour daily of brisk walking for 7 days each week or 1 hour daily of jogging for 3.5 days each week.
Achieving an increase in
pa from baseline of at least 10
met–hours weekly will require a significant amount of behaviour support. Participants in the intervention arm will therefore receive an intensive behaviour support program based on the Theory of Planned Behaviour [
11] and modelled after the successful behavioural change program in the Diabetes Prevention Program [
10] and the Look AHEAD trial [
8]. The
pa intervention will be delivered in 3 distinct phases and will consist of behaviour support sessions and supervised
pa sessions (
Table 2). The intervention will include a personalized
pa prescription that accounts for the individual’s baseline fitness test results,
pa history, performance status, personal preferences, and individual barriers to activity.
Table 1.
Inclusion and exclusion criteria for the challenge trial.
Table 1.
Inclusion and exclusion criteria for the challenge trial.
2.3. Behaviour Support Sessions
Behaviour support sessions will include training in behavioural strategies to promote the adoption and longterm maintenance of
pa. Key behavioural strategies will include an emphasis on the unique benefits of
pa for colon cancer survivors; strategies for making
pa enjoyable, for overcoming barriers, for securing social support from family and friends, and for identifying environmental opportunities; and time management, selfmonitoring, goal setting, planning, stimulus control, and self-reinforcement. At the core of the behavioural intervention will be a
pa guidebook that will contain topics and materials that the
pacs can use to reinforce and expand on during counselling sessions. The guidebook, called
Step Up to the Challenge!, will be distributed to each
pa intervention participant as an ongoing resource. It is modeled after a guidebook originally developed for breast cancer survivors and has been shown to be effective for increasing motivation,
pa, and quality of life in breast cancer survivors [
12,
13,
14]. Throughout all phases of the study,
pacs are able to provide additional behaviour support sessions if they determine that a patient is experiencing difficulty with adherence.
Advanced behavioural strategies will be considered for patients who have significant struggles in adopting or maintaining pa despite continued support from the pac. A behavioural toolbox will assist in overcoming barriers to pa, many of which will likely be related to issues of opportunity to perform exercise in the winter. The primary approach will be to have a facility available free of charge year round at each centre. All patients will also be provided with pedometers to motivate them and to help them track their pa.
Table 2.
Physical activity program intervention.
Table 2.
Physical activity program intervention.
2.4. Supervised Physical Activity Sessions
In addition to counselling sessions focusing on behaviour support, patients will also receive supervised pa sessions. These sessions will be combined with behaviour support sessions and will also occur independently. Their focus will be to teach proper pa technique and how to monitor intensity and to progress pa safely and effectively. In the first 6 months, these mandatory sessions will be supervised by the pac. Thereafter, supervision is strongly recommended. The supervision may be 1:1 with the pac or in a group format. Throughout all phases of the study, pacs will be able to provide additional supervised pa sessions if they determine that a patient is experiencing difficulties with adherence. Patients will be provided free access to a fitness facility at times outside of their supervised pa sessions.
