
Sugar-Sweetened Beverages, Foods of Low Nutritional Value, and Child Undernutrition in Cambodia

 , ,
, ,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Sociodemographic and Nutritional Status Characteristics
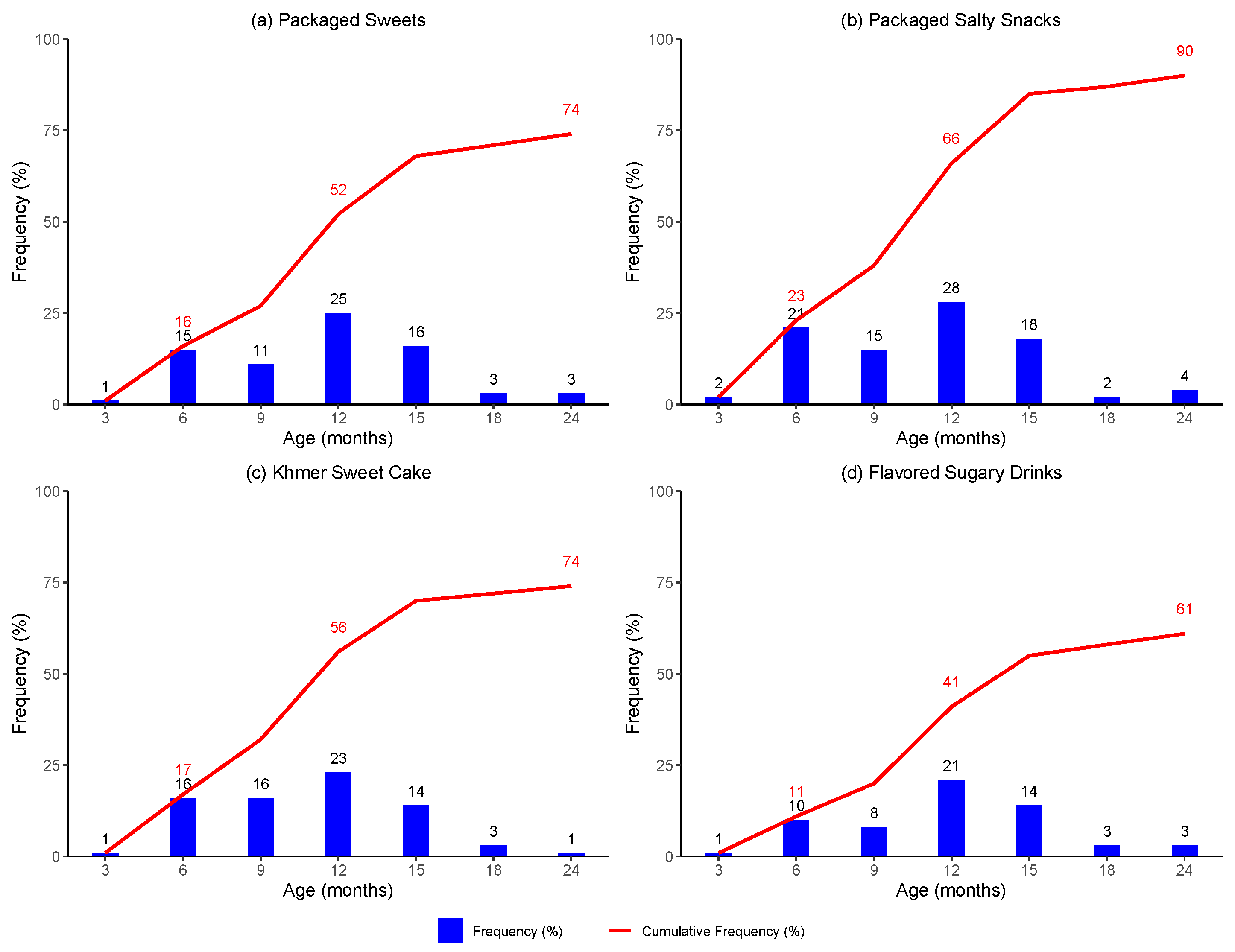
3.2. First Introduction of Foods and Beverages
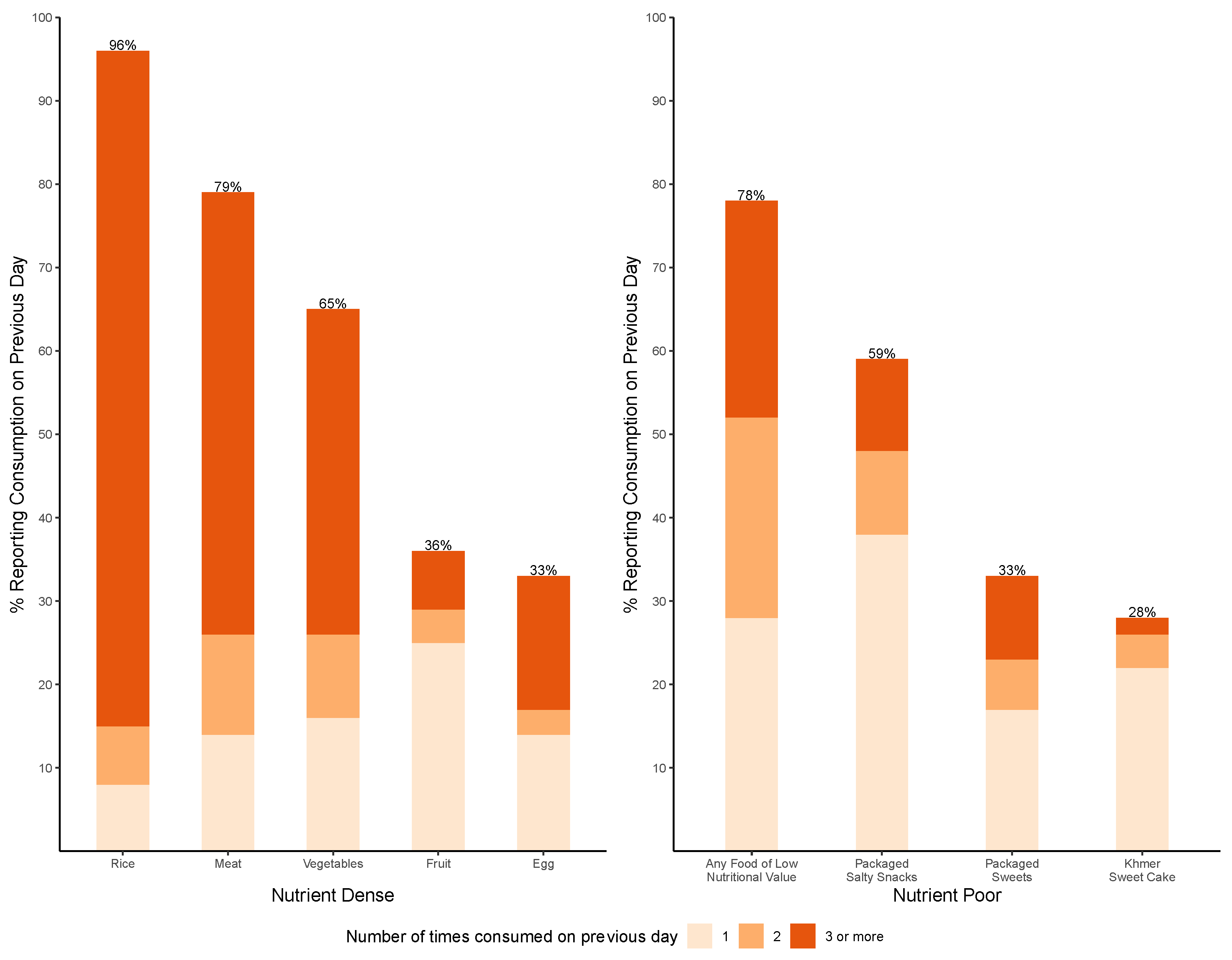
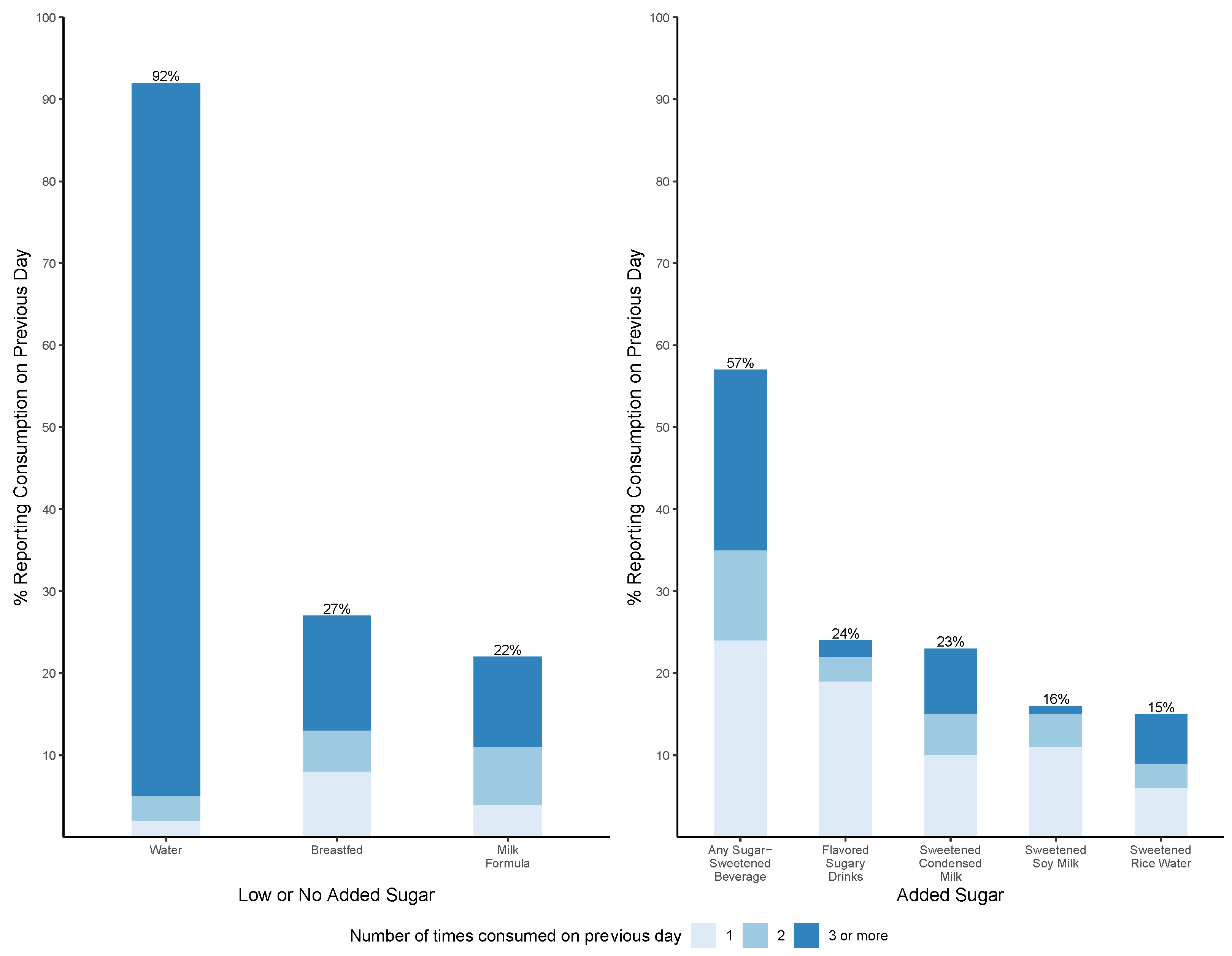
3.3. Frequency of Reported Food and Beverage Intake at 24 Months
3.4. Association between Food and Beverage Intake and Stunting at 24 Months of Age
3.5. Association between Food and Beverage Intake and Wasting at 24 Months of Age
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations Children’s Fund (UNICEF); World Health Organization; International Bank for Reconstruction and Development/The World Bank. Levels and Trends of Child Malnutrition: Key Findings of the 2021 Edition of the Joint Child Malnutrition Estimates. Available online: https://www.who.int/publications/i/item/9789240073791 (accessed on 16 June 2023).
- World Health Organization. Malnutrition. Available online: https://www.who.int/news-room/fact-sheets/detail/malnutrition (accessed on 19 June 2023).
- National Institute of Statistics (NIS) [Cambodia]; Ministry of Health (MoH) [Cambodia]; ICF. Cambodia Demographic and Health Survey 2021–2022 Final Report. Available online: https://dhsprogram.com/publications/publication-FR377-DHS-Final-Reports.cfm (accessed on 16 June 2023).
