
The Role of Rehabilitation Nurses in Empowering Mastectomised Women for Self-Care: A Scoping Review

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Methodology
2.1. Study Design
2.1.1. Research
2.1.2. Research Question
2.1.3. Strategy PCC
- Population (P): Mastectomised women;
- Concept (C): Interventions of the Rehabilitation Nurse;
- Context (C): Empowerment for self-care.
2.1.4. Inclusion Criteria
2.1.5. Study Types
2.1.6. Search Strategy
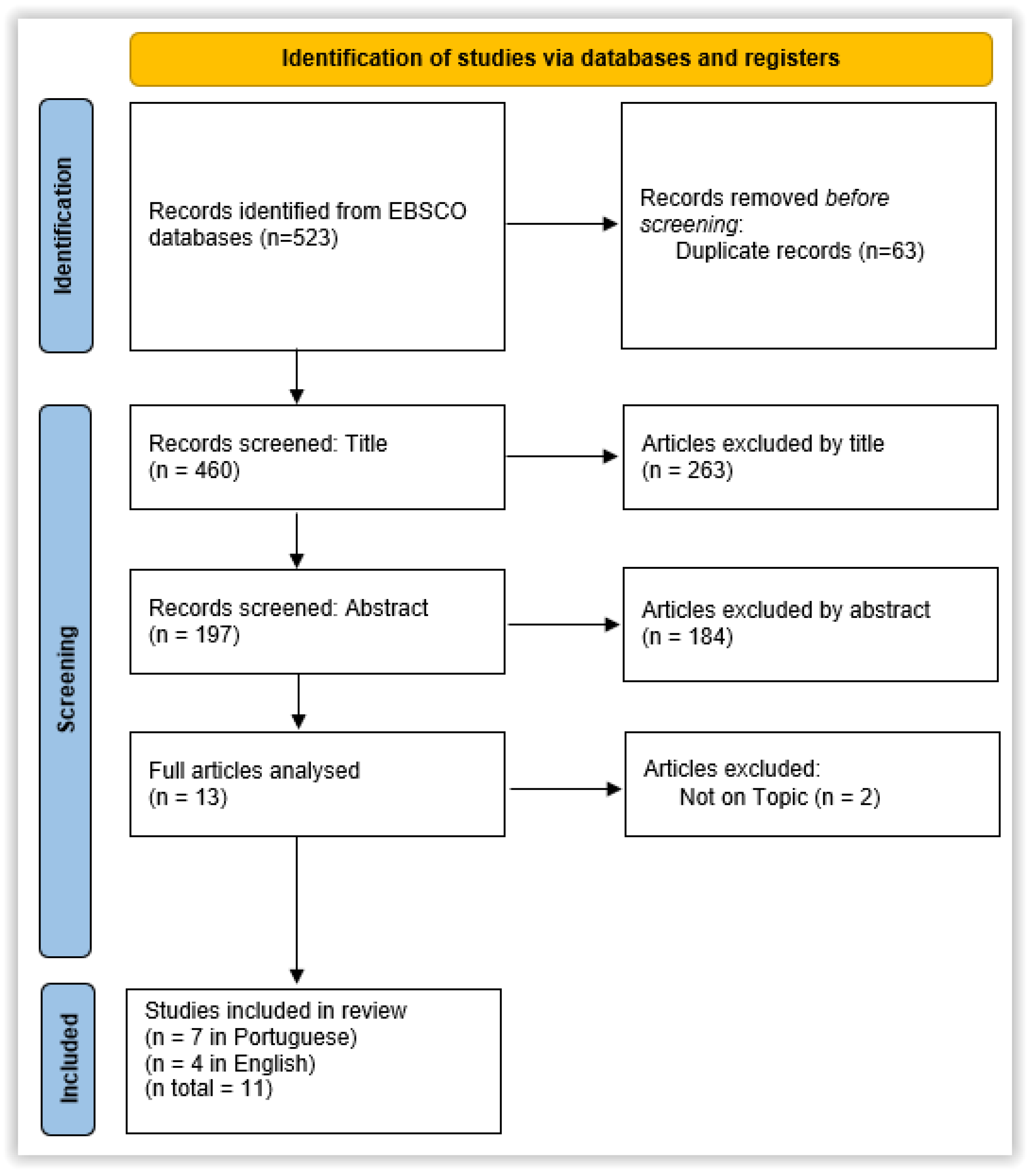
2.1.7. Study Selection Process
2.1.8. Data Analysis and Extraction
2.1.9. Data Synthesis and Evaluating the Quality of Studies
3. Results
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Acknowledgments
Conflicts of Interest
References
- Watkins, E.J. Overview of breast cancer. JAAPA 2019, 32, 13–17. [Google Scholar] [CrossRef]
- Harfouche, A.; Silva, S.; Faria, J.; Araújo, R.; Gouveia, A.; Lacerda, M.; D’Orey, L. Cancro de Mama: Valor em Saúde, Custos e Financiamento. Acta Med. Port. 2017, 30, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Pereira, D.; Martinelli Braga, A.A. A Mastectomia E A Ressignificação do Corpo no Feminino. Rev. Psicol. Divers. e Saúde 2016, 5, 47–64. [Google Scholar] [CrossRef]
- Gupta, M.; Goyal, N. Applied Anatomy of Breast Cancer. In Breast Cancer; Springer Nature: Singapore, 2022; pp. 23–35. [Google Scholar]
- IPO Mastectomia. Lisboa. 2019. Available online: https://www.ipolisboa.min-saude.pt/wp-content/uploads/2020/04/Cancro-Mama_Mastectomia.pdf (accessed on 21 April 2025).
