
Unpacking the Public Health Triad of Social Inequality in Health, Health Literacy, and Quality of Life—A Scoping Review of Research Characteristics
 ,
,  , , , , , , , , , ,
, , , , , , , , , ,
Abstract
1. Background
- What are the characteristics of the studies that use the three concepts of social inequality in health, health literacy, and quality of life together?
- How are the three concepts presented in the research?
- Which definitions and measurements are used for the three concepts?
2. Materials and Methods
Design
- Step 1: Identifying the research question
- Step 2: Identifying the relevant studies
- Step 3: Data selection
- Step 4: Charting the data
- Step 5: Collating, summarizing, and reporting the results
- Step 6: Consultation exercise
3. Results
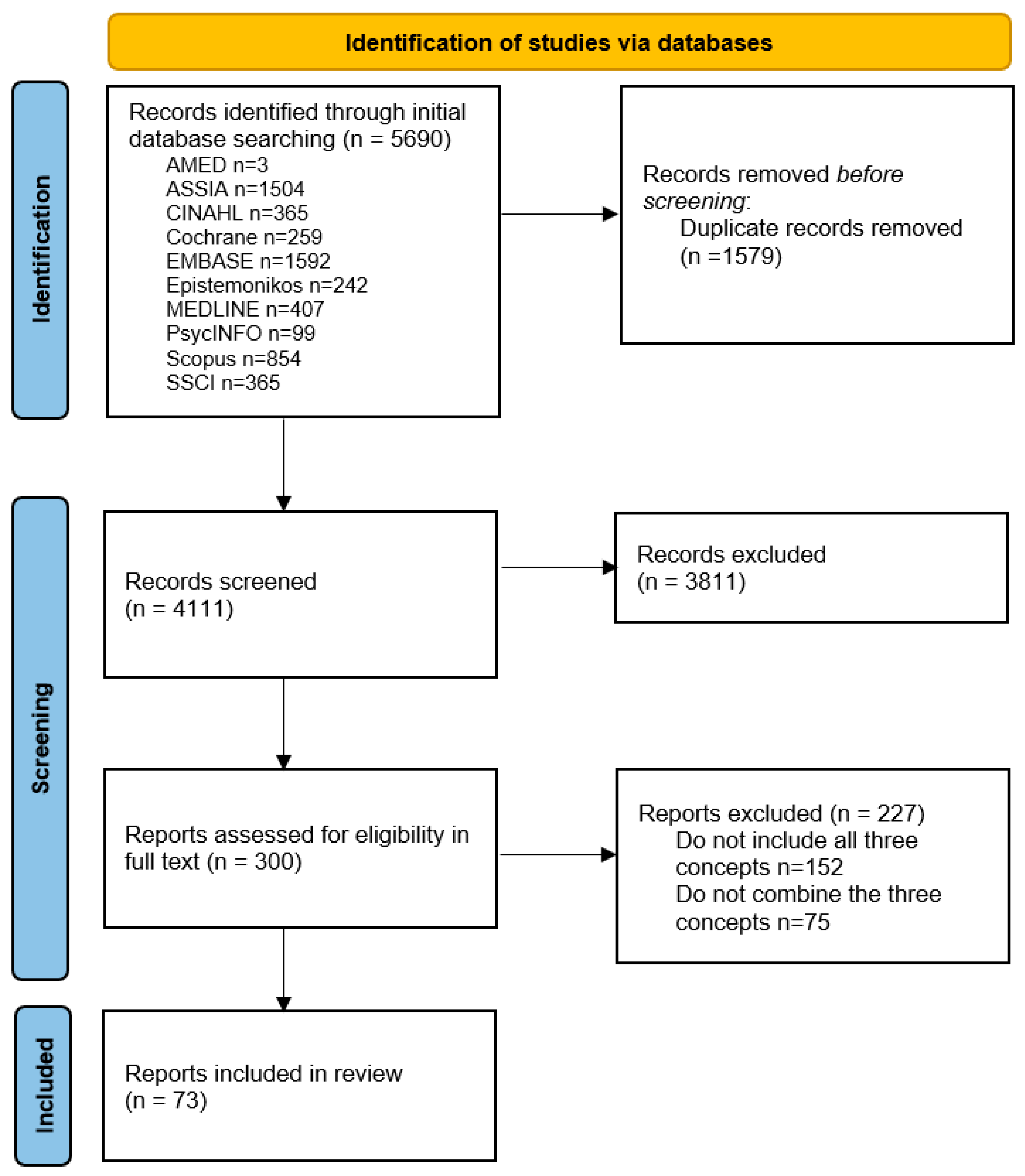
3.1. Search Results
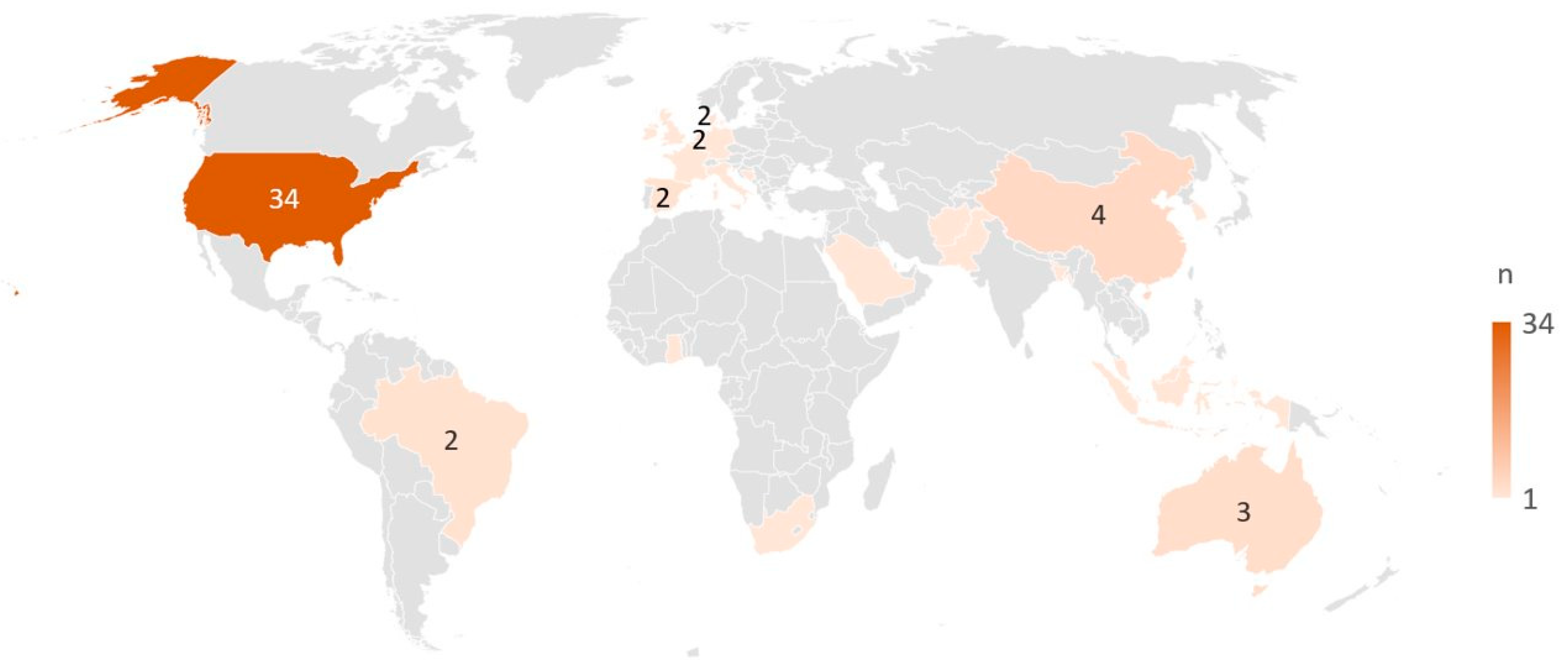
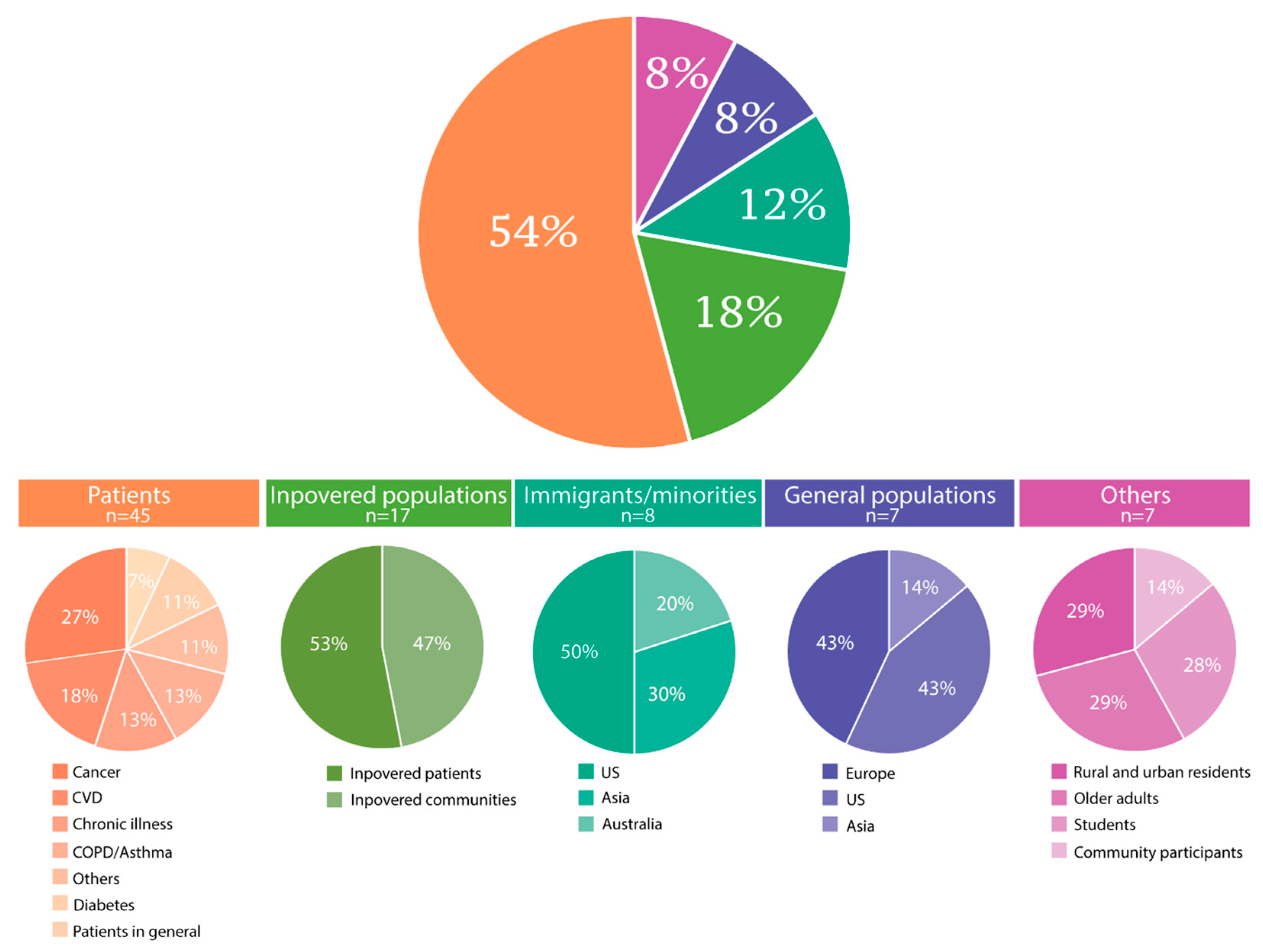
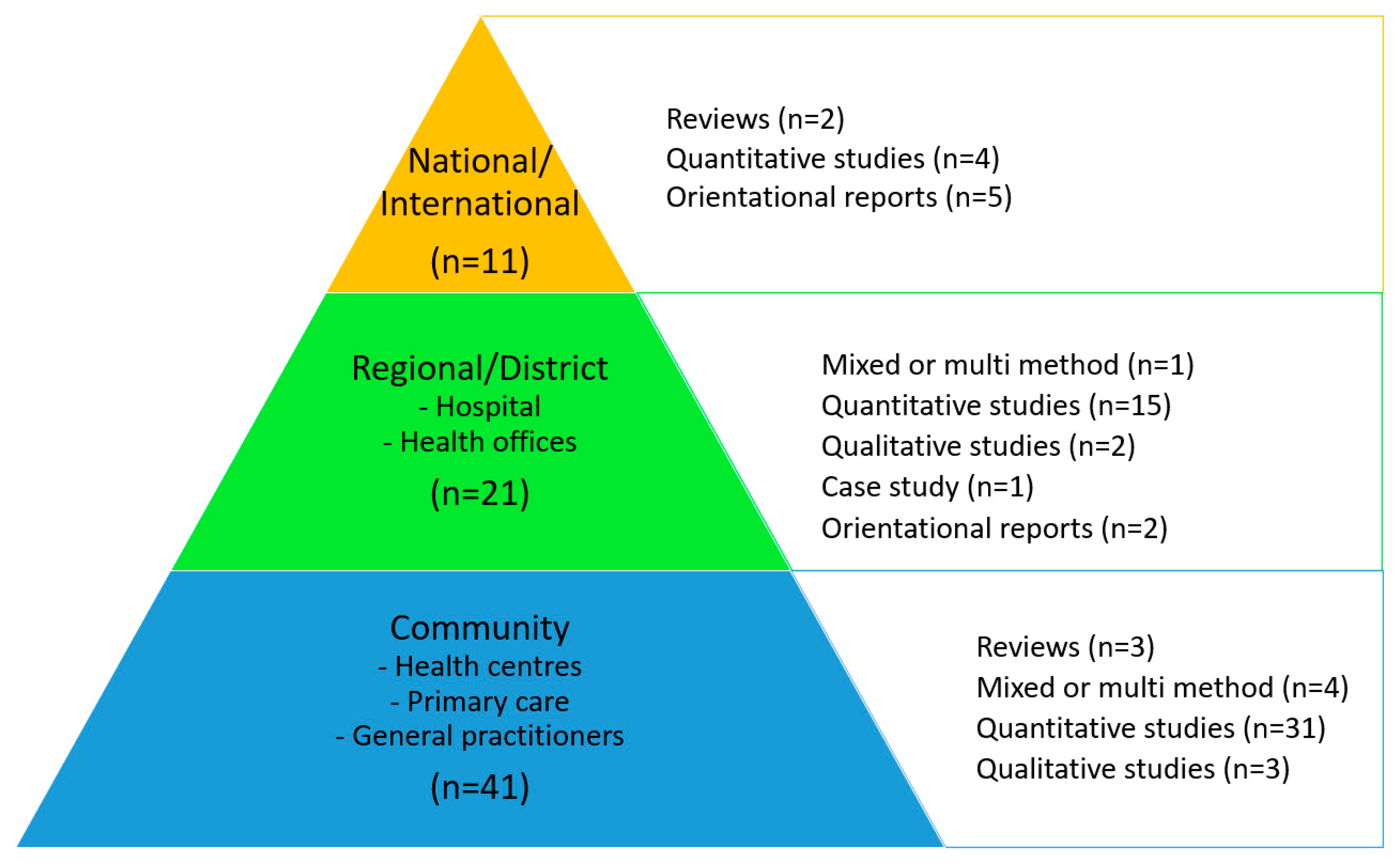
3.2. Characteristics of the Included Citations
3.3. Presence, Definitions, and Measurements of the Three Concepts
3.4. Results of the Consultation Exercise
4. Discussion
Principal Findings and Comparison with Prior Work
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| HL | Health literacy |
| EQ5D | EuroQL 5D |
| HLQ | Health literacy questionnaire |
| HLS | Health literacy survey |
| IMRAD | Introduction, methods, results, and discussion |
| PCC | Population, concept, and context |
| PedsQL | Pediatric Quality of Life Scale |
| QL | Quality of life |
| SF-36 | Short-Form 36 |
References
- Arcaya, M.C.; Arcaya, A.L.; Subramanian, S.V. Inequalities in health: Definitions, concepts, and theories. Glob. Health Action 2015, 8, 27106. [Google Scholar] [CrossRef] [PubMed]
- Marmot, M.; Friel, S. Global health equity: Evidence for action on the social determinants of health. J. Epidemiol. Community Health 2008, 62, 1095–1097. [Google Scholar] [CrossRef]
- Nutbeam, D.; Lloyd, J.E. Understanding and Responding to Health, Literacy as a Social Determinant of Health. Annu. Rev. Public Health 2021, 42, 159–173. [Google Scholar] [CrossRef] [PubMed]
- Stormacq, C.; Van den Broucke, S.; Wosinski, J. Does health literacy mediate the relationship between socioeconomic status and health disparities? Integrative review. Health Promot. Int. 2019, 34, e1–e17. [Google Scholar] [CrossRef] [PubMed]
- Stiglitz, J.E.; Sen, A.; Fitoussi, J.-P. Report by the Commission on the Measurement of Economic Performance and Social Progress; Commission on the measurement of economic performance and social progress. Government of the French Republic: Paris, France, 2009. [Google Scholar]
- United Nations (UN). Sustainable Development Goals Knowledge Platform. Available online: https://sustainabledevelopment.un.org/ (accessed on 3 March 2023).
- Krieger, N. A glossary for social epidemiology. J. Epidemiol. Community Health 2001, 55, 693–700. [Google Scholar] [CrossRef]
- Marmot, M. Achieving health equity: From root causes to fair outcomes. Lancet 2007, 370, 1153–1163. [Google Scholar] [CrossRef]
- Mielck, A.; Vogelmann, M.; Leidl, R. Health-related quality of life and socioeconomic status: Inequalities among adults with a chronic disease. Health Qual. Life Outcomes 2014, 12, 58. [Google Scholar] [CrossRef]
- Nutbeam, D.; Kickbusch, I. Health promotion glossary. Health Promot. Int. 1998, 13, 349–364. [Google Scholar] [CrossRef]
- Pelikan, J.M.; Ganahl, K.; Roethlin, F. Health literacy as a determinant, mediator and/or moderator of health: Empirical models using the European, Health, Literacy, Survey dataset. Glob. Health Promot. 2018, 25, 57–66. [Google Scholar] [CrossRef]
- Hoffmann, S.; Sander, L.; Wachtler, B.; Blume, M.; Schneider, S.; Herke, M.; Piscke, C.R.; Fialho, P.M.M.; Schuettig, W.; Tallarek, M.; et al. Moderating or mediating effects of family characteristics on socioeconomic inequalities in child health in high-income countries–a scoping review. BMC Public Health 2022, 22, 338. [Google Scholar] [CrossRef]
- Walters, R.; Leslie, S.J.; Polson, R.; Cusack, T.; Gorely, T. Establishing the efficacy of interventions to improve health literacy and health behaviours: A systematic review. BMC Public Health 2020, 20, 1040. [Google Scholar] [CrossRef] [PubMed]
- Heine, M.; Lategan, F.; Erasmus, M.; Lombaard, C.-M.; Mc Carthy, N.; Olivier, J.; van Niekerk, M.; Hanekom, S. Health education interventions to promote health literacy in adults with selected non-communicable diseases living in low-to-middle income countries: A systematic review and meta-analysis. J. Eval. Clin. Pract. 2021, 27, 1417–1428. [Google Scholar] [CrossRef] [PubMed]
