Summary
Surgical replacement of the aortic arch is an established procedure that requires cardiopulmonary bypass and deep hypothermic circulatory arrest. However, this approach is associated with major perioperative risks. These risks and the fact that thoracic aneurysms have become more ubiquitous are the main argument for less invasive strategies. To treat complex coarctation (recurrence, hypoplastic aortic arch), various surgical approaches have been proposed. In these cases, resection with end-to-end anastomosis may be demanding and expose the patient to a substantial morbidity. Cardiopulmonary bypass (CPB) and deep hypothermic circulatory arrest may be necessary to control the distal aortic arch.
We present a less invasive, combined surgical and endovascular approach that allows partial or total exclusion of the aortic arch without the need for extracorporeal circulation, deep hypothermia and circulatory arrest. This technique was applied to 7 patients over the last 22 years.
All procedures were technically successful and 6 of 7 patients recovered well. Arteriography confirmed proper position of the stent graft and complete exclusion of the lesion at the end of the procedure. One patient had an endoleak type I and underwent successful additional retrograde stent-graft placement over the proximal landing zone three weeks following the initial procedure. One patient had a diffuse cerebral and spinal damage, most probably due to embolic shower during the procedure.
Clinical follow-up (between 8 and 18 months) has been fully uncomplicated in the 6 other patients and CT-scan at 6 months demonstrated complete exclusion of the arch lesion.
Assuming that technical refinements may improve the steps of the endovascular intervention, this combined approach may turn out to be the preferred therapeutic modality to repair aortic arch lesions in patients with multiple co-morbidities who otherwise would not be candidates for a conventional operative repair. Long-term observation is necessary to confirm the stability of this type of repair.
Introduction
Treatment of aneurysms, dissection and symptomatic atherosclerotic lesions located in the aortic arch represent a continuing formidable challenge. Until recently, surgical repair was the only effective treatment, involving often complex operations with substantial perioperative risk and mortality [1,2,3]. The early outcome has improved slightly in recent years, despite significant advances in perioperative care and surgical techniques (deep hypothermic circulatory arrest, antegrade cerebral perfusion and myocardial protection) [4]. Transluminal endovascular stent graft placement has been introduced as a promising alternative to repair aneurysms of the abdominal aorta and to a certain extent those involving the descending thoracic aorta [5,6,7,8,9,10]. This approach deemed to be less invasive but still allows complete exclusion of the lesion with an endoluminal prosthesis; however this technique requires safe landing zones of normal aorta. The aortic arch with its curvature and the origin of the supraaortic vessels still represents a location with special challenges for endovascular treatment.
Percutaneous balloon dilatation with or without stenting is often considered to be the first therapeutical option for simple re-coarctation in children and adult patients. However, some complex forms (complicated by pseudoaneurysms and those associated with diffuse hypoplasia of the aortic arch) may be more challenging to manage. Surgical treatment requires cardiopulmonary bypass (CPB) and exposure of the previously operated aortic segments, with inherent risks of injury to the adjacent nerves, bleeding and paraplegia. Aortic arch augmentation requires deep hypothermic circulatory arrest, exposing the patient to the risk of cerebrovascular complications.
We report on a promising less invasive approach that allows partial or complete repair of the aortic arch following “debranching” of the supraaortic vessels and revascularisation from the ascending aorta. This technique combines surgical and endovascular steps which do not require extracorporeal circulation.
Clinical experience
During a 30 months period between 2002 and 2004, 331 patients received surgical treatment for diseases of the thoracic aorta and 25 received endovascular stent-graft of the descending aorta. Complete arch replacement was performed using conventional surgical technique (cardiopulmonary bypass, deep hypothermia and antegrade cerebral perfusion) in 26 patients. We report on 7 additional patients who presented with complex previous aortic history (one case), several co-morbidities (six cases) that were estimated to be a contraindication for conventional surgical repair including cardiopulmonary bypass, deep hypothermia and circulatory arrest. Six patients received complete aortic arch repair and in one patient partial repair (distal to the innominate artery) was performed. Computed tomography with angiography and 3-D reconstruction confirmed the feasibility of the procedure.