- Hobson, P.; Meara, J. Quality of life in chronic disease rehabilitation. Rev. Clin. Gerontol. 2004, 14, 317–325. [Google Scholar] [CrossRef]
- Al Aateibi, B.S.; Sadoun, M.M.; Alnuaimi, N.R.; Alghamdi, S.A.S.; Alharthi, M.F.A.; Khayat, H.M.; Almatrafi, R.J.S.; Falattah, M.M.B.; Ridha, W.A.A.; Albariqi, N.A.A.; et al. Comprehensive Review of Nurses’ Role in Chronic Disease Management: Collaborative Care Approaches. J. Ecohumanism 2024, 3, 6651–6659. [Google Scholar] [CrossRef]
- Galanti, G.-A. Culturally Competent Rehabilitation Nursing. Rehabil. Nurs. 2005, 30, 123–126. [Google Scholar] [CrossRef]
- Camicia, M. Transforming Health Care through Improving Care Transitions: A Duty To Embrace. Rehabil. Nurs. 2015, 40, 1–2. [Google Scholar] [CrossRef]
- Vaughn, S.; Rye, J.; Allen, A.; Bok, A.; Mauk, K.; Park, L.; Pierce, L.; Wintersgill Holler, W. Inside Looking Out. Rehabil. Nurs. 2023, 48, 23–38. [Google Scholar] [CrossRef]
- Vaughn, S.; Mauk, K.L.; Jacelon, C.S.; Larsen, P.D.; Rye, J.; Wintersgill, W.; Cave, C.E.; Dufresne, D. The Competency Model for Professional Rehabilitation Nursing. Rehabil. Nurs. 2016, 41, 33–44. [Google Scholar] [CrossRef]
- OE. Padrões de Qualidade dos Cuidados de Enfermagem. Lisboa, 2001. Available online: https://www.ordemenfermeiros.pt/media/8903/divulgar-padroes-de-qualidade-dos-cuidados.pdf (accessed on 21 April 2025).
