

Trends in the Use of Non-Pharmaceutical Interventions in Schools During the COVID-19 Pandemic, February 2021 to December 2023: A Mixed Methods Study

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Data Collection and Preparation
2.3. Analyses
3. Results
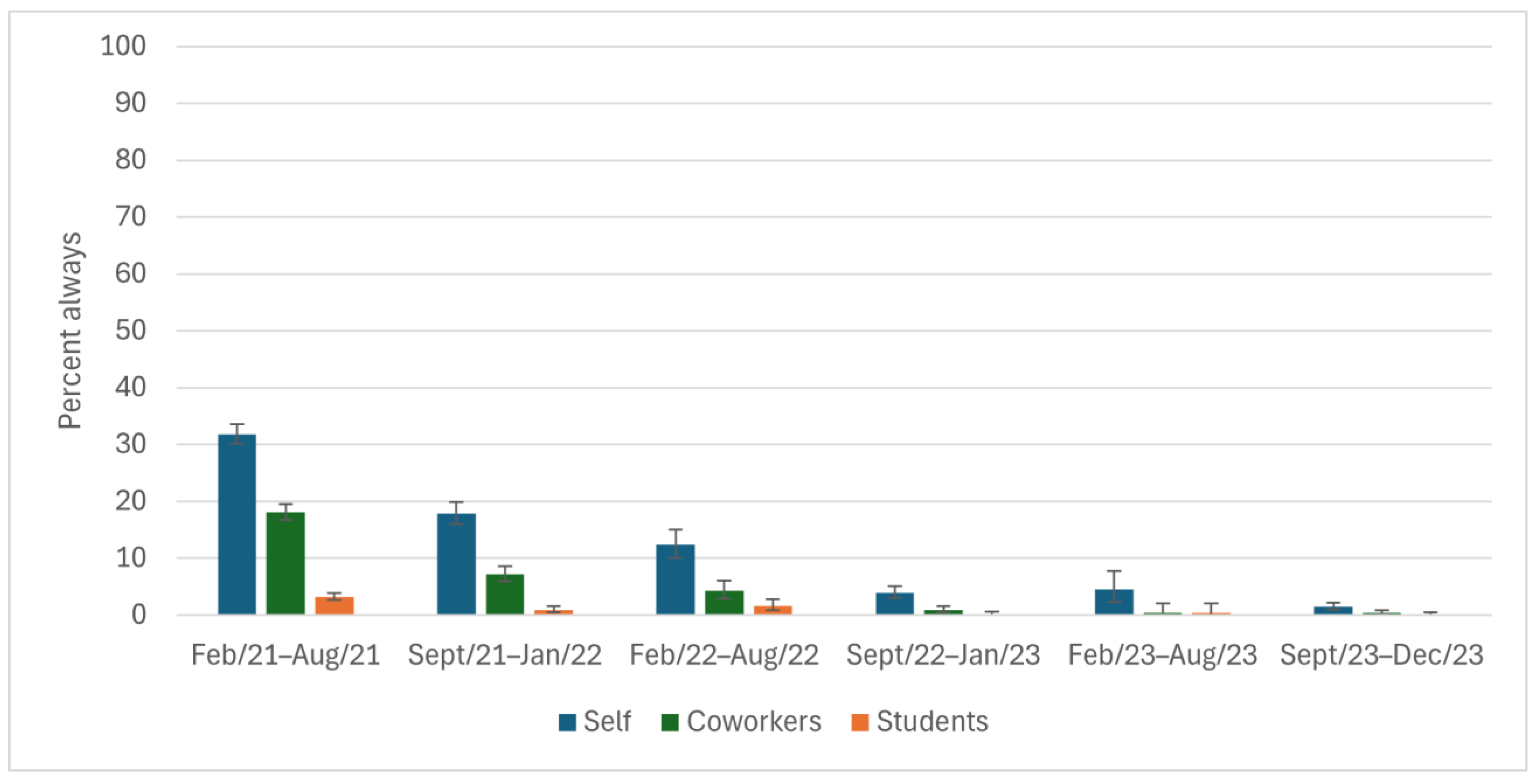
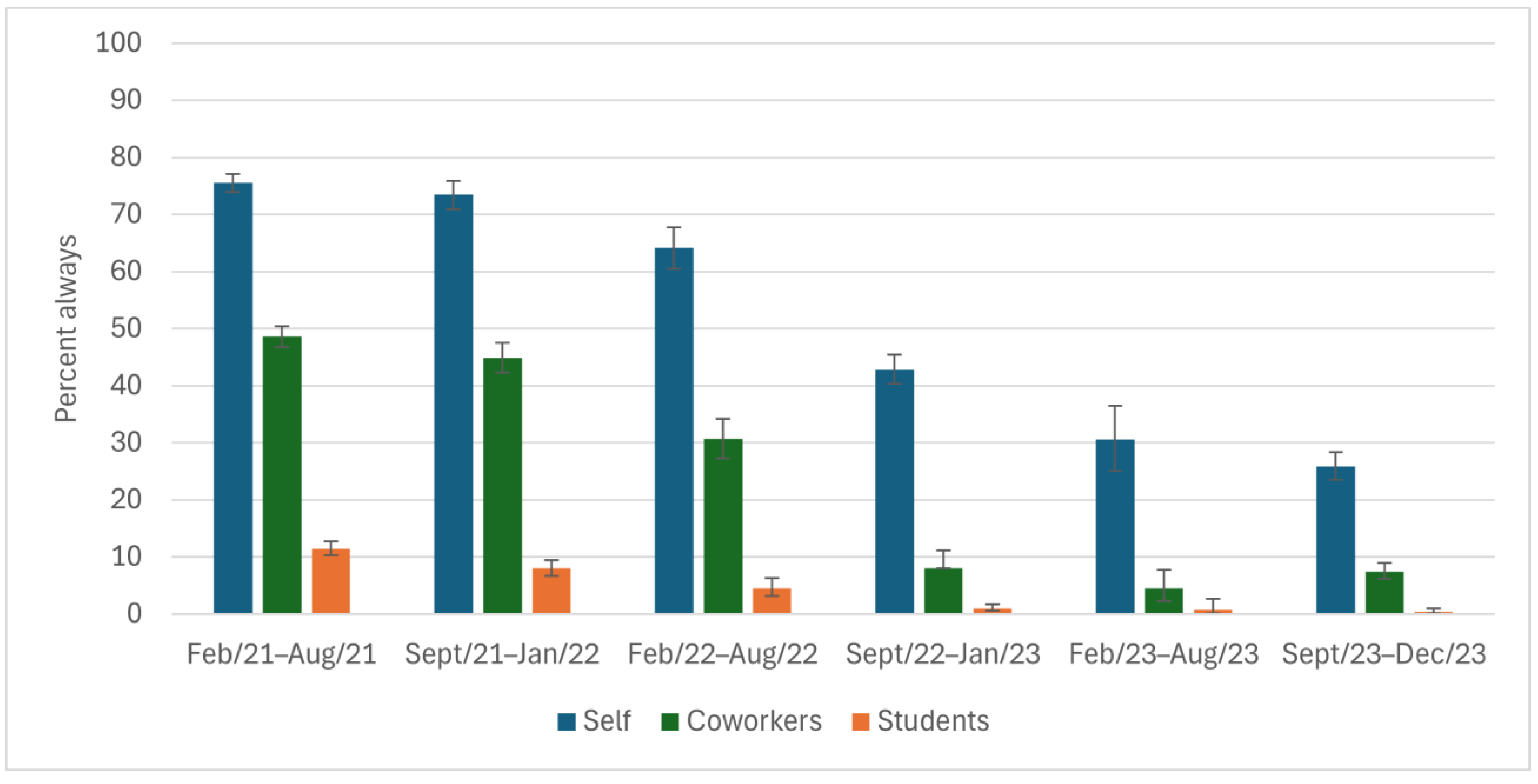
3.1. Quantitative Results: Reported Use over Time
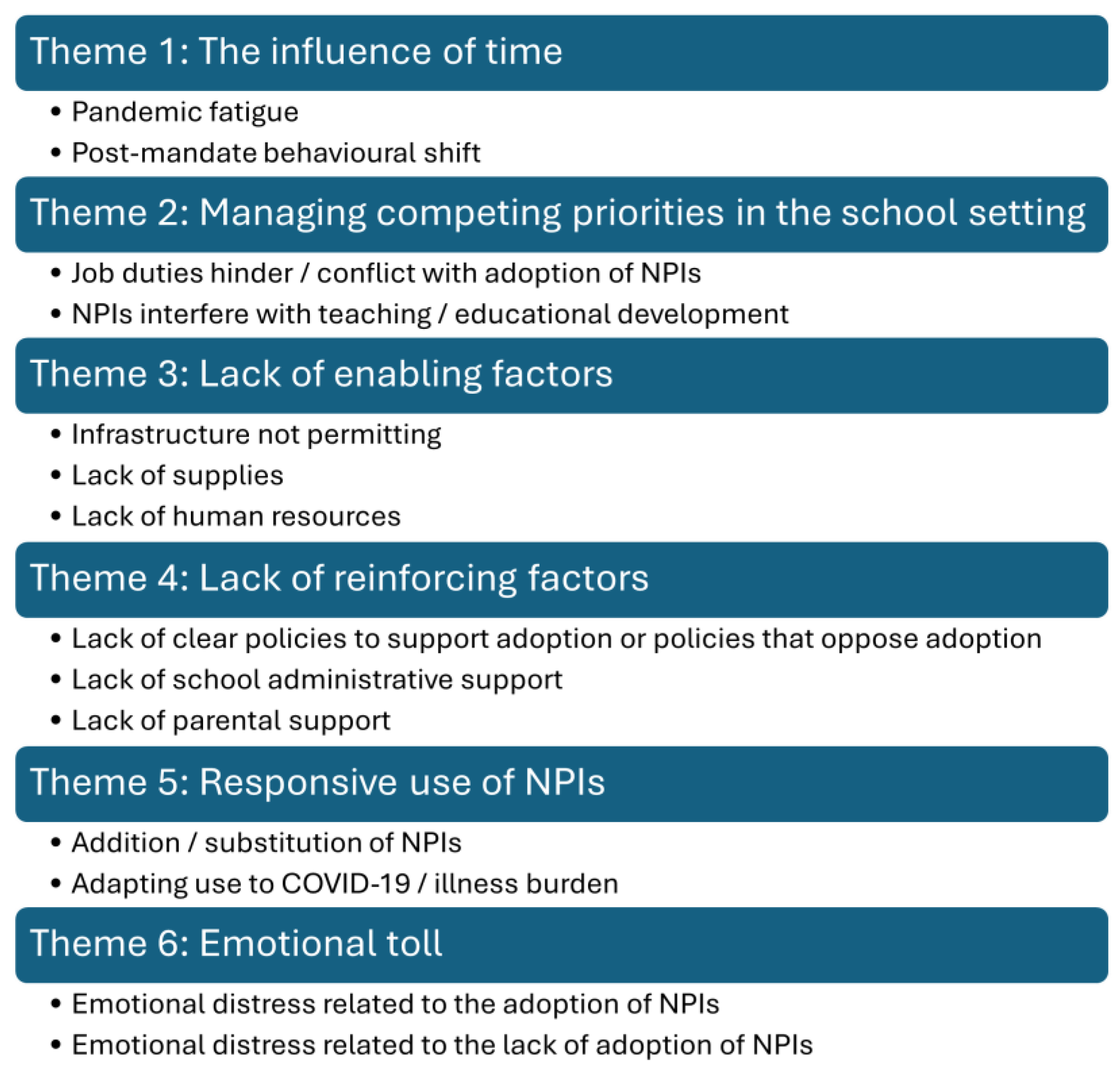
3.2. Qualitative Results: Themes
3.2.1. Theme 1: The Influence of Time
“Over the past 3 months, fewer & fewer students are adhering to COVID protocols within my school; administration has become lax/no longer interested in enforcement.”(Teacher, secondary school, March 2021)
“I can say that students have become less and less likely to use hand sanitizer regularly as the pandemic continues. Additionally, they are becoming more and more relaxed about masks and the new thing is to wear them under their noses.”(Teacher, mixed elementary and secondary school, April 2021)
“The majority of staff and students comply but I have noticed a difference in the strict adherence to physically distancing and masking. They are more relaxed.”(Administrator, elementary school, December 2021)
“When masking requirements dropped many teachers and students at my schools stopped trying to avoid spreading illness.”(Teacher, elementary school, July 2022)
“There was a big change in masking when mandate was dropped. Out of twenty students in June, there was only one that continued masking until the end of the school year. About half the staff (maybe as much as 75%) stopped masking when the mandate was removed.”(Teacher, elementary school, July 2022)
“Due to the lifting of isolation requirements when ill, many in my school (including adults & students) still come to school when they have mild to moderate symptoms such as hacking coughs, runny noses, sore throats, fatigue..etc.”(Teacher, elementary school, October 2022)
“While last year [September 2022–June 2023], the culture at school seemed to be that people stayed home if they were sick, even if symptoms were mild, this year the culture seems to have shifted, and more students and teachers are coming to school sick. Sometimes they mask; sometimes they don’t. The school has returned to pre-Covid rules regarding illness, so employees are required to bring a doctor’s note if they are absent for three days or more.”(Professional support role, elementary and secondary school, October 2023)
“Once the mask mandate was lifted, I really feel like people stopped covering their mouths when they coughed and people came to work sick again.”(Teacher, secondary school, August 2022)
“It seems everything we learned during the pandemic about how to keep each other healthy has been lost.”(Teacher, secondary school, May 2023)
3.2.2. Theme 2: Managing Competing Priorities in the School Setting
“I teach students with special needs, so physically distancing myself is impossible. In order to provide the necessary support, I need to touch their hands, their learning materials, the food containers etc.”(Teacher, secondary school, April 2021)
“Close contact is required with unmasked children to assist with opening containers in lunches during nutrition break. Close contact is also required when assistance is required, for example dressing for outside, helping with shoe, packing or unpacking backpacks, and assisting with toileting accidents.”(Early childhood educator, elementary school, April 2021)
“Physical distancing is tough with my job-guidance deals with private, often confidential information and sometimes upset and/or emotional students. I physical [sic] distance when I can. Sometimes panic attacks etc. (very prevalent now) require student to remove mask to breath and calm down.”(Teacher, secondary school, October 2021)
“I want to wear a mask at work, but I cannot as I have students who read lips. They are hard of hearing.”(Teacher, secondary school, September 2023)
“Covid safety requirements in classrooms are not in line with “best practices” pedagogically-speaking; meaning, what we must do for our health/safety is in direct contrast to what we know is best for kids’ learning in K and Gr. 1. It’s challenging and stressful.”(Teacher, elementary school, August 2021)
“There were many protocols we had to ensure in our schools (handwashing, hand sanitizing, monitoring physical distance, teaching and monitoring protocols) at the same time as being expected to teach all of the curriculum.”(Teacher, elementary school July 2021)
“Getting students to wear their masks consistently and properly is an exhausting struggle”(Teacher, secondary school, December 2021)
“Students are often coming to school sick; I have had several students who seem very ill in class but have come back to school because “they’ve missed too much already.”(Teacher, secondary school, October 2022)
