Abstract
The first artificial pacemaker was implanted 51 years ago. Considerable progress has been made in recent decades and pacemakers have become fully automated cardiac rhythm management (CRM) systems representing a new, growing, and important set of therapies constituting a challenge for cardiologists and family practitioners. In the 25th year since the first implant of an automatic defibrillator (ICD) in Switzerland the present review puts the key CRM developments into perspective and is intended as a contribution to improved understanding and thereby management of patients under electrical therapy of the heart, a growing domain that is evolving towards a tool for full cardiac (and other) disease management. With the initial aim of preventing Adams-Stokes attacks by implanting a pacemaker with an electrode sutured on the heart, pacemakers have evolved to become devices able to automatically sense, analyse, and deliver appropriate electrical therapy against cardiac arrhythmias in their different forms. Automatic atrial and/or ventricular pacing, cardiac resynchronisation for correction of heart failure, and defibrillation for primary or secondary prevention of sudden cardiac death have demonstrably improved clinically important endpoints such as quality of life, symptom relief, hospitalisation rate and mortality. The increasing number of studies with documented endpoint reductions has resulted in corresponding treatment recommendations in the form of guidelines. The complexity of the indications and individual CRM programming possibilities, combined with the growing prevalence of patients seen to be benefiting from CRM in daily practice, has revealed the need for practising physicians to stay abreast of latest developments and be able to counsel their patients adequately. New ways of controlling vital signs via multiple sensors open the way to automatic remote and permanent assessment of many patient- or device-related parameters and thereby remind us of the importance of understanding the basic physiology of haemodynamics and cardiac function.
Introduction
The present publication revisits the evolution of electrical therapy since the first implantation of a cardiac pacemaker [1] and honours the memory of Prof. Senning (Figure 1). His pioneering genius has brought rapid growth in applications and technical perfection during recent decades: evolving from cardiac surgery, electrical pacemaker therapy has broadened its scope to become the domain of “clinical electrophysiology”, now a specialist domain of cardiology. Today these treatments include bradycardic and tachycardic rhythm disorders, with heart failure (now accessible to cardiac resynchronisation therapy) and ventricular tachycardias and fibrillation becoming intrinsically tied to the therapeutic concept of “pacing”, resulting in the transition from a pacemaker device to a “cardiac rhythm management system”. As the complexity and the therapeutic range of these devices widens to include more diagnostic and monitoring features, the term “cardiac electronic implanted device” (CIED) is now also in use.
Figure 1.
Ake Senning (1915–2001), on 8 October 1958, in Stockholm.
Cardiac rhythm management system
Electronic system including the following components: Power Source + electronics + sensors + diagnostics + data memory + appropriate electric impulses + electrodes + telemetry + modem + programming deviceable
Normal heart rhythm
Sinus node tissue exhibits the specific ability to generate an automatic rhythm, at a dominant pace, under normal conditions. Therefore the natural rhythm originates in this region (primum movens). Spontaneous electrical discharge, i.e., automatic rhythm, may also occur in the atrioventricular (AV) node, representing a secondary pacemaker which may be a backup at its own (lower) rate in cases of sinus rhythm failure. In addition, tertiary centres capable of generating an automatic rhythm exist in the peripheral Purkinje network and may develop under pathological circumstances such as ischaemic, metabolic or structural heart tissue damage or degeneration. This ectopic appearance of electrical impulses may be responsible for single extrasystole or rapid ectopic focal arrhythmia.
The impulses generated by the sinus node spread across the atria, causing their contraction and following privileged, albeit anatomically not clearly identifiable, conduction pathways leading to the AV node. In the AV node, the excitation wave is delayed and synchronised so that a single impulse is forwarded to the His bundle. The latter subdivides into the Tawara branch and further to the Purkinje system, which ensures an electrically and mechanically coordinated excitation of both ventricles.
Modern rhythm management encompasses substitution or correction of deficient impulse generation or conduction, which means that modern pacemakers are able to substitute a defective sinus node and bridge intra-atrial, atrioventricular or intraventricular conduction disorders, as well as controlling accelerated rhythms, tachycardias or fibrillation by means of tiered pacing manoeuvres or high energy defibrillation shocks.
The pacemaker (PM)/implantable cardioverterdefibrillator (ICD) and cardiac rhythm management system (CRM)
The basic concept of a PM/CRM relies on detection, signal processing and subsequent adequate discharge of electrical energy while signal and impulse transmission are ensured by one or more electrodes. Initially these devices were “handmade” by devoted engineers (Figure 2).

Figure 2.
First Swiss built Pacemaker by Dr Ing. Istvan Babotai. Dr Babotai custom-made Pacemaker about 1965.
The discharge (stimulus—shock)
Conceptually, the goal of any pacemaker is to ensure adequate activation of the atria and/or the ventricles in place of a defective physiological rhythm generator and/or conduction pathway. The excitability of a cell follows an all-or-none principle depending upon its instant depolarisation/repolarisation status at the time of impulse application and upon the applied energy load. The diastolic excitability threshold of resting myocardium should be below 1 V for a stimulus lasting 0.5 msec, depending on the electrode’s positioning and characteristics. To reverse the chaotic activation seen during ventricular fibrillation, the required voltage is much higher and requires approximately 500 V during 3.0 msec, which corresponds to an energy load of 30 joules.
Before the system can attempt to correct activation or conduction disorders it needs to diagnose the type and level of this disorder, i.e., it must be able to sense. This is achieved through measurement and monitoring of the endocardial signal which generally has an intensity of few mV only.
Although the key for understanding modern pacemaker technology is hidden in its electronic module and software, information remains accessible via its diagnostic module and programmed reactions to changes in the rhythm. Thus, the type of reaction to sensed signals will depend upon the possibilities and settings of its inbuilt electronics, which should be as flexible as possible to allow for customised programming in all clinical situations encountered.