- OE. Padrões de Qualidade dos Cuidados Especializados em Enfermagem de Reabilitação. Lisboa, 2018. Available online: https://diariodarepublica.pt/dr/detalhe/regulamento/350-2015-67552234 (accessed on 21 April 2025).
- Wang, T.-C.; Chang, P.-H.; Chen, W.H.; Hung, C.-C.; Chen, J.-P.; Lin, Y.-C.; Chiou, A.-F. The Effectiveness of an Upper Limb Rehabilitation Program on Quality of Life in Breast Cancer Patients after Mastectomy: A Randomized Controlled Trial. Semin. Oncol. Nurs. 2023, 39, 151512. [Google Scholar] [CrossRef]
- Rodrigues, T.; Moreira, M.T.; Lima, A.; Fernandes, R.; Gomes, B. Contributions of a Rehabilitation Nursing Program in the Self-Care of Women Undergoing Breast Surgery. Nurs. Rep. 2023, 13, 913–922. [Google Scholar] [CrossRef]
- Tang, X. The effect of multi-supportive nursing on the postoperative rehabilitation of breast cancer patients. Am. J. Transl. Res. 2021, 13, 7327–7334. [Google Scholar] [PubMed]
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid. Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef]
- Sampaio, R.; Mancini, M. Estudos de revisão sistemática: Um guia para síntese criteriosa da evidência científica. Rev. Bras. Fisioter. 2007, 11, 83–89. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- JBI. Critical Appraisal Tools. Joanna Briggs Institute. Available online: https://jbi.global/critical-appraisal-tools (accessed on 1 June 2025).
- da Silva, C.H.H.C.; de Araújo Cunha, T.A.; Dantas, C.S.; de Jesus, C.S. A importância da enfermagem no pós-operatório de mulheres mastectomizadas com dissecção de linfonodos axilares: Revisão integrativa. Res. Soc. Dev. 2021, 10, e57210616177. [Google Scholar] [CrossRef]
- Merêncio, K.; Ventura, M. Vivências da mulher mastectomizada: A enfermagem de reabilitação na promoção da autonomia. Rev. Enferm. Ref. 2020, 2, 1–8. [Google Scholar]
- dos Santos Cesário, J.M.; de Oliveira Hernandes, L.; Botion, B.M.; da Silva, G.K.A.; da Cunha, A.P.; Gomes, D.M.; da Silva Vitorino, P.G.; de Paula Flauzino, V.H. A prática clínica do enfermeiro na reabilitação estética de pacientes mastectomizadas. Res. Soc. Dev. 2022, 11, e504111032865. [Google Scholar] [CrossRef]
- Panobianco, M.S.; Felipe, I.D.O.; Canete, A.C.S.; Nunes, L.C.; Prado, M.A.S. Assistência de enfermagem em núcleo de reabilitação: O papel do enfermeiro. Rev. Enferm. UERJ 2020, 28, e51082. [Google Scholar] [CrossRef]
- Baldaia, C.; Fernandes, C.; Ferreira, L. Exergames na reabilitação da pessoa mastectomizada: Uma scoping review. Onconews 2024, 47. Available online: https://scielo.pt/scielo.php?script=sci_arttext&pid=S2183-69142023000200003 (accessed on 21 April 2025).
