
Predictors of Free Sugars Intake Trajectories across Early Childhood—Results from the SMILE Birth Cohort Study

 , ,
, ,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Key Measures
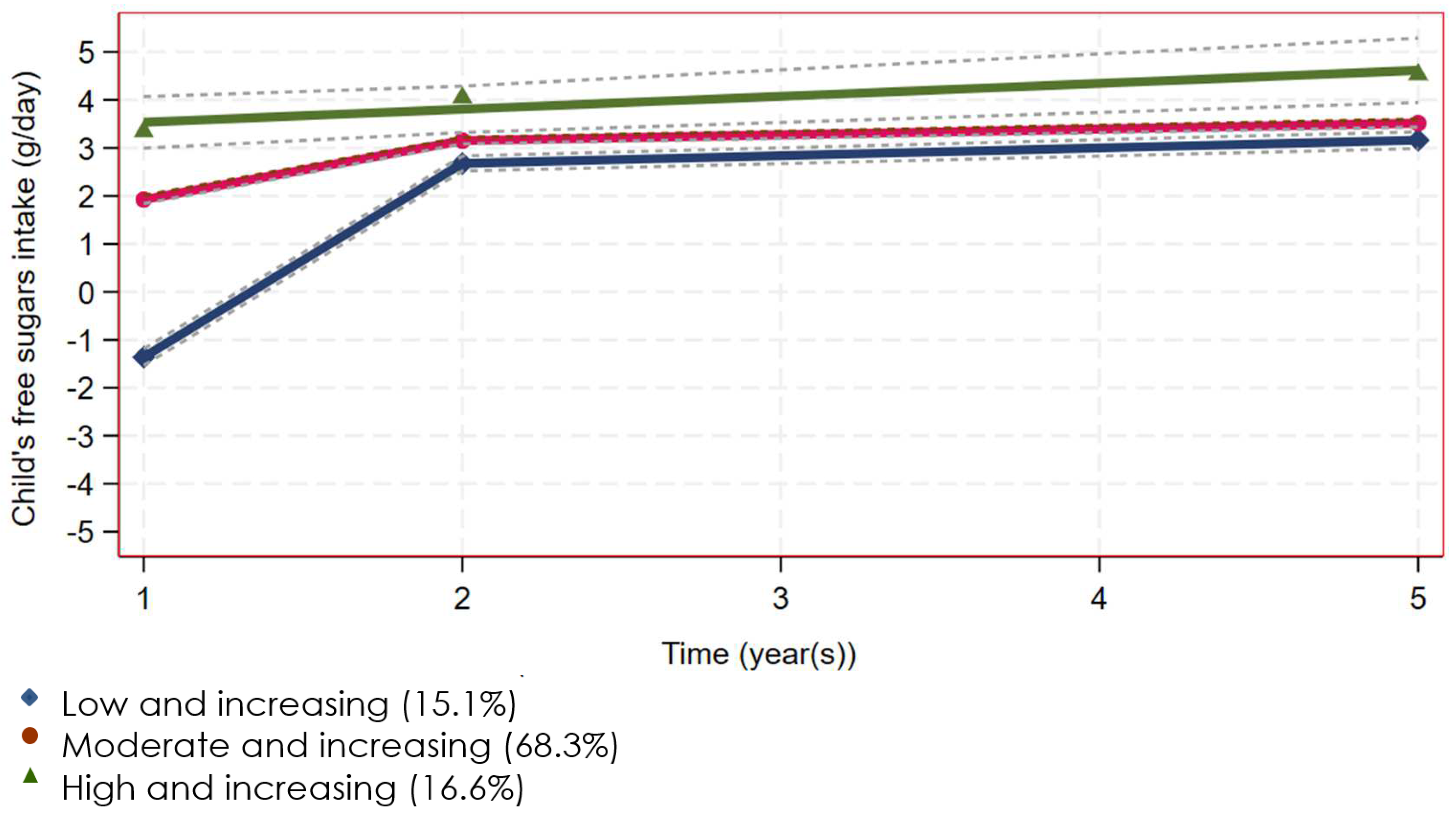
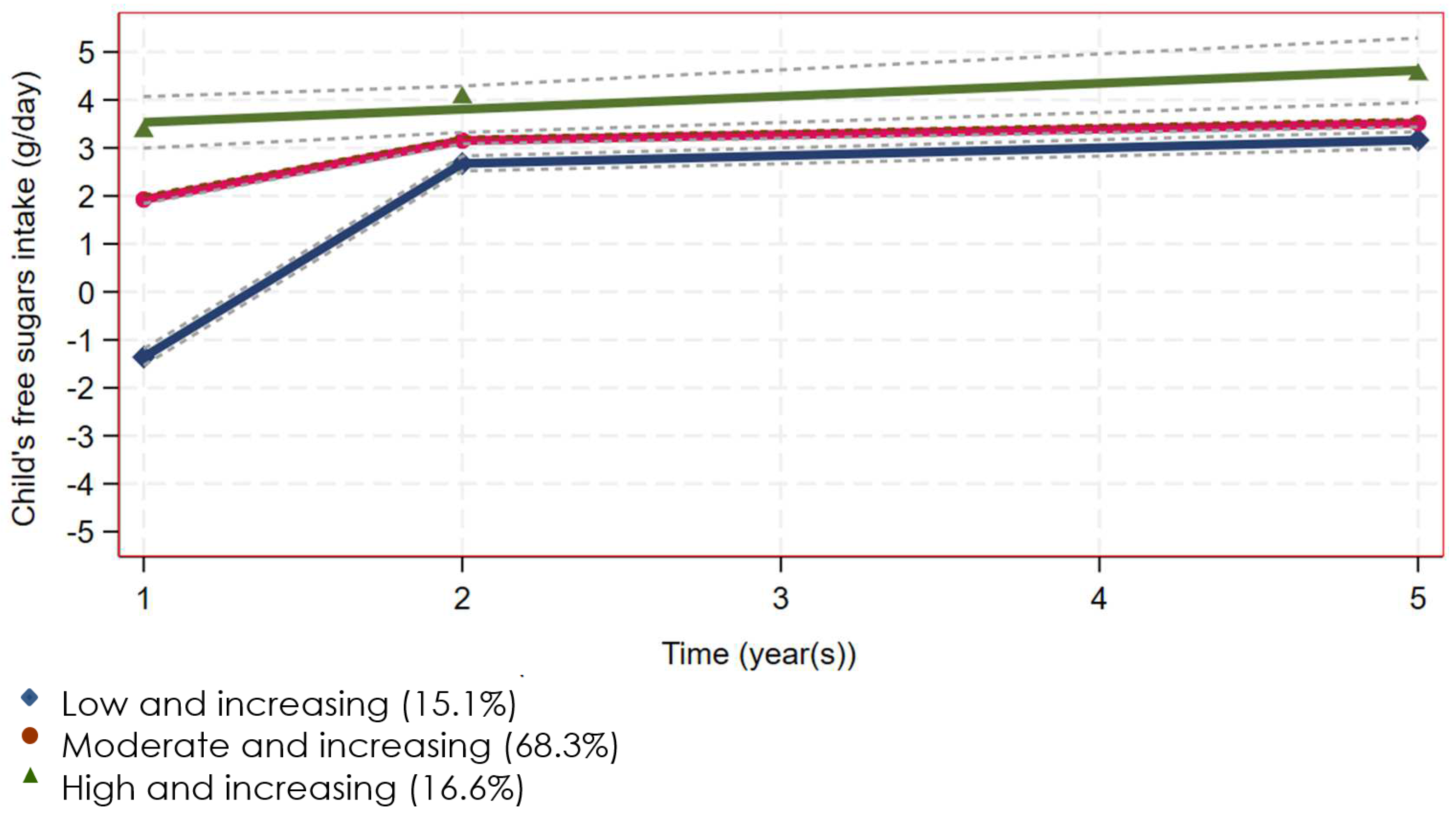
2.2.1. Outcome Variable—Trajectories of Children’s Free Sugars Intake
2.2.2. Explanatory Variables
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schwarzenberg, S.J.; Georgieff, M.K. Advocacy for Improving Nutrition in the First 1000 Days to Support Childhood Development and Adult Health. Pediatrics 2018, 141, e20173716. [Google Scholar] [CrossRef]
- Nicklaus, S.; Schwartz, C. Early influencing factors on the development of sensory and food preferences. Curr. Opin. Clin. Nutr. Metab. Care 2019, 22, 230–235. [Google Scholar] [CrossRef]
- Appleton, K.M.; Tuorila, H.; Bertenshaw, E.J.; de Graaf, C.; Mela, D.J. Sweet taste exposure and the subsequent acceptance and preference for sweet taste in the diet: Systematic review of the published literature. Am. J. Clin. Nutr. 2018, 107, 405–419. [Google Scholar] [CrossRef] [PubMed]
- Johnson, B.J.; Bell, L.K.; Zarnowiecki, D.; Rangan, A.M.; Golley, R.K. Contribution of discretionary foods and drinks to Australian children’s intake of energy, saturated fat, added sugars and salt. Children 2017, 4, 104. [Google Scholar] [CrossRef]
- Hauner, H.; Bechthold, A.; Boeing, H.; Bronstrup, A.; Buyken, A.; Leschik-Bonnet, E.; Linseisen, J.; Schulze, M.; Strohm, D.; Wolfram, G.; et al. Evidence-based guideline of the German Nutrition Society: Carbohydrate intake and prevention of nutrition-related diseases. Ann. Nutr. Metab 2012, 60 (Suppl. 1), 1–58. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Hu, F.B. The role of sugar-sweetened beverages in the global epidemics of obesity and chronic diseases. Nat. Rev. Endocrinol. 2022, 18, 205–218. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Carbohydrate Intake for Adults and Children: WHO Guideline; World Health Organization: Geneva, Switzerland, 2023. [Google Scholar]
- Moynihan, P.J.; Kelly, S.A. Effect on caries of restricting sugars intake: Systematic review to inform WHO guidelines. J. Dent. Res. 2014, 93, 8–18. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guideline: Sugars Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Louie, J.C.; Moshtaghian, H.; Rangan, A.M.; Flood, V.M.; Gill, T.P. Intake and sources of added sugars among Australian children and adolescents. Eur. J. Nutr. 2016, 55, 2347–2355. [Google Scholar] [CrossRef] [PubMed]