Detection (sensors)
The diagnostic module must permanently analyse the heart rhythm and be able to deliver an accurate diagnosis of any arrhythmic event so that the pulse generator can react correctly. This can be extremely challenging, e.g., in differentiating between fast atrial fibrillation and ventricular tachycardia, which is the reason why all systems rely on sensors to monitor not only QRS but also various other parameters.
Data on intrinsic electrical activity are sampled in close-loop or Holter-like fashion and various derived indexes (pulse variations, regularity, APB and VPB, etc.) in order to serve as arrhythmia monitoring and baseline for appropriate pacemaker reaction. Moreover, an adaptation of the originally fixed basic pacing rate was developed on the basis of various parameters. The signals considered for adaptation of pacemaker rate include central venous temperature, blood-pH, oxygen saturation, QT interval, physical activity, intracardiac acceleration dp/dt, intrathoracic impedance, minute ventilation, etc. have been evaluated alone or in combination as blended sensors [2] to be able to adapt heart rate to metabolic demand. In addition, pure rhythm monitoring devices exist that are capable of recording and diagnosing rhythm disorders over several months to years. These may prove especially helpful for aetiological diagnosis of unexplained episodes of dizziness, identifying intermittent atrial fibrillation [3] and detecting causes of syncope [4]. With the increasing importance of cardiac resynchronisation therapy and therefore the care of patients with heart failure, continuous monitoring of intracardiac pressures and fluid status may become a critical annex for therapeutic decisions in patient care [5], and attention has recently been focused on heart sounds where intensity could be related to dp/dt [6]; so auscultation is back.
This extreme diversity, together with its corollary of multiple possibilities [7], shows how recent developments have led to an encompassing diagnostic and therapeutic concept which represents a considerable challenge for the fields of cardiology and sometimes medicine in general, for example correlation of rhythm disturbance and sleep disorders [8].
The logical inference from the above is that modern pacemakers will only perform as well as they were programmed, “well”-describing their ability to substitute as completely and physiologically as possible the defective functions previously discussed. Maximal individualised tailoring of all parameters being one of the key requirements for modern pacemakers, it is not surprising that the resultant range of possible settings exceed the capabilities and time allocation possibilities of even the most thorough cardiologist [9].
This is why future pacemakers will become more user-friendly and offer automatic programming of settings required for different functions.
To describe and harmonise understanding of potential functions of a CRM, a pacemaker/defibrillatorcode was defined by international authorities and last updated in 2002 (Table 1) [10].

Table 1.
The NBG Code.
Haemodynamics of pacemaker therapy
From the early days of pacing there was interest in the haemodynamic consequences of the paced rhythm. After solving the deadly threat of Adams-Stokes attacks, the loss of synchronised atrial contraction in VOO or VII pacemakers provoked discomfort. Also, in order to optimise the effectiveness of ventricular contraction, nature has developed the atrial systole. The atria not only optimise ventricular filling but also optimise enddiastolic wall tension, lower mean venous pressure in lung capillaries and V. cava. Studies on the physiological heart cycle leave no doubt about the fact that the atrial systole is of critical haemodynamic importance. The atria contribute to ventricular filling, an effect which becomes increasingly important as diastolic myocardial characteristics worsen. This late diastolic “atrial kick” closes the AV valves and prevents the valvular regurgitation seen in atrioventricular dyssynchrony [11]. Even if the heart, at least in the short term, can accommodate without an atrial systolic fraction of this kind, it needs to compensate for insufficient ventricular filling by increasing contractility and heart rate, both leading to ventricular overload and dilatation in the long term [12,13,14].
In bradycardia, cardiac output can be preserved or augmented by increasing the ejection volume. However, contractility and elasticity reserves decrease with increasing age of the patient. Furthermore, reduced rate responsiveness is frequently observed in the elderly, meaning that patients requiring pacemaker therapy will need to benefit from the possibility of an adaptive heart rate in order to improve or to optimise their cardiac output.
Rate
In cases of increased metabolic demand, the cardiac output (CO) must increase to an adequate extent. The simple formula: CO = stroke volume × heart rate is valid under the premiss of sufficient diastolic ventricular filling. Under fixed rate conditions, for example, the heart must increase its stroke volume to accommodate increased metabolic demand, and if the contractility reserve is limited CO can only be adapted by accelerating the heart rate. This essential fact is often forgotten in discussions of rate-responsive pacemakers, and becomes clinically relevant in patients with aged or diseased hearts. As an example, young healthy individuals in resting supine position tolerate ventricular pacing within a heart rate range of 30–180 bpm at an unchanged CO. In aged hearts, this range is considerably narrowed, and heart rates below 60 or above 110 bpm can lead to a reduction in CO.
The optimal heart rate is therefore the rate where the highest CO is achieved at the lowest myocardial workload [15]. The sensors described above are intended to permanently adapt the pacing rate, be it during sleep, exercise or cardiac decompensation [16].
AV sequence
Assuming normal sinus node function, atrium-driven ventricular pacemakers respect the requirements of rate responsiveness and AV sequence. Atrial contraction not in phase with the ventricles leads to atrial dilatation, setting the scene for subsequent development of atrial fibrillation. Studies on the physiological cycle of heart movements leave us in no doubt that the timed atrial systole is of equal critical haemodynamic importance to rate. Many publications have also reported improved physical performance in physiologically paced patients, and further support the above statements [17,18]. These two elements are supported by the observations according to which atrial-driven ventricular stimulation also prevents severe complications in the long term, such as heart failure, atrial fibrillation, thromboembolism and stroke [19,20,21]. The first pacemaker to resolve AV sequence as well as rate adaptation was built in 1986 (Figure 3).