- Sun, L.-H. Application value of Neuman’s nursing model in the perioperative period of radical mastectomy. Am. J. Transl. Res. 2024, 16, 4928–4938. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos Scofano, B.; Almeida de Lima, A.; Dos Reis Silva, R.; Garcia Penna, L.H.; Silva de Andrade, K.B.; Brito Pinheiro, A.P. Ações/plano de alta da enfermagem í mulher submetida í mastectomia. Nursing 2020, 23, 3736–3744. [Google Scholar] [CrossRef]
- Zúñiga-Tapia, R.; Panobianco, M.S.; Prado, M.A.S.; Henríquez, P.C. Experience in a rehabilitation center for mastectomized women at the start of the COVID-19 pandemic. Rev. Gaúcha Enferm. 2021, 42, e20200331. [Google Scholar] [CrossRef]
- Casassola, G.M.; Gonçalves, G.R.; Stallbaum, J.H.; Pivetta, H.M.F.; Braz, M.M. Intervenções fisioterapêuticas utilizadas na reabilitação funcional do membro superior de mulheres pós-mastectomia. Fisioter. Bras. 2020, 21, 93–103. [Google Scholar] [CrossRef]
- Mathieu, J.; Daneau, C.; Lemeunier, N.; Doyon, A.; Marchand, A.-A.; Descarreaux, M. Conservative interventions and clinical outcome measures used in the perioperative rehabilitation of breast cancer patients undergoing mastectomy: A scoping review. BMC Womens Health 2022, 22, 343. [Google Scholar] [CrossRef]
- JBI. Supporting Document for the Joanna Briggs Institute Levels of Evidence and Grades of Recommendation. Adelaide. 2014. Available online: https://jbi.global/sites/default/files/2019-05/JBI%20Levels%20of%20Evidence%20Supporting%20Documents-v2.pdf (accessed on 1 June 2025).
- Zeighami Mohammadi, S.; Mohammad Khan Kermanshahi, S.; Vanaki, Z. Reconstruction of feminine identity: The strategies of women with breast cancer to cope with body image altered. Int. J. Women’s Health 2018, 10, 689–697. [Google Scholar] [CrossRef] [PubMed]
- Latifi, M.; Salimi, S.; Barahmand, N.; Fahimnia, F.; Allahbakhshian Farsani, L. Postmastectomy Information Needs and Information-seeking Motives for Women with Breast Cancer. Adv. Biomed. Res. 2018, 7, 75. [Google Scholar]
- Fu, M.R.; Axelrod, D.; Guth, A.A.; Rampertaap, K.; El-Shammaa, N.; Hiotis, K.; Scagliola, J.; Yu, G.; Wang, Y. mHealth self-care interventions: Managing symptoms following breast cancer treatment. mHealth 2016, 2, 28. [Google Scholar] [CrossRef] [PubMed]
- Flores, A.M.; Dwyer, K. Shoulder Impairment Before Breast Cancer Surgery. J. Women’s Health Phys. Therap. 2014, 38, 118–124. [Google Scholar] [CrossRef]
- Lee, M.; Kim, S.; Shim, J. Comparison of Shoulder Range of Motion, Pain, Function, Scapular Position Between Breast Cancer Surgery and Shoulder Surgery Female Patients. Phys. Ther. Korea 2015, 22, 9–18. [Google Scholar] [CrossRef]
- Crosbie, J.; Kilbreath, S.L.; Dylke, E.; Refshauge, K.M.; Nicholson, L.L.; Beith, J.M.; Spillane, A.J.; White, K. Effects of Mastectomy on Shoulder and Spinal Kinematics During Bilateral Upper-Limb Movement. Phys. Ther. 2010, 90, 679–692. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Zhao, L.; Chen, M.; Li, S.; Liao, Y. The effects of rapid rehabilitation nursing on improving postoperative rehabilitation effect and life quality of early breast cancer patients. Medicine 2024, 103, e40533. [Google Scholar] [CrossRef] [PubMed]
- Truong, A.N. Rehabilitation of Patients with Breast Cancer. In Breast Cancer; Springer: New York, NY, USA, 2001; pp. 430–451. [Google Scholar]
- Kamusińska, E.; Ciosek, M.; Karwat, I.D. The importance of rehabilitation in the treatment of breast cancer. Med. Stud. 2014, 3, 214–220. [Google Scholar] [CrossRef]
- Kuliński, W.; Kosno, M. Quality of life in women after mastectomy. clinical and social study. Wiadomości Lek. 2021, 74, 429–435. [Google Scholar] [CrossRef]
- Mehta, J.; Vaghela, N.; Patel, H. The effect of physiotherapy in patients with modified radical mastectomy. Natl. J. Physiol. Pharm. Pharmacol. 2017, 8, 163–166. [Google Scholar] [CrossRef]