- Larsen, M.H.; Mengshoel, A.M.; Andersen, M.H.; Borge, C.R.; Ahlsen, B.; Dahl, K.G.; Eik, H.; Holmen, H.; Lerdal, A.; Mariussen, K.M.; et al. “A bit of everything”: Health literacy interventions in chronic conditions—A systematic review. Patient Educ. Couns. 2022, 105, 2999–3016. [Google Scholar] [CrossRef]
- Osborne, R.H.; Cheng, C.C.; Nolte, S.; Elmer, S.; Besancon, S.; Budhathoki, S.S.; Debussche, X.; Dias, S.; Kolarčik, P.; Loureiro, M.I.; et al. Health literacy measurement: Embracing diversity in a strengths-based approach to promote health and equity, and avoid epistemic injustice. BMJ Global, Health 2022, 7, e009623. [Google Scholar] [CrossRef]
- World Health Organization. WHOQOL: Measuring Quality of Life: World Health Organization; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- International Society for Quality of Life Research. Dictionary of Quality of Life and Health Outcomes Measurement; Isoqol, Nancy, Mayo: Milwaukee, WI, USA, 2015. [Google Scholar]
- Kim, E.; Cho, S.I. Trajectories of health-related quality of life by change pattern of objective and subjective social status. SSM Popul. Health 2022, 17, 101061. [Google Scholar] [CrossRef] [PubMed]
- Knorst, J.K.; Sfreddo, C.S.; Meira, G.d.F.; Zanatta, F.B.; Vettore, M.V.; Ardenghi, T.M. Socioeconomic status and oral health-related quality of life: A systematic review and meta-analysis. Community Dent. Oral Epidemiol. 2021, 49, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Didsbury, M.S.; Kim, S.; Medway, M.M.; Tong, A.; McTaggart, S.J.; Walker, A.M.; White, S.; Mackie, F.E.; Kara, T.; Craig, J.C.; et al. Socio-economic status and quality of life in children with chronic disease: A systematic review. J. Paediatr. Child Health 2016, 52, 1062–1069. [Google Scholar] [CrossRef]
- Zarcadoolas, C.; Pleasant, A.; Greer, D.S. Understanding health literacy: An expanded model. Health Promot. Int. 2005, 20, 195–203. [Google Scholar] [CrossRef]
- World Health Organization. Health Literacy Development for the Prevention and Control of Noncommunicable Diseases: Volume 1: Overview 2022; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Zheng, M.; Jin, H.; Shi, N.; Duan, C.; Wang, D.; Yu, X.; Li, X. The relationship between health literacy and quality of life: A systematic review and meta-analysis. Health Qual. Life Outcomes 2018, 16, 201. [Google Scholar] [CrossRef]
- Elisabeth Stømer, U.; Klopstad Wahl, A.; Gunnar Gøransson, L.; Hjorthaug Urstad, K. Health literacy in kidney disease: Associations with quality of life and adherence. J. Ren. Care 2020, 46, 85–94. [Google Scholar] [CrossRef]
- Lastrucci, V.; Lorini, C.; Caini, S.; Bonaccorsi, G. Health literacy as a mediator of the relationship between socioeconomic status and health: A cross-sectional study in a population-based sample in, Florence. PLoS ONE 2019, 14, e0227007. [Google Scholar] [CrossRef] [PubMed]
- Svendsen, M.T.; Bak, C.K.; Sørensen, K.; Pelikan, J.; Riddersholm, S.J.; Skals, R.K.; Mortensen, R.N.; Maindal, H.T.; Bøggild, H.; Nielsen, G.; et al. Associations of health literacy with socioeconomic position, health risk behavior, and health status: A large national population-based survey among Danish adults. BMC Public Health 2020, 20, 565. [Google Scholar] [CrossRef] [PubMed]
- Holmen, H.; Flølo, T.N.; Tørris, C.; Løyland, B.; Almendingen, K.; Bjørnnes, A.K.; Früh, E.A.; Grov, E.K.; Helseth, S.; Kvarme, L.G.; et al. The Combined Use of the Concepts’ Social Inequality in Health, Health Literacy and Quality of Life—Protocol for a Scoping Review 2021. Available online: https://osf.io/76nsb (accessed on 3 March 2023).
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.D.J.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Chapter 11: Scoping Reviews (2020 version). In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, South Australia, 2020. [Google Scholar] [CrossRef]
- Osborne, R.H.; Batterham, R.W.; Elsworth, G.R.; Hawkins, M.; Buchbinder, R. The grounded psychometric development and initial validation of the Health Literacy Questionnaire (HLQ). BMC Public Health 2013, 13, 658. [Google Scholar] [CrossRef]
- Sørensen, K.; Van den Broucke, S.; Pelikan, J.M.; Fullam, J.; Doyle, G.; Slonska, Z.; Kondilis, B.; Stoffels, V.; Osborne, R.H.; Brand, H. Measuring health literacy in populations: Illuminating the design and development process of the European Health, Literacy Survey Questionnaire (HLS-EU-Q). BMC Public Health 2013, 13, 948. [Google Scholar] [CrossRef]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [CrossRef]