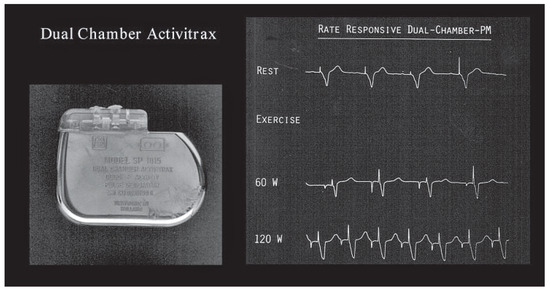
Figure 3.
First dual chamber rate responsive pacemaker. From: Vogt P, Herpers L, Kappenberger C. Single versus Dual chamber rate responsive cardiac pacing. PACE 1986;11:1896–901.
PM-induced dyssynchrony
The effects of ventricular pacing on contractility were initially described in patients with hypertrophic cardiomyopathy. These observations suggested that the effects of electrical cardiac stimulation went beyond rhythm control and had broader implications for activation, contraction and relaxation of the heart [13].
On the other hand the pacing-induced interventricular dyssynchrony during RV pacing represents a loss of energy and results in an increased cardiac workload which could promote the development of heart failure. This hypothesis is supported by echocardiographic observations in patients with a left bundle branch block, showing that cardiac working capacity was reduced due to paradoxical septal wall motion [13,14]. Starting from these observations, fears arose that traditional right ventricular pacing may have long-term deleterious effects on heart function [14,23]. They were further fuelled by the findings of clinical trials, such as the DAVID trial (ICD with VVI) [22], showing increased mortality in excessively paced patients (who may not have needed any pacing at all!). Similarly, the MOST study [23] showed increasing hospitalisation rates in ventricular-paced patients with sinus node disease.
The indications for electrical therapy of the heart are constantly evolving. Classical indications, such as sinus node disease with syncope and AV-block with Adams-Stokes attacks, are well accepted, though their effect on mortality endpoints never was and never will (who would dare today?) be proven according to evidence-based medicine criteria. The established “physiological” dual chamber pacing which restores heart rate and sequence, as described above, has proved its superiority vs. single chamber pacing in terms of improvement of quality of life and reduction of atrial fibrillation events in observational studies and prospective trials [19,24,25].
As the Danish long-term study showed, deleterious effects of inappropriate ventricular pacing could be avoided by using purely atrial pacing, which afforded the best long-term results in preventing heart failure, atrial fibrillation and mortality [19]. The annual risk of developing an AV block was estimated at around 0.6%/year [20], which should encourage the use of atrial pacing whenever possible. However, this is not what happens. Some concern may arise regarding inappropriate AV delays, leading, as could be anticipated, to haemodynamic consequences [26,27]. By using hysteresis, managed ventricular pacing (MVP), slowing baseline heart rate at night, and using “mode switch” in cases of atrial tachycardia, unnecessary ventricular pacing can be avoided while offering ventricular backup if needed. The fear of worsening ventricular function with ectopic right ventricular pacing and its suggested potential long-term deleterious effects, observed in only about 4% of the treated patients, seems exaggerated [13,28]. Nevertheless, research is still ongoing for even more physiological pacing localisations (septum, His bundle and left ventricle).
Resynchronisation
One common characteristic of many dilatative cardiomyopathies is a conduction delay, as evidenced by widening of the QRS complex. The latter generally points to the existence of an underlying mechanical dyssynchrony in ventricular contraction, but it may be difficult to know which came first, dyssynchrony or myopathy. Note however that a wide QRS does not necessarily imply underlying mechanical dyssynchrony, and that severe ventricular dysfunction may exist in the presence of normal QRS complexes [29]. Ventricular resynchronisation can improve heart function (ejection fraction, mitral regurgitation) but requires multifocal, at least right and left ventricular, pacing, e.g., with an electrode for left ventricular activation placed in a lateral cardiac vein through the coronary sinus or epicardial. Cardiac resynchronisation therapy (CRT) can allow for simultaneous contraction of the septal and free-left ventricular wall, and thus correct ventricular dyssynchrony with favourable effects on ventricular function (Figure 4 and Figure 5). After a proof of concept in a single patient [30] many reports and randomised controlled trials provided convincing evidence that CRT reflects a new approach to improvement of the failing heart muscle. Careful correlation between LBBB variation and mechanical contraction-sequence may lead to more specific selection of CRT candidates [13,29]. This may in part explain why individual response to cardiac resynchronization therapy may vary. However, numerous studies of heart failure populations have established the success of this therapeutic concept [31,32] firmly enough to justify its recommendation in the ESC guidelines for the treatment of heart failure [60], stating that cardiac resynchronisation therapy is indicated (evidence class IIA) in patients with a wide QRS complex >120 msec and an ejection fraction below 30–35%.
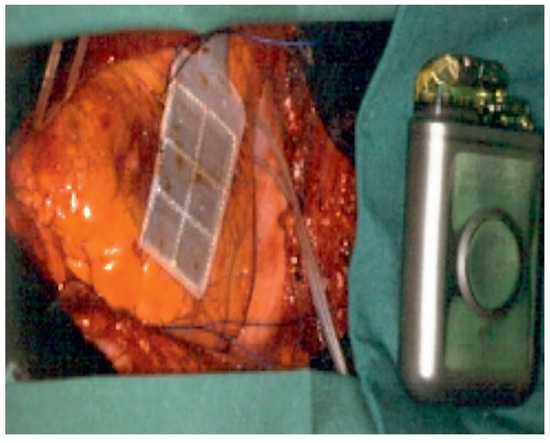
Figure 4.
The first Automatic Implantable Defibrillator in Switzerland (March 1984). Note the epicardial patch electrode that had to be implanted via thoracotomy and the defibrillator was placed in the abdomen under the diaphragme (USZ).
