Geo-Relationship between Cancer Cases and the Environment by GIS: A Case Study of Trabzon in Turkey

Abstract
:1. Introduction
2. Method
2.1. Background: Cancer Registry Process in Turkey
2.2. Geographical Information Systems and Cancer Maps
2.3. The Registration Process of Cancer Cases in Turkey
2.4. The Study Area
2.5. Data Collection and Organization
2.6. Statistical Analysis
3. Results and Discussion
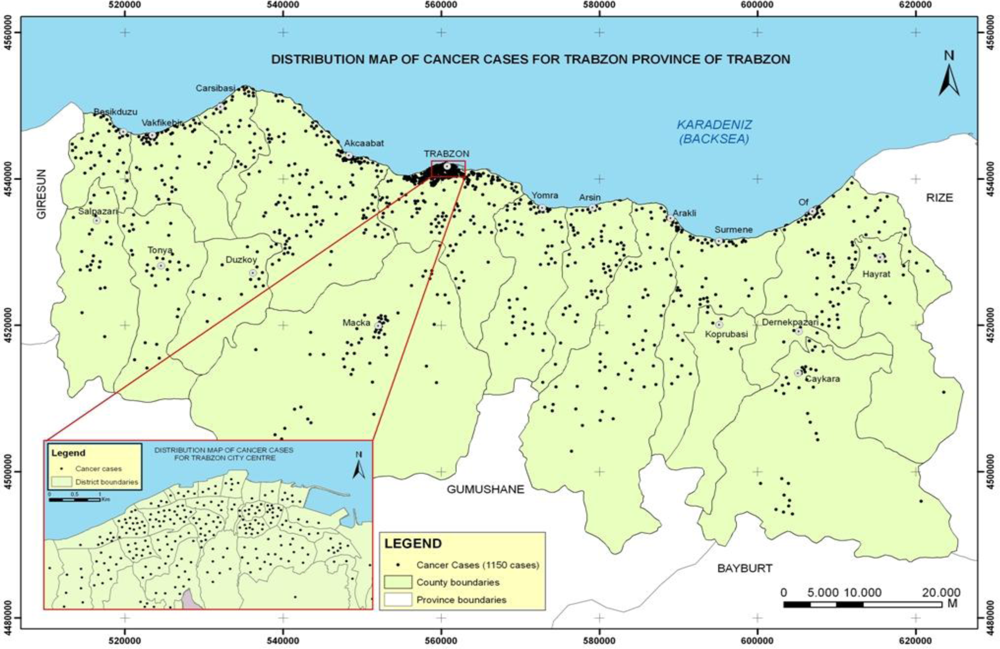