- World Health Organization; United Nations Children’s Fund (UNICEF). Indicators for Assessing Infant and Young Child Feeding Practices. Available online: https://www.who.int/publications/i/item/9789240018389 (accessed on 16 June 2023).
- Victora, C.G.; de Onis, M.; Hallal, P.C.; Blössner, M.; Shrimpton, R. Worldwide timing of growth faltering: Revisiting implications for interventions. Pediatrics 2010, 125, 473–480. [Google Scholar] [CrossRef]
- Popkin, B.M.; Adair, L.S.; Ng, S.W. Global nutrition transition and the pandemic of obesity in developing countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [PubMed]
- Pries, A.M.; Rehman, A.M.; Filteau, S.; Sharma, N.; Upadhyay, A.; Ferguson, E.L. Unhealthy Snack Food and Beverage Consumption Is Associated with Lower Dietary Adequacy and Length-for-Age z-Scores among 12-23-Month-Olds in Kathmandu Valley, Nepal. J. Nutr. 2019, 149, 1843–1851. [Google Scholar] [CrossRef] [PubMed]
- Zahid, N.; Khadka, N.; Ganguly, M.; Varimezova, T.; Turton, B.; Spero, L.; Sokal-Gutierrez, K. Associations between Child Snack and Beverage Consumption, Severe Dental Caries, and Malnutrition in Nepal. Int. J. Environ. Res. Public Health 2020, 17, 7911. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Giovannucci, E.L. Ultra-processed foods and health: A comprehensive review. Crit. Rev. Food Sci. Nutr. 2022, 63, 10836–10848. [Google Scholar] [CrossRef] [PubMed]
- Petridi, E.; Karatzi, K.; Magriplis, E.; Charidemou, E.; Philippou, E.; Zampelas, A. The impact of ultra-processed foods on obesity and cardiometabolic comorbidities in children and adolescents: A systematic review. Nutr. Rev. 2023, 7, nuad095. [Google Scholar] [CrossRef] [PubMed]
- Veit, M.; van Asten, R.; Olie, A.; Prinz, P. The role of dietary sugars, overweight, and obesity in type 2 diabetes mellitus: A narrative review. Eur. J. Clin. Nutr. 2022, 76, 1497–1501. [Google Scholar] [CrossRef] [PubMed]
- Lobstein, T.; Brinsden, H.; Neveux, M. World Obesity Atlas 2022. Available online: https://www.worldobesityday.org/assets/downloads/World_Obesity_Atlas_2022_WEB.pdf (accessed on 9 July 2023).
- Popkin, B.M. The nutrition transition and obesity in the developing world. J. Nutr. 2001, 131, 871–873. [Google Scholar] [CrossRef]
- Pries, A.M.; Huffman, S.L.; Champeny, M.; Adhikary, I.; Benjamin, M.; Coly, A.N.; Diop, E.H.I.; Mengkheang, K.; Sy, N.Y.; Dhungel, S.; et al. Consumption of commercially produced snack foods and sugar-sweetened beverages during the complementary feeding period in four African and Asian urban contexts. Matern. Child Nutr. 2017, 13 (Suppl. S2), e12412. [Google Scholar] [CrossRef]
- Popkin, B.M.; Corvalan, C.; Grummer-Strawn, L.M. Dynamics of the double burden of malnutrition and the changing nutrition reality. Lancet 2020, 395, 65–74. [Google Scholar] [CrossRef]
- Windus, J.L.; Burrows, T.L.; Duncanson, K.; Collins, C.E.; Rollo, M.E. Scoping review of nutrition intervention and dietary assessment studies in Khmer populations living in Cambodia. J. Hum. Nutr. Diet. 2021, 34, 953–968. [Google Scholar] [CrossRef] [PubMed]
- Turton, B.; Durward, C.; Crombie, F.; Sokal-Gutierrez, K.; Soeurn, S.; Manton, D.J. Evaluation of a community-based early childhood caries (ECC) intervention in Cambodia. Community Dent. Oral Epidemiol. 2021, 49, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Turton, B.; Durward, C.; Manton, D.; Bach, K.; Yos, C. Socio-behavioural risk factors for early childhood caries (ECC) in Cambodian preschool children: A pilot study. Eur. Arch. Paediatr. Dent. 2016, 17, 97–105. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development. Available online: https://www.who.int/publications/i/item/924154693X (accessed on 24 July 2023).