3.2.3. Theme 3: Lack of Enabling Factors
“We do not have enough space to physically distance in a school. This is impossible with class sizes. Let’s stop pretending this is a reality.”(Teacher, elementary school, March 2021)
“I teach grade 2 students and it is very hard for them to remember to physically distance. It is also impossible for everyone in my class including myself to maintain physical distance as it is an overcrowded classroom of 21 students. There is only enough room for the desks in the class to be placed less than 1 m apart.”(Teacher, elementary school, March 2021)
“Students would love to physically distance themselves from me, but there is no room in the classroom for them to do so. Class sizes are larger than they’ve ever been. Even before the pandemic.”(Teacher, elementary school, October 2021)
“I am a kindergarten teacher who was in person until the lockdowns. I was in a room with no sink or bathroom. I was left to only use hand sanitizer for washing hands.”(Teacher, elementary school, May 2021)
“It is impossible to follow all rules in current school settings. Not enough sinks, washrooms to wash hands. One sink per 25 students if we are lucky. By the time hands are washed- a lesson is over.”(Teacher, elementary school, December 2022)
“I’m in a portable. Time is tight and the washroom is far. Handwashing feels like a luxury.”(Teacher, elementary school, October 2023)
“We have everyone sanitize as best we can- but often we are out of sanitizer and are looking for more.”(Educational assistant, elementary school, February 2021)
“Students are required to wear masks but often the masks are ill-fitting and slip off their noses.”(Teacher, secondary school, April 2021)
“The water available for the kids to wash their hands is ice cold. Truly ice cold. It is painful (even as an adult) to wash hands for a full 20 s.”(Teacher, elementary school, January 2022)
“…there is no way to dry our hands—school cannot afford paper towel.”(Teacher, elementary school, October 2023)
“The rules changed a lot over the academic year. No one stayed home unless they tested positive for covid. Education workers couldn’t stay home as there were often no supply/occasional workers to cover us, so we only stayed home if we had covid or if we were required to isolate as someone in our home had covid.“(Teacher, elementary school, July 2022)
“We have almost no supply teachers so staying home makes it challenging for the rest of the school team. Many staff come in sick because they don’t want to strain a system that is already running on duct tape and hope.”(Teacher, elementary school, October 2022)
“We have a severe supply teacher shortage so many, including myself, are coming to school sick because the impact on other staff and the students is so high when we can’t get a supply teacher! I taught 1.5 days last week when I should have been home sick for this reason!”(Teacher, elementary school, October 2022)
3.2.4. Theme 4: Lack of Reinforcing Factors
“I have been directed to return to work on Monday if my result is negative even though Hospital Test Centre says I should isolate.”(Teacher, elementary school, March 2021)
“There is much confusion from the families we teach about when to stay home and for how long. Very little clarity has been given by the board or our union.”(Teacher, elementary school, March 2021)
“Very mixed messages between school boards and what Health Unit recommendations are in situations that cause stress.”(Educational assistant, elementary school, May 2021)
“The [school board] staff ‘attendance program’ has also discouraged sick staff from staying home when ill, in fear, which also may impact medically fragile people.”(Teacher, elementary school, November 2023)
“We are doing the best, but without strict masking guidelines, students are happy to be mask free.”(Principal/vice principal, elementary school, October 2022)
“Even staff who have been off with COVID do not mask upon their return as it is “guidance only.”(Teacher, elementary school, December 2022)
“Staff and students do not generally stay home unless vomiting or feverish, and are returning from being sick and NOT wearing a mask.”(Teacher, elementary school, October 2023)
“1. Many students are still being sent with symptoms. My principal will keep kids at school if she can and they are never placed in the isolation room. 2.When I said my coworkers and I usually wear masks, the only time we don’t is when eating in the staff room. We’re spread out there. There is however 2 non-teaching staff who don’t wear masks after school but our principal doesn’t think Covid is a big deal so it’s not dealt with”.(Teacher, elementary school, March 2021)
“One of my students was sick with a cough and cold and on medication. He was crying and not able to cope with school. My principal would not send the student home.”(Teacher, elementary school, October 2021)