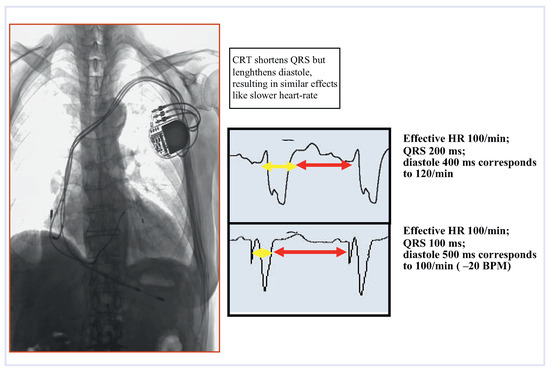
Figure 5.
The “mechanistic” concept of cardiac resynchronisation therapy (CRT). Note the LV electrode placed through the coronary sinus.
Areas of scientific uncertainty, such as indications for pacemaker therapy in early stages of heart failure, may still be open to discussion. To date, more than 100 studies of the effects of CRT are still ongoing. However, the concept that electrical stimulation is more than rhythm control is here to stay, and with CRT alone and combined with ICD the risk of heart failure events seems to be reduced even in relatively asymptomatic patients with a low ejection fraction and wide QRS complex [33,34,38].
Therapy of tachycardic arrhythmia
Today, electrical therapy of tachycardia is limited almost exclusively to defibrillation of ventricular tachycardia, but the theory of capturing reentry circuits with overdrive pacing has been applied in the past and may resurrect.
The general principle of applying an electric shock to reverse ventricular tachycardia and fibrillation was first observed in 1899 [35]. Michel Mirowski (Figure 6) first conceived the vision of an automatic implantable defibrillator (AID) [36]. With the awareness that antiarrhythmic drugs failed to meet important clinical endpoints, such as the prevention of sudden cardiac death [37], implantable “reanimators” met with increasing interest. In Switzerland the first automatic implantable defibrillator (AID) was implanted in 1984 (Figure 7). The analysis of rhythm disorders preceding sudden cardiac death events—generally monomorphic ventricular tachycardia—led to the combined application of antitachycardia pacing and defibrillation through a single device integrating an implantable pacemaker and cardioverter and defibrillator (ICD). The transvenous implant technique made wide application possible. Such a device now encompasses all current knowledge on tachycardia and delivers appropriate treatment in life-threatening situations in addition to bradycardia control and AV and VV synchronisation. It is indeed a cardiac rhythm management system.
Figure 6.
Prof. Michel Mirowski (1924–1990).
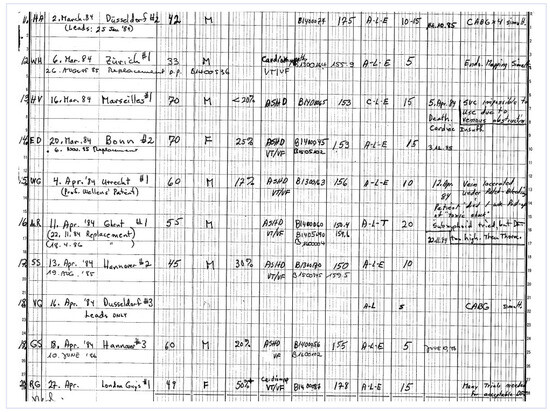
Figure 7.
The first ICD (AID) implant in Switzerland. Page from the personal agenda du Dr Seah Nisam documenting the first ICD implantation at University Hospital in Zürich on March 6th 1984 (by personal permission).
Automatic implantable defibrillators were initially intended for the treatment of patients who had survived an episode of ventricular fibrillation (secondary prevention) and were therefore considered to be at high risk of recurrence of ventricular fibrillation. Increasing device sophistication opened the way for use in primary prevention, as evidenced by the results from the large MADIT II trial [39]. Thereafter, guidelines recommended ICD for the treatment of patients with ischaemic cardiomyopathy and an ejection fraction below 30% [61]. On the other hand, it is worth remembering that the CABG Patch Study [40] of patients after coronary bypass operation showed no benefit from an ICD. As the device fulfills the concept of defibrillation with extreme reliability, it has to be stressed that in the trials under discussion patient selection and background therapies influence the outcome more than technical perfection. In this light historic trials may be obsolete today, as technology and diagnostics improve, but they should be remembered as milestones in the development of device therapy.
Patient and device follow-up
Follow-up of the device-treated patient is essential for clinical success and should therefore not be limited to technical control. Here the primary care physician and the attending cardiologist have a true medical mission. This means that during the follow-up visit (to be distinguished from the system interrogation), patient interrogation plays the central role. The task is to ensure that the primary goal of therapy—to improve symptoms, avoid syncopes, improve heart failure and not provoke side effects—is achieved. In addition, ICD patients need to be reassured concerning minimisation of sudden cardiac death risk, and comforted in the idea of having subscribed to the best existing life insurance. Discharge of an ICD is truly a shock (-event) and must be discussed with the patient and his relatives to facilitate coping and handling. This subject also needs to be addressed in view of the not inconsiderable amount of inappropriate discharges (about 8%/year). Adequate information on the usefulness and functioning of a defibrillator is therefore of crucial importance for the patients’ families. The general experience is that they are then very grateful indeed for the treatment [38].
The physical examination should focus on the implant scar, palpation should check the implant pocket and correct positioning of the device. A 12-channel ECG will show the baseline rhythm and document instant heart and pacemaker function. If CRT was implanted, specific attention should be given to the V1 lead, since R >S in V1 may already document adequate pacing of the left ventricle but other algorithms have been described [41]. Digital ECG recorders deserve specific attention as pacemaker impulses may not appear at all if outside recording frequency or stimulus artefact detectors inappropriately inscribe a stimulus where it has not occurred. Adequate filter modulation may correct this problem. The once universal magnet test may not be adequate outside the implanting centres, as magnet mode may have been switched off and the multiplicity of available devices preempts appropriate handling.