3.1. Mapping of the Distribution of Cancer Cases
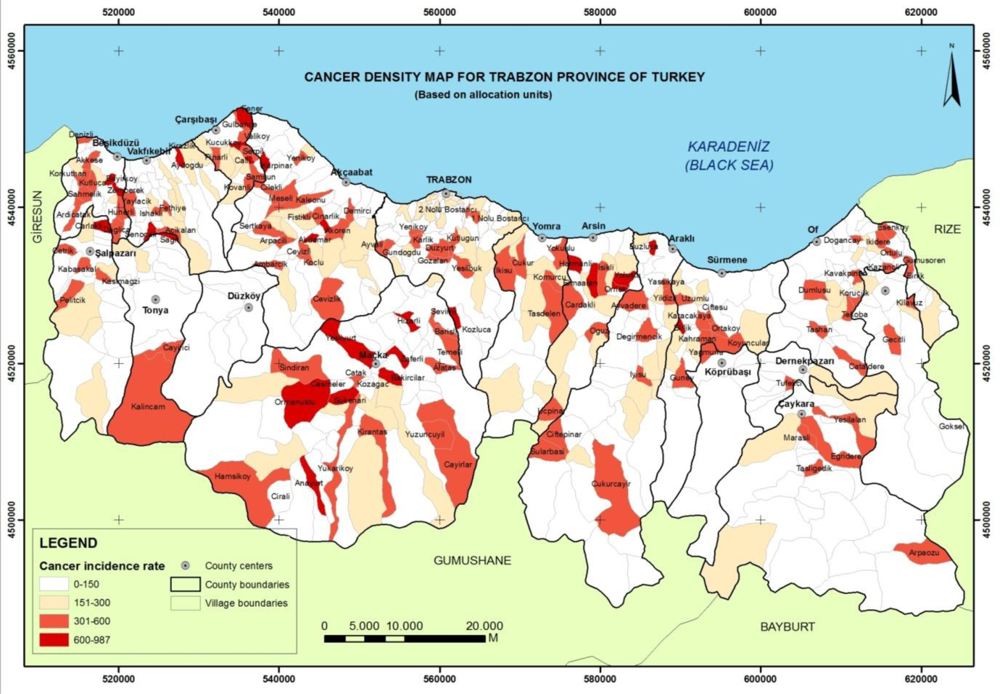
3.2. The Cancer Incidence Map
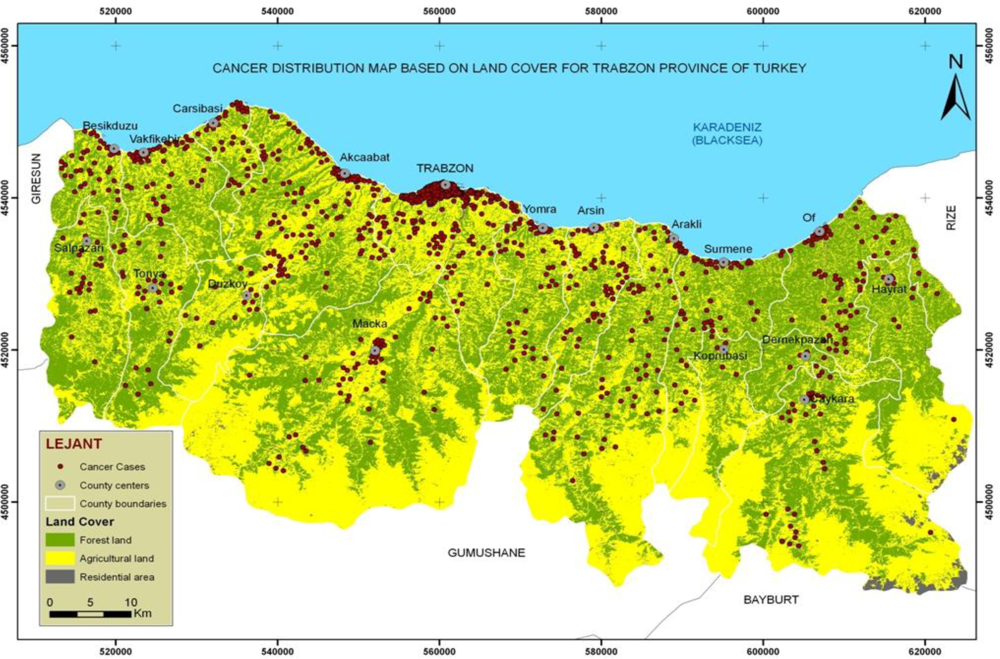
3.3. Relationship between the Cancer Cases and Land Cover
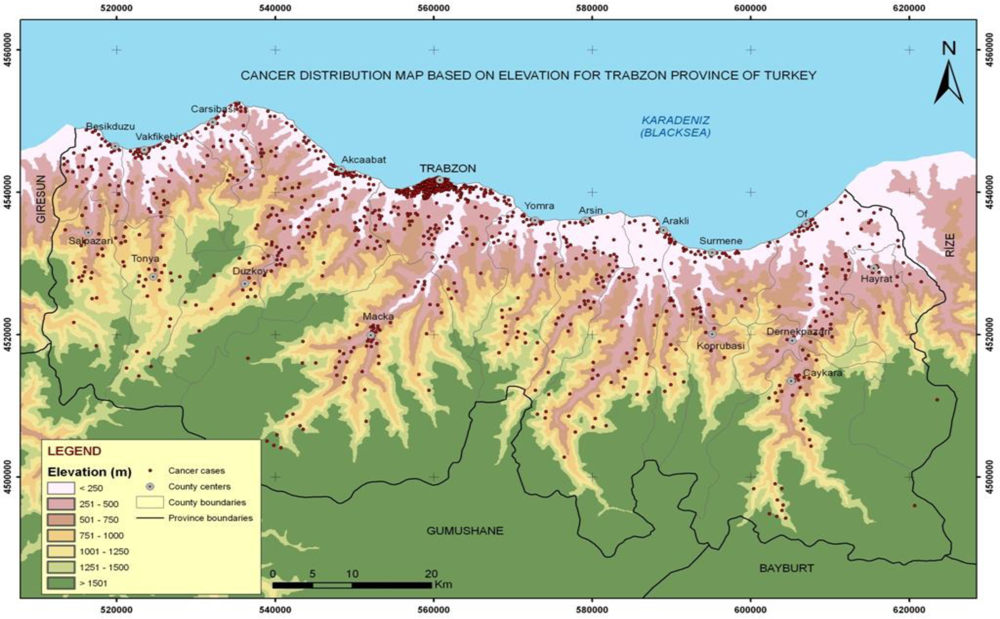
3.4. Relationship between the Distribution of Cancer Cases and Elevation
4. Conclusions
Acknowledgments
References
- The International Union Against Cancer. World Cancer Campaign.