“Our school board has decided that anything related to keeping staff or students safe is a “political issue” and I am quite literally the ONLY person wearing a respirator in my schools... Principals and system administrators refuse to wear a mask, even when clearly symptomatic.”(Teacher, elementary school, October 2023)
“Poverty and affordable child care affects families differently. Many of our families can’t afford to keep their kids at home or stay home from work if they are feeling unwell.”(Teacher, elementary school, July 2021)
“MANY parents send the kids to school deliberately ill and noticeably sick (some with child care needs due to work and some at home parents) in December 2021 at least 1/2 of my class reported being given medication (the pink one- the bubblegum flavour one etc in the AM before school).”(Teacher, elementary school, February 2022)
“Now that COVID protocols have been lifted, parents are sending their sick kids to school every day. Parents are even refusing to pick up their sick children.”(Teacher, elementary school, September 2022)
“It appears that parents believe COVID is over and this year [2022,2023] so many kids are coming to school very sick.”(Teacher, elementary school, October 2022)
3.2.5. Theme 5: Responsive Use of NPIs
“If we need to be closer to them (to give instructions or explain paperwork), then I always wear a face shield on top of my mask.”(Teacher, secondary school, March 2021)
“I wear my mask all the time and eat by myself. I keep windows open all the time.”(Teacher, elementary school, October 2022)
“Last year 99% of my students masked all day. This year 4/27 mask. We have a HEPA filter running in the middle of the classroom. I religiously turn it up to max when they are gone and keep 2+ windows open throughout the entire day.”(Teacher, elementary school, February 2023)
“I use a microphone, but teachers and both administrators (principal and VP) frequently hold their masks off of their faces to project into the room. All should be issued microphones to discourage this behaviour.”(Teacher, elementary school, October 2021)
“I have noticed an uptick in students who are off sick returning and wearing a mask for a few days after their return... the same goes for staff members... I am not currently masking, though I plan to begin again during cold and flu season, especially before I receive my flu shot.”(Teacher, secondary school, September 2023)
“I have worn a mask and distanced at school when positive for COVID. Once I tested negative on RAT test and symptoms subsided, I stopped wearing a mask at work.”(Teacher, elementary school, September 2023)
3.2.6. Theme 6: Emotional Toll
“I used to wear my mask regularly last year but this year I feel some social pressure to not wear the mask as much.”(Teacher, secondary school, October 2023)
“I am the only masking member of staff, and it is deeply unpopular with my colleagues, who talk about my “paranoia” and speculate, publicly, about my mental health.”(Teacher, secondary school, October 2023)
“I stayed home 3 days (+2 days from the weekend), because the internet said it was less contagious after 5 days, and wore a mask the first day back, but that alarmed students because they thought I had COVID, so I didn’t wear a mask the Friday.”(Teacher, secondary school, October 2023)
“We have no choice but to risk health for employment. Many in schools refuse to follow public health measures.”(Teacher, secondary school, March 2021)
“Very few other teachers or students wearing masks at school. Lots of people coming into school when sick, it feels very dangerous and stressful.”(Teacher, elementary school, October 2022)
“Admin does NOT wear masks, they tell us Covid is over!?? So many students & staff are continually sick & often don’t stay home. I am seeing already that Long Covid will be the reality for many staff & students 2, 3 + reinfections of Covid seems to be the norm. I am living a nightmare everyday—no-one seems worried or concerned. I am terrified for the future.”(Teacher, elementary school, February 2023)
“It seems so bizarre to me that with the 6th wave here and being recommended to continue wearing masks (indoors with people) that schools and people inside no longer are mandated to do so? I do not feel safe in this environment!”(Educational assistant, secondary school, April 2022)
“The complete disregard for the health and safety of the medically vulnerable (including myself) during this time of the pandemic has been disheartening and a complete failure of the provincial government and public health.”(Teacher, elementary school, January 2023)
4. Discussion
5. Study Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Novel Coronavirus (2019-nCoV): Situation Report—1: 21 January 2020. 2020. Available online: https://www.who.int/publications/m/item/situation-report---1 (accessed on 30 October 2024).