Lesions were large atherosclerotic aneurysms (n = 4), grade IV atherosclerosis of the aortic arch with recurrent cerebral embolisation and a small aneurysm (n = 2) and hypoplastic aortic arch combined to complex coarctation (n = 1) following multiple procedures over the last 20 years.
Illustrative cases
- Case1
- 78-year-old man had a false atherosclerotic aneurysm (5.5 cm in size) located in the concavity of the aortic arch, with the entry being just opposite to the origin of the left common carotid artery. The patient and his relatives refused a conventional surgical approach. He has several cardiovascular risk factors, including coronary artery disease, cerebrovascular disease, arterial hypertension and obstructive lung disease.
- Case2
- The second patient was a 71-year-old woman with recurrent transient cerebral ischaemic episodes most probably caused by an atherosclerosis grade IV of the aortic arch with thick (1.5 cm) and mobile plaques and who had a small atherosclerotic aneurysm in the aortic arch as well (Figure 1)
- Case3
- The 21-year-old female presented with severe exercise arterial hypertension of the upper extremities (systolic blood pressure 220 mm Hg). She suffered from headache since 2 years. At the age of 3 weeks, she underwent surgery because of aortic coarctation. End-to-end anastomosis was performed. Two years later, percutaneous balloon dilatation was per-formed because of re-coarctation. At the age of 6 years, she suffered from arterial hyper-tension. A pericardial patch was used to enlarge the distal aortic arch and the proximal de-scending aorta. In the following, she required treatment with a beta-blocker and a con-verting-enzyme inhibitor.

Figure 1.
CT-scan demonstrates a small atherosclerotic aneurysm located in the mid-aortic arch and severe atheromatosis of the aortic arch.
Figure 1.
CT-scan demonstrates a small atherosclerotic aneurysm located in the mid-aortic arch and severe atheromatosis of the aortic arch.

Under this treatment, blood pressure remained slightly elevated. She presented later with severe arterial hypertension at rest and during exercise and MR-angiography revealed a long stenotic segment in the proximal descending aorta (diameter 3–4 mm) with a tubular hypoplasia of the midand distal aortic arch (8 mm), as well as an aneurysm (2.9 cm) at the site of previous coarctation repair. At that time, she was presented to the cardiologists, who decided to perform percutaneous balloon dilatation and stenting with a Wallstent. As expected, the hypoplastic segment could not be dilated, the pressure gradient remained constant (90 mm Hg) and the pseudoaneurysm was left untreated (Figure 2). A triple antihypertensive treatment including a calcium-channel blocker was started.
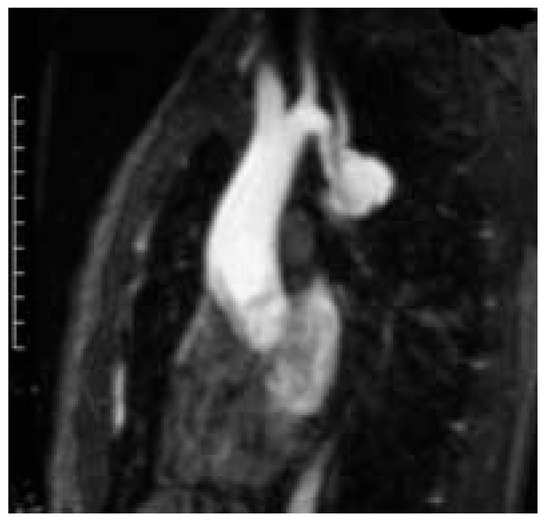
Figure 2.