- The World Bank. GDP per Capita (Constant 2015 US$)-Cambodia. Available online: https://data.worldbank.org/indicator/NY.GDP.PCAP.KD?locations=KH (accessed on 10 November 2023).
- Athavale, P.; Khadka, N.; Roy, S.; Mukherjee, P.; Chandra Mohan, D.; Turton, B.B.; Sokal-Gutierrez, K. Early Childhood Junk Food Consumption, Severe Dental Caries, and Undernutrition: A Mixed-Methods Study from Mumbai, India. Int. J. Environ. Res. Public Health 2020, 17, 8629. [Google Scholar] [CrossRef] [PubMed]
- Huffman, S.L.; Piwoz, E.G.; Vosti, S.A.; Dewey, K.G. Babies, soft drinks and snacks: A concern in low- and middle-income countries? Matern. Child Nutr. 2014, 10, 562–574. [Google Scholar] [CrossRef]
- Pries, A.M.; Huffman, S.L.; Mengkheang, K.; Kroeun, H.; Champeny, M.; Roberts, M.; Zehner, E. High use of commercial food products among infants and young children and promotions for these products in Cambodia. Matern. Child Nutr. 2016, 12, 52–63. [Google Scholar] [CrossRef]
- Pries, A.M.; Filteau, S.; Ferguson, E.L. Snack food and beverage consumption and young child nutrition in low- and middle-income countries: A systematic review. Matern. Child Nutr. 2019, 15 (Suppl. S4), e12729. [Google Scholar] [CrossRef]
- Hinnouho, G.M.; Ferguson, E.L.; MacDougall, A.; Kroeun, H.; Sophonneary, P.; Chea, M.; Pries, A.M. High consumption of unhealthy commercial foods and beverages tracks across the complementary feeding period in rural/peri-urban Cambodia. Matern. Child Nutr. 2023, 19, e13485. [Google Scholar] [CrossRef]
- Pan American Health Organization. Guiding Principles for Complementary Feeding of the Breastfed Child. Available online: https://www.who.int/publications/i/item/9275124604 (accessed on 16 June 2023).
- Contreras, M.; Zelaya Blandón, E.; Persson, L.Å.; Ekström, E.C. Consumption of highly processed snacks, sugar-sweetened beverages and child feeding practices in a rural area of Nicaragua. Matern. Child Nutr. 2016, 12, 164–176. [Google Scholar] [CrossRef]
- Mennella, J.A. Ontogeny of taste preferences: Basic biology and implications for health. Am. J. Clin. Nutr. 2014, 99, 704S–711S. [Google Scholar] [CrossRef]
- Puspikawati, S.I.; Dewi, D.M.S.K.; Astutik, E.; Kusuma, D.; Melaniani, S.; Sebayang, S.K. Density of outdoor food and beverage advertising around gathering place for children and adolescent in East Java, Indonesia. Public Health Nutr. 2021, 24, 1066–1078. [Google Scholar] [CrossRef] [PubMed]
- Mazarello Paes, V.; Hesketh, K.; O’Malley, C.; Moore, H.; Summerbell, C.; Griffin, S.; van Sluijs, E.M.; Ong, K.K.; Lakshman, R. Determinants of sugar-sweetened beverage consumption in young children: A systematic review. Obes. Rev. 2015, 16, 903–913. [Google Scholar] [CrossRef] [PubMed]
- De Cosmi, V.; Scaglioni, S.; Agostoni, C. Early Taste Experiences and Later Food Choices. Nutrients 2017, 9, 107. [Google Scholar] [CrossRef]
- Sharma, N.; Ferguson, E.L.; Upadhyay, A.; Zehner, E.; Filteau, S.; Pries, A.M. Perceptions of commercial snack food and beverages for infant and young child feeding: A mixed-methods study among caregivers in Kathmandu Valley, Nepal. Matern. Child Nutr. 2019, 15 (Suppl. S4), e12711. [Google Scholar] [CrossRef]
- Ruottinen, S.; Niinikoski, H.; Lagström, H.; Rönnemaa, T.; Hakanen, M.; Viikari, J.; Jokinen, E.; Simell, O. High sucrose intake is associated with poor quality of diet and growth between 13 months and 9 years of age: The special Turku Coronary Risk Factor Intervention Project. Pediatrics 2008, 121, 1676–1685. [Google Scholar] [CrossRef] [PubMed]
- Marrón-Ponce, J.A.; Sánchez-Pimienta, T.G.; Rodríguez-Ramírez, S.; Batis, C.; Cediel, G. Ultra-processed foods consumption reduces dietary diversity and micronutrient intake in the Mexican population. J. Hum. Nutr. Diet. 2023, 36, 241–251. [Google Scholar] [CrossRef]