- Devenish, G.; Golley, R.; Mukhtar, A.; Begley, A.; Ha, D.; Do, L.; Scott, J.A. Free sugars intake, sources and determinants of high consumption among Australian 2-year-olds in the SMILE cohort. Nutrients 2019, 11, 161. [Google Scholar] [CrossRef] [PubMed]
- Devenish, G.; Ytterstad, E.; Begley, A.; Do, L.; Scott, J. Intake, sources, and determinants of free sugars intake in Australian children aged 12-14 months. Matern. Child. Nutr. 2019, 15, e12692. [Google Scholar] [CrossRef]
- Nguyen, H.V.; Ha, D.H.; Dao, A.T.M.; Golley, R.K.; Scott, J.A.; Spencer, J.; Bell, L.; Devenish-Coleman, G.; Do, L.G. Pairwise approach for analysis and reporting of child’s free sugars intake from a birth cohort study. Community Dent. Oral. Epidemiol. 2023, 51, 820–828. [Google Scholar] [CrossRef]
- Nagin, D.S.; Jones, B.L.; Passos, V.L.; Tremblay, R.E. Group-based multi-trajectory modeling. Stat. Methods Med. Res. 2018, 27, 2015–2023. [Google Scholar] [CrossRef]
- Nguena Nguefack, H.; Pagé, M.; Katz, J.; Choinière, M.; Vanasse, A.; Dorais, M.; Samb, O.; Lacasse, A. Trajectory modelling techniques useful to epidemiological research: A comparative narrative review of approaches. Clin. Epidemiol. 2020, 12, 1205–1222. [Google Scholar] [CrossRef]
- Manohar, N.; Hayen, A.; Do, L.; Scott, J.; Bhole, S.; Arora, A. Early life and socio-economic determinants of dietary trajectories in infancy and early childhood—Results from the HSHK birth cohort study. Nutr. J. 2021, 20, 76. [Google Scholar] [CrossRef]
- Ha, D.H.; Nguyen, H.V.; Bell, L.K.; Devenish-Coleman, G.; Golley, R.K.; Thomson, W.M.; Manton, D.J.; Leary, S.D.; Scott, J.A.; Spencer, J.; et al. Trajectories of child free sugars intake and dental caries—A population-based birth cohort study. J. Dent. 2023, 134, 104559. [Google Scholar] [CrossRef]
- Dalrymple, K.V.; Vogel, C.; Godfrey, K.M.; Baird, J.; Harvey, N.C.; Hanson, M.A.; Cooper, C.; Inskip, H.M.; Crozier, S.R. Longitudinal dietary trajectories from preconception to mid-childhood in women and children in the Southampton Women’s Survey and their relation to offspring adiposity: A group-based trajectory modelling approach. Int. J. Obes. 2022, 46, 758–766. [Google Scholar] [CrossRef] [PubMed]