Computed tomography of the 21-year-old patient with complex aortic coarctation. Following percutaneous dilatation with deployment of a Wallstent into the descending aorta, pseudoaneurysm at the site of previous coarctation interventions was still perfused.
In 2002, at the age of 21 years, she was referred to our institution because she wanted a definitive treatment. Angiography showed an increase of the aneurysm to 3.5 cm and a suboptimal position of the Wallstent which was lying in the origin of the left carotid artery.
Endovascular and operative technique
- Complete aortic arch repair
The procedure is performed in the operating theater. An arterial perfusion cannula is inserted into the left and right radial arteries and a sheat into the femoral artery for pigtail catheter angiography. Transesophageal echocardiography is performed routinely to assist the delivery of the endovascular device. Surgical debranching of the supraaortic vessels is performed through complete or superior median sternotomy. Epicardial scanning and palpation help to exclude calcified or soft atherosclerotic lesions in the ascending aorta.
The ascending aorta, the aortic arch and the supraaortic branches are dissected free using a “minimal touch” technique to prevent embolisation in case of severe atherosclerosis. Heparin is given at a dosage of 100 IE/kg. The first surgical step includes the construction of a bifurcated bypass graft (Vaskutek Gelsoft, Vaskutek Ltd., Renfrewshire, UK) from the ascending aorta to the innominate artery and the left common carotid artery. Both vessels are transected, oversewn at their aortic origin with a running polypropylene suture and anastomosed to the corresponding limb in an end-to-end fashion. If perfusion pressure distal to the occlusion is superior to 60 mm Hg, no additional cerebral protection is used; if it is less than 60, a temporary shunt is inserted.
The left subclavian artery is either transposed into the left carotid artery or revascularised at the end of the procedure using an additional 8 mm graft (Figure 3 and Figure 4).
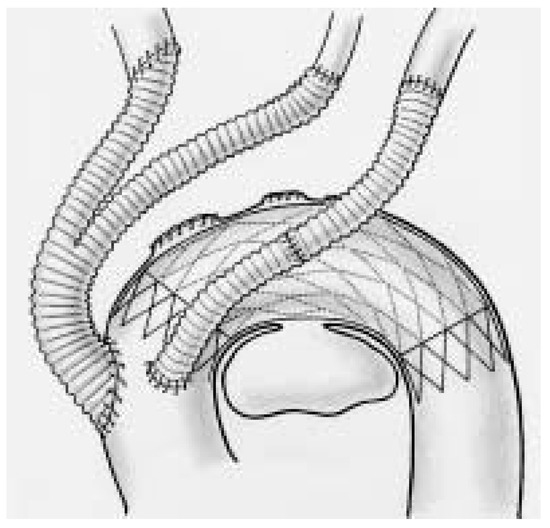
Figure 3.
Schematic representation of the combined surgical/endovascular approach which allows complete repair of the aortic arch following debranching and revascularization of the supraaortic vessels.
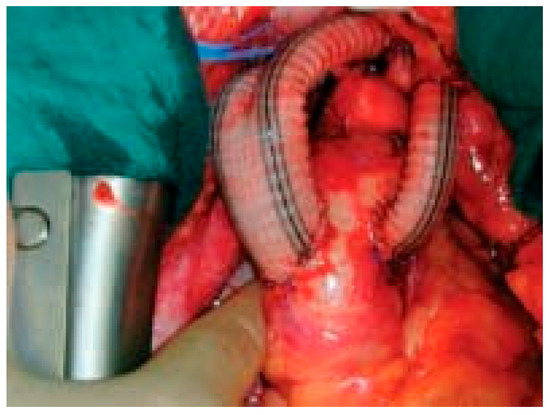
Figure 4.
Intraoperative view at the end of the procedure.