- Motbainor, A.; Worku, A.; Kumie, A. Stunting Is Associated with Food Diversity while Wasting with Food Insecurity among Underfive Children in East and West Gojjam Zones of Amhara Region, Ethiopia. PLoS ONE 2015, 10, e0133542. [Google Scholar] [CrossRef]
- Molani Gol, R.; Kheirouri, S.; Alizadeh, M. Association of Dietary Diversity With Growth Outcomes in Infants and Children Aged Under 5 Years: A Systematic Review. J. Nutr. Educ. Behav. 2022, 54, 65–83. [Google Scholar] [CrossRef]
- Darapheak, C.; Takano, T.; Kizuki, M.; Nakamura, K.; Seino, K. Consumption of animal source foods and dietary diversity reduce stunting in children in Cambodia. Int. Arch. Med. 2013, 6, 29. [Google Scholar] [CrossRef]
- Sié, A.; Tapsoba, C.; Dah, C.; Ouermi, L.; Zabre, P.; Bärnighausen, T.; Arzika, A.M.; Lebas, E.; Snyder, B.M.; Moe, C.; et al. Dietary diversity and nutritional status among children in rural Burkina Faso. Int. Health 2018, 10, 157–162. [Google Scholar] [CrossRef]
- Valenzuela, M.J.; Waterhouse, B.; Aggarwal, V.R.; Bloor, K.; Doran, T. Effect of sugar-sweetened beverages on oral health: A systematic review and meta-analysis. Eur. J. Public Health 2021, 31, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Dimaisip-Nabuab, J.; Duijster, D.; Benzian, H.; Heinrich-Weltzien, R.; Homsavath, A.; Monse, B.; Sithan, H.; Stauf, N.; Susilawati, S.; Kromeyer-Hauschild, K. Nutritional status, dental caries and tooth eruption in children: A longitudinal study in Cambodia, Indonesia and Lao PDR. BMC Pediatr. 2018, 18, 300. [Google Scholar] [CrossRef]
- Renggli, E.P.; Turton, B.; Sokal-Gutierrez, K.; Hondru, G.; Chher, T.; Hak, S.; Poirot, E.; Laillou, A. Stunting Malnutrition Associated with Severe Tooth Decay in Cambodian Toddlers. Nutrients 2021, 13, 290. [Google Scholar] [CrossRef]
- Turton, B.; Chher, T.; Hak, S.; Sokal-Gutierrez, K.; Lopez Peralta, D.; Laillou, A.; Singh, A. Associations between dental caries and ponderal growth in children: A Cambodian study. J. Glob. Health 2022, 12, 04046. [Google Scholar] [CrossRef]
- Turton, B.; Sullivan, S.; Chher, T.; Hak, S.; Sokal-Gutierrez, K.; Wieringa, F.; Singh, A. Caries Incidence Is Associated with Wasting among Cambodian Children. J. Dent. Res. 2023, 102, 157–163. [Google Scholar] [CrossRef]
- Alkarimi, H.A.; Watt, R.G.; Pikhart, H.; Sheiham, A.; Tsakos, G. Dental caries and growth in school-age children. Pediatrics 2014, 133, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Lui, D.T.; Wahab, R.M.A.; Kuppusamy, E.; Hamzaid, N.H.; Hassan, M.R.; Yazid, F. Association of early childhood caries and nutritional status: A scoping review. J. Clin. Pediatr. Dent. 2023, 47, 11–25. [Google Scholar] [CrossRef]
- Da Silveira, A.C.; Leite, Á.J.M.; Cabral, P.C.; de Oliveira, A.C.; de Oliveira, K.A.; de Lira, P.I.C. Toxic stress, health and nutrition among Brazilian children in shelters. BMC Pediatr. 2021, 21, 112. [Google Scholar] [CrossRef] [PubMed]
- Rachmi, C.N.; Agho, K.E.; Li, M.; Baur, L.A. Stunting coexisting with overweight in 2·0–4·9-year-old Indonesian children: Prevalence, trends and associated risk factors from repeated cross-sectional surveys. Public Health Nutr. 2016, 19, 2698–2707. [Google Scholar] [CrossRef]
- Greffeuille, V.; Sophonneary, P.; Laillou, A.; Gauthier, L.; Hong, R.; Hong, R.; Poirot, E.; Dijkhuizen, M.; Wieringa, F.; Berger, J. Persistent Inequalities in Child Undernutrition in Cambodia from 2000 until Today. Nutrients 2016, 8, 297. [Google Scholar] [CrossRef]
- World Health Organization. The Double Burden of Malnutrition: Policy Brief. Available online: https://www.who.int/publications/i/item/WHO-NMH-NHD-17.3 (accessed on 24 July 2023).