- Varni, J.W.; Limbers, C.A.; Burwinkle, T.M. Impaired health-related quality of life in children and adolescents with chronic conditions: A comparative analysis of 10 disease clusters and 33 disease categories/severities utilizing the PedsQLTM 4.0 Generic Core Scales. Health Qual. Life Outcomes 2007, 5, 43. [Google Scholar] [CrossRef]
- Veritas-Health-Innovation. Covidence Systematic Review Software; Veritas-Health-Innovation: Melbourne, Australia, 2020. [Google Scholar]
- Reynolds, E.; Martel, L.D.; Bah, M.O.; Bah, M.; Bah, M.B.; Boubacar, B.; Camara, N.; Camara, Y.B.; Corvil, S.; Diallo, B.I.; et al. Implementation of DHIS2 for Disease Surveillance in Guinea: 2015–2020. Front. Public Health 2022, 9, 761196. [Google Scholar] [CrossRef] [PubMed]
- QSR International, Pty, Ltd. NVivo Qualitative Data Analysis Software; QSR International, Pty, Ltd.: Denver, CO, USA, 2012. [Google Scholar]
- Jamieson, L.M.; Divaris, K.; Parker, E.J.; Lee, J.Y. Oral health literacy comparisons between Indigenous, Australians and American, Indians. Community Dent. Health 2013, 30, 52–57. [Google Scholar] [PubMed]
- Tan, S.S.; Pisano, M.M.; Boone, A.L.D.; Baker, G.; Pers, Y.M.; Pilotto, A.; Valsecchi, V.; Zora, S.; Zhang, X.; Fierloos, I.; et al. Evaluation, Design of EFFICHRONIC: The Chronic Disease Self-Management, Programme (CDSMP) Intervention for Citizens with a Low Socioeconomic Position. Int. J. Environ. Res. Public Health 2019, 16, 1883. [Google Scholar] [CrossRef] [PubMed]
- Uddin, M.N.; Bhar, S.; Al Mahmud, A.; Islam, F.M.A. Psychological distress and quality of life: Rationale and protocol of a prospective cohort study in a rural district in, Bangaladesh. BMJ Open 2017, 7, e016745. [Google Scholar] [CrossRef]
- Irwin, K. Improving cancer care for underserved communities in northeastern, Massachusetts: Serious mental illness and cancer. Psycho-Oncology 2018, 27 (Suppl. S1), 37–38. [Google Scholar]
- Min Fui, W.; Abdul Majid, H.; Ismail, R.; Su, T.T.; Maw Pin, T.; Said, M.A. Psychosocial factors associated with mental health and quality of life during the COVID-19 pandemic among low-income urban dwellers in Peninsular Malaysia. medRxiv 2022, 17, e0264886. [Google Scholar] [CrossRef]
- Washington, D.M.; Curtis, L.M.; Waite, K.; Wolf, M.S.; Paasche-Orlow, M.K. Sociodemographic, Factors, Mediate, Race and Ethnicity-associated, Childhood, Asthma, Health, Disparities: A Longitudinal Analysis. J. Racial Ethn. Health Disparities 2018, 5, 928–938. [Google Scholar] [CrossRef]
- Fung, C.S.C.; Yu, E.Y.T.; Guo, V.Y.; Wong, C.K.H.; Kung, K.; Ho, S.Y.; Lam, L.Y.; Ip, P.; Fong, D.Y.; Lam, D.C.; et al. Development of a Health, Empowerment Programme to improve the health of working poor families: Protocol for a prospective cohort study in Hong Kong. BMJ Open 2016, 6, e010015. [Google Scholar] [CrossRef]
- Ladak, L.A.; Gallagher, R.; Hasan, B.S.; Awais, K.; Abdullah, A.; Gullick, J. Exploring the influence of socio-cultural factors and environmental resources on the health related quality of life of children and adolescents after congenital heart disease surgery: Parental perspectives from a low middle income country. J. Patientreported Outcomes 2020, 4, 72. [Google Scholar] [CrossRef]
- Langton, C.E. Pathways to increasing child health: Implications for policy, research, and practice. Diss. Abstr. Int. Sect. A Humanit. Soc. Sci. 2012, 73, 1197. [Google Scholar]
- Reid, A.L.; Porter, K.J.; You, W.; Kirkpatrick, B.M.; Yuhas, M.; Vaught, S.S.; Zoellner, J.M. Low Health Literacy Is Associated With Energy-Balance-Related Behaviors, Quality of Life, and BMI Among Rural Appalachian Middle School Students: A Cross-Sectional, Study. J. Sch. Health 2021, 91, 608–616. [Google Scholar] [CrossRef] [PubMed]
- Webb, J. Social aspects of chronic transfusions: Addressing social determinants of health, health literacy, and quality of life. Hematology 2020, 2020, 175–183. [Google Scholar] [CrossRef]
- Alruthia, Y.; Sales, I.; Almalag, H.; Alwhaibi, M.; Almosabhi, L.; Albassam, A.A.; Alharbi, F.A.; Bashatah, A.; Asiri, Y. The relationship between health-related quality of life and trust in primary care physicians among patients with diabetes. Clin. Epidemiol. 2020, 12, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Amoah, P.A.; Phillips, D.R. Health literacy and health: Rethinking the strategies for universal health coverage in, Ghana. Public Health 2018, 159, 40–49. [Google Scholar] [CrossRef] [PubMed]
- An, J.Y.; Moon, H.; Cha, S. Health literacy, depression, and stress among, Chinese immigrants in, South, Korea. Public Health Nurs. 2019, 36, 603–614. [Google Scholar] [CrossRef] [PubMed]