Introduction of the stent-graft prosthesis was performed in an antegrade way (n = 2) through a separate 8 mm graft which is anastomosed to the ascending aorta in an end-to-side fashion. After completion of the endovascular procedure, it is attached to the graft to the left subclavian artery. In four patients, the stentgraft was introduced retrogradely through a femoral artery access. In all cases adenosine was used to decrease systolic blood pressure to 50 mm Hg during stent-graft release in order to prevent uncontrolled displacement of the device.
The proximal landing zone is located in the most cranial part of the ascending aorta, occluding all supraaortic branches. The following prostheses were used: Talent (Medtronic, Minneapolis, MN) in 5 cases and the Endomed (Endofit Inc, Phoenix, AZ) in 2 cases.
Additional procedure
One 71-year-old female underwent double coronary artery bypass grafting in the beating heart technique immediately after aortic arch repair. The left internal thoracic artery was grafted to the left anterior descending branch and a saphenous vein graft was anastomosed to the right coronary artery.
- Partial debranching and extra-anatomic bypass in complex aortic coarctation
Surgical approach was performed through a median sternotomy. An arterial perfusion cannula was inserted into the left radial artery and a sheat into the femoral artery for pigtail catheter angiography. Intravascular ultrasound was used for proper intraoperative localisation of the aneurysm at the level of the previous coarctation patch repair.
The ascending aorta, the aortic arch and the supraaortic branches were dissected free. The descending aorta was exposed retro-pericardially by gentle luxation of the heart, using techniques known from off-pump coronary artery bypass surgery. After systemic heparinisation, the descending aorta was partially side-clamped and an end-to-side anastomosis with a ring-reinforced 16 mm ePTFE (ImpraFlex, Impra Inc., Tempe, AZ, USA) was performed using a running 5.0 polypropylene suture. Following local haemostasis, the posterior pericardium was readapted. The graft was positioned along the inferior aspect of the heart and the right atrium to the ascending aorta, where the proximal end-to-side anastomosis was performed. To maintain antegrade perfusion of the left carotid and subclavian artery, a 8 mm ePTFE bypass graft was constructed between the ascending aorta and the left carotid artery (which had been oversewn at the level of the aortic origin), and finally the left subclavian artery was transposed directly to the left carotid artery through the sternotomy approach.
Finally, a covered Wall-Graft stent-graft prosthesis was inserted within the previous Wallstent, expanded into the mid aortic arch and the proximal descending aorta and allowed complete exclusion of the aneurysm (Figure 5).
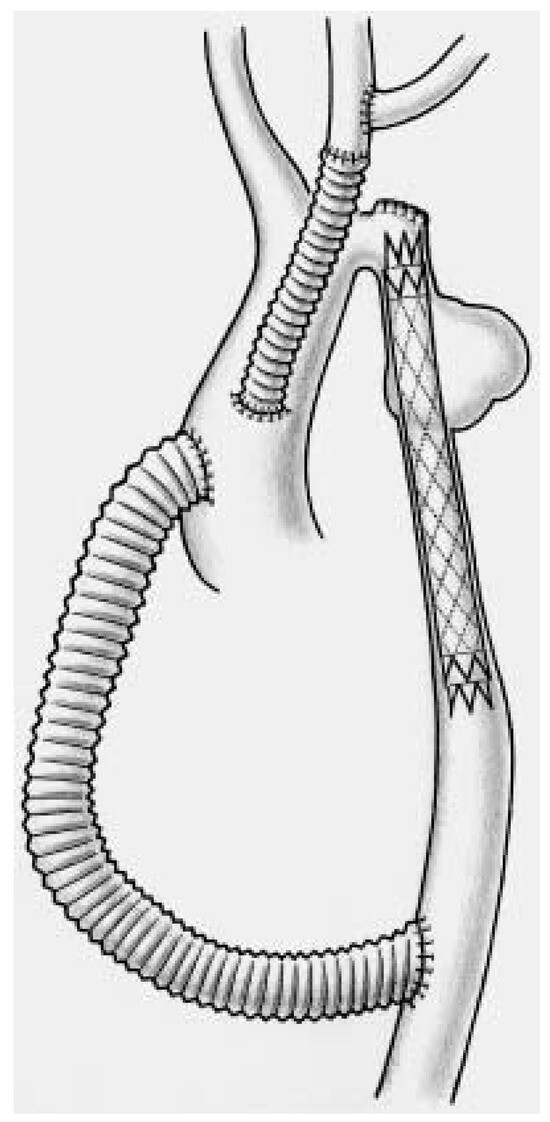
Figure 5.