- Horiuchi, Y.; Kusama, K.; Kanha, S.; Yoshiike, N.; FIDR research team. Urban-Rural Differences in Nutritional Status and Dietary Intakes of School-Aged Children in Cambodia. Nutrients 2018, 11, 14. [Google Scholar] [CrossRef]
- Biswas, T.; Townsend, N.; Magalhaes, R.J.S.; Hasan, M.; Mamun, A. Patterns and determinants of the double burden of malnutrition at the household level in South and Southeast Asia. Eur. J. Clin. Nutr. 2021, 75, 385–391. [Google Scholar] [CrossRef]
- Jimenez-Cruz, A.; Bacardi-Gascon, M.; Pichardo-Osuna, A.; Mandujano-Trujillo, Z.; Castillo-Ruiz, O. Infant and toddlers’ feeding practices and obesity amongst low-income families in Mexico. Asia Pac. J. Clin. Nutr. 2010, 19, 316–323. [Google Scholar] [PubMed]
- Saravia, L.; González-Zapata, L.I.; Rendo-Urteaga, T.; Ramos, J.; Collese, T.S.; Bove, I.; Delgado, C.; Tello, F.; Iglesia, I.; Gonçalves Sousa, E.D.; et al. Development of a Food Frequency Questionnaire for Assessing Dietary Intake in Children and Adolescents in South America. Obesity 2018, 26 (Suppl. S1), S31–S40. [Google Scholar] [CrossRef] [PubMed]
- Sotos-Prieto, M.; Moreno-Franco, B.; Ordovás, J.M.; León, M.; Casasnovas, J.A.; Peñalvo, J.L. Design and development of an instrument to measure overall lifestyle habits for epidemiological research: The Mediterranean Lifestyle (MEDLIFE) index. Public Health Nutr. 2015, 18, 959–967. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mean ± SD or N (%), n = 377 |
|---|---|
| Child | |
| Sex | |
| Male | 169 (44.8) |
| Female | 208 (55.2) |
| Age (months) | 22.7 ± 2.9 |
| Household Characteristics | |
| Monthly income (USD †) | |
| Less than $50 | 29 (8.1) |
| $51–150 | 87 (24.2) |
| $151–250 | 130 (36.2) |
| More than $250 | 113 (31.5) |
| Electricity | 320 (84.7) |
| Running water | 103 (27.3) |
| Number of people in household | 5.0 ± 1.7 |
| Cooking fuel source | |
| Wood | 241 (63.9) |
| Charcoal | 16 (4.2) |
| Gas | 50 (13.3) |
| Combination | 70 (18.6) |
| Location | |
| Rural | 167 (45.0) |
| Semi-urban | 204 (55.0) |
| Parent Characteristics | |
| Mother’s age (years) | 28.1 ± 5.5 |
| Father’s age (years) | 30.1 ± 5.9 |
| Parent education | |
| Unable to read | 49 (13.1) |
| Primary school | 173 (46.3) |
| High school | 141 (37.7) |
| University | 11 (2.9) |
| Mother’s occupation | |
| Stay-at-home | 98 (26.0) |
| Seller | 19 (5.0) |
| Farmer | 22 (5.8) |
| Government worker | 3 (0.8) |
| Other | 235 (62.3) |
| Father’s occupation | |
| Stay-at-home | 34 (9.1) |
| Seller | 19 (5.1) |
| Farmer | 39 (10.4) |
| Government worker | 12 (3.2) |
| Other | 271 (72.3) |
| Nutritional Status of Child | |
| Stunted (LAZ ‡/HAZ ‡ < −2 SD below median) | 156 (43.1) |