- Ahmed, E.; Sayed, A.; Mekkawy, M. Effect of Applying Shoulder Exercises on Shoulder Function after Modified Radical Mastectomy. Assiut Sci. Nurs. J. 2017, 5, 74–84. [Google Scholar]
- Park, H.S.; Cho, G.Y.; Park, K.Y. The Effects of a Rehabilitation Program on Physical Health, Physiological Indicator and Quality of Life in Breast Cancer Mastectomy Patients. J. Korean Acad. Nurs. 2006, 36, 310. [Google Scholar] [CrossRef]
- Elder, E.E.; Brandberg, Y.; Björklund, T.; Rylander, R.; Lagergren, J.; Jurell, G.; Wickman, M.; Sandelin, K. Quality of life and patient satisfaction in breast cancer patients after immediate breast reconstruction: A prospective study. Breast 2005, 14, 201–208. [Google Scholar] [CrossRef]
- Soanes, L.; White, I.D. Sexual Consequences of Cancer and Its Treatment in Adolescents and Young Adults. In Cancer in Adolescents and Young Adults; Springer International Publishing: Cham, Switzerland, 2017; pp. 603–631. [Google Scholar]


{kind=link}
{kind=link}
| References | Objectives | Interventions | Level of Evidence |
|---|---|---|---|
| [22] | Recognise the importance of the nurse in the post-operative period to assist women in rehabilitation after mastectomy with axillary lymph node dissection. | - Education for mastectomised women on shoulder mobilisation, medication administration, weightlifting, and anxiety control. - Promotion of self-care, encouraging physical exercise and skin care. - Psychological support through listening and welcoming to help women cope with body image changes, define strategies for self-image acceptance, involve family, develop individualised care plans, and guide towards community support groups. | 2.b Systematic review of quasi-experimental designs |
| [23] | Describe the experiences of mastectomised women in the home setting. Identify the importance attributed by women to the intervention of the Rehabilitation Nurse. | - Empower, educate, and teach about exercises to improve the range of motion and reduce oedema, the use of devices like compression sleeves, and skin care. - Promotion of functionality using strategies to perform ADL with less pain and effort, and task adaptation to facilitate independence. - Emotional support promoting acceptance and self-confidence. | 3 Single qualitative study |
| [24] | Identify nursing actions that restore self-esteem in patients undergoing mastectomy. | - Prevent complications secondary to surgery and promote independence in functional capacity recovery. - Perform physical exercises and lymphatic drainage exercises. - Emotional support for prevention of psychological and body image-related complications. - Encourage self-reflection. - Support return-to-life activities, social, leisure, work, and family. - Implement respiratory rehabilitation programs. | 3.b Systematic review of comparable cohorts |
| [25] | Recognise how mastectomised women describe and understand the nursing care received in a rehabilitation centre. | - Education on lymphedema prevention. - Perform physical exercises aimed at preventing and controlling complications with the arm and shoulder after surgery. - Promote social and leisure activities (such as discussion groups). | 3 Single qualitative study |
| [26] | Map the use of exergames in the rehabilitation of individuals undergoing breast surgery, identifying health gains from implementing this technology. | - Functional exercises associated with exergames. | 1.b Systematic review of RCT |
| [15] | What is the relationship between implementing a rehabilitation program and the self-care performance capacity in women undergoing breast surgery with lymph node dissection? | - Education on lymphedema risk-reduction measures, upper limb and cervical spine mobilisation exercises, and scar massage. - Application of a daily 45 min program for 3 months. | 2.c Quasi-experimental prospectively controlled study |
