
The Impact of Air Quality on Patient Mortality: A National Study

Abstract
1. Introduction
2. Data and Methods
2.1. Data Sources
2.2. Data Preparation
2.3. Variables
2.3.1. Exposure Data
2.3.2. Outcome Data
2.4. Statistical Analysis
3. Results
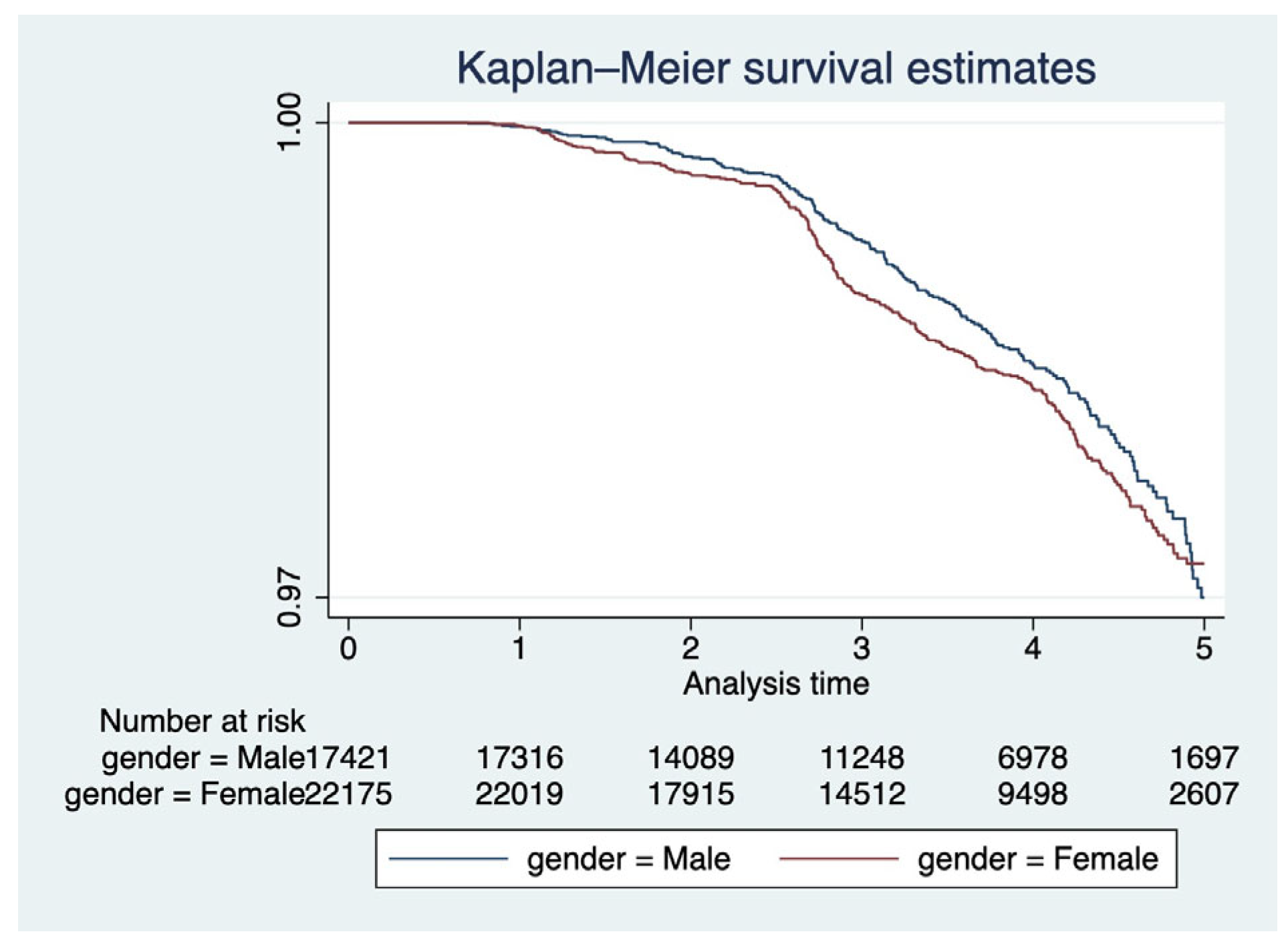
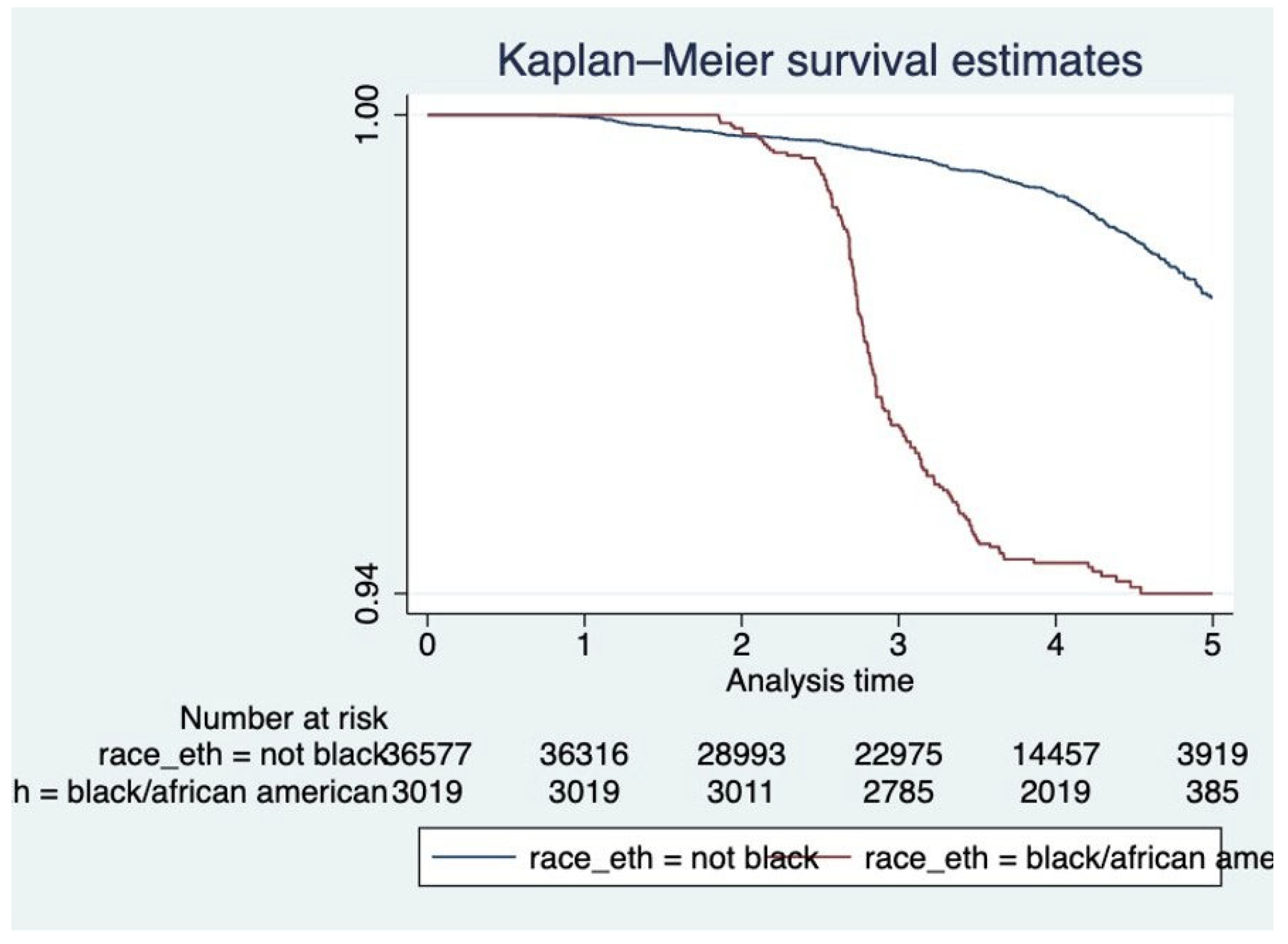
3.1. Bivariate Analysis
3.2. Time-Independent Analysis
4. Discussion
4.1. Time-Independent Analysis
4.2. Strengths
4.3. Limitations
4.4. Public Health Significance
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Environmental Protection Agency. Research on Health Effects from Air Pollution. Available online: https://www.epa.gov/air-research/research-health-effects-air-pollution (accessed on 1 January 2023).