- Cancer Control: Knowledge into Action. In WHO Guide for Effective Programmes: Module 1-Planning; World Health Organization: Geneva, Switzerland, 2006.
- San, TA; Sari, D; Turkistanli, EC. Knowledge, Attitudes, Risk Factors, and Early Detection of Cancer Relevant to the School Teachers in Izmir, Turkey. Prev. Med 2005, 40, 636–641. [Google Scholar]
- World Health Organization. WHO Global Infobase Online.
- .
- World Health Organization. 58th World Health Assembly Approved Resolution on Cancer Prevention and Control Report 2005.
- Sengelen, M. Cancer Statistics in Turkey. Science Expertise Thesis, Hacettepe University, Health Science Institute, Ankara, Turkey, 2002 (In Turkish).
- Colak, E; Yomralioglu, T. Creating GIS-Based Cancer Density Maps for Trabzon Province of Turkey. Proceedings of the ESRI Health GIS Conference, Chicago, IL, USA, October 23–26; 2005. [Google Scholar]
- Kistemann, T; Dangendorf, F; Schweikart, J. New Perspectives on the Use of Geographical Information Systems (GIS) in Environmental Health Sciences. Int. J. Hyg. Environ. Health 2002, 205, 169–181. [Google Scholar]
- Vieira, V; Webster, T; Aschengrau, A; Ozonoff, D. A Method for Spatial Analysis of Risk in a Polulation-Based Case-Control Study. Int. J. Hyg. Environ. Health 2002, 205, 115–120. [Google Scholar]
- Friis, R; Sellers, T. Epidemiology for Public Health Practice; Apsen Publications: Gaithersburg, MD, USA, 1996. [Google Scholar]
- Cromley, EK; McLafferty, SL. GIS and Public Health; The Guilford Press: New York, NY, USA, 2002; pp. 158–232. [Google Scholar]
- National Cancer Control Programmes. In Policies and Managerial Guideliness, 2nd ed; World Health Organization: Geneva, Switzerland, 2002.
- Snow, J. On the Mode of Communication of Cholera, 2nd ed; John Churchill: London, UK, 1855. [Google Scholar]
- Haviland, A. The Geographical Distribution of Heart Disease and Dropsy. In Cancer in Phthisis in Females in England and Wales; Swan Schonnenschein: London, UK, 1875. [Google Scholar]
- Walter, SD. Disease Mapping: a Historical Perspective. In Spatial Epidemiology: Methods and Applications, 1st ed; Elliott, P, Wakefield, J, Best, N, Briggs, D, Eds.; Oxford University Press: New York, NY, USA, 2000; pp. 223–239. [Google Scholar]
- Morra, P; Bagli, S; Spadoni, G. The Analysis of Human Health Risk with a Detailed Procedure Operating in a GIS Environment. Environ. Int 2006, 32, 444–454. [Google Scholar]
- Pearce, J; Boyle, P. Examining the Relationship between Lung Cancer and Radon in Small Areas across Scotland. Health Place 2005, 11, 275–282. [Google Scholar]
- Poulstrup, A; Hansen, HL. Use of GIS and Exposure Modeling as Tools in a Study of Cancer Incidence in a Population Exposed to Airborne Dioxin. Environ. Health Perspect 2004, 112, 1032–1036. [Google Scholar]
- Elliott, P; Wakefield, J; Best, N; Briggs, D. Spatial Epidemiology: Methods and Applications. In Spatial Epidemiology: Methods and Applications, 1st ed; Elliott, P, Wakefield, J, Best, N, Briggs, D, Eds.; Oxford University Press: New York, NY, USA, 2000; pp. 3–15. [Google Scholar]