- Hoofman, J.; Secord, E. The Effect of COVID-19 on Education. Pediatr. Clin. N. Am. 2021, 68, 1071–1079. [Google Scholar] [CrossRef] [PubMed]
- Mazrekaj, D.; De Witte, K. The Impact of School Closures on Learning and Mental Health of Children: Lessons From the COVID-19 Pandemic. Perspect. Psychol. Sci. 2024, 19, 686–693. [Google Scholar] [CrossRef] [PubMed]
- Science, M.; Thampi, N.; Bitnun, A.; Born, K.B.; Blackman, N.; Cohen, E.; Cohn, R.D.; Dubey, V.; Gallagher-Mackay, K.; Khan, S.; et al. Infection prevention and control considerations for schools during the 2022–2023 academic year. In Science Briefs of the Ontario COVID-19 Science Advisory Table; The Ontario COVID-19 Science Advisory Table: Toronto, ON, Canada, 2022; Volume 3. [Google Scholar] [CrossRef]
- Whitley, J.; Beauchamp, M.H.; Brown, C. The impact of COVID-19 on the learning and achievement of vulnerable Canadian children and youth. Facets 2021, 6, 1693–1713. [Google Scholar] [CrossRef]
- Public Health Agency of Canada. Non-Pharmaceutical Interventions to Reduce SARS-CoV-2 and COVID-19 with Relative Hospitalization Rates. 2022. Available online: https://www.canada.ca/en/public-health/services/reports-publications/canada-communicable-disease-report-ccdr/monthly-issue/2022-48/issue-10-october-2022/effectiveness-non-pharmaceutical-interventions-reduce-sars-cov-2-transmission-canada-association-covid-19-hospitalization-rates.html (accessed on 1 November 2024).
- Government of Ontario Newsroom. Ontario Confirms First Case of Wuhan Novel Coronavirus. 2020. Available online: https://news.ontario.ca/en/release/55486/ontario-confirms-first-case-of-wuhan-novel-coronavirus (accessed on 1 November 2024).
- Office of the Premier; Government of Ontario Newsroom. Ontario Enacts Declaration of Emergency to Protect the Public. 2020. Available online: https://news.ontario.ca/en/release/56356/ontario-enacts-declaration-of-emergency-to-protect-the-public (accessed on 1 November 2024).
- Office of the Premier; Government of Ontario Newsroom. School Closures Extended to Keep Students, Staff and Families Safe. 2020. Available online: https://news.ontario.ca/en/release/56776/school-closures-extended-to-keep-students-staff-and-families-safe (accessed on 1 November 2024).
- Office of the Premier; Government of Ontario Newsroom. Ontario Extends School and Child Care Closures to Fight Spread of COVID-19. 2020. Available online: https://news.ontario.ca/en/release/56529/ontario-extends-school-and-child-care-closures-to-fight-spread-of-covid-19 (accessed on 1 November 2024).
- Office of the Premier; Government of Ontario Newsroom. Health and Safety Top Priority as Schools Remain Closed. 2020. Available online: https://news.ontario.ca/en/release/56971/health-and-safety-top-priority-as-schools-remain-closed (accessed on 1 November 2024).
- Gallagher-Mackay, K.; Srivastava, P.; Underwood, K.; Dhuey, E.; McCready, L.; Born, K.B.; Maltsev, A.; Perkhun, A.; Steiner, R.; Barrett, K.; et al. COVID-19 and Education Disruption in Ontario: Emerging Evidence on Impacts. In Science Briefs of the Ontario COVID-19 Science Advisory Table; The Ontario COVID-19 Science Advisory Table: Toronto, ON, Canada, 2021; Volume 2. [Google Scholar] [CrossRef]
- Ontario COVID-19 Science Advisory Table. Ontario Returns to School: An Overview of the Science. 2022. Available online: https://covid19-sciencetable.ca/wp-content/uploads/2022/01/Ontario-Returns-to-School-An-Overview-of-the-Science_20220112-1.pdf (accessed on 11 November 2024).
- Science, M.; Thampi, N.; Bitnun, A.; Allen, U.; Birken, C.; Blackman, N.; Cohen, E.; Dubey, V.; Dye, L.; Gallagher-Mackay, K.; et al. School Operation for the 2021–2022 Academic Year in the Context of the COVID-19 Pandemic. In Science Briefs of the Ontario COVID-19 Science Advisory Table; The Ontario COVID-19 Science Advisory Table: Toronto, ON, Canada, 2021; Volume 2. [Google Scholar] [CrossRef]
- Viner, R.; Russell, S.; Saulle, R.; Croker, H.; Stansfield, C.; Packer, J.; Nicholls, D.; Goddings, A.-L.; Bonell, C.; Hudson, L.; et al. School Closures During Social Lockdown and Mental Health, Health Behaviors, and Well-being Among Children and Adolescents During the First COVID-19 Wave: A Systematic Review. JAMA Pediatr. 2022, 176, 400–409. [Google Scholar] [CrossRef]
- Mossong, J.; Hens, N.; Jit, M.; Beutels, P.; Auranen, K.; Mikolajczyk, R.; Massari, M.; Salmaso, S.; Tomba, G.S.; Wallinga, J.; et al. Social Contacts and Mixing Patterns Relevant to the Spread of Infectious Diseases. PLoS Med. 2008, 5, e74. [Google Scholar] [CrossRef]
- Haug, N.; Geyrhofer, L.; Londei, A.; Dervic, E.; Desvars-Larrive, A.; Loreto, V.; Pinior, B.; Thurner, S.; Klimek, P. Ranking the effectiveness of worldwide COVID-19 government interventions. Nat. Hum. Behav. 2020, 4, 1303–1312. [Google Scholar] [CrossRef]
- Ontario Ministry of Education. Archived—Approach to Reopening Schools for the 2020–2021 School Year. 2020. Available online: https://www.ontario.ca/page/approach-reopening-schools-2020-2021-school-year#section-5 (accessed on 1 November 2024).