- National Institute of Environmental Health Sciences. Air Pollution and Your Health. Available online: https://www.niehs.nih.gov/health/topics/agents/air-pollution/index.cfm (accessed on 1 March 2023).
- Manisalidis, I.; Stavropoulou, E.; Stavropoulos, A.; Bezirtzoglou, E. Environmental and Health Impacts of Air Pollution: A Review. Frontiers 2020, 8, 14. Available online: https://www.frontiersin.org/articles/10.3389/fpubh.2020.00014/full (accessed on 1 March 2023). [CrossRef] [PubMed]
- World Health Organization. How Air Pollution Is Destroying Our Health. 2023. Available online: https://www.who.int/news-room/spotlight/how-air-pollution-is-destroying-our-health (accessed on 1 March 2023).
- World Health Organization. Air Quality and Health. 2023. Available online: https://www.who.int/teams/environment-climate-change-and-health/air-quality-and-health/health-impacts (accessed on 1 March 2023).
- Yazdi, M.D.; Wang, Y.; Di, Q.; Requia, W.J.; Wei, Y.; Shi, L.; Sabath, M.B.; Dominici, F.; Coull, B.; Evans, J.S.; et al. Long-term effect of exposure to lower concentrations of air pollution on mortality among us medicare participants and vulnerable subgroups: A doubly-robust approach. Lancet Planet. Health 2021, 5, e689–e697. [Google Scholar] [CrossRef] [PubMed]
- Yazdi, M.D.; Wang, Y.; Di, Q.; Wei, Y.; Requia, W.J.; Shi, L.; Sabath, M.B.; Dominici, F.; Coill, A.B.; Evans, J.S.; et al. Long-term association of air pollution and hospital admissions among medicare participants using a doubly robust additive model. Circulation 2021, 143, 1584–1596. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Adar, M.; Baxter, L.T.; Morley, M. Spatial variability of PM2.5-associated mortality in the United States: A nationwide modeling study using Medicare and Medicaid data. Environ. Pollut. 2023, 327, 121527. Available online: https://www.sciencedirect.com/science/article/abs/pii/S0269749123003470 (accessed on 1 July 2025).
- Delfino, E.S.; Wang, S.N.; DeAlwis, M.J.; Shultz, B.L. Disparities in Air Pollution Exposure and Associated Health Effects in the United States. ACS Environ. Health Sustain. 2023, 1, 177–189. Available online: https://pubs.acs.org/doi/full/10.1021/envhealth.3c00106 (accessed on 1 July 2025).
- Sacks, M.M.; Karas, L.A.; Szpiro, M.H.; Casey, A.L.; Koutrakis, P. Air inequality: Temporal trends and racial/ethnic disparities in ambient air pollution exposure in the United States. arXiv 2023, arXiv:2303.12559. [Google Scholar]
- Beamer, A.E.; Mayer, M.A.; Stanley, C.A.; Gray, B.J. Air pollution and neighborhood socioeconomic deprivation: A synergistic risk factor for COVID-19 incidence and mortality in the United States. BMC Public Health 2023, 23, 1421. [Google Scholar]
- Outpatient Electronic Health Record Data from Primary Care and Family Medicine Practices to Support Cdc’s Covid-19 Emergency Response (American Board of Family Medicine). Available online: https://govtribe.com/file/government-file/po-75d30121p10944-abfm-dot-pdf (accessed on 1 March 2023).
- Environmental Protection Agency. Airdata. Available online: https://aqs.epa.gov/aqsweb/airdata/download_files.html (accessed on 1 November 2022).
- Environmental Protection Agency. Air Data Basic Information. Available online: https://www.epa.gov/outdoor-air-quality-data/air-data-basic-information (accessed on 1 March 2023).