- Angner, E.; Miller, M.J.; Ray, M.N.; Saag, K.G.; Allison, J.J. Health literacy and happiness: A community-based study. Soc. Indic. Res. 2010, 95, 325–338. [Google Scholar] [CrossRef]
- Apter, A.J.; Bryant, S.; Morales, K.H.; Wan, F.; Hardy, S.; Reed-Wells, S.; Dominguez, M.; Gonzalez, R.; Mak, N.; Nardi, A.; et al. Using IT to improve access, communication, and asthma in African, American and Hispanic/Latino Adults: Rationale, design, and methods of a randomized controlled trial. Contemp. Clin. Trials 2015, 44, 119–128. [Google Scholar] [CrossRef]
- Apter, A.J.; Morales, K.H.; Han, X.; Perez, L.; Huang, J.; Ndicu, G.; Localio, A.; Nardi, A.; Klusaritz, H.; Rogers, M.; et al. A patient advocate to facilitate access and improve communication, care, and outcomes in adults with moderate or severe asthma: Rationale, design, and methods of a randomized controlled trial. Contemp. Clin. Trials 2017, 56, 34–45. [Google Scholar] [CrossRef][Green Version]
- Asare, M.; McIntosh, S.; Culakova, E.; Alio, A.; Umstattd, M.M.R.; Kleckner, A.S.; Ylitalo, K.R.; Kamen, C.S. Assessing Physical, Activity, Behavior of Cancer, Survivors by, Race and Social, Determinants of Health. Int. Q. Community Health Educ. 2019, 40, 7–16. [Google Scholar] [CrossRef]
- Batista, M.J.; Lawrence, H.P.; Sousa, M. Oral health literacy and oral health outcomes in an adult population in Brazil. BMC Public Health 2017, 18, 60. [Google Scholar] [CrossRef]
- Blancafort, A.S.; Monteserin, N.R.; Moral, I.; Roque, F.M.; Rojano, I.L.X.; Coll-Planas, L. Promoting social capital, self-management and health literacy in older adults through a group-based intervention delivered in low-income urban areas: Results of the randomized trial, AEQUALIS. BMC Public Health 2021, 21, 84. [Google Scholar] [CrossRef] [PubMed]
- Clarke, H.; Voss, M. The role of a multidisciplinary student team in the community management of chronic obstructive pulmonary disease. Prim. Health Care Res. Dev. 2016, 17, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Curtis, L.M.; Wolf, M.S.; Weiss, K.B.; Grammer, L.C. The impact of health literacy and socioeconomic status on asthma disparities. J. Asthma 2012, 49, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Durand, M.A.; Yen, R.W.; O’Malley, A.J.; Schubbe, D.; Politi, M.C.; Saunders, C.H.; Dhage, S.; Rosenkranz, K.; Margenthaler, J.; Tosteson, A.N.A.; et al. What matters most: Randomized controlled trial of breast cancer surgery conversation aids across socioeconomic strata. Cancer 2021, 127, 422–436. [Google Scholar] [CrossRef] [PubMed]
- Ernsting, C.; Dombrowski, S.U.; Oedekoven, M.; Kanzler, M.; Kuhlmey, A.; Gellert, P. Using Smartphones and Health Apps to Change and Manage Health Behaviors: A Population-Based Survey. J. Med. Internet Res. 2017, 19, e101. [Google Scholar] [CrossRef] [PubMed]
- Faruqi, N.; Stocks, N.; el Spooner, C.; Haddad, N.; Harris, M.F. Research protocol: Management of obesity in patients with low health literacy in primary health care. BMC Obes. 2015, 2, 5. [Google Scholar] [CrossRef]
- Goss, H.R.; McDermott, C.; Hickey, L.; Issartel, J.; Meegan, S.; Morrissey, J.; Murrin, C.; Peers, C.; Smith, C.; Spillane, A.; et al. Understanding disadvantaged adolescents’ perception of health literacy through a systematic development of peer vignettes. BMC Public Health 2021, 21, 593. [Google Scholar] [CrossRef] [PubMed]
- Graham, L.A.; Hawn, M.T.; Dasinger, E.A.; Baker, S.J.; Oriel, B.S.; Wahl, T.S.; Richman, J.S.; Copeland, L.A.; Itani, K.M.F.; Burns, E.A.; et al. Psychosocial Determinants of Readmission after Surgery. Med. Care 2021, 59, 864–871. [Google Scholar] [CrossRef]
- Guhl, E.; Althouse, A.; Sharbaugh, M.; Pusateri, A.M.; Paasche-Orlow, M.; Magnani, J.W. Association of income and health-related quality of life in atrial fibrillation. Open Heart 2019, 6, e000974. [Google Scholar] [CrossRef]
- Harsch, S.; Jawid, A.; Jawid, M.E.; Saboga, N.L.; Sahrai, D.; Bittlingmayer, U.H. The relationship of health literacy, wellbeing and religious beliefs in neglected and unequal contexts-Results of a survey study in central, Afghanistan. Health Promot. J. Aust. 2021, 32 (Suppl. S1), 80–87. [Google Scholar] [CrossRef]
- Hickey, K.T.; Masterson, C.R.M.; Reading, M.; Sciacca, R.R.; Riga, T.C.; Frulla, A.P.; Casida, J.M. Low health literacy: Implications for managing cardiac patients in practice. Nurse Pract. 2018, 43, 49–55. [Google Scholar] [CrossRef]