- Flinton, DM; Walters, NJ. Occupational Activity and Risk of Prostate Cancer in Ireland. J. Radiother. Pract 2004, 4, 102–106. [Google Scholar]
- Grauman, DJ; Robert, E; Tarone, RE; Devesa, SS; Fraumeni, JF. Alternate Ranging Methods for Cancer Mortality Maps. J. Natl. Cancer Inst 2000, 92, 534–543. [Google Scholar]
- Gregorio, DI; Cromley, E; Mrozinski, R; Walsh, SJ. Subject Loss in Spatial Analysis of breast cancer. Health Place 1999, 5, 173–177. [Google Scholar]
- Mosavi-Jarrahi, A; Moini, M; Mohagheghi, M; Alebouyeh, M; Yazdizadeh, B; Shahabian, A; Nahvijo, A; Alizadeh, R. Clustering of Childhood Cancer in the Inner City of Tehran Metropolitan Area: A GIS-Based Analysis. Int. J. Hyg. Environ. Health 2007, 210, 113–119. [Google Scholar]
- Oliver, MN; Matthews, KA; Siadaty, M; Hauck, FR; Pickle, LW. Geographic Bias Related to Geocoding in Epidemiologic Studies. Int. J. Health Geogr 2005, 4, 29. [Google Scholar]
- Pickle, LW; Waller, LA; Lawson, AB. Current Practices in Cancer Spatial Data Analysis: A Call for Guidance. Int. J. Health Geogr 2005, 4, 3. [Google Scholar]
- Roche, LM; Skinner, R; Weinstein, RB. Use of a Geographic System to Identify and Characterize Areas with High Proportions of Distant Stage Breast Cancer. J. Publ. Health Manag. Pract 2002, 8, 26–32. [Google Scholar]
- Scott, D; Curtis, B; Twumasi, FO. Towards the Creation of a Health Information System for Cancer in KwaZulu-Natal, South Africa. Health Place 2002, 8, 237–249. [Google Scholar]
- Lawson, AB. Statistical Methods in Spatial Epidemiology, 2nd ed; John Wiley & Sons: England, UK, 2006. [Google Scholar]
- Pickle, LW. Spatial Analysis of Disease. In Biostatistical Applications in Cancer Research; Beam, C, Ed.; Klewer Academic Publishers: Boston, USA, 2002; pp. 113–150. [Google Scholar]
- Waller, LA; Gotway, CA. Applied Spatial Statistics for Public Health Data; John Wiley & Sons, Inc: Hoboken, NJ, USA, 2004. [Google Scholar]
- Cancer Control Department. Cancer Control Policy and Cancer Data 1995–99, Republic of Turkey, Ministry of Health, Report No: 618; Ankara, Turkey, 2000 (In Turkish).
- Turkey State Planning Organization. Socio-economic Development Ranking of Provinces of Turkey, May 2003; ; Issue No: 2671; Turkey, 2003; pp. 250.
- .
- Annoni, A; Luzet, C; Gubler, E; Ihde, J. Map Projections for Europe; European Commission Joint Research Centre, Institute for Environment and Sustainability: Italy, 2003. [Google Scholar]
- Bilge, N. Standardization of Education and Radiotherapy Centers related to Cancer in Turkey. In Cancer Rate in Turkey; Tuncer, I, Ed.; TUBITAK and Cukurova University: Adana, Turkey, 1994. (In Turkish) [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data Theme | Data Sets | Data Set Name | Display | Attribute Name / Explanation | |
|---|---|---|---|---|---|
| Administrative Unit | County | ILCE |  Polygon (Area) Polygon (Area) | IDBK ISIM … | Administration Unit Code Administration Unit Name |