- Cosier, D.; Charlton, K.; Schoenaker, D. The association between dietary trajectories across childhood and blood pressure in early adolescence: The Longitudinal Study of Australian Children. Eur. J. Clin. Nutr. 2023, 77, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Echeverria, M.S.; Schuch, H.S.; Cenci, M.S.; Motta, J.V.S.; Bertoldi, A.D.; Hallal, P.C.; Demarco, F.F. Trajectories of sugar consumption and dental caries in early childhood. J. Dent. Res. 2022, 101, 724–730. [Google Scholar] [CrossRef] [PubMed]
- Peres, M.A.; Sheiham, A.; Liu, P.; Demarco, F.F.; Silva, A.E.; Assunção, M.C.; Menezes, A.M.; Barros, F.C.; Peres, K.G. Sugar consumption and changes in dental caries from childhood to adolescence. J. Dent. Res. 2016, 95, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Do, L.; Scott, J.; Thomson, W.; Stamm, J.; Rugg-Gunn, A.; Levy, S.; Wong, C.; Devenish, G.; Ha, D.; Spencer, A. Common risk factor approach to address socioeconomic inequality in the oral health of preschool children—A prospective cohort study. BMC Public Health 2014, 14, 429. [Google Scholar] [CrossRef] [PubMed]
- Food Standards Australia and New Zealand. USNUT 2011-2013. Australian Food, Supplement and Nutrient Database. Available online: http://www.foodstandards.gov.au/science/monitoringnutrients/ausnut/pages/default.aspx (accessed on 18 December 2019).
- Devenish, G.; Mukhtar, A.; Begley, A.; Do, L.; Scott, J. Development and Relative Validity of a Food Frequency Questionnaire to Assess Intakes of Total and Free Sugars in Australian Toddlers. Int. J. Environ. Res. Public Health 2017, 14, 1361. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; White, I.R.; Carlin, J.B.; Spratt, M.; Royston, P.; Kenward, M.G.; Wood, A.M.; Carpenter, J.R. Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. BMJ 2009, 338, b2393. [Google Scholar] [CrossRef]
- Bell, L.K.; Golley, R.K.; Daniels, L.; Magarey, A.M. Dietary patterns of Australian children aged 14 and 24 months, and associations with socio-demographic factors and adiposity. Eur. J. Clin. Nutr. 2013, 67, 638–645. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Socio-Economic Indexes for Areas. Available online: http://www.abs.gov.au/websitedbs/censushome.nsf/home/seifa (accessed on 16 December 2019).
- Friel, S.; Hattersley, L.; Ford, L. Evidence Review: Addressing the Social Determinants of Inequities in Healthy Eating; Victorian Health Promotion Foundation: Melbourne, VC, USA, 2015. [Google Scholar]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef]
- Spence, A.C.; Campbell, K.J.; Lioret, S.; McNaughton, S.A. Early childhood vegetable, fruit, and discretionary food intakes do not meet dietary guidelines, but do show socioeconomic differences and tracking over time. J. Acad. Nutr. Diet. 2018, 118, 1634–1643.e1631. [Google Scholar] [CrossRef]