- Johnson, D.R.; McDermott, R.A.; Clifton, P.M.; D’Onise, K.; Taylor, S.M.; Preece, C.L.; Schmidt, B.A. Characteristics of Indigenous adults with poorly controlled diabetes in north, Queensland: Implications for services. BMC Public Health 2015, 15, 325. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T.; Martin, C.K.; Newton, R.L.; Apolzan, J.W., Jr.; Arnold, C.L.; Davis, T.C.; Denstel, K.D.; Mire, E.F.; Thethi, T.K.; Brantley, P.J.; et al. Promoting Successful Weight, Loss in Primary Care in Louisiana (PROPEL): Rationale, design and baseline characteristics. Contemp. Clin. Trials 2018, 67, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.P.; Bennett, C.L.; Chan, C.; Chmiel, J.; Falcone, D.; Knight, S.J.; Kuzel, T.; Davis, T.C.; Elstein, A.S.; Moran, E.; et al. QOL and outcomes research in prostate cancer patients with low socioeconomic status. Oncology 1999, 13, 823–832. [Google Scholar] [PubMed]
- Kim, S.P.; Knight, S.J.; Tomori, C.; Colella, K.M.; Schoor, R.A.; Shih, L.; Kuzel, T.; Nadler, R.B.; Bennett, C.L. Health literacy and shared decision making for prostate cancer patients with low socioeconomic status. Cancer Investig. 2001, 19, 684–691. [Google Scholar] [CrossRef] [PubMed]
- Lang, L.P. Self-Care Management in Homeless Adults with Hypertension. A Dissertation Submitted to the School of Nursing in Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy in Nursing. Ph.D. Thesis, Azusa Pacific University, Azusa, CA, USA, 2020. [Google Scholar]
- Macabasco-O’Connell, A.; DeWalt, D.A.; Broucksou, K.A.; Hawk, V.; Baker, D.W.; Schillinger, D.; Ruo, B.; Bibbins-Domingo, K.; Holmes, G.M.; Erman, B.; et al. Relationship between literacy, knowledge, self-care behaviors, and heart failure-related quality of life among patients with heart failure. J. Gen. Intern. Med. 2011, 26, 979–986. [Google Scholar] [CrossRef]
- McDougall, J.A.; Blair, C.K.; Wiggins, C.L.; Goodwin, M.B.; Chiu, V.K.; Rajput, A.; Kinney, A.Y. Socioeconomic disparities in health-related quality of life among colorectal cancer survivors. J. Cancer Surviv. 2019, 13, 459–467. [Google Scholar] [CrossRef]
- Meyers, A.G.; Salanitro, A.; Wallston, K.A.; Cawthon, C.; Vasilevskis, E.E.; Goggins, K.M.; Davis, C.M.; Rothman, R.L.; Castel, L.D.; Donato, K.M.; et al. Determinants of health after hospital discharge: Rationale and design of the Vanderbilt Inpatient Cohort Study (VICS). BMC Health Serv. Res. 2014, 14, 10. [Google Scholar] [CrossRef]
- Miller, D.B.; Cage, J.L.; Nowacki, A.S.; Jackson, B.; Modlin, C.S. Health, Literacy (HL) & Health-Related, Quality of Life (HRQL) Among Minority Men. J. Natl. Med. Assoc. 2018, 110, 124–129. [Google Scholar] [CrossRef]
- Myaskovsky, L.; Burkitt, K.H.; Lichy, A.M.; Ljungberg, I.H.; Fyffe, D.C.; Ozawa, H.; Switzer, G.E.; Fine, M.J.; Boninger, M.L. The association of race, cultural factors, and health-related quality of life in persons with spinal cord injury. Arch. Phys. Med. Rehabil. 2011, 92, 441–448. [Google Scholar] [CrossRef]
- Omachi, T.A.; Sarkar, U.; Yelin, E.H.; Blanc, P.D.; Katz, P.P. Lower health literacy among, COPD patients is associated with poorer, COPD functional outcomes and greater risk of COPD-related emergency utilization. J Gen Intern Med. 2013, 28, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Ownby, R.L.; Acevedo, A.; Waldrop-Valverde, D.; Caballero, J.; Simonson, M.; Davenport, R.; Kondwani, K.; Jacobs, R.J. A Mobile App for Chronic Disease Self-Management: Protocol for a Randomized Controlled Trial. JMIR Res. Protoc. 2017, 6, e53. [Google Scholar] [CrossRef]
- Park, N.H.; Song, M.S.; Shin, S.Y.; Jeong, J.-H.; Lee, H.Y. The effects of medication adherence and health literacy on health-related quality of life in older people with hypertension. Int. J. Older People Nurs. 2018, 13, e12196. [Google Scholar] [CrossRef] [PubMed]
- Prihanto, J.B.; Wahjuni, E.S.; Nurhayati, F.; Matsuyama, R.; Tsunematsu, M.; Kakehashi, M. Health, Literacy, Health, Behaviors, and Body, Mass, Index, Impacts on, Quality of Life: Cross-Sectional, Study of University, Students in, Surabaya, Indonesia. Int. J. Environ. Res. Public Health 2021, 18, 13132. [Google Scholar] [CrossRef]
- Rak, E.C. Quality of life of persons with diabetes: Understanding the effects of health literacy, self-efficacy and knowledge of chronic illness and disability. Diss. Abstr. Int. Sect. B Sci. Eng. 2012, 73, 2535. [Google Scholar]
- Rijken, M.; van der Heide, I. Identifying subgroups of persons with multimorbidity based on their needs for care and support. BMC Fam. Pract. 2019, 20, 179. [Google Scholar] [CrossRef]