 | District/Village | MAKO | Polygon (Area) | IDBK ISIM IDBT NUFS … | Administration Unit Code Administration Unit Name Administration Unit Type Population |
Transportation | Road | YOLH |  Line Line | ISIM YOTP BADK SADK … | Road Name Road Type Beginning Address Code Finishing Address Code |
Topography | Elevation | YUKS | Line | YUKS … | Elavation |
| Digital Elevation Model Produced from Elavation | SAYM |  Raster Raster | YUGR … | Elevation Classification | |
Land Cover | Satellite image | Raster | Landsat 7 | ETM+ image, 2003 | |
| Land Cover Produced from Landsat7 ETM+ image | AROR | Raster | ARKS … | Land Cover Classification | |
Health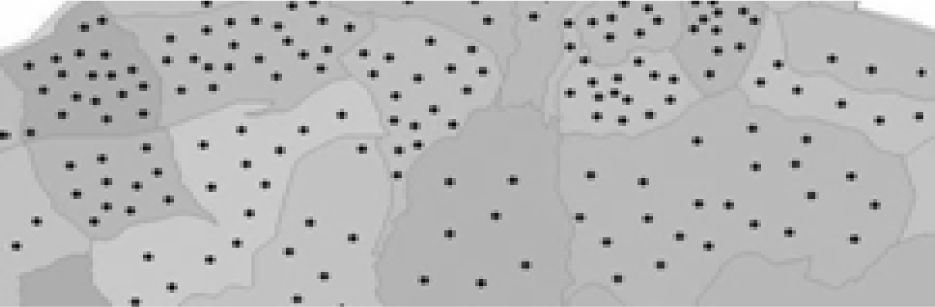 | Cancer Registry | KAKA |  Point Point | SEX AGE ADRS IDBK TOPO TOPL DATE | Patient’s sex Patient’s age Patient’s address Admin. Unit of Address Disease Name Disease Type Diagnosis Date |
| Cancer Types | Man (%) | Women (%) | Total (%) |
|---|---|---|---|
| Lung | 28.5 | 5.2 | 19.1 |
| Skin | 11.1 | 14.3 | 12.3 |
| Breast | 0.3 | 24.2 | 9.9 |
| Stomach | 9.3 | 9.7 | 9.5 |
| Bladder | 10.5 | 1.3 | 6.8 |
| Prostate | 8.2 | - | 4.9 |
| Thyroid | 1.2 | 10.2 | 4.8 |
| Other | 30.9 | 35.1 | 32.7 |
| Group of Incidence Rates | Number of Administrative Units | Percentage |
|---|---|---|
| 0 | 232 | 39 |
| 1–150 | 124 | 21 |
| 151–300 | 109 | 18 |
| 301–600 | 105 | 18 |
| 601–987 | 26 | 4 |
| Total | 596 | 100% |
| Land Cover Class | The number of Cancer Cases | Percentage |
|---|---|---|
| Forestry | 389 | 34 |
| Agricultural area | 299 | 26 |
| Hazelnut | 243 | 21 |
| Residential area | 211 | 18 |
| Tea | 8 | 1 |
| Total | 1,150 | 100% |
| LAND COVER | CANCER TYPES | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Lung/Bronchial &Larynx/Throat | Skin | Breast | Stomach & Colon/Rectum | Bladder | Prostate | Thyroid | Other Types | Total | ||
| Agricultural area | Count | |||||||||
| Expected count | 125 | 62 | 52 | 85 | 34 | 27 | 23 | 142 | 550 | |
| % of Total | 122.9 | 67.9 | 54.5 | 76 | 37.3 | 26.8 | 26.3 | 138.2 | 550 | |
| Adj. | 10.9% | 5.4% | 4.5% | 7.4% | 3% | 2.3% | 2% | 12.3% | 47.8% | |
| Residual | 0.3 | −1.1 | −0.5 | 1.5 | −0.8 | 0.1 | −0.9 | 0.5 | ||
| Residential area | Count | |||||||||
| Expected count | 55 | 19 | 29 | 25 | 12 | 9 | 5 | 57 | 211 | |
| % of Total | 47.2 | 26.1 | 20.9 | 29.2 | 14.3 | 10.3 | 10.1 | 53 | 211 | |
| Adj. | 4.8% | 1.7% | 2.5% | 2.2% | 1% | 0.08% | 0.4% | 5% | 18.3% | |
| Residual | 1.4 | −1.6 | 2.1 | −0.9 | −0.7 | −0.5 | −1.8 | 0.7 | ||
| Forestry | Count | |||||||||
| Expected count | 77 | 61 | 33 | 49 | 32 | 20 | 27 | 90 | 389 | |
| % of Total | 86.9 | 48 | 38.6 | 53.8 | 26.4 | 18.9 | 18.6 | 97.8 | 389 | |
| Adj. | 6.7% | 5.3% | 2.9% | 4.3% | 2.8% | 1.7% | 2.3% | 7.8% | 33.8% | |
| Residual | −1.5 | 2.5 | −1.2 | −0.9 | 1.4 | 0.3 | 2.5 | −1.1 | ||
| Total | Count | 257 | 142 | 114 | 159 | 78 | 56 | 55 | 289 | 1150 |
| % of Total | 22.3% | 12.3% | 9.9% | 13.8% | 6.8% | 4.9% | 4.8% | 25.1% | 100% | |