The functional integrity of the device is best-tested with the programming device, presupposing availability of adequate equipment and knowledge. Unfortunately, programmers remain device-specific and no universal equipment is available at present. The complexity of pacemaker, CRT and ICD settings and controls is such that the limits of practicability can be reached or even exceeded for a clinical setting [9]. This has produced the paradoxical situation that in specific situations default settings were shown to be equivalent to individual single item programming and customisation of an ICD [42].
Interrogation of the device memory goes far beyond status information on battery life and electrode integrity, but is indeed a full diagnostic procedure on the patient’s rhythm history. In recent years developments for telemonitoring have been successfully introduced [43] and these may be of help for patient survey in general and may even prove cost-effective [44,45] (Figure 8). The storage of significant events in the pacemaker’s memory may indicate “silent” arrhythmias or confirm discharges as reported by the patient, monitor physical activity and fluid balance in heart failure patients [46] or all the information gained from the above-mentioned sensors. This information will improve therapies offered to the patient and open a new dimension in patient care and clinical research, namely the remote continuous observation of a disease [61]. This is the point where the pacemaker of 50 years ago evolves into a disease management product, and finally we may end up with a cardiac implanted electronic device (CIED) even without electrical therapy features but purely diagnostic and monitoring functions.
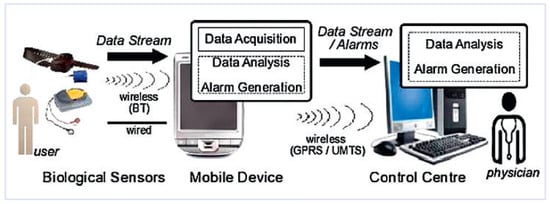
Figure 8.
The components of remote monitoring.
Not surprisingly, editorials call this the subject of the year [47]!
“Recalls”
Pacemakers, defibrillators and leads have an excellent safety track record (see manufacturers’ annual reports, since we lack sufficient alternative databases) and a reported extremely high reliability with less than one defective device per 10 000 patients per year [48]. However, component defects may trigger uncertainty and overreaction. Accurate, immediate, and professional briefing of all implanting centres and attending physicians is crucial for the prevention of “orchestrated panic attacks” in the lay public [49]. Transparency and communication are the keys to preventing this. Manufacturers’ attention can be drawn to system defects based on individual physician reports, so their role is not merely one of observation. If needful and appropriate, the manufacturer may then issue a memo, warning or, in extreme situations, a product recall. Unfortunately, there is no unified semantics and the English word “recall” triggers unnecessary fears and interventions. Such a recall in the sense of a “dangerous device” that needs explantation is only justified if a sudden unforeseeable drop in energy or dysfunction may be expected to expose a high proportion of patients to a lifethreatening risk. Pacemaker implant databases in all implanting centres and of all manufacturers allow for fast and accurate identification of defective batches and for early patient briefing, control visits and if necessary a decision on device replacement. Interestingly, in this situation a global clinical evaluation remains provenly superior to systematic device replacement [50,51], and watchful waiting is often wiser than hastily heroic device replacement.
Patient counselling
Life with a implanted device
Patients under pacemaker therapy frequently wonder what they are allowed to do and what not. As a general rule, a pacemaker or an ICD tolerates everything (beware however of strong magnetic fields). Hence the patients’ general health status should be the limiting factor. Sports should not be prohibited, even if opinions may diverge [52,53], as inappropriate therapy delivery has been reported more frequent during sports. As cases of death were not reported in parallel, these findings might be regarded as a proof of therapy efficacy. Whether sky jumping or scuba diving is appropriate should be left to the patient’s appreciation. Activities during which sudden incapacitation is not acceptable are prohibited (aircraft pilot, professional driver), also due to the risk of momentarily disabling inappropriate discharges. Unfortunately, but understandably, no data are available on these specific issues and not even on exercise testing with an ICD. There is currently no legal framework, outside professional limitations, for the physician to intervene otherwise than by detailed patient briefing and counselling; however, clear safety issues for patients with ICD have been published [54].
Electrosmog and pacemaker systems
Possible sources of electrical and electromagnetic interference are ubiquitous. Devices are increasingly resistant to such interference, but sources have become more perfidious. However, earlier taboos such as MRI examinations may now be breached with adequate electrodes and resistant systems [55].
Conclusion
Cardiac rhythm management (CRM) is the result of over 50 years of medical and technical progress in heart diseases related to electricity, yet I do not see evidence that this is a bygone era. Alternatives to pacemaker, resynchronisation or defibrillation do not exist today, but some hope on new therapies such as stem cells or new antiarrhythmic drugs such as multichannel blockers may offer a perspective. For the time being, the therapeutic solution for rhythm and heart failure disorders will increasingly depend on CRM systems. The constantly increasing implant rate reflects population trends and the prevalence of otherwise disabling cardiac diseases. Therefore this area is expected to continue to grow. Access to therapy rather than true financial issues or political directives seem to explain the huge geographic discrepancies [56]. Bearing in mind that even if for an individual patient the cost of therapy is not an issue, for the society cost impact may be high and demand prioritisation in the allocation of health care resources [57]. Again this is not the problem of the ill patient but a decision of its environment, say society.
In consequence, cardiologists and family practitioners will be increasingly exposed to the multiple aspects of implantable devices, and the potential of remote disease management will open new horizons for patient management in general. The challenge will be to merge this technical progress with the human dimension.
Acknowledgments
The author thanks Seah Nisam for the documentation of the first AID implant and B. von Segesser for the photographs of historic pacemakers.
Conflicts of Interest
Consultant to Medtronic and Schiller. Sponsored research by Schiller and Medtronic.