- Ontario Ministry of Education. Archived—COVID-19: Health, Safety and Operational Guidance for Schools (2021–2022). 2021. Available online: https://www.ontario.ca/document/covid-19-health-safety-and-operational-guidance-schools-2021-2022 (accessed on 1 November 2024).
- Jarnig, G.; Kerbl, R.; van Poppel, M.N.M. How Middle and High School Students Wear Their Face Masks in Classrooms and School Buildings. Healthcare 2022, 10, 1641. [Google Scholar] [CrossRef] [PubMed]
- Amin-Chowdhury, Z.; Bertran, M.; Kall, M.; Ireland, G.; Aiano, F.; Powell, A.; Jones, S.E.; Brent, A.J.; Brent, B.E.; Baawuah, F.; et al. Parents’ and teachers’ attitudes to and experiences of the implementation of COVID-19 preventive measures in primary and secondary schools following reopening of schools in autumn 2020: A descriptive cross-sectional survey. BMJ Open 2022, 12, e052171. [Google Scholar] [CrossRef]
- España, G.; Cavany, S.; Oidtman, R.; Barbera, C.; Costello, A.; Lerch, A.; Poterek, M.; Tran, Q.; Wieler, A.; Moore, S.; et al. Impacts of K-12 school reopening on the COVID-19 epidemic in Indiana, USA. Epidemics 2021, 37, 100487. [Google Scholar] [CrossRef]
- Hast, M.; Swanson, M.; Scott, C.; Oraka, E.; Espinosa, C.; Burnett, E.; Kukielka, E.A.; Rice, M.E.; Mehari, L.; McCloud, J.; et al. Prevalence of risk behaviors and correlates of SARS-CoV-2 positivity among in-school contacts of confirmed cases in a Georgia school district in the pre-vaccine era, December 2020–January 2021. BMC Public Health 2022, 22, 101. [Google Scholar] [CrossRef]
- Heinsohn, T.; Lange, B.; Vanella, P.; Rodiah, I.; Glöckner, S.; Joachim, A.; Becker, D.; Brändle, T.; Dhein, S.; Ehehalt, S.; et al. Infection and transmission risks of COVID-19 in schools and their contribution to population infections in Germany: A retrospective observational study using nationwide and regional health and education agency notification data. PLoS Med. 2022, 19, e1003913. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Bajaj, A.; Mohanty, V.; Arora, S.; Gangil, N.; Grover, S. Assessing Social Distancing Strategies in Government Schools of Delhi, India: A Formative Research Study. Int. J. Clin. Pediatr. Dent. 2023, 16, 101–106. [Google Scholar] [CrossRef]
- Kratzer, S.; Pfadenhauer, L.M.; Biallas, R.L.; Featherstone, R.; Klinger, C.; Movsisyan, A.; Rabe, J.E.; Stadelmaier, J.; Rehfuess, E.; Wabnitz, K.; et al. Unintended consequences of measures implemented in the school setting to contain the COVID-19 pandemic: A scoping review. Cochrane Database Syst. Rev. 2022, 6, Cd015397. [Google Scholar] [CrossRef]
- Krishnaratne, S.; Littlecott, H.; Sell, K.; Burns, J.; Rabe, J.E.; Stratil, J.M.; Litwin, T.; Kreutz, C.; Coenen, M.; Geffert, K.; et al. Measures implemented in the school setting to contain the COVID-19 pandemic. Cochrane Database Syst. Rev. 2022, 1, Cd015029. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Pol, S.J.; Korczak, D.J.; Coelho, S.; Segovia, A.; Matava, C.T.; Parekh, R.S.; Science, M.; Caldeira-Kulbakas, M.; Crosbie, J.; et al. Impact of COVID-19 Public Health Protocols on Teachers Instructing Children and Adolescents During an In-Person Simulation. J. Can. Acad. Child Adolesc. Psychiatry 2022, 31, 52–63. [Google Scholar]
- Littlecott, H.; Krishnaratne, S.; Burns, J.; Rehfuess, E.; Sell, K.; Klinger, C.; Strahwald, B.; Movsisyan, A.; Metzendorf, M.I.; Schoenweger, P.; et al. Measures implemented in the school setting to contain the COVID-19 pandemic. Cochrane Database Syst. Rev. 2024, 5, Cd015029. [Google Scholar] [CrossRef] [PubMed]
- Mickells, G.E.; Figueroa, J.; West, K.W.; Wood, A.; McElhanon, B.O. Adherence to Masking Requirement During the COVID-19 Pandemic by Early Elementary School Children. J. Sch. Health 2021, 91, 555–561. [Google Scholar] [CrossRef]
- Statistics Canada. Research to Insights: A Look at Canada’s Economy and Society Three Years After the Start of the COVID-19 Pandemic. 2023. Available online: https://www150.statcan.gc.ca/n1/pub/11-631-x/11-631-x2023004-eng.htm (accessed on 15 September 2024).
- Government of Ontario. Statement from Ontario’s Chief Medical Officer of Health. 2022. Available online: https://news.ontario.ca/en/statement/1001732/statement-from-ontarios-chief-medical-officer-of-health (accessed on 5 December 2024).
- Coleman, B.L.; Gutmanis, I.; Bondy, S.J.; Harrison, R.; Langley, J.; Fischer, K.; Cooper, C.; Valiquette, L.; Muller, M.P.; Powis, J.; et al. Canadian health care providers’ and education workers’ hesitance to receive original and bivalent COVID-19 vaccines. Vaccine 2024, 42, 126271. [Google Scholar] [CrossRef]
- Creswell, J.W. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches, 3rd ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2009. [Google Scholar]
- Creswell, J.W.; Plano-Clark, V.L. Designing and Conducting Mixed Methods Research; SAGE Publications: Thousand Oaks, CA, USA, 2007. [Google Scholar]
- Rossman, G.B.; Wilson, B.L. Numbers and Words: Combining Quantitative and Qualitative Methods in a Single Large-Scale Evaluation Study. Eval. Rev. 1985, 9, 627–643. [Google Scholar] [CrossRef]
- Fereday, J.; Muir-Cochrane, E. Demonstrating Rigor Using Thematic Analysis: A Hybrid Approach of Inductive and Deductive Coding and Theme Development. Int. J. Qual. Methods 2006, 5, 80–92. [Google Scholar] [CrossRef]
- Crabtree, B.F.; Miller, W.F. A template approach to text analysis: Developing and using codebooks. In Doing Qualitative Research; Research Methods for Primary Care; Sage Publications, Inc.: Thousand Oaks, CA, USA, 1992; Volume 3, pp. 93–109. [Google Scholar]
- Roberts, K.; Dowell, A.; Nie, J.-B. Attempting rigour and replicability in thematic analysis of qualitative research data; a case study of codebook development. BMC Med. Res. Methodol. 2019, 19, 66. [Google Scholar] [CrossRef]
- Boyatzis, R. Transforming Qualitative Information: Thematic Analysis and Code Development; Sage: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- Proudfoot, K. Inductive/Deductive Hybrid Thematic Analysis in Mixed Methods Research. J. Mix. Methods Res. 2023, 17, 308–326. [Google Scholar] [CrossRef]
- StataCorp. Stata Statistical Software: Release 18.5; StataCorp LLC: College Station, TX, USA, 2024. [Google Scholar]
- SocioCultural Research Consultants LLC. Dedoose Version 9.2.22, Cloud Application for Managing, Analyzing, and Presenting Qualitative and Mixed Method Research Data; SocioCultural Research Consultants LLC: Los Angeles, CA, USA, 2024. [Google Scholar]
- Gershon, R.R.M.; Karkashian, C.D.; Grosch, J.W.; Murphy, L.R.; Escamilla-Cejudo, A.; Flanagan, P.A.; Bernacki, E.; Kasting, C.; Martin, L. Hospital safety climate and its relationship with safe work practices and workplace exposure incidents. Am. J. Infect. Control 2000, 28, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Zohair, D. Safety climate in industrial organizations: Theoretical and applied implications. J. Appl. Psychol. 1980, 65, 96–102. [Google Scholar] [CrossRef]
- Serrano, F.; Saragosa, M.; Nowrouzi-Kia, B.; Woodford, L.; Casole, J.; Gohar, B. Understanding Education Workers’ Stressors after Lockdowns in Ontario, Canada: A Qualitative Study. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 836–849. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.M.; Oudyk, J.; Cedillo, L.; Inouye, K.; Potter, G.; Mustard, C. Perceived Adequacy of Infection Control Practices and Symptoms of Anxiety Among In-Person Elementary School Educators in Ontario. J. Occup. Environ. Med. 2022, 64, e763–e768. [Google Scholar] [CrossRef]
- Public Health Agency of Canada. Respiratory Infectious Diseases: How to Reduce the Spread with Personal Protective Measures. 2024. Available online: https://www.canada.ca/en/public-health/services/diseases/respiratory-infectious-diseases-reduce-spread-personal-protective-measures.html (accessed on 12 December 2024).