Artist drawing of the situation following Wallstent insertion to treat complex coarctation. The hypoplastic aortic arch remained untreated (!!).
Results
All procedures were technically successful and 6 of 7 patients recovered without neurological, cardiac or bleeding complications. One patient with severe atheromatosis grade IV suffered from perioperative diffuse cerebral and spinal embolism leading to coma and paraparesis. He could be weaned from respirator but unfortunately he did not show any clinical improvement.
Arteriography confirmed proper position of the stent graft and complete exclusion of the lesion at the end of the procedure. CT-scans were performed in every patient before discharge (Figure 6). One patient had an endoleak type I and underwent successful additional retrograde stent-graft placement over the proximal landing zone three weeks following the initial procedure.
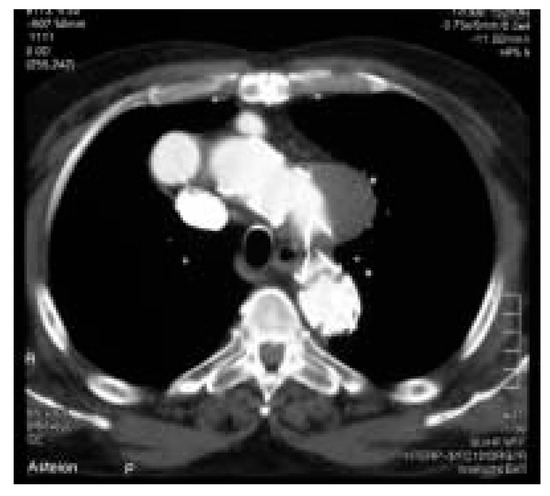
Figure 6.
Postoperative CT-scan (in patient from Figure 1) showing complete exclusion of the aneurysm in the mid-aortic arch.
Clinical follow-up extends up to 30 months and has been uncomplicated in all patients. CT-scan at 6 months demonstrated complete exclusion of the arch lesion in all cases and did not reveal any persisting endoleak.
The young patient with coarctation recovered extremely well without any cardiac, neurologic or bleeding complication and was discharged after one week of hospitalisation. At 6 months follow-up she did well and had a normal blood pressure (systolic pressure 110) both at rest and at exercise under a mild dosage of beta-blocker. Postoperative magnetic resonance imaging demonstrated a patent aortic bypass and the complete exclusion of the pseudoaneurysm (Figure 7).

Figure 7.
Postoperative MR-angiography shows the patent ascending-to-descending aortic bypass, an ascending aorta-to-left carotid bypass and the transposition of the left subclavian artery to the left carotid artery.
Comment
The feasibility of stent graft repair for aneurysms and dissection of the descending aorta has been documented and some agreement exists regarding the major constraints necessary to assure success [5,6,7,8,9,10]. Dake first reported the clinical feasibility of endovascular repair with Dacron-covered, self-expanding stainless steel straight stent grafts in 13 cases with descending aortic aneurysms [6]. As thoracic aneurysms have become more ubiquitous, the demand for less invasive strategies has increased recently. However, only a minority of patients is presently suitable for endovascular treatment, because stent graft repair requires adequate proximal and distal landing zones, which are not always available in this region.