| ELEVATION (Meter) | CANCER TYPES | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Lung/Bronchus&Larynx/Throat | Skin | Breast | Stomach & Colon/Rectum | Bladder | Prostate | Thyroid | Other Types | Total | ||
| 0–250 | Count | 145 | 66 | 77 | 83 | 42 | 29 | 21 | 160 | 623 |
| Expected count | 139.2 | 76.9 | 61.8 | 86.1 | 42.3 | 30.3 | 29.8 | 156.6 | 623 | |
| % of Total | 2.6% | 5.7% | 6.7% | 7.2% | 3.7% | 2.5% | 1.8% | 13.9% | 54.2% | |
| Adj. Residual | 0.8 | −2.0 | 3.0 | −0.5 | −0.1 | −0.4 | −2.4 | 0.5 | ||
| 251–500 | Count | 53 | 37 | 23 | 29 | 15 | 9 | 17 | 55 | 238 |
| Expected count | 53.2 | 29.4 | 23.6 | 32.9 | 16.1 | 11.6 | 11.4 | 59.8 | 238 | |
| % of Total | 4.6% | 3.2% | 2% | 2.5% | 1.3% | 0.8% | 1.5% | 4.8% | 20.7% | |
| Adj. Residual | 0 | 1.7 | −0.1 | −0.8 | −0.3 | −0.9 | 1.9 | −0.8 | ||
| 501–750 | Count | 24 | 17 | 6 | 26 | 12 | 6 | 5 | 32 | 128 |
| Expected count | 28.6 | 15.8 | 12.7 | 17.7 | 8.7 | 6.2 | 6.1 | 32.2 | 128 | |
| % of Total | 2.1% | 1.5% | 0.5% | 2.3% | 1% | 0.5% | 0.4% | 2.8% | 11.1% | |
| Adj. Residual | −1.0 | 0.3 | −2.1 | 2.3 | 1.2 | −0.1 | −0.5 | 0 | ||
| 751–1000 | Count | 14 | 12 | 5 | 8 | 3 | 10 | 5 | 19 | 76 |
| Expected count | 17 | 9.4 | 7.5 | 10.5 | 5.2 | 3.7 | 3.6 | 19.1 | 76 | |
| % of Total | 1.2% | 1% | 0.4% | 0.7% | 0.3% | 0.9% | 0.4% | 1.7% | 6.6% | |
| Adj. Residual | v0.9 | 0.9 | −1.0 | −0.9 | −1.0 | 3.5 | 0.8 | 0 | ||
| >1000 | Count | 21 | 10 | 3 | 13 | 6 | 2 | 7 | 23 | 85 |
| Expected count | 19 | 10.5 | 8.4 | 11.8 | 5.8 | 4.1 | 4.1 | 21.4 | 85 | |
| % of Total | 1.8% | 0.9% | 0.3% | 1.1% | 0.5% | 0.2% | 0.6% | 2% | 7.4% | |
| Adj. Residual | 0.5 | −0.2 | −2.0 | 0.4 | 0.1 | −1.1 | 1.6 | 0.4 | ||
| Total | Count | 257 | 142 | 114 | 159 | 78 | 56 | 55 | 289 | 1,150 |
| % of Total | 22.3% | 12.3% | 9.9% | 13.8% | 6.8% | 4.9% | 4.8% | 25.1% | 100% | |
© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Yomralioglu, T.; Colak, E.H.; Aydinoglu, A.C. Geo-Relationship between Cancer Cases and the Environment by GIS: A Case Study of Trabzon in Turkey. Int. J. Environ. Res. Public Health 2009, 6, 3190-3204. https://doi.org/10.3390/ijerph6123190
Yomralioglu T, Colak EH, Aydinoglu AC. Geo-Relationship between Cancer Cases and the Environment by GIS: A Case Study of Trabzon in Turkey. International Journal of Environmental Research and Public Health. 2009; 6(12):3190-3204. https://doi.org/10.3390/ijerph6123190
Chicago/Turabian StyleYomralioglu, Tahsin, Ebru H. Colak, and Arif C. Aydinoglu. 2009. "Geo-Relationship between Cancer Cases and the Environment by GIS: A Case Study of Trabzon in Turkey" International Journal of Environmental Research and Public Health 6, no. 12: 3190-3204. https://doi.org/10.3390/ijerph6123190
APA StyleYomralioglu, T., Colak, E. H., & Aydinoglu, A. C. (2009). Geo-Relationship between Cancer Cases and the Environment by GIS: A Case Study of Trabzon in Turkey. International Journal of Environmental Research and Public Health, 6(12), 3190-3204. https://doi.org/10.3390/ijerph6123190