References
- Elmquist, R.; Senning, A. An Implantable Pacemaker for the Heart Medical Electronics. In Proceedings of the Second International Conference on Medical Electronics, Paris, 1959; Smyth, C.N., Ed.; Ilffe + Sons: London, 1959. [Google Scholar]
- Coman, J.; Freedman, R.; Koplan, B.A.; Reeves, R.; Santucci, P.; Stolen, K.Q.; Kraus, S.M.; Meyer, T.E.; LIFE Study Results. A blended sensor restores chronotropic response more favorably than an accelerometer alone in pacemaker patients: the LIFE study results. Pacing Clin Electrophysiol. 2008, 31, 1433–1442. [Google Scholar] [CrossRef]
- Hohnloser, S.H.; Capucci, A.; Fain, E.; Gold, M.R.; van Gelder, I.C.; Healey, J.; et al. Asymptomatic atrial fibrillation and stroke Evaluation in pacemaker patients and the atrial fibrillation reduction atrial pacing trial (ASSERT). Am Heart J. 2006, 152, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Krahn Andrew, D.; Klein George, J.; Yee, R.; Takle-Newhouse, T.; Norris, C. Use of an Extended Monitoring Strategy in Patients With Problematic Syncope. Circulation. 1999, 99, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Bourge Robert, C.; Abraham William, T.; et al. Randomized Controlled Trial of an Implantable Continuous Hemodynamic Monitor in Patients With Advanced Heart Failure. The COMPASS-HF Study. J Am Coll Cardiol. 2008, 51, 1073–1079. [Google Scholar] [CrossRef] [PubMed]
- Zuber, M.; Toggweiler, S.; Roos, M.; Kobza, R.; Jamshidi, P.; Erne, P. Comparison of different approaches for optimization of atrioventricular and interventricular delay in biventricular pacing. Europace. 2008, 10, 367–373l. [Google Scholar] [CrossRef]
- Benditt, D.G.; Mianulli, M.; Lurie, K.; Sakaguchi, S.; Adler, S. Multiple-sensor systems for physiologic cardiac pacing. Ann Intern Med. 1994, 121, 960–968. [Google Scholar] [CrossRef]
- Scharf, C.; Cho, Y.K.; Bloch, K.E.; Brunckhorst, C.; Duru, F.; Balaban, K.; Foldvary, N.; Liu, L.; Burgess, R.C.; Candinas, R.; et al. Diagnosis of sleep-related breathing disorders by visual analysis of transthoracic impedance signals in pacemakers. Circulation. 2004, 110, 2562–2567. [Google Scholar] [CrossRef]
- Schoenfeld, M.H. Manpower concerns in cardiac electrophysiology and pacing. Pacing Clin Electrophysiol. 1995, 18, 1977–1979. [Google Scholar] [CrossRef]
- Bernstein, A.D.; Daubert, J.C.; Fletcher, R.D.; Hayes, D.L.; Luderitz, B.; Reynolds, D.W.; Schoenfeld, M.H.; Sutton, R. The revised NASPE/BPEG generic code for antibradycardia, adaptive-rate and multisite pacing. Pacing Clin Electrophysiol. 2002, 25, 260–264. [Google Scholar] [CrossRef]
- Rutishauser, W.; Wirz, P.; Gander, M.; et al. Atriogenic diastolic reflux in patients with atrioventricular block. Circulation. 1966, 34, 807–817. [Google Scholar] [CrossRef]
- Reynolds, D.W.; Wilson, M.P.; Burrow, R.D.; Schaefer, C.F.; Lazzara, R.; Thadani, U. Hemodynamic evaluation of atrioventricular sequential versus ventricular pacing in patients with normal and poor ventricular function at variable heart rates and posture. J Am Coll Cardiol. 1983, 1, 636. [Google Scholar]
- Sweeney Michael, O.; Prinzen Frits, W. Ventricular Pump Function and Pacing: Physiological and Clinical Integration. Circ Arrhythmia Electrophysiol. 2008, 1, 127–139. [Google Scholar] [CrossRef]
- Lee, K.L.; et al. Adverse effect of ventricular pacing on heart failure and atrial fibrillation among patients with normal baseline QRS duration in a clinical trial of pacemaker therapy for sinus node dysfunction. Circulation. 2003, 107, 2932–2937. [Google Scholar]
- Levine, H.J. Optimum heart rate of large failing hearts. Am J Cardiol. 1988, 64, 633–636. [Google Scholar] [CrossRef] [PubMed]
- Duru, F.; Bloch, K.E.; Weilenmann, D.; Candinas, R. Clinical evaluation of a pacemaker algorithm that adjusts the pacing rate during sleep using activity variance. Pacing Clin Electrophysiol. 2000, 23, 1509–1515. [Google Scholar] [CrossRef] [PubMed]
- Karlof, I. Haemodynamic effect of atrial triggered versus fixed rate pacing at rest and during exercise in complete heart block. Acta Med Scand. 1975, 197, 195–206. [Google Scholar]
- Kappenberger, L.; Gloor, H.O.; Babotal, I.; et al. Hemodynamic effects of atrial synchronization in acute and long-term ventricular pacing. PACE. 1982, 5, 639. [Google Scholar] [CrossRef]
- Andersen, H.R.; Nielsen, J.C.; Thomsen, P.E.; Thuesen, L.; Mortensen, P.T.; Vesterlund, T.; et al. Long-term follow-up of patients from a randomised trial of atrial versus ventricular pacing for sick-sinus syndrome. Lancet. 1997, 350, 1210–1216. [Google Scholar] [CrossRef]
- Andersen, H.R.; Nielsen, J.C.; Thomsen, P.E.; Thuesen, L.; Vesterlund, T.; Pedersen, A.K.; Mortensen, P.T. Atrioventricular conduction during long-term follow-up of patients with sick sinus syndrome. Circulation. 1998, 98, 1315–21. [Google Scholar] [CrossRef]
