Abstract
We present a case of recurrent takotsubo syndrome with contemporary brady- and tachyarrhythmic presentation, a rare clinical pattern for which the correct treatment is still a matter of debate.
Introduction
Takotsubo syndrome (TTS) is an acute nonischemic cardiomyopathy whose main feature is a typical left ventricular dysfunction usually involving the apical or, less frequently, midventricular or basal segments [1]. Although the underlying pathophysiology remains unknown, there is evidence in the literature for the association between TTS and arrhythmias such as ventricular tachycardias, torsade de pointe, atrial fibrillation, and atrioventricular (AV) node conduction disturbances [2]. The latter is reported in less than 3% of cases. However, an acute manifestation of TTS with a total AV block accounts for only 0.5–1% of cases in the literature [3,4], and in some of these, it is unclear whether TTS is the cause or a consequence of the complete AV block [5]. Furthermore, the optimal management of patients with advanced or complete AV block, as well as the right time to implant a pacemaker (PM), is still a matter of debate.
Case Description
We present the case of an 89-year old female patient who was referred to the emergency department for dizziness and presyncopal events that had begun about two days earlier. During the collection of her recent medical history, she reported a severe psychological trauma about three days prior, with severe chest pain followed by a progressive decrease in pain and the appearance of dizziness, widespread weakness, and presyncopal events. Her previous medical history included an episode of TTS three years earlier with a typical presentation (chest pain, widespread ST-elevation without specularity, prolonged QT interval) and angiographical documentation of normal coronary arteries.
The electrocardiogram (ECG) revealed a complete AV block with a wide QRS ventricular escapement (Figure 1A). A previous ECG recorded two years prior showed a sinus rhythm with a low-amplitude P wave, a first-degree AV block, and a complete right bundle branch block associated with a left anterior fascicular block with a QRS duration of more than 150 ms.
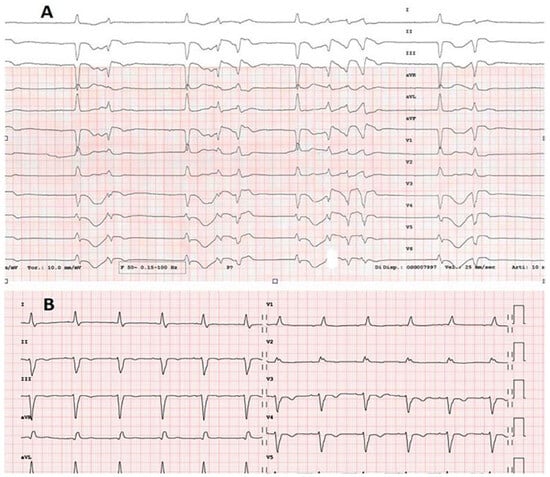
Figure 1.
(A) Twelve-lead electrocardiogram (ECG) reveals complete atrioventricular (AV) block with wide QRS ventricular escapement, premature ventricular beat and polymorphic non-sustained tachycardia. (B) Twelve lead ECG recorded after left ventricular function recovery reveals sinus rhythm with first degree AV block, right bundle branch block and left anterior fascicular block.
The echocardiogram showed severe systolic dysfunction with akinesia of all apical and hypercontractility of the basal segments (Figure 2). The initial troponin I level was 272 ng/l (upper limit of normal <14 ng/l). Electrolytes were within normal range. Other labor tests, such as blood cell count, liver and kidney function, were within normal range. The patient presented with multiple episodes of non-sustained polymorphic bradycardia-dependent ventricular tachycardia, resulting in hemodynamic instability. Based on the data collected, a TTS relapse with an atypical presentation characterized by complete AV block and bradycardia-induced tachyarrhythmias was diagnosed. A temporary transjugular PM was implanted in the right ventricle. Ventricular tachycardias no longer occurred when setting a pacing rate above 80 bpm.