- Cameron, A.J.; Ball, K.; Pearson, N.; Lioret, S.; Crawford, D.A.; Campbell, K.; Hesketh, K.; McNaughton, S.A. Socioeconomic variation in diet and activity-related behaviours of Australian children and adolescents aged 2-16 years. Pediatr. Obes. 2012, 7, 329–342. [Google Scholar] [CrossRef]
- Darmon, N.; Drewnowski, A. Contribution of food prices and diet cost to socioeconomic disparities in diet quality and health: A systematic review and analysis. Nutr. Rev. 2015, 73, 643–660. [Google Scholar] [CrossRef]
- Pryer, J.A.; Rogers, S. Dietary patterns among a national sample of British children aged 1½ − 4½; years. Public Health Nutr. 2009, 12, 957–966. [Google Scholar] [CrossRef] [PubMed]
- Lioret, S.; Betoko, A.; Forhan, A.; Charles, M.A.; Heude, B.; de Lauzon-Guillain, B.; Eden Mother-Child Cohort Study Group. Dietary patterns track from infancy to preschool age: Cross-sectional and longitudinal perspectives. J. Nutr. 2015, 145, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Dubois, L.; Farmer, A.; Girard, M.; Burnier, D.; Porcherie, M. Demographic and socio-economic factors related to food intake and adherence to nutritional recommendations in a cohort of pre-school children. Public Health Nutr. 2011, 14, 1096–1104. [Google Scholar] [CrossRef] [PubMed]
- Innes-Hughes, C.; Hardy, L.L.; Venugopal, K.; King, L.A.; Wolfenden, L.; Rangan, A. Children’s consumption of energy-dense nutrient-poor foods, fruit and vegetables: Are they related? An analysis of data from a cross sectional survey. Health Promot. J. Austr. 2011, 22, 210–216. [Google Scholar] [CrossRef]
- Jones, L.R.; Steer, C.D.; Rogers, I.S.; Emmett, P.M. Influences on child fruit and vegetable intake: Sociodemographic, parental and child factors in a longitudinal cohort study. Public Health Nutr. 2010, 13, 1122–1130. [Google Scholar] [CrossRef]
- Fayet-Moore, F.; McConnell, A.; Tuck, K.; Petocz, P.; Cassettari, T.; Rahimi-Ardabili, H.; Blumfield, M.; Marshall, S. Patterns of discretionary food intake among Australian children and their association with socio-demographic, lifestyle, and adiposity measures. Nutr. Diet. 2022, 79, 623–635. [Google Scholar] [CrossRef]
- McPhail, D.; Beagan, B.; Chapman, G.E. “I Don’t Want to be Sexist But…”. Food Cult. Soc. 2012, 15, 473–489. [Google Scholar] [CrossRef]