- Connolly, S.J.; Kerr, C.R.; Gent, M.; Roberts, R.S.; Yusuf, S.; Gillis, A.M.; et al. Effects of physiologic pacing versus ventricular pacing on the risk of stroke and death due to cardiovascular causes. Canadian Trial of Physiologic Pacing Investigators. N Engl J Med. 2000, 342, 1385–1391. [Google Scholar] [CrossRef]
- The DAVID Trial Investigators. Dual-chamber pacing or ventricular backup pacing in patients with an implantable defibrillator: the Dual Chamber and VVI Implantable Defibrillator (DAVID) trial. JAMA. 2002, 288, 3115–3123. [Google Scholar] [CrossRef]
- Sweeney Michael, O.; Hellkamp Anne, S. Heart Failure During Cardiac Pacing. Circulation. 2006, 113, 2082–2088. [Google Scholar] [CrossRef]
- Toff, W.D.; Camm, A.J.; Skehan, J.D. Single-chamber versus dual-chamber pacing for high-grade atrioventricular block. N Engl J Med. 2005, 353, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Fored, C.M.; Granath, F.; Gadler, F.; Blomqvist, P.; Rynder, J.; Linde, C.; Ekbom, A.; Rosenqvist, M. Atrial vs. dual-chamber cardiac pacing in sinus node disease: a register-based cohort study. Europace 2008, 10, 825–831. [Google Scholar] [CrossRef] [PubMed]
- Plummer, C.J.; McComb, J.M.; STOP AF Trial. Detection of atrial fibrillation by permanent pacemakers: observations from the STOP AF trial. Card Electrophys Rev. 2003, 7, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Chirife, R.; Ortega, D.F.; Salazar, A.I. Nonphysiological left heart AV intervals as a result of DDD and AAI “physiological” pacing. Pacing Clin Electrophysiol. 1991, 14 11 Pt 2, 1752–1756. [Google Scholar] [CrossRef]
- Sweeney, M.O.; Hellkamp, A.S.; Ellenbogen, K.A.; Greenspon, A.J.; Freedman, R.A.; Lee, K.L.; Lamas, G.A. Adverse effect of ventricular pacing on heart failure and atrial fibrillation among patients with normal baseline QRS duration in a clinical trial of pacemaker therapy for sinus node dysfunction. Circulation. 2003, 23, 2932–2937. [Google Scholar] [CrossRef]
- Jansen, A.; Kirn, B.; Van Gelder, B.; Bracke, F.; Starc, V.; Prinzen, F.W. Myocardial internal strain fraction predicts volume response in patients with cardiac resynchronization therapy. Circulation. 2006, 114, Suppl. [Google Scholar]
- Cazeau, S.; Ritter, P.; Lazarus, A.; Gras, D.; Backdach, H.; Mundler, O.; Mugica, J. Multisite pacing for end-stage heart failure: early experience. Pacing Clin Electrophysiol. 1996, 19 11 Pt 2, 1748–1757. [Google Scholar] [CrossRef]
- Cazeau, S.; Leclercq, C.; Lavergne, T.; Walker, S.; Varma, C.; Linde, C.; Garrigue, S.; Kappenberger, L.; Haywood, G.A.; Santini, M.; et al. Multisite Stimulation in Cardiomyopathies (MUSTIC) Study Investigators. Effects of multisite biventricular pacing in patients with heart failure and intraventricular conduction delay. N Engl J Med. 2001, 344, 873–880. [Google Scholar] [CrossRef]
- Abraham, W.T.; Fisher, W.G.; Smith, A.L.; Delurgio, D.B.; Leon, A.R.; Loh, E.; et al. Randomized controlled trial of cardiac resynchronization in chronic heart failure. N Engl J Med. 2002, 346, 1845–1853. [Google Scholar] [CrossRef]
- Bristow, M.R.; Saxon, L.A.; Boehmer, J.; Krueger, S.; Kass, D.A.; De Marco, T.; et al. Comparison of Medical Therapy, Pacing and Defibrillation in Heart Failure (COMPANION) Investigators. Cardiac resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004, 350, 2140–2150. [Google Scholar] [CrossRef] [PubMed]
- Cleland, J.; Daubert, J.C.; Erdmann, E.; Freemantle, N.; Gras, D.; Kappenberger, L.; Tavazzi, L.; Cardiac Resynchronization-Heart Failure (CAREHF) Study Investigators. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005, 352, 1539–1549. [Google Scholar] [CrossRef] [PubMed]
- Prevost, J.-L.; Battelli, F. La mort par les décharges électriques. Journal de Physiol. 1899, 1, 1085–1100. [Google Scholar]
- Mirowski, M.; Reid, P.R.; Mower, M.M.; Watkins, L.; Gott, V.L.; Schauble, J.F.; et al. Termination of malignant ventricular arrhythmias with an implanted automatic defibrillator in human beings. N Engl J Med. 1980, 303, 322–324. [Google Scholar] [CrossRef]
- Echt, D.S.; Liebson, P.R.; Mitchell, L.B.; Peters, R.W.; Obias-Manno, D.; Barker, A.H.; et al. Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The Cardiac Arrhythmia Suppression Trial. N Engl J Med. 1991, 324, 781–788. [Google Scholar] [CrossRef]
- Moss, A.J.; Hall, W.J.; Cannom, D.S.; Klein, H.; Brown, M.W.; Daubert, J.P.; et al. Cardiac-Resynchronization Therapy for the Prevention of Heart-Failure Events (MADIT-CRT). N Engl J Med. 2009, 361, 1329. [Google Scholar] [CrossRef]
- Moss, A.J.; Zareba, W.; Hall, W.J.; Klein, H.; Wilber, D.J.; Cannom, D.S.; et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002, 346, 877–883. [Google Scholar] [CrossRef]
- Bigger, J.T., Jr. Prophylactic use of implanted cardiac defibrillators in patients at high risk for ventricular arrhythmias after coronary-artery bypass graft surgery. Coronary Artery Bypass Graft (CABG) Patch Trial Investigators. N Engl J Med. 1997, 337, 1569–1575. [Google Scholar] [CrossRef]