Different types of branched stent-grafts to treat aortic arch aneurysms have been developed but only partial repair of the arch was performed with intentional covering of the left carotid and subclavian artery origins so far [5,6]. Inoue developed different types of branched stent graft to treat aortic arch aneurysms [9]. However in this series, 14 of 15 patients had distal arch stent graft placement only, including the subclavian artery with a singlebranched stent graft while total arch reconstruction with a triple branched graft was performed in one patient and was followed by a perigraft leakage.
The present experience demonstrates that a complete repair of the aortic arch to treat aneurysmatic or atherosclerotic lesions is feasible through a combined surgical/endovascular approach which does not require extracorporeal circulation with its inherent risks. The antegrade or retrograde introduction and deployment of the stent-graft to cover the aortic arch is performed only after reconstruction and proximal oversewing of the supraaortic vessels. This eliminates so far in the majority of the cases the risk of cerebral embolism during introduction and deployment of the stent graft. This approach seems to be reasonable in patients judged to be at high-risk for conventional surgical repair because of age and/or severe coexisting morbidity and in those who refuse a conventional approach. However, a diffuse cerebral but also spinal ischaemia occurred in a 60-year-old male with extremely severe atheromatosis of the aortic arch and of the proximal segment of the supraaortic vessels as well.
The prevalence of recurrent coarctation varies widely from 7 to 60% [11]. In uncomplicated cases, the standard approach is percutaneous balloon dilatation and stenting [12]. However, in the presence of diffuse tubular hypoplasia of the aortic arch or in case of aneurysmatic lesions from previous interventions, this approach cannot be recommended. Most of the procedures performed directly on the narrowed segment require cardiopulmonary bypass and extensive dissection of the adjacent structures to the aorta with a significant risk of injury to the recurrent and phrenic nerves and perioperative bleeding. Extra-anatomic ascending-to-descending aortic bypass represent a valid alternative because it does not need local dissection, nor cross-clamping of the diseased aortic segments, nor cardiopulmonary bypass, and yields excellent mid-term results [13,14]. Some patients with a re-coarctation have rather a hypoplasia of the aortic arch than restenosis at the original coarctation site. This might be due to inadequate initial repair or inappropriate growth of the anastomosis and in some cases of the aortic arch.
We described earlier the advantages of a combined surgical-endovascular approach for traumatologic pathologies [15]. In complex aortic coarctation, extra-anatomic aortic bypass combined to partial debranching of the supraaortic vessels allowed to obtain a normal perfusion to the low part of the descending aorta with restoration of a normal pressure in the head and in the upper extremities. The endovascular approach completely excluded the pseudoaneurysm at the previous site of coarctation repair. Transposition of the left subclavian to the left carotid artery restored antegrade flow and was performed through the same incision. CPB was not necessary for nay step of this complex procedure.
Symptomatic atherosclerotic lesions of the aortic arch and aneurysms localised in the proximal and middle segments of the aortic arch will constitute the main lesions to be considered for this procedure [16]. Minimising the surgical approach may include debranching of the supraaortic branches through a combined cervical and superior sternotomy.
We have used intraoperative angiography to assess proper aneurysm exclusion in all cases. However, intravascular ultrasound may be considered as an appropriate alternative even though it would introduce an additional expensive technology, which is not necessary for treatment of such lesions.
In selected patients, the combined surgical/endovascular complete debranching of the aortic arch represents an attractive concept with the potential to improve significantly the perioperative outcome; so far the risks of prolonged cardiopulmonary bypass, deep hypothermia, circulatory arrest as well as the majority of surgical manipulations on the aortic arch are eliminated. Assuming that technical refinements may improve all steps of the endovascular intervention, this combined approach may turn out to be the preferred therapeutic modality to repair aortic arch lesions in patients with multiple co-morbidities who otherwise would not be candidates for a conventional operative repair. However, longterm observation is necessary to confirm the stability of this type of repair.