2.5. Primary and Secondary Endpoints
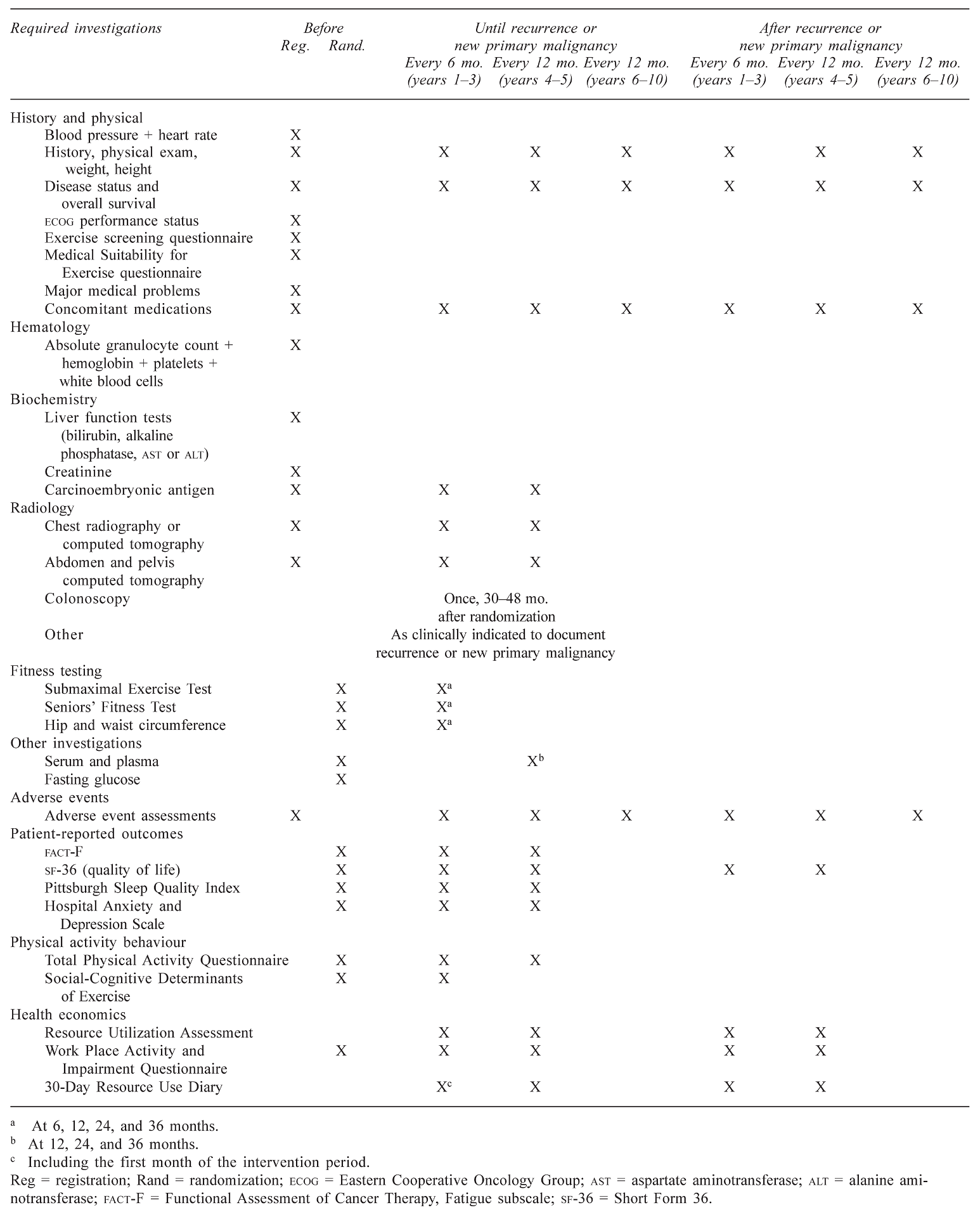
Table 3 presents the nature and timing of the study evaluations. The primary endpoint is
dfs, because available data demonstrate that 3-year
dfs is highly correlated with overall survival in patients with resected colon cancer [
15]. This endpoint is now accepted for registration of trials by the U.S. Food and Drug Administration. Secondary endpoints will include overall survival,
pros assessing quality of life [the Short Form (SF-36) and Functional Assessment of Cancer Therapy, General subscale], fatigue (Functional Assessment of Cancer Therapy, Fatigue subscale), sleep quality (Pittsburgh Sleep Quality Index), and anxiety and depression (Hospital Anxiety and Depression Scale), and objective testing of physical functioning consisting of anthropometric measurements, cardiovascular fitness (submaximal exercise test using the Balke treadmill protocol [
16]); and physical functioning (Seniors Fitness Test [
17]). Adherence to
pa will be assessed at baseline and every 6–12 months by using a slight modification of the Past Year Total Physical Activity Questionnaire [
18,
19]. The Past Year Total Physical Activity Questionnaire has been shown to have acceptable reliability and validity for measurement of past-year
pa [
19]. Correlative biologic markers will include blood measures of insulin, insulin-like growth factors, and selected cytokines. Finally, an economic evaluation will be performed to assess cost-effectiveness and cost–utility of the
pa intervention. Patient utilities will be measured using the SF-6D, which is derived from the SF-36 quality-oflife measure [
20] that has been validated in population surveys and clinical trials settings. Resource utilization and
wpai will be collected prospectively as part of the economic analysis.