- Python. 2023. Available online: https://www.python.org/ (accessed on 1 December 2022).
- Stata. 2023. Available online: Https://www.stata.com/new-in-stata/ (accessed on 1 December 2022).
- United States Census Bureau. Census Regions and Divisions of the United States. Available online: https://www2.census.gov/geo/pdfs/maps-data/maps/reference/usregdiv.pdf (accessed on 1 March 2023).
- Yeung, J. Pandemic Lockdowns Improved Air Quality in 84% of Countries Worldwide, Report Finds. CNN. Available online: https://www.cnn.com/2021/03/16/health/world-air-quality-report-intl-hnk-scn/index.html (accessed on 1 March 2023).
- Liu, Y.; Reid, R.C.; Cozzi-Lepri, M.; Fann, N.; Lim, C.H.; Vallve, D.; Armstrong, B.; Schwartz, J.; Jaakkola, J.J.; Zanobetti, A.; et al. Mortality risk attributable to wildfirerelated PM2.5 pollution: A global case–crossover study. Lancet Planet. Health 2021, 5, e741–e749. [Google Scholar] [CrossRef]
- Purple Air. Real Time Air Quality Map. Available online: https://map.purpleair.com/ (accessed on 1 March 2023).
- Di, Q.; Wang, Y.; Zanobetti, A.; Wang, Y.; Koutrakis, P.; Choirat, C.; Dominici, F.; Schwartz, J.D. Air Pollution and Mortality in the Medicare Population. N. Engl. J. Med. 2017, 376, 2513–2522. Available online: https://pubmed.ncbi.nlm.nih.gov/28657878/ (accessed on 1 July 2025). [CrossRef] [PubMed]
- Wu, W.; Nethery, J.; Sabath, B.M.; Braun, D.; Dominici, F. Exposure to air pollution and COVID19 mortality in the United States. Environ. Health Perspect. 2020, 129, 127009. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Covariate | Total N = 39,596 (100%) |
|---|---|
| Gender | |
| Female | 56.00% |
| Male | 44.00% |
| Age | |
| 80+ years | 7.04% |
| <80 years | 92.96% |
| Race | |
| Black/African American | 7.62% |
| Other | 92.38% |
| Region | |
| East North Central | 5.48% |
| West South Central | 7.56% |
| West North Central | 30.62% |
| Pacific | 15.74% |
| South Atlantic | 8.57% |
| Middle Atlantic | 2.22% |
| New England | 16.16% |
| East South Central | 4.60% |
| Mountain | 9.04% |
| Year of Entry | |
| 2016 | 9.94% |
| 2017 | 28.35% |
| 2018 | 25.83% |
| 2019 | 11.20% |
| 2020–2022 | 24.67% |
| Unadjusted | Adjusted | |
|---|---|---|
| HR 95% CI | HR 95% CI | |
| Covariate | ||
| Air Quality | ||
| AQI > 50 | 3.52 * (2.96, 4.19) | 4.02 * (3.36, 4.82) |
| AQI <= 50 | 1.00 | 1.00 |
| Gender | ||
| Female | 1.11 (0.93, 1.32) | 0.93 (0.78, 1.11) |
| Male | 1.00 | 1.00 |
| Age | ||
| 80 + years | 4.69 * (3.82, 5.74) | 6.73 * (5.47, 8.28) |
| <80 years | 1.00 | 1.00 |
| Race | ||
| Black/African American | 3.93 * (3.26, 4.23) | 4.27 * (3.47, 5.26) |
| Other | 1.00 | 1.00 |
| Region | ||
| East North Central | 0.23 * (0.09, 0.55) | 0.39 * (0.16, 0.96) |
| West South Central | 1.15 (0.72, 1.84) | 1.03 (0.64, 1.67) |
| West North Central | 2.37 * (1.60, 3.51) | 2.93 * (1.97, 4.36) |
| Pacific | 0.23 * (0.12, 0.42) | 0.29 * (0.15, 0.54) |