References
- Crawford, E.S.; Svensson, L.G.; Coselli, J.S.; et al. Surgical treatment of aneurysm and/or dissection of the ascending aorta, transverse aortic arch and ascending aorta and transverse aortic arch. Factors influencing survival in 717 patients. J Thorac Cardiovasc Surg 1989, 98, 659–674. [Google Scholar] [CrossRef] [PubMed]
- Hagl, C.; Ergin, M.A.; Galla, S.D.; et al. Neurologic outcome after ascending aorta/aortic arch operations: effects of brain protection technique in high risk patients. J Thorac Cardiovasc Surg 2001, 121, 1107–1121. [Google Scholar] [CrossRef] [PubMed]
- Westaby, S.; Katsumata, T.; Vaccari, G. Arch and descending aortic aneurysms: influence of perfusion technique on neurological outcome. Eur J Cardiothorac Surg 1999, 15, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Kazui, T.; Washiyama, N.; Muhammad, B.A.; Terada, H.; Yamashita, K.; Takinami, M. Improved results of atherosclerotic arch aneurysm operations with a refined technique. J Thorac Cardiovasc Surg 2001, 121, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K.; Iwase, T.; Sato, M.; et al. Clinical application of transluminal endovascular graft placement for aortic aneurysms. Ann Thorac Surg 1997, 63, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Dake, M.D.; Miller, D.C.; Seimba, C.P.; et al. Transluminal placement of endovascular stent-grafts for the treatment of descending thoracic aortic aneurysms. N Engl J Med 1994, 331, 1729–1734. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R.C. Stent grafts for the thoracic aorta: a new paradigm? Ann Thorac Surg 2002, 74, S1818–20. [Google Scholar] [CrossRef] [PubMed]
- Nienaber, C.A.; Fattori, R.; Lund, G.; et al. Nonsurgical reconstruction of thoracic aortic dissection by stent-graft placement. N Engl J Med 1999, 340, 1539–1545. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K.; Hosokawa, H.; Iwase, T.; et al. Aortic arch reconstruction by transluminally placed endovascular branched stent graft. Circulation 1999, 100 (Suppl. SII), II316–II321. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Criado, F.J.; Clark, N.S.; Barnatan, M.F.; et al. Stent-graft repair in the aortic arch and descending thoracic aorta: a 4-year experience. J Vasc Surg 2002, 36, 1121–1128. [Google Scholar] [CrossRef] [PubMed]
- Amato, J.J.; Douglas, W.I.; James, T.; Desai, U. Coarctation of the aorta. Semin Thorac Cardiovasc Surg 2000, 3, 125–141. [Google Scholar] [CrossRef] [PubMed]
- Magee, A.G.; Brzezinska, G.; Qureshi, S.A.; Rosenthal, E.; Zubrzycka, M.; Ksiazyk, J.; et al. Stent implantation for aortic coarctation and recoarctation. Heart 1999, 82, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Kanter, K.R.; Erez, E.; Williams, W.H.; Tam, V.K. Extra-anatomic bypass via sternotomy for complex aortic arch stenosis in children. J Thorac Cardiovasc Surg 2000, 120, 885–890. [Google Scholar] [CrossRef] [PubMed]
- Connolly, H.M.; Schaff, H.V.; Izhar, U.; Dereani, J.A.; Warnes, C.A.; Orszulak, T.A. Posteriorpericardial ascending-to-descending aortic bypass: an alternative surgical approach for complex coarctation of the aorta. Circulation 2001, 104, 1133–1137. [Google Scholar] [CrossRef]
- Carrel, T.; Dai-Do, D.; Müller, M.; et al. Combined endovascular and surgical treatment of complex traumatic lesions of the thoracic aorta. Lancet 1997, 350, 1146. [Google Scholar] [CrossRef] [PubMed]
- Schmidli, J.; Do, D.; Triller, J.; Carrel, T. A less invasive approach to completely repair the aortic arch. Ann Thorac Surg 2005, in press.






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2005 by the author. Attribution - Non-Commercial - NoDerivatives 4.0.