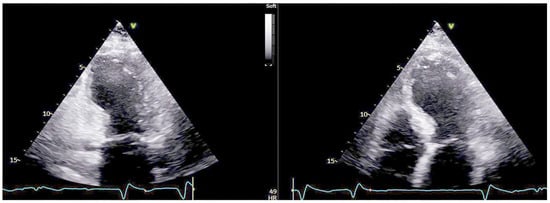
Figure 2.
Transthoracic echocardiogram at admission showing the typical apical ballooning pattern.
The diagnosis of takotsubo syndrome was confirmed by the almost complete restoration of the systolic function in the following days and the troponin curve trend, which showed a relatively modest area under the curve in comparison to the severe akinesia documented on the echocardiogram. These signs and humoral alterations are included in the InterTAK (international takotsubo) diagnostic criteria [6], which aid in the identification and stratification of TTS. In this case, the patient clearly met two out of eight InterTAK criteria (echographic transient left ventricular dysfunction and elevation of cardiac biomarkers). During clinical observation, the patient fully recovered 1:1 AV conduction (Figure 1B), along with systolic function, within five days. However, because this was the second episode of TTS and due to the multi-fascicular disturbance on the ECG tracing, it was decided to implant a definitive dual-chamber PM, which was completed without any complications.
Discussion
It is known that one out of eight patients will have another acute episode of TTS within five years of the first event [7], so we must be aware that a recurrence of TTS can present differently in the same patient. Furthermore, even though it is a rare occurrence, cardiologists should be aware of this uncommon arrhythmic pattern of TTS, especially in patients with preexistent conduction disease.
Author Contributions
All the authors contributed to the conception or design of the work, drafting the work or revising it critically for important intellectual content; final approval of the version to be published.
Institutional Review Board Statement
Written informed consent was obtained.
Conflicts of Interest
The authors have no potential conflicts of interest to declare.
References
- Ghadri, J.R.; Wittstein, I.S.; Prasad, A.; Sharkey, S.; Dote, K.; Akashi, Y.J.; et al. International Expert Consensus Document on Takotsubo Syndrome (Part II): Diagnostic Workup, Outcome, and Management. Eur Heart J. 2018, 39, 2047–2062. [Google Scholar] [CrossRef] [PubMed]
- Syed, F.F.; Asirvatham, S.J.; Francis, J. Arrhythmia occurrence with takotsubo cardiomyopathy: a literature review. Europace 2011, 13, 780–788. [Google Scholar] [CrossRef] [PubMed]
- Le, M.T.; Grimard, C.; Varenne, O.; Jakamy, R.; Rosencher, J. Tako-Tsubo cardiomyopathy and high-degree atrio-ventricular block: do we need to wait left ventricular function recovery to implant a pacemaker? Int J Cardiol. 2014, 176, e56–e59. [Google Scholar] [CrossRef] [PubMed]
- Vavilis, G.; Y-Hassan, S. Atrio-ventricular block and takotsubo syndrome: A review illustrated with two case reports. Clin Case Rep. 2022, 10, e05417. [Google Scholar] [CrossRef] [PubMed]
- Di Valentino, M.; Moccetti, M.; Previsdomini, M.; Biasco, L.; Menafoglio, A. A rare complication of electric cardioversion in an elderly patient “Electrical Takotsubo”. Cardiovasc Med. 2018, 21, 78–81. [Google Scholar]
- Ghadri, J.R.; Wittstein, I.S.; Prasad, A.; Sharkey, S.; Dote, K.; Akashi, Y.J.; et al. International Expert Consensus Document on Takotsubo Syndrome (Part I): Clinical Characteristics, Diagnostic Criteria, and Pathophysiology. Eur Heart J. 2018, 39, 2032–2046. [Google Scholar] [CrossRef] [PubMed]
- Singh, T.; Khan, H.; Gamble, D.T.; Scally, C.; Newby, D.E.; Dawson, D. Takotsubo Syndrome: Pathophysiology, Emerging Concepts, and Clinical Implications. Circulation Erratum in: Circulation. 2022, 145, e1053. 2022, 145, 1002–1019. [Google Scholar] [CrossRef] [PubMed]


© 2024 by the author. Attribution - Non-Commercial - NoDerivatives 4.0