| South Atlantic | 0.21 * (0.11, 0.43) | 0.24 * (0.12, 0.49) |
| Middle Atlantic | 1.21 (0.61, 2.39) | 2.09 * (1.05, 4.16) |
| New England | 0.76 (0.49, 1.18) | 0.53 * (0.34, 0.82) |
| East South Central | 0.14 * (0.05, 0.40) | 0.24 * (0.08, 0.70) |
| Mountain | 1.00 | 1.00 |
| Year of Entry | ||
| 2016 | 1.00 | |
| 2017 | 2.19 * (1.58, 3.02) | 3.33 * (2.38, 4.66) |
| 2018 | 2.91 * (2.05, 4.14) | 4.62 * (3.22, 6.63) |
| 2019 | 10.90 * (7.41, 16.05) | 35.64 * (23.68, 53.63) |
| 2020–2022 | 1.90 * (0.96, 3.76) | 4.24 * (2.10, 8.53) |
| Model A | Model B | Model C | Model D | Model E | |
|---|---|---|---|---|---|
| Covariate | HR 95% CI | HR 95% CI | HR 95% CI | HR 95% CI | HR 95% CI |
| Air Quality | |||||
| AQI > 50 | 3.52 * | 3.67 * | 3.27 * | 3.65 * | 3.70 * |
| (2.96, 4.19) | (3.08, 4.36) | (2.75, 3.89) | (3.06, 4.35) | (3.11, 4.40) | |
| AQI <= 50 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Gender | |||||
| Female | 1.10 | ||||
| (0.92, 1.31) | |||||
| Male | 1.00 | ||||
| Age | |||||
| 80+ years | 4.99 * | ||||
| (4.08, 6.11) | |||||
| <80 years | 1.00 | ||||
| Race | |||||
| Black/African American | 3.34 * | ||||
| (2.94, 4.26) | |||||
| Other | 1.00 | ||||
| Region | |||||
| East North Central | 0.30 * | ||||
| (0.13, 0.74) | |||||
| West South Central | 1.31 | ||||
| (0.82, 2.10) | |||||
| West North Central | 2.63 * | ||||
| (1.77, 3.90) | |||||
| Pacific | 0.28 * | ||||
| (0.15, 0.52) | |||||
| South Atlantic | 0.21 * | ||||
| (0.10, 0.42) | |||||
| Middle Atlantic | 1.50 | ||||
| (0.76, 2.96) | |||||
| New England | 0.64 | ||||
| (0.41, 1.00) | |||||
| East South Central | 0.21 * | ||||
| (0.07, 0.61) | |||||
| Mountain | 1.00 | ||||
| Year of Entry | |||||
| 2016 | 1.00 | ||||
| 2017 | 2.31 * | ||||
| (1.67, 3.19) | |||||
| 2018 | 2.95 * | ||||
| (2.08, 4.19) | |||||
| 2019 | 12.40 * | ||||
| (8.42, 18.27) | |||||
| 2020–2022 | 2.39 * | ||||
| (1.21, 4.73) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Periyakoil, D.; Chu, I.; Prata, N.; Diener-West, M. The Impact of Air Quality on Patient Mortality: A National Study. Int. J. Environ. Res. Public Health 2025, 22, 1123. https://doi.org/10.3390/ijerph22071123
Periyakoil D, Chu I, Prata N, Diener-West M. The Impact of Air Quality on Patient Mortality: A National Study. International Journal of Environmental Research and Public Health. 2025; 22(7):1123. https://doi.org/10.3390/ijerph22071123
Chicago/Turabian StylePeriyakoil, Divya, Isabella Chu, Ndola Prata, and Marie Diener-West. 2025. "The Impact of Air Quality on Patient Mortality: A National Study" International Journal of Environmental Research and Public Health 22, no. 7: 1123. https://doi.org/10.3390/ijerph22071123
APA StylePeriyakoil, D., Chu, I., Prata, N., & Diener-West, M. (2025). The Impact of Air Quality on Patient Mortality: A National Study. International Journal of Environmental Research and Public Health, 22(7), 1123. https://doi.org/10.3390/ijerph22071123