- Roberto, L.L.; Noronha, D.D.; Souza, T.O.; Miranda, E.J.P.; Martins, A.M.E.B.L.; Paula, A.M.B.; Ferreira, E.F.E.; Haikal, D.S. Lack of access to information on oral health problems among adults: An approach based on the theoretical model for literacy in health. Cienc. Saude Coletiva 2018, 23, 823–835. (In Portuguese) [Google Scholar] [CrossRef]
- Scheuer, S. The patient navigation project for socially vulnerable cancer patients improves quality of life and health literacy. J. Glob. Oncol. 2018, 4 (Suppl. S2), 110s. [Google Scholar] [CrossRef]
- Simon, M.A.; Li, Y.; Dong, X. Levels of health literacy in a community-dwelling population of Chinese older adults. J. Gerontol. Ser. A-Biol. Sci. Med. Sci. 2014, 69 (Suppl. S2),, S54–S60. [Google Scholar] [CrossRef][Green Version]
- Todorovic, N.; Jovic-Vranes, A.; Djikanovic, B.; Pilipovic-Broceta, N.; Vasiljevic, N.; Lucic-Samardzija, V.; Peric, A. Assessment of health literacy in the adult population registered to family medicine physicians in the Republic of Srpska Bosnia and Herzegovina. Eur. J. Gen. Pract. 2019, 25, 32–38. [Google Scholar] [CrossRef]
- Virlée, J.; van Riel, A.C.R.; Hammedi, W. Health literacy and its effects on well-being: How vulnerable healthcare service users integrate online resources. J. Serv. Mark. 2020, 34, 697–715. [Google Scholar] [CrossRef]
- Walker, R.J.; Gebregziabher, M.; Martin-Harris, B.; Egede, L.E. Independent effects of socioeconomic and psychological social determinants of health on self-care and outcomes in, Type 2 diabetes. Gen. Hosp. Psychiatry 2014, 36, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Li, H.; Li, L.; Xu, D.; Kane, R.L.; Meng, Q. Health literacy and ethnic disparities in health-related quality of life among rural women: Results from a Chinese poor minority area. Health Qual. Life Outcomes 2013, 11, 153. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Kane, R.L.; Xu, D.; Meng, Q. Health literacy as a moderator of health-related quality of life responses to chronic disease among, Chinese rural women. BMC Women’s Health 2015, 15, 34. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Z.; Lee, J.; Liu, W. Korean and Vietnamese immigrants are not the same: Health literacy, health status, and quality of life. J. Hum. Behav. Soc. Environ. 2020, 30, 711–729. [Google Scholar] [CrossRef]
- Xu, R.H.; Zhou, L.M.; Wong, E.L.Y.; Wang, D. The association between patients’ ehealth literacy and satisfaction with shared decision-making and well-being: Multicenter cross-sectional study. J. Med. Internet Res. 2021, 23, e26721. [Google Scholar] [CrossRef]
- Aaby, A.; Friis, K.; Christensen, B.; Maindal, H.T. Health, Literacy among, People in, Cardiac, Rehabilitation: Associations with Participation and Health-Related Quality of Life in the Heart Skills Study in Denmark. Int. J. Environ. Res. Public Health 2020, 17, 443. [Google Scholar] [CrossRef]
- Ghisi, G.L.D.M.; Chaves, G.S.D.S.; Britto, R.R.; Oh, P. Health literacy and coronary artery disease: A systematic review. Patient Educ. Couns. 2018, 101, 177–184. [Google Scholar] [CrossRef]
- Gibbs, J.F.; Guarnieri, E.; Chu, Q.D.; Murdoch, K.; Asif, A. Value-based chronic care model approach for vulnerable older patients with multiple chronic conditions. J. Gastrointest. Oncol. 2021, 12 (Suppl. S2), S324–S338. [Google Scholar] [CrossRef]
- Maliski, S.L.; Connor, S.E.; Oduro, C.; Litwin, M.S. Access to health care and quality of life for underserved men with prostate cancer. Semin. Oncol. Nurs. 2011, 27, 267–277. [Google Scholar] [CrossRef]
- Schaffler, J.; Leung, K.; Tremblay, S.; Merdsoy, L.; Lambert, S.D.; Belzile, E.; Lambrou, A.; Lambert, S.D. The Effectiveness of Self-Management Interventions for Individuals with Low Health Literacy and/or Low Income: A Descriptive Systematic Review. JGIM J. Gen. Intern. Med. 2018, 33, 510–523. [Google Scholar] [CrossRef] [PubMed]
- Stormacq, C.; Wosinski, J.; Boillat, E.; Den Broucke, S.V. Effects of health literacy interventions on health-related outcomes in socioeconomically disadvantaged adults living in the community: A systematic review. JBI Evid. Synth. 2020, 18, 1389–1469. [Google Scholar] [CrossRef] [PubMed]
- Hardgraves, V.M.; Henry, L.J.; Patton, S.K. “I’m Gonna Hang on to These as Long as I Can”: Examining the Perspectives and Knowledge of Oral Health Issues of Older Adults Living Independently. Am. J. Lifestyle Med. 2021, 15598276211026842. [Google Scholar] [CrossRef]
- Lowe, S.M.; Nobriga, C.V. Head and Neck Cancer in a Rural, U.S. Population: Quality of Life Coping Health Care Literacy and Access to Services. Am. J. Speech-Lang. Pathol. 2021, 30, 1116–1133. [Google Scholar] [CrossRef] [PubMed]