- U.S. Centers for Disease Control and Prevention. Hygiene and Respiratory Viruses Prevention. 2024. Available online: https://www.cdc.gov/respiratory-viruses/prevention/hygiene.html (accessed on 11 December 2024).
- Lau, C.H.; Springston, E.E.; Sohn, M.W.; Mason, I.; Gadola, E.; Damitz, M.; Gupta, R.S. Hand hygiene instruction decreases illness-related absenteeism in elementary schools: A prospective cohort study. BMC Pediatr. 2012, 12, 52. [Google Scholar] [CrossRef]
- U.S. Centers for Disease Control and Prevention. Preventing Spread of Infections in K-12 Schools. 2024. Available online: https://www.cdc.gov/orr/school-preparedness/infection-prevention/index.html (accessed on 9 December 2024).
- Chang, L.Y.; Wang, C.J.; Chiang, T.L. Childhood Handwashing Habit Formation and Later COVID-19 Preventive Practices: A Cohort Study. Acad. Pediatr. 2022, 22, 1390–1398. [Google Scholar] [CrossRef]
- U.S. Centers for Disease Control and Prevention. About Hand Hygiene as a Family Activity. 2024. Available online: https://www.cdc.gov/clean-hands/prevention/index.html (accessed on 13 November 2024).
- Kim, J.; Oh, S. The relationship between mothers’ knowledge and practice level of cough etiquette and their children’s practice level in South Korea. Child Health Nurs. Res. 2021, 27, 385–394. [Google Scholar] [CrossRef]
- Howard, J.T.; Howard, K.J. The effect of perceived stress on absenteeism and presenteeism in public school teachers. J. Workplace Behav. Health 2020, 35, 100–116. [Google Scholar] [CrossRef]
- Kim, J.; Suh, E.E.; Ju, S.; Choo, H.; Bae, H.; Choi, H. Sickness Experiences of Korean Registered Nurses at Work: A Qualitative Study on Presenteeism. Asian Nurs. Res. Korean Soc. Nurs. Sci. 2016, 10, 32–38. [Google Scholar] [CrossRef]
- Woodland, L.; Brooks, S.K.; Webster, R.K.; Amlôt, R.; Rubin, G.J. Risk factors for school-based presenteeism in children: A systematic review. BMC Psychol. 2023, 11, 169. [Google Scholar] [CrossRef] [PubMed]
- Czumbel, I.; Quinten, C.; Lopalco, P.; Semenza, J.C. Management and control of communicable diseases in schools and other child care settings: Systematic review on the incubation period and period of infectiousness. BMC Infect. Dis. 2018, 18, 199. [Google Scholar] [CrossRef]
- Richardson, M.; Elliman, D.; Maguire, H.; Simpson, J.; Nicoll, A. Evidence base of incubation periods, periods of infectiousness and exclusion policies for the control of communicable diseases in schools and preschools. Pediatr. Infect. Dis. J. 2001, 20, 380–391. [Google Scholar] [CrossRef]
- Gravina, N.; Nastasi, J.A.; Sleiman, A.A.; Matey, N.; Simmons, D.E. Behavioral strategies for reducing disease transmission in the workplace. J. Appl. Behav. Anal. 2020, 53, 1935–1954. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, F.; Ontario College of Teachers. Transition to Teaching 2021: 20th Annual Survey of Ontario’s Early-Career Elementary and Secondary Teachers. 2021. Available online: https://www.oct.ca/-/media/PDF/transition_to_teaching_2021/2021T2Ten.pdf (accessed on 10 December 2024).
- Woodland, L.; Smith, L.E.; Webster, R.K.; Amlôt, R.; Rubin, J.G. Why do children attend school, engage in other activities or socialise when they have symptoms of an infectious illness? A cross-sectional survey. BMJ Open 2023, 13, e071599. [Google Scholar] [CrossRef]
- Donaldson, A.L.; Harris, J.P.; Vivancos, R.; O’Brien, S.J. Risk factors associated with outbreaks of seasonal infectious disease in school settings, England, UK. Epidemiol. Infect. 2020, 148, e287. [Google Scholar] [CrossRef] [PubMed]
- Chafloque Céspedes, R.; Vara-Horna, A.; Lopez-Odar, D.; Santi-Huaranca, I.; Diaz-Rosillo, A.; Asencios-Gonzalez, Z. Absenteeism, Presentism and Academic Performance in Students from Peruvian Universities. Propósitos Represent. 2018, 6, 109–133. [Google Scholar] [CrossRef]
- Komp, R.; Kauffeld, S.; Ianiro-Dahm, P. Student Presenteeism in Digital Times-A Mixed Methods Approach. Int. J. Environ. Res. Public Health 2022, 19, 16982. [Google Scholar] [CrossRef]
- Bornand, E.; Letourneux, F.; Deschanvres, C.; Boutoille, D.; Lucet, J.-C.; Lepelletier, D.; Leclere, B.; Mayol, S.; Peiffer-Smadja, N.; Birgand, G. Social representations of mask wearing in the general population during the COVID-19 pandemic. Front. Public Health 2023, 11, 1136980. [Google Scholar] [CrossRef]
- Yang, L.; Constantino, S.M.; Grenfell, B.T.; Weber, E.U.; Levin, S.A.; Vasconcelos, V.V. Sociocultural determinants of global mask-wearing behavior. Proc. Natl. Acad. Sci. USA 2022, 119, e2213525119. [Google Scholar] [CrossRef] [PubMed]
- Duong, D. Calls for masking in schools as respiratory infections overwhelm children’s hospitals. CMAJ 2022, 194, E1619. [Google Scholar] [CrossRef] [PubMed]
- Neumann, M.; Moore, S.T.; Baum, L.M.; Oleinikov, P.; Xu, Y.; Niederdeppe, J.; Lewis, N., Jr.; Gollust, S.E.; Fowler, E.F. Politicizing Masks? Examining the Volume and Content of Local News Coverage of Face Coverings in the U.S. Through the COVID-19 Pandemic. Political Commun. 2024, 41, 66–106. [Google Scholar] [CrossRef]
- Scoville, C.; McCumber, A.; Amironesei, R.; Jeon, J. Mask Refusal Backlash: The Politicization of Face Masks in the American Public Sphere During the Early Stages of the COVID-19 Pandemic. Socius 2022, 8, 23780231221093158. [Google Scholar] [CrossRef]
- WHO Regional Office for Europe. Pandemic Fatigue: Reinvigorating the Public to Prevent COVID-19. 2020. Available online: https://iris.who.int/bitstream/handle/10665/337574/WHO-EURO-2020-1573-41324-56242-eng.pdf?sequence=1 (accessed on 1 November 2024).