- Luderitz, B.; Jung, W.; Deister, A.; Marneros, A.; Manz, M. Patient acceptance of the implantable cardioverter defibrillator in ventricular tachyarrhythmias. Pacing Clin Electrophysiol. 1993, 16, 1815–1821. [Google Scholar] [CrossRef]
- Ammann, P.; Sticherling, C.; Kalusche, D.; Eckstein, J.; Bernheim, A.; Schaer, B.; Osswald, S. An electrocardiogram-based algorithm to detect loss of left ventricular capture during cardiac resynchronization therapy. Ann Intern Med. 2005, 142, 968–973. [Google Scholar] [CrossRef]
- Ricci, R.P.; Morichelli, L.; Santini, M. Home monitoring remote control of pacemaker and implantable cardioverter defibrillator patients in clinical practice: impact on medical management and health-care resource utilization. Europace 2008, 10, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Varma, N. Rationale and design of a prospective study of the efficacy of a remote monitoring system used in implantable cardioverter defibrillator follow-up: the Lumos-T Reduces Routine Office Device FollowUp Study (TRUST) study. Am Heart J. 2007, 154, 1029–1034. [Google Scholar] [CrossRef]
- Wilkoff, B.L.; Ousdigian, K.T.; Sterns, L.D.; Wang, Z.J.; Wilson, R.D.; Morgan, J.M. A comparison of empiric to physician-tailored programming of implantable cardioverter-defibrillators: results from the prospective randomized multicenter EMPIRIC trial. J Am Coll Cardiol. 2006, 48, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.M.; Wang, L.; Chau, E.; Chan, R.H.; Kong, S.L.; Tang, M.O.; et al. Intrathoracic impedancemonitoring in patients with heart failure: Correlation with fluid status and feasibility of early warning preceding hospitalization. Circulation. 2005, 112, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Kusumoto, F.; Goldschlager, N. Subject of the year: remote monitoring. J Interv Card Electrophysiol. 2009, 25, 89–90. [Google Scholar] [CrossRef][Green Version]
- Maisel, W.H.; Moynahan, M.; Zuckerman, B.D.; Gross, T.P.; Tovar, O.H.; Tillman, D.-B.; Schultz, D.B. Pacemaker and ICD generator malfunctions: analysis of Food and Drug Administration annual reports. JAMA. 2006, 295, 1901–1906. [Google Scholar] [CrossRef]
- Fuhrer, J. Kommentar der AG «Herzschrittmacher und Elektrophysiologie» der SGK. Zum Vorgehen bei Rückrufen kardialer Implantate Schweizerische 2007, 88, 10. [Google Scholar]
- Prystowsky Eric. Complications associated with Generator Replacement in Response to Device Directories. J Cardiovasc Electrophysiol. 2008, 19, 266–269. [Google Scholar] [CrossRef]
- Amin Mitesh, S.; Wood Mark, A.; Shepard Richard, K.; Kalahasy, G.; Ellenbogen, K. Clinical Judgement versus Decision analysis for Managing Device Advisories. PACE. 2008, 31, 1263–40. [Google Scholar]
- Lampert, R.; Cannom, D.; Olshansky, B. Safety of sports participation in patients with implantable cardioverter defibrillators: a survey of Heart Rhythm Society members. J Cardiovasc Electrophysiol. 2006, 17, 11–15. [Google Scholar] [CrossRef]
- Kobza, R.; Duru, F.; Erne, P. Leisure-time activities of patients with ICDs: findings of a survey with respect to sports activity, high altitude stays, and driving patterns. Pacing Clin Electrophysiol. 2008, 31, 845. [Google Scholar] [CrossRef]
- Epstein Andrew, E.; et al. Public Safety Issues in Patients With Implantable Defibrillators A Scientific Statement From the American Heart Association and the Heart Rhythm Society. Circulation. 2007, 115, 1170–1176. [Google Scholar] [PubMed]
- ACC; NASCI; SCMR; Levine, G.N.; et al. An American Heart Association Scientific Statement From the Committee on Diagnostic and Interventional Cardiac Catheterization Safety of Magnetic Resonance Imaging in Patients With Cardiovascular Devices. Circulation. 2007, 116, 2878–2891. [Google Scholar] [CrossRef] [PubMed]
- Wolpert, C.; Vardas, P. The Current Status of Cardiac Electrophysiology in ESC Members Countries. In The EHRA White Book; 2008. [Google Scholar]
- Szucs, T.D.; Kappenberger, L. ICD’s in congestive heart failure-is there bang for the beat? Cardiovasc Drugs Ther. 2004, 18, 95–98. [Google Scholar] [CrossRef] [PubMed]
- Haran, B.; David, S. Remote monitoring and follow-up of pacemakers and implantable cardioverter defibrillators. Europace. 2009, 11, 701–709. [Google Scholar]
- Available online: www.escardio/org guidelines.
- Available online: www.hrsonline.org guidelines.
- Zile, M.R.; Bennett, T.D.; St John Sutton, M.; Cho, Y.K.; Adamson, P.B.; et al. Transition from chronic compensated to acute decompensated heart failure: pathophysiological insights obtained from continuous monitoring of intracardiac pressures. Circulation. 2008, 118, 1433–1441. [Google Scholar] [CrossRef]









© 2010 by the author. Attribution-Non-Commercial-NoDerivatives 4.0.