- Talmage, C.A.; Figueroa, H.L.; Wolfersteig, W.L. Cultivating a culture of health in the southwest: Linking access and social determinants to quality of life amongst diverse communities. J. Health Hum. Serv. Adm. 2018, 40, 397–432. [Google Scholar]
- White, B.M.; Hall, E.S.; Johnson, C. Environmental health literacy in support of social action: An environmental justice perspective. Journal of Environmental, Health 2014, 77, 24–29. [Google Scholar] [PubMed]
- Albus, C. Health literacy: Is it important for cardiovascular disease prevention? Eur. J. Prev. Cardiol. 2018, 25, 934–935. [Google Scholar] [CrossRef]
- Bragard, I.; Coucke, P.A.; Petre, B.; Etienne, A.M.; Guillaume, M. Health literacy, a way to reduce social health inequalities. Rev. Med. De Liege 2017, 72, 32–36. [Google Scholar]
- de Vries, E.; Buitrago, G.; Quitian, H.; Wiesner, C.; Castillo, J.S. Access to cancer care in, Colombia, a middle-income country with universal health coverage. J. Cancer Policy 2018, 15, 104–112. [Google Scholar] [CrossRef]
- Griech, S.F.; Skrzat, J.M. Roles for Physical, Therapists to Address Health Literacy as a Social, Determinant of Cardiovascular Disease: A Clinical Perspective. Cardiopulm. Phys. Ther. J. 2020, 31, 29–34. [Google Scholar] [CrossRef]
- Kuehnert, P.; Fawcett, J.; DePriest, K.; Chinn, P.; Cousin, L.; Ervin, N.; Flanagan, J.; Fry-Bowers, E.; Killion, C.; Maliski, S.; et al. Defining the social determinants of health for nursing action to achieve health equity: A consensus paper from the American Academy of Nursing. Nurs. Outlook 2022, 70, 10–27. [Google Scholar] [CrossRef]
- Merriman, B.; Ades, T.; Seffrin, J.R. Health literacy in the information age: Communicating cancer information to patients and families. Electroanalysis 2002, 52, 130–133. [Google Scholar] [CrossRef] [PubMed]
- Rozier, R.G. Oral health in, North, Carolina: Innovations, opportunities, and challenges. North Carol. Med. J. 2012, 73, 100–107. [Google Scholar] [CrossRef]
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [PubMed]
- Degan, T.J.; Kelly, P.J.; Robinson, L.D.; Deane, F.P.; Wolstencroft, K.; Turut, S.; Meldrum, R. Health literacy in people living with mental illness: A latent profile analysis. Psychiatry Res 2019, 280, 112499. [Google Scholar] [CrossRef] [PubMed]
- Løyland, B.; Miaskowski, C.; Dahl, E.; Paul, S.M.; Rustøen, T. Psychological distress and quality of life in long-term social assistance recipients compared to the Norwegian population. Scand J. Public Health 2011, 39, 303–311. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.F.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H.; (HLS-EU) Consortium Health Literacy Project European. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef]
- Costa, D.S.J.; Mercieca-Bebber, R.; Rutherford, C.; Tait, M.-A.; King, M.T. How is quality of life defined and assessed in published research? Qual. Life Res. 2021, 30, 2109–2121. [Google Scholar] [CrossRef]
- Haraldstad, K.; Wahl, A.; Andenæs, R.; Andersen, J.R.; Andersen, M.H.; Beisland, E.; Borge, C.R.; Engebretsen, E.; Eisemann, M.; Halvorsrud, L.; et al. A systematic review of quality of life research in medicine and health sciences. Qual. Life Res. 2019, 28, 2641–2650. [Google Scholar] [CrossRef]
- Dahlgren, G.; Whitehead, M. The Dahlgren-Whitehead model of health determinants: 30 years on and still chasing rainbows. Public health 2021, 199, 20–24. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PCC Element | Scoping Review Target | Inclusion Criteria | Exclusion Criteria |
|---|---|---|---|
| Population | Citations reflecting on or involving humans throughout a life course. | All ages and all life situations reflecting or involving humans from birth to death. | Animal studies. Autopsy studies. |
| Concept | Any associations between the concepts of social inequality in health, health literacy, and quality of life. | All three concepts must be applied in their widest form together in the research citation (according to the search terms). | Citations reporting on only one or two of the concepts. |
| Context | All contexts involving humans. |
| (a) | ||||||
|---|---|---|---|---|---|---|
| Author | Social Inequality in Health Definition | Social Inequality in Health Assessment | Health Literacy Definition | Health Literacy Assessment | Quality of Life Definition | Quality of Life Assessment |
| Alruthia, Y., et al. [52] | ||||||
| Amoah, P. A., et al. [53] | ||||||
| An, J. Y., et al. [54] | ||||||
| Angner, E., et al. [55] | ||||||
| Apter, A. J., et al. [56] | ||||||
| Apter, A. J., et al. [57] | ||||||