- Damiano, S.R.; Paxton, S.J.; Wertheim, E.H.; McLean, S.A.; Gregg, K.J. Dietary restraint of 5-year-old girls: Associations with internalization of the thin ideal and maternal, media, and peer influences. Int. J. Eat. Disord. 2015, 48, 1166–1169. [Google Scholar] [CrossRef] [PubMed]
- McPhie, S.; Skouteris, H.; Daniels, L.; Jansen, E. Maternal correlates of maternal child feeding practices: A systematic review. Matern. Child Nutr. 2014, 10, 18–43. [Google Scholar] [CrossRef] [PubMed]
- North, K.; Emmett, P. Multivariate analysis of diet among three-year-old children and associations with socio-demographic characteristics. The Avon Longitudinal Study of Pregnancy and Childhood (ALSPAC) Study Team. Eur. J. Clin. Nutr. 2000, 54, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Vilela, S.; Oliveira, A.; Pinto, E.; Moreira, P.; Barros, H.; Lopes, C. The influence of socioeconomic factors and family context on energy-dense food consumption among 2-year-old children. Eur. J. Clin. Nutr. 2015, 69, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Public Health Association of Australia. Marketing of Food and Beverages to Children: Background Paper; Public Health Association of Australia: Canberra, Australia, 2018. [Google Scholar]
- Thompson, F.E.; Subar, A.F. Dietary Assessment Methodology. In Nutrition in the Prevention and Treatment of Disease, 3rd ed.; Coulston, A.M., Boushey, C., Ferruzzi, M., Eds.; Academic Press: London, UK, 2013. [Google Scholar]

{kind=link}
| Trajectory 1 (n = 165) | Trajectory 2 (n = 1095) | Trajectory 3 (n = 126) | Total (n = 1386) | |
|---|---|---|---|---|
| Child age | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) |
| 1 year old | 0.31 (0.22) | 7.91 (6.22) | 30.50 (24.82) | 8.8 (12.0) |
| 2 years old | 19.66 (15.45) | 28.40 (23.09) | 80.91 (85.19) | 32.2 (37.8) |
| 5 years old | 18.27 (18.65) | 28.92 (31.99) | 87.29 (76.65) | 44.2 (45.7) |
| p-Mann-Kendall trend | <0.001 | <0.001 | <0.001 | <0.001 |
| Trajectory 2 Compared with Trajectory 1 | Trajectory 3 Compared with Trajectory 1 | |||||
|---|---|---|---|---|---|---|
| aRRR | 95% CI | p Value | aRRR | 95% CI | p Value | |
| Maternal characteristics | ||||||
| Mother’s age | 1.01 | 0.96–1.05 | 0.806 | 0.94 | 0.89–1.00 | 0.047 |
| Mother’s highest education level | ||||||
| High school (n = 191) | 1.00 | 0.54–1.84 | 0.991 | 1.51 | 0.68–3.36 | 0.315 |
| Vocational training (n = 294) | 0.78 | 0.50–1.22 | 0.278 | 0.75 | 0.38–1.48 | 0.403 |
| Tertiary education (n = 600) | REF | REF | ||||
| IRSAD decile | 0.91 | 0.85–0.98 | 0.013 | 0.84 | 0.75–0.93 | <0.001 |