| [27] | Determine the value of using Neuman’s Systems Model in providing care to women undergoing mastectomy. | - Assessment of stressors and their source pre-operatively, peri-operatively, and post-operatively. - Education on the surgical plan and possible complications pre-operatively. - Education on post-operative care. | 1.d Pseudo-RCTs |
| [28] | Analyse scientific productions from the last 10 years addressing actions and guidelines on the discharge plan for women undergoing mastectomy. | - Promotion of self-care, considering the participation of the mastectomised woman herself in the process of preventing complications, recovery, and rehabilitation after surgery. - Education for the woman and family/caregivers about post-operative care and warning signs. - Formulate discharge plans with the woman and family/caregivers. - Emotional support. | 3.b Systematic review of comparable cohorts |
| [29] | Describe the experience lived in an interdisciplinary follow-up centre for mastectomised women at a public university in São Paulo during the beginning of the COVID-19 pandemic. | - Physical exercise for lymphedema reduction and prevention. - Group therapy. - Teaching exercises to be performed at home. - Clarify doubts the woman may have about the process. | 3.d Case—controlled study |
| [30] | Identify functionality indicators and types of interventions used for functional assessment and rehabilitation of the upper limb in post-mastectomy women. | - Perform joint mobilisation, stretching, and muscle strengthening. | 1.b Systematic review of RCT |
| [31] | Identify and describe conservative interventions and clinical outcome assessment tools used in the peri-operative physical rehabilitation of women with breast cancer awaiting or having undergone mastectomy. | - Patient education. - Performance of physical exercise. - Performance of lymphatic drainage. - Assessment of shoulder joint range of motion. - Assessment of muscle strength. | 2.b Systematic review of quasi-experimental designs |
| Interventions: | Articles: |
|---|---|
| Education on care for upper limb mobilisation and lymphedema prevention. | [15,22,23,25,31] |
| Promotion of self-care. | [22,28] |
| Empowerment for return to daily life activities. | [23,24] |
| Education for family/caregivers. | [22,28] |
| Education, empowerment, and promotion of physical exercise. | [23,29] |
| Emotional and social support. | [22,24,27,28] |
| Performance of exercises for muscle strengthening and lymphedema prevention. | [25,26,28,29,30,31] |
| Functional respiratory rehabilitation. | [24] |
| Assessment of muscle strength and joint range of motion. | [24] |
| Discharge plan with the woman and family/caregivers. | [28] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigues, M.; Deus, I.; Bengalinha, P.; Duro, R.; Carpinteiro, D.; Ferreira, R.; Silva, C.; Fonseca, C. The Role of Rehabilitation Nurses in Empowering Mastectomised Women for Self-Care: A Scoping Review. Int. J. Environ. Res. Public Health 2025, 22, 957. https://doi.org/10.3390/ijerph22060957
Rodrigues M, Deus I, Bengalinha P, Duro R, Carpinteiro D, Ferreira R, Silva C, Fonseca C. The Role of Rehabilitation Nurses in Empowering Mastectomised Women for Self-Care: A Scoping Review. International Journal of Environmental Research and Public Health. 2025; 22(6):957. https://doi.org/10.3390/ijerph22060957
Chicago/Turabian StyleRodrigues, Madalena, Inês Deus, Pedro Bengalinha, Raquel Duro, David Carpinteiro, Rogério Ferreira, Celso Silva, and César Fonseca. 2025. "The Role of Rehabilitation Nurses in Empowering Mastectomised Women for Self-Care: A Scoping Review" International Journal of Environmental Research and Public Health 22, no. 6: 957. https://doi.org/10.3390/ijerph22060957
APA StyleRodrigues, M., Deus, I., Bengalinha, P., Duro, R., Carpinteiro, D., Ferreira, R., Silva, C., & Fonseca, C. (2025). The Role of Rehabilitation Nurses in Empowering Mastectomised Women for Self-Care: A Scoping Review. International Journal of Environmental Research and Public Health, 22(6), 957. https://doi.org/10.3390/ijerph22060957