2.6. Statistical Considerations
The analysis will be performed using the intent-to-treat principle and is powered to detect a HR of 0.75 for dfs between patients randomized to two treatment arms. To detect such a HR with a power of 80% and a twotailed alpha of 0.05, we will need to observe 380 events during follow-up. It is anticipated that a total of 962 patients will be randomized over 3 years. To observe 380 events, we assume that the patients in the comparison group will have a 3-year dfs of 75% and will not materially change their pa behaviour from baseline. It is also assumed that 20% of patients randomized to the intervention group will not adhere to their pa program. With these assumptions, it is estimated that, to observe 380 events among 962 patients randomized, 4.7 years of additional follow-up after the last patient is randomized will be required, which leads to an approximate total study duration of 7.7 years. Four interim analyses will be performed: the first analysis will assess the feasibility of accrual principles, the second will assess the feasibility of the pa behaviour change, and the final two will assess for unexpectedly large magnitudes of benefit or futility.
2.7. Trial Management
The development and oversight of the CO.21 trial is provided by the Trial Steering Committee, which includes the study chairs and the Design and Conduct Committee members; the coordinators for Quality of Life, Economic Evaluations, and Correlative Sciences committees; and the ncic ctg central office physician coordinator, senior biostatistician, and study coordinator. Because of the complexities of delivering a lifestyle intervention and because of the uniqueness of this study, four working groups were established to provide expertise in protocol development and trial implementation in four key areas: pa, pros, health economics, and correlative studies. Each of these working groups is chaired by a member of the Trial Steering Committee with expertise in the respective field. A pa Working Group will provide oversight to the pa and behaviour support components of the study, including monitoring of adherence. This working group is led by the study chair.
3. DISCUSSION
Colorectal cancer is the third most common cancer in Canadian men and women and the second leading cause of cancer-related death [
21]. There are more than 110,000 colorectal cancer survivors in Canada. This growing number of survivors has generated interest in behaviour and lifestyle interventions that might further improve disease outcomes and quality of life. In colon cancer,
pa has been strongly associated with improved disease outcomes, and there are plausible biologic mechanisms for this association. However, the data published to date have been observational. Moreover, few colon cancer survivors currently exercise, partly because of the physical and psychological effects of their disease and treatments, and partly because of the lack of guidance and support from cancer care organizations. However, recent progress in behavioural change suggests that, with appropriate support, such populations can be motivated to adopt long-term lifestyle changes. Consequently, all the necessary evidence, rationale, and justification exist to warrant the conduct of an RCT of
pa and disease outcomes in colon cancer survivors.
Moreover, in the era of molecularly targeted anticancer therapy, funding of new and expensive agents is becoming increasingly difficult. Should a pa intervention be found to have a significant clinical benefit in colon cancer patients, this type of intervention could be a very cost-effective therapy, with the potential for many other non-cancer-related health benefits. The magnitude of the associations between pa and disease outcomes in the observational studies of colon cancer compares favourably with the benefit observed with the use of adjuvant chemotherapy, but would likely involve lower toxicity and cost. Importantly, the costeffectiveness of this pa intervention will be prospectively evaluated as part of this clinical trial, because all interventions are recognized to have a cost component that needs to be considered when evaluating the effectiveness of the intervention to reduce the burden of a disease at a population level.
Positive findings from the challenge trial would support a new and additional paradigm to be tested in patients with other forms of cancer and would enhance interest in applying these results to test strategies for cancer prevention. One of the greatest challenges to implementing pa programs in any population has been ensuring adequate support and resources to promote behaviour change with regard to pa. Cancer patients are, in general, a sedentary but motivated population. Previous work has suggested good adherence and a willingness to pursue lifestyle modifications following a diagnosis of cancer. If this RCT is able to demonstrate a significant benefit in dfs, that finding would provide an impetus to patients to participate in pa and to oncologists and cancer care organizations to promote pa. It could also potentially lead to changes in public perception that might influence the policies by which pa experts are utilized within the health care system. The challenge trial will also have an opportunity to evaluate the cost-effectiveness of potential policy recommendations.
Table 3.
Study evaluations.
Table 3.
Study evaluations.

 ,
, 

{kind=link}