| Household composition at birth | ||||||
| Single-parent household (n = 63) | 1.69 | 0.59–4.86 | 0.328 | 3.13 | 0.92–10.66 | 0.068 |
| Two-parent household (n = 1022) | REF | REF | ||||
| Child characteristics | ||||||
| Child sex | ||||||
| Male (n = 577) | REF | REF | ||||
| Female (n = 508) | 0.85 | 0.58–1.24 | 0.392 | 0.55 | 0.32–0.97 | 0.040 |
| Number of older siblings | ||||||
| None (n = 531) | REF | REF | ||||
| One (n = 384) | 1.35 | 0.88–2.08 | 0.175 | 1.36 | 0.72–2.59 | 0.346 |
| Two or more (n = 170) | 1.60 | 0.86–2.98 | 0.137 | 2.31 | 0.98–5.43 | 0.055 |
| Duration of breastfeeding (weeks) | ||||||
| <17 (n = 334) | 1.69 | 1.01–2.84 | 0.048 | 1.62 | 0.78–3.40 | 0.199 |
| 17–25 (n = 106) | 1.33 | 0.68–2.60 | 0.405 | 1.02 | 0.37–2.85 | 0.969 |
| 26–51 (n = 218) | 1.71 | 1.00–2.91 | 0.049 | 1.84 | 0.84–4.04 | 0.128 |
| ≥52 (n = 427) | REF | REF | ||||
| Age of introduction of complementary foods (weeks) | ||||||
| <17 (n = 275) | 1.32 | 0.61–2.83 | 0.480 | 1.55 | 0.54–4.46 | 0.420 |
| 17–25 (n = 707) | 0.99 | 0.53–1.88 | 0.985 | 0.71 | 0.28–1.83 | 0.481 |
| ≥26 (n = 103) | REF | REF | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bell, L.K.; Nguyen, H.V.; Ha, D.H.; Devenish-Coleman, G.; Golley, R.K.; Do, L.G.; Scott, J.A. Predictors of Free Sugars Intake Trajectories across Early Childhood—Results from the SMILE Birth Cohort Study. Int. J. Environ. Res. Public Health 2024, 21, 174. https://doi.org/10.3390/ijerph21020174
Bell LK, Nguyen HV, Ha DH, Devenish-Coleman G, Golley RK, Do LG, Scott JA. Predictors of Free Sugars Intake Trajectories across Early Childhood—Results from the SMILE Birth Cohort Study. International Journal of Environmental Research and Public Health. 2024; 21(2):174. https://doi.org/10.3390/ijerph21020174
Chicago/Turabian StyleBell, Lucinda K., Huy V. Nguyen, Diep H. Ha, Gemma Devenish-Coleman, Rebecca K. Golley, Loc G. Do, and Jane A. Scott. 2024. "Predictors of Free Sugars Intake Trajectories across Early Childhood—Results from the SMILE Birth Cohort Study" International Journal of Environmental Research and Public Health 21, no. 2: 174. https://doi.org/10.3390/ijerph21020174
APA StyleBell, L. K., Nguyen, H. V., Ha, D. H., Devenish-Coleman, G., Golley, R. K., Do, L. G., & Scott, J. A. (2024). Predictors of Free Sugars Intake Trajectories across Early Childhood—Results from the SMILE Birth Cohort Study. International Journal of Environmental Research and Public Health, 21(2), 174. https://doi.org/10.3390/ijerph21020174