- Brankston, G.; Merkley, E.; Loewen, P.J.; Avery, B.P.; Carson, C.A.; Dougherty, B.P.; Fisman, D.N.; Tuite, A.R.; Poljak, Z.; Greer, A.L. Pandemic fatigue or enduring precautionary behaviours? Canadians’ long-term response to COVID-19 public health measures. Prev. Med. Rep. 2022, 30, 101993. [Google Scholar] [CrossRef]
- Crane, M.A.; Shermock, K.M.; Omer, S.B.; Romley, J.A. Change in Reported Adherence to Nonpharmaceutical Interventions During the COVID-19 Pandemic, April-November 2020. JAMA 2021, 325, 883–885. [Google Scholar] [CrossRef]
- Delussu, F.; Tizzoni, M.; Gauvin, L. Evidence of pandemic fatigue associated with stricter tiered COVID-19 restrictions. PLoS Digit. Health 2022, 1, e0000035. [Google Scholar] [CrossRef]
- Morris, K.J.; Ashida, S.; Ramirez, M.R.; Tarr, G.A.M. Psychological distress as a driver of early COVID-19 pandemic fatigue: A longitudinal analysis of the time-varying relationship between distress and physical distancing adherence among families with children and older adults. BMJ Public Health 2024, 2, e001256. [Google Scholar] [CrossRef]
- Petherick, A.; Goldszmidt, R.; Andrade, E.B.; Furst, R.; Hale, T.; Pott, A.; Wood, A. A worldwide assessment of changes in adherence to COVID-19 protective behaviours and hypothesized pandemic fatigue. Nat. Hum. Behav. 2021, 5, 1145–1160. [Google Scholar] [CrossRef]
- Rader, B.; Sehgal, N.K.R.; Michelman, J.; Mellem, S.; Schultheiss, M.D.; Hoddes, T.; MacFarlane, J.; Clark, G.; O’Banion, S.; Eastham, P.; et al. Adherence to non-pharmaceutical interventions following COVID-19 vaccination: A federated cohort study. NPJ Digit. Med. 2024, 7, 241. [Google Scholar] [CrossRef]
- Wu, X.; Lu, Y.; Jiang, B. Built environment factors moderate pandemic fatigue in social distance during the COVID-19 pandemic: A nationwide longitudinal study in the United States. Landsc. Urban Plan. 2023, 233, 104690. [Google Scholar] [CrossRef] [PubMed]
- Ajiboye, A.S.; Dunphy, C.; Vo, L.; Howard-Williams, M.; Ladva, C.N.; Robinson, S.J.; McCord, R.; Gakh, M.; Weber, R.; Sunshine, G. Changes in Self-Reported Mask Use After the Lifting of State-Issued Mask Mandates in 20 US States, February-June 2021. J. Public Health Manag. Pract. 2024, 30, E335–E343. [Google Scholar] [CrossRef]
- Wollast, R.; Schmitz, M.; Bigot, A.; Speybroeck, N.; Lacourse, É.; de la Sablonnière, R.; Luminet, O. Trajectories of health behaviors during the COVID-19 pandemic: A longitudinal analysis of handwashing, mask wearing, social contact limitations, and physical distancing. Psychol. Health 2024, 39, 1899–1926. [Google Scholar] [CrossRef] [PubMed]
- Armitage, C.J.; Keyworth, C.; Gartland, N.; Coleman, A.; Fishwick, D.; Johnson, S.; van Tongeren, M. Theory-based Trial to Promote Uptake and Sustained Use of Face Coverings During the COVID-19 Pandemic. Ann. Behav. Med. 2023, 57, 921–928. [Google Scholar] [CrossRef] [PubMed]
- Bussemakers, C.; Stappers, N.; Kroese, F.; van den Putte, B.; de Bruin, M. Psychosocial determinants of handwashing and physical distancing behaviour during the COVID-19 pandemic in the Netherlands: A longitudinal analysis. Br. J. Health Psychol. 2025, 30, e12755. [Google Scholar] [CrossRef]
- Bardosh, K.; de Figueiredo, A.; Gur-Arie, R.; Jamrozik, E.; Doidge, J.; Lemmens, T.; Keshavjee, S.; Graham, J.E.; Baral, S. The unintended consequences of COVID-19 vaccine policy: Why mandates, passports and restrictions may cause more harm than good. BMJ Glob. Health 2022, 7, e008684. [Google Scholar] [CrossRef]
- Dominant Variant in Canada: Government of Canada. COVID-19 Epidemiology Update: Current Situation [Internet]. 2024. Available online: https://health-infobase.canada.ca/covid-19/current-situation.html (accessed on 1 October 2024).
- Akanteva, A.; Dick, D.W.; Amiraslani, S.; Heffernan, J.M. Canadian COVID-19 pandemic public health mitigation measures at the province level. Sci. Data 2023, 10, 882. [Google Scholar] [CrossRef]
- Vaccination: Health Canada. Health Canada Authorizes First COVID-19 Vaccine [Internet]. 2020. Available online: https://www.canada.ca/en/health-canada/news/2020/12/health-canada-authorizes-first-covid-19-vaccine0.html (accessed on 1 October 2024).
- Health Canada. Health Canada Authorizes the Use of the Pfizer-BioNTech Comirnaty COVID-19 Vaccine as a Booster Shot [Internet]. 2021. Available online: https://www.canada.ca/en/health-canada/news/2021/11/health-canada-authorizes-the-use-of-the-pfizer-biontech-comirnaty-covid-19-vaccine-as-a-booster-shot.html (accessed on 1 October 2024).
- Health Canada. Health Canada Authorizes First Bivalent COVID-19 Booster for Adults 18 Years and Older [Internet]. Government of Canada, 2022. Available online: https://www.canada.ca/en/health-canada/news/2022/09/health-canada-authorizes-first-bivalent-covid-19-booster-for-adults-18-years-and-older.html (accessed on 1 October 2024).
- Health Canada. Health Canada Authorizes COVID-19 Vaccine Booster Targeting the Omicron BA.4/BA.5 Subvariants [Internet]. 2022. Available online: https://www.canada.ca/en/health-canada/news/2022/10/health-canada-authorizes-covid-19-vaccine-booster-targeting-the-omicron-ba4ba5-subvariants.html (accessed on 1 October 2024).
- Health Canada. Health Canada Authorizes Moderna COVID-19 Vaccine Targeting the Omicron XBB.1.5 Subvariant [Internet]. 2023. Available online: https://www.canada.ca/en/health-canada/news/2023/09/health-canada-authorizes-moderna-covid-19-vaccine-targeting-the-omicron-xbb15-subvariant.html (accessed on 1 October 2024).