| Wasted (WAZ ‡ < −2 SD below median) | 58 (15.7) |
| Exposure Variable | OR | [95% CI] | p-Value |
|---|---|---|---|
| Any flavored sugary drinks ‡ | 2.02 | [1.18–3.43] | 0.01 |
| Any FLNV ‡ | 0.89 | [0.51–1.55] | 0.69 |
| Number of FLNV on previous day | |||
| One | 1.01 | [0.54–1.91] | 0.96 |
| Two | 0.94 | [0.47–1.86] | 0.86 |
| Three or more | 0.68 | [0.34–1.34] | 0.27 |
| Any packaged salty snacks | 0.69 | [0.43–1.09] | 0.11 |
| Number of packaged salty snacks on previous day | |||
| One | 0.74 | [0.44–1.23] | 0.24 |
| Two or more | 0.58 | [0.31–1.11] | 0.10 |
| Any packaged sweets | 1.03 | [0.63–1.68] | 0.91 |
| Number of packaged sweets on previous day | |||
| One | 1.24 | [0.67–2.32] | 0.49 |
| Two or more | 0.82 | [0.42–1.61] | 0.57 |
| Exposure Variable | OR | [95% CI] | p-Value |
|---|---|---|---|
| Any flavored sugary drinks ‡ | 2.21 | [1.20–4.08] | 0.01 |
| Any FLNV ‡ | 1.79 | [0.84–3.79] | 0.13 |
| Number of FLNV on previous day | |||
| One | 1.81 | [0.78–4.20] | 0.17 |
| Two | 2.64 | [1.10–6.33] | 0.03 |
| Three or more | 1.12 | [0.43–2.91] | 0.82 |
| Any packaged salty snacks | 1.34 | [0.73–2.44] | 0.34 |
| Number of packaged salty snacks on previous day | |||
| One | 1.48 | [0.78–2.82] | 0.23 |
| Two or more | 1.06 | [0.46–2.43] | 0.89 |
| Any packaged sweets | 1.25 | [0.68–2.30] | 0.469 |
| Number of packaged sweets on previous day | |||
| One | 2.22 | [1.11–4.44] | 0.02 |
| Two or more | 0.46 | [0.15–1.35] | 0.16 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brown, A.; Trimble, M.; Sokal-Gutierrez, K.; Fernald, L.; Madsen, K.; Turton, B. Sugar-Sweetened Beverages, Foods of Low Nutritional Value, and Child Undernutrition in Cambodia. Int. J. Environ. Res. Public Health 2024, 21, 169. https://doi.org/10.3390/ijerph21020169
Brown A, Trimble M, Sokal-Gutierrez K, Fernald L, Madsen K, Turton B. Sugar-Sweetened Beverages, Foods of Low Nutritional Value, and Child Undernutrition in Cambodia. International Journal of Environmental Research and Public Health. 2024; 21(2):169. https://doi.org/10.3390/ijerph21020169
Chicago/Turabian StyleBrown, Akemi, Margaret Trimble, Karen Sokal-Gutierrez, Lia Fernald, Kristine Madsen, and Bathsheba Turton. 2024. "Sugar-Sweetened Beverages, Foods of Low Nutritional Value, and Child Undernutrition in Cambodia" International Journal of Environmental Research and Public Health 21, no. 2: 169. https://doi.org/10.3390/ijerph21020169
APA StyleBrown, A., Trimble, M., Sokal-Gutierrez, K., Fernald, L., Madsen, K., & Turton, B. (2024). Sugar-Sweetened Beverages, Foods of Low Nutritional Value, and Child Undernutrition in Cambodia. International Journal of Environmental Research and Public Health, 21(2), 169. https://doi.org/10.3390/ijerph21020169