| Asare, M., et al. [58] | ||||||
| Batista, M. J., et al. [59] | ||||||
| Blancafort Alias, S., et al. [60] | ||||||
| Clarke, H., et al. [61] | ||||||
| Curtis, L. M., et al. [62] | ||||||
| Durand, M. A., et al. [63] | ||||||
| Ernsting, C., et al. [64] | ||||||
| Faruqi, N., et al. [65] | ||||||
| Fung, C. S. C., et al. [47] | ||||||
| Goss, H. R., et al. [66] | ||||||
| Graham, L. A., et al. [67] | ||||||
| Guhl, E., et al. [68] | ||||||
| Harsch, S., et al. [69] | ||||||
| Hickey, K. T., et al. [70] | ||||||
| Irwin, K., et al. [44] | ||||||
| Jamieson, L. M., et al. [41] | ||||||
| Johnson, D. R., et al. [71] | ||||||
| Katzmarzyk, P. T., et al. [72] | ||||||
| Kim, S. P., et al. [73] | ||||||
| Kim, S. P., et al. [74] | ||||||
| Lang, L. P. [75] | ||||||
| Langton, C. E. [49] | ||||||
| Macabasco-O’Connell, A. et al. [76] | ||||||
| McDougall, J. A., et al. [77] | ||||||
| Meyers, A. G., et al. [78] | ||||||
| Miller, D. B., et al. [79] | ||||||
| Myaskovsky, L., et al. [80] | ||||||
| Omachi, T. A. et al. [81] | ||||||
| Ownby, R. L., et al. [82] | ||||||
| Park, N. H., et al. [83] | ||||||
| Prihanto, J. B., et al. [84] | ||||||
| Rak, E. C. [85] | ||||||
| Reid, A. L., et al. [50] | ||||||
| Rijken, M., et al. [86] | ||||||
| Roberto, L. L., et al. [87] | ||||||
| Scheuer, S. [88] | ||||||
| Simon, M. A., et al. [89] | ||||||
| Tan, S. S., et al. [42] | ||||||
| Todorovic, N., et al. [90] | ||||||
| Uddin, M. N., et al. [43] | ||||||
| Virlée, J., et al. [91] | ||||||
| Walker, R. J., et al. [92] | ||||||
| Wang, C., et al. [93] | ||||||
| Wang, C., et al. [94] | ||||||
| Washington, D. M., et al. [46] | ||||||
| Wong Min, F., et al. [45] | ||||||
| Xiao, Z., et al. [95] | ||||||
| Xu, R. H., et al. [96] | ||||||
| Aaby, A., et al. [97] | ||||||
| (b) | ||||||
| Author | Social Inequality in Health Definition | Health Literacy Definition | Quality of Life Definition | |||
| Reviews | ||||||
| Ghisi, G., et al. [98] | ||||||
| Gibbs, J. F., et al. [99] | ||||||
| Maliski, S. L., et al. [100] | ||||||
| Schaffler, J., et al. [101] | ||||||
| Stormacq, C., et al. [102] | ||||||
| Qualitative Studies | ||||||
| Hardgraves, V. M., et al. [103] | ||||||
| Ladak, L. A., et al. [48] | ||||||
| Lowe, S. M., et al. [104] | ||||||
| Talmage, C. A., [105] | ||||||
| White, B. M., [106] | ||||||
| Case Study | ||||||
| Webb, J. [51] | ||||||
| Orientational Reports | ||||||
| Albus, C., [107] | ||||||
| Bragard, L., et al. [108] | ||||||
| de Vries, E., et al. [109] | ||||||
| Griech, S. F., et al. [110] | ||||||
| Kuehnert, et al. [111] | ||||||
| Merriman, B., et al. [112] | ||||||
| Rozier, R. G. [113] | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holmen, H.; Flølo, T.; Tørris, C.; Løyland, B.; Almendingen, K.; Bjørnnes, A.K.; Albertini Früh, E.; Grov, E.K.; Helseth, S.; Kvarme, L.G.; et al. Unpacking the Public Health Triad of Social Inequality in Health, Health Literacy, and Quality of Life—A Scoping Review of Research Characteristics. Int. J. Environ. Res. Public Health 2024, 21, 36. https://doi.org/10.3390/ijerph21010036
Holmen H, Flølo T, Tørris C, Løyland B, Almendingen K, Bjørnnes AK, Albertini Früh E, Grov EK, Helseth S, Kvarme LG, et al. Unpacking the Public Health Triad of Social Inequality in Health, Health Literacy, and Quality of Life—A Scoping Review of Research Characteristics. International Journal of Environmental Research and Public Health. 2024; 21(1):36. https://doi.org/10.3390/ijerph21010036
Chicago/Turabian StyleHolmen, Heidi, Tone Flølo, Christine Tørris, Borghild Løyland, Kari Almendingen, Ann Kristin Bjørnnes, Elena Albertini Früh, Ellen Karine Grov, Sølvi Helseth, Lisbeth Gravdal Kvarme, and et al. 2024. "Unpacking the Public Health Triad of Social Inequality in Health, Health Literacy, and Quality of Life—A Scoping Review of Research Characteristics" International Journal of Environmental Research and Public Health 21, no. 1: 36. https://doi.org/10.3390/ijerph21010036
APA StyleHolmen, H., Flølo, T., Tørris, C., Løyland, B., Almendingen, K., Bjørnnes, A. K., Albertini Früh, E., Grov, E. K., Helseth, S., Kvarme, L. G., Malambo, R., Misvær, N., Rasalingam, A., Riiser, K., Sandbekken, I. H., Schippert, A. C., Sparboe-Nilsen, B., Sundar, T. K. B., Sæterstrand, T., ... Torbjørnsen, A. (2024). Unpacking the Public Health Triad of Social Inequality in Health, Health Literacy, and Quality of Life—A Scoping Review of Research Characteristics. International Journal of Environmental Research and Public Health, 21(1), 36. https://doi.org/10.3390/ijerph21010036