- Vaccination (Children/Adolescents): Health Canada. Health Canada Authorizes Use of the Pfizer-BioNTech COVID-19 Vaccine in Children 12 to 15 Years of Age [Internet]. 2021. Available online: https://www.canada.ca/en/health-canada/news/2021/05/health-canada-authorizes-use-of-the-pfizer-biontech-covid-19-vaccine-in-children-12-to-15-years-of-age.html (accessed on 1 October 2024).
- Health Canada. Health Canada Authorizes Use of Comirnaty (the Pfizer-BioNTech COVID-19 Vaccine) in Children 5 to 11 Years of Age [Internet]. 2021. Available online: https://www.canada.ca/en/health-canada/news/2021/11/health-canada-authorizes-use-of-comirnaty-the-pfizer-biontech-covid-19-vaccine-in-children-5-to-11-years-of-age.html (accessed on 1 October 2024).
- Health Canada. Health Canada Authorizes Use of Moderna COVID-19 Vaccine in Children 6 Months to 5 Years of Age [Internet]. 2022. Available online: https://www.canada.ca/en/health-canada/news/2022/07/health-canada-authorizes-use-of-moderna-covid-19-vaccine-in-children-6-months-to-5-years-of-age.html (accessed on 1 October 2024).
- Government of Canada. Regulatory Decision Summary-Comirnaty Original/Omicron BA.1-Health Canada [Internet]. 2022. Available online: https://covid-vaccine.canada.ca/info/regulatory-decision-summary-detail.html?linkID=RDS01012 (accessed on 1 October 2024).
- Government of Canada. Regulatory Decision Summary-Comirnaty Original & Omicron BA.4/BA.5-Health Canada [Internet]. 2022. Available online: https://covid-vaccine.canada.ca/info/regulatory-decision-summary-detail.html?linkID=RDS01006 (accessed on 1 October 2024).
- Government of Canada. Regulatory Decision Summary-Comirnaty Original & Omicron BA.4/BA.5-Health Canada [Internet]. 2022. Available online: https://covid-vaccine.canada.ca/info/regulatory-decision-summary-detail.html?linkID=RDS01030 (accessed on 1 October 2024).
- Public Health Agency of Canada. Summary of NACI Statement of August 19, 2022: Recommendations on the Use of a First Booster Dose of Pfizer-BioNTech Comirnaty COVID-19 Vaccine in Children 5 to 11 Years of Age [Internet]. 2022. Available online: https://www.canada.ca/en/public-health/services/immunization/national-advisory-committee-on-immunization-naci/recommendations-use-first-booster-dose-pfizer-biontech-comirnaty-covid-19-vaccine-children-5-11-years/summary-august-19-2022.html (accessed on 1 October 2024).
- Government of Canada. Regulatory Decision Summary-Spikevax-Health Canada [Internet]. 2023. Available online: https://covid-vaccine.canada.ca/info/regulatory-decision-summary-detail.html?linkID=RDS01052 (accessed on 1 October 2024).
- Government of Canada. Regulatory Decision Summary-Spikevax Bivalent-Health Canada [Internet]. 2023. Available online: https://covid-vaccine.canada.ca/info/regulatory-decision-summary-detail.html?linkID=RDS01076 (accessed on 1 October 2024).
- Government of Canada. Regulatory Decision Summary for Comirnaty Omicron XBB.1.5 [Internet]. 2023. Available online: https://covid-vaccine.canada.ca/info/RDS1695846822831-comirnaty-omicron-xbb-1-5-en.html (accessed on 1 October 2024).
- Mask Mandates: Ontario Ministry of Education. Guide to Reopening Ontario’s Schools [Internet]. 2020. Available online: https://web.archive.org/web/20200901004807/https://www.ontario.ca/page/guide-reopening-ontarios-schools (accessed on 1 October 2024).
- Ontario Ministry of Education. Guide to Reopening Ontario’s Schools [Internet]. 2021. Available online: https://web.archive.org/web/20210303235742/https://www.ontario.ca/page/guide-reopening-ontarios-schools (accessed on 1 October 2024).
- CBC News. Ontario Lifts Mask Mandates in Most Spaces, but It’s No ‘Light Switch’ for Pre-Pandemic Life, Expert Says. 2022. Available online: https://www.cbc.ca/news/canada/toronto/covid19-ont-masks-march-21-2022-1.6385293 (accessed on 1 October 2024).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Participants N = 3617 |
|---|---|
| Age in years, mean (95% CI) | 45.3 (45.0, 46.0) |
| Gender | |
| Female | 3091 (85.5) |
| Male | 517 (14.3) |
| Other | 9 (0.2) |
| Education, highest achieved | |
| Diploma, college, or less | 341 (9.4) |
| Bachelor’s degree/teaching certification | 2441 (67.5) |
| Graduate school (master’s or PhD) | 835 (23.1) |
| Occupation | |
| Teacher | 2923 (80.8) |
| Educational assistant | 224 (6.2) |
| Early childhood educator | 80 (2.2) |
| Principal/vice principal | 133 (3.7) |
| Administration 1 | 87 (2.4) |
| Professional student services roles 2 | 130 (3.6) |
| Support staff 3 | 40 (1.1) |
| Chronic illness 4 | |
| Yes | 921 (25.5) |
| No | 2696 (74.5) |
| Postal district | |
| Eastern Ontario | 643 (17.8) |
| Central Ontario | 1251 (34.6) |
| Metropolitan Toronto | 721 (19.9) |
| Southwestern Ontario | 831 (23.0) |
| Northern Ontario | 171 (4.7) |
| School setting | |
| Elementary | 2227 (61.6) |
| Secondary | 1103 (30.5) |
| Both/mixed setting | 287 (7.9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robertson, N.M.; Fischer, K.; Gutmanis, I.; Zhu, V.; CCS-2 Working Group; Coleman, B.L. Trends in the Use of Non-Pharmaceutical Interventions in Schools During the COVID-19 Pandemic, February 2021 to December 2023: A Mixed Methods Study. Int. J. Environ. Res. Public Health 2025, 22, 394. https://doi.org/10.3390/ijerph22030394
Robertson NM, Fischer K, Gutmanis I, Zhu V, CCS-2 Working Group, Coleman BL. Trends in the Use of Non-Pharmaceutical Interventions in Schools During the COVID-19 Pandemic, February 2021 to December 2023: A Mixed Methods Study. International Journal of Environmental Research and Public Health. 2025; 22(3):394. https://doi.org/10.3390/ijerph22030394
Chicago/Turabian StyleRobertson, Nicole M., Kailey Fischer, Iris Gutmanis, Veronica Zhu, CCS-2 Working Group, and Brenda L. Coleman. 2025. "Trends in the Use of Non-Pharmaceutical Interventions in Schools During the COVID-19 Pandemic, February 2021 to December 2023: A Mixed Methods Study" International Journal of Environmental Research and Public Health 22, no. 3: 394. https://doi.org/10.3390/ijerph22030394
APA StyleRobertson, N. M., Fischer, K., Gutmanis, I., Zhu, V., CCS-2 Working Group, & Coleman, B. L. (2025). Trends in the Use of Non-Pharmaceutical Interventions in Schools During the COVID-19 Pandemic, February 2021 to December 2023: A Mixed Methods Study. International Journal of Environmental Research and Public Health, 22(3), 394. https://doi.org/10.